Predictive Value of the Third Ventricle Width for Neurological Status in Multiple Sclerosis


Abstract
1. Introduction
2. Methods
2.1. Participants and Procedures
2.2. Clinical and Neuropsychological Assessments
- Symbol Digit Modalities Test (SDMT) [20] is a simple substitution task evaluating attention and information processing speed. The written version of SDMT was administered. The test score was the number of correctly paired numbers with given geometric figures in 90 s.
- The Polish version of the California Verbal Learning Test (CVLT) [21] was used to assess verbal memory. The initial five learning trials were administered, and the test score was the total number of correct responses recorded across the five trials.
- Brief Visuospatial Memory Test-Revised (BVMT-R) [22] was used to evaluate visual memory. The initial three learning trials were administered, the test score was the sum of all three trials.
2.3. MR Examination
2.4. Statistical Analysis
3. Results
3.1. Clinical and Neuropsychological Outcomes
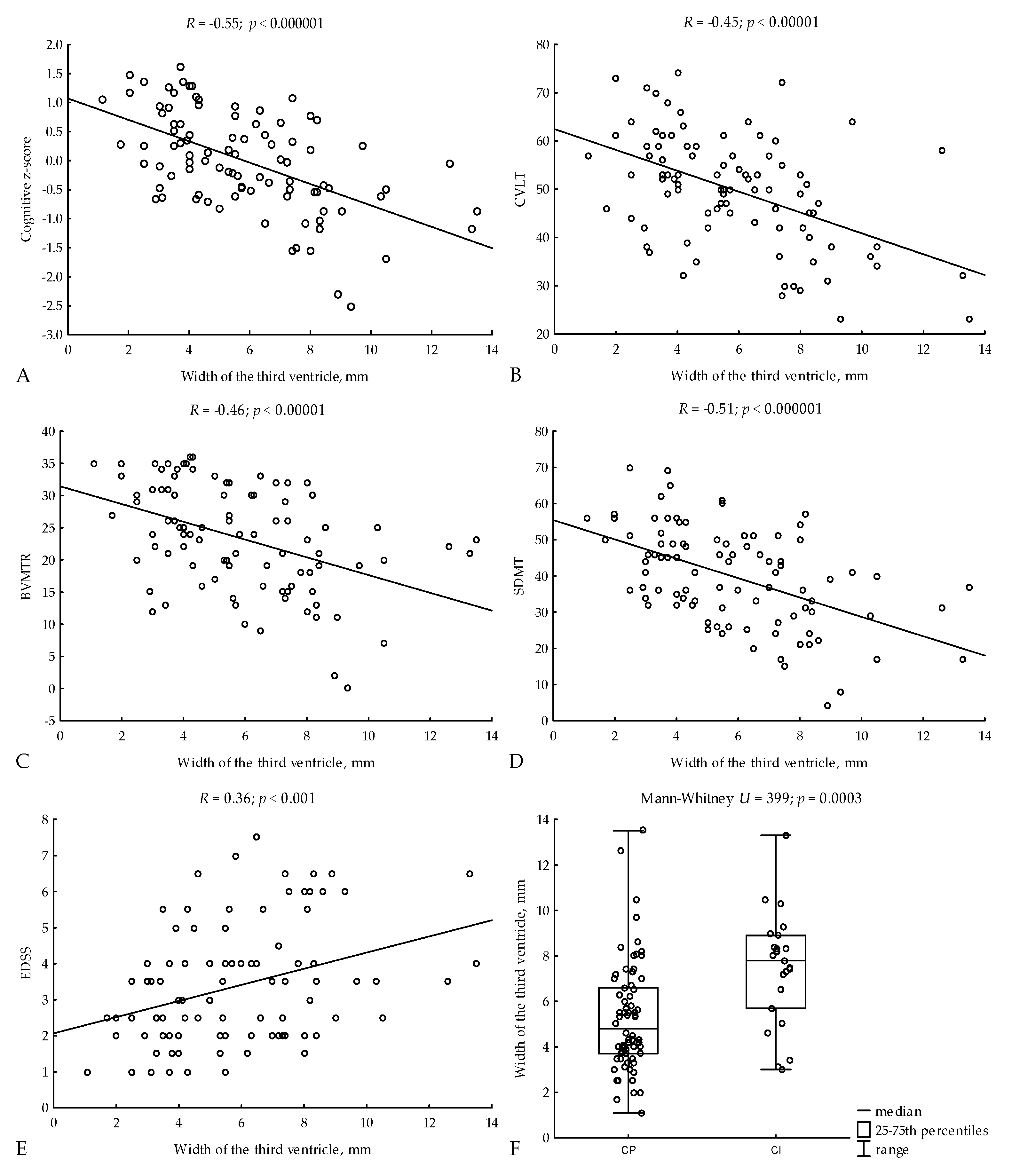
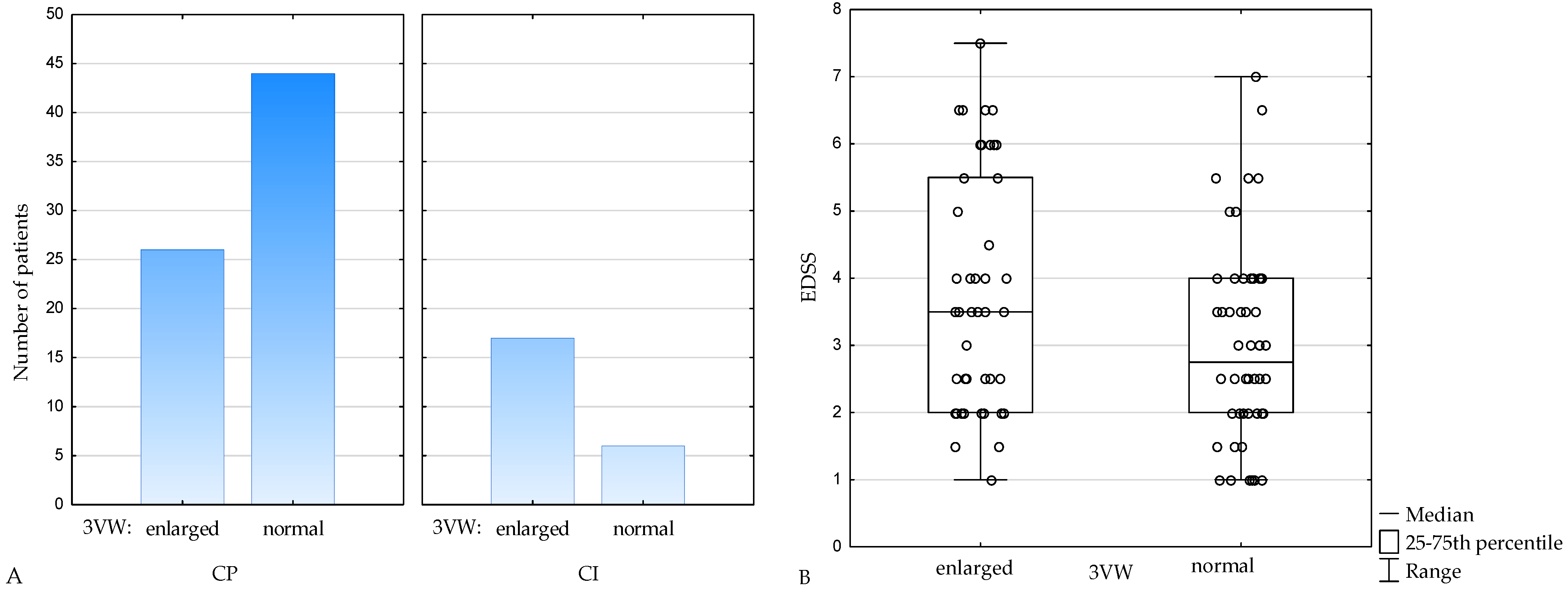
3.2. Relations of 3VW to Clinical and Neuropsychological Outcomes
3.3. Predictive Value of 3VW for Cognitive Impairment and Disability—Multiple Regression Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Preziosa, P.; Rocca, M.A.; Pagani, E.; Stromillo, M.L.; Enzinger, C.; Gallo, A.; Hulst, H.E.; Atzori, M.; Pareto, D.; Riccitelli, G.C.; et al. Structural MRI correlates of cognitive impairment in patients with multiple sclerosis: A multicenter study. Hum. Brain Mapp. 2016, 37, 1627–1644. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M.; Enzinger, C.; Langkammer, C.; Petrovic, K.; Loitfelder, M.; Tscherner, M.; Jehna, M.; Bachmaier, G.; Wallner-Blazek, M.; Ropele, S.; et al. Cognitive impairment in relation to MRI metrics in patients with clinically isolated syndrome. Mult. Scler. J. 2011, 17, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Benedict, R.H.B.; Weinstock-Guttman, B.; Fishman, I.; Sharma, J.; Tjoa, C.W.; Bakshi, R. Prediction of neuropsychological impairment in multiple sclerosis: Comparison of conventional magnetic resonance imaging measures of atrophy and lesion burden. Arch. Neurol. 2004, 61, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Sanfilipo, M.P.; Benedict, R.H.; Weinstock-Guttman, B.; Bakshi, R. Gray and white matter brain atrophy and neuropsychological impairment in multiple sclerosis. Neurology 2006, 66, 685–692. [Google Scholar] [CrossRef]
- Roosendaal, S.D.; Bendfeldt, K.; Vrenken, H.; Polman, C.H.; Borgwardt, S.; Radue, E.W.; Kappos, L.; Pelletier, D.; Hauser, S.L.; Matthews, P.M.; et al. Grey matter volume in a large cohort of MS patients: Relation to MRI parameters and disability. Mult. Scler. J. 2011, 17, 1098–1106. [Google Scholar] [CrossRef]
- Vingara, L.K.; Yu, H.J.; Wagshul, M.E.; Serafin, D.; Christodoulou, C.; Pelczer, I.; Krupp, L.B.; Maletić-Savatić, M. Metabolomic approach to human brain spectroscopy identifies associations between clinical features and the frontal lobe metabolome in multiple sclerosis. NeuroImage 2013, 82, 586–594. [Google Scholar] [CrossRef]
- Jacobsen, C.; Hagemeier, J.; Myhr, K.-M.; Nyland, H.; Lode, K.; Bergsland, N.; Ramasamy, D.P.; Dalaker, T.O.; Larsen, J.P.; Farbu, E.; et al. Brain atrophy and disability progression in multiple sclerosis patients: A 10-year follow-up study. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1109–1115. [Google Scholar] [CrossRef]
- Narayana, P.A. Magnetic Resonance Spectroscopy in the Monitoring of Multiple Sclerosis. J. Neuroimaging 2005, 15, 46S–57S. [Google Scholar] [CrossRef]
- Cappelle, S.; Pareto, D.; Tintoré, M.; Vidal-Jordana, A.; Alyafeai, R.; Alberich, M.; Sastre-Garriga, J.; Auger, C.; Montalban, X.; Rovira, À. A validation study of manual atrophy measures in patients with Multiple Sclerosis. Neuroradiology 2020, 62, 955–964. [Google Scholar] [CrossRef]
- Nishizawa, K.; Fujimori, J.; Nakashima, I. Two-dimensional measurements with cut-off values are useful for assessing brain volume, physical disability, and processing speed in multiple sclerosis. Mult. Scler. Relat. Disord. 2022, 59, 103543. [Google Scholar] [CrossRef]
- Laffon, M.; Malandain, G.; Joly, H.; Cohen, M.; Lebrun-Frenay, C. The HV3 Score: A New Simple Tool to Suspect Cognitive Impairment in Multiple Sclerosis in Clinical Practice. Neurol. Ther. 2014, 3, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Lutz, T.; Bellenberg, B.; Schneider, R.; Weiler, F.; Köster, O.; Lukas, C. Central Atrophy Early in Multiple Sclerosis: Third Ventricle Volumetry versus Planimetry. J. Neuroimaging 2017, 27, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Artemiadis, A.; Anagnostouli, M.; Zalonis, I.; Chairopoulos, K.; Triantafyllou, N. Structural MRI correlates of cognitive function in multiple sclerosis. Mult. Scler. Relat. Disord. 2018, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.P.; Nieto, A.; Barroso, J.; Martin, V.; Hernández, M.A. Brain atrophy as a marker of cognitive impairment in mildly disabling relapsing-remitting multiple sclerosis. Eur. J. Neurol. 2008, 15, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Wollenweber, F.A.; Schomburg, R.; Probst, M.; Schneider, V.; Hiry, T.; Ochsenfeld, A.; Mueller, M.; Dillmann, U.; Fassbender, K.; Behnke, S. Width of the third ventricle assessed by transcranial sonography can monitor brain atrophy in a time- and cost-effective manner—Results from a longitudinal study on 500 subjects. Psychiatry Res. Neuroimaging 2011, 191, 212–216. [Google Scholar] [CrossRef]
- Siegert, R.J.; Abernethy, D.A. Depression in multiple sclerosis: A review. J. Neurol. Neurosurg. Psychiatry. 2005, 76, 469–475. [Google Scholar] [CrossRef]
- Beiske, A.G.; Svensson, E.; Sandanger, I.; Czujko, B.; Pedersen, E.D.; Aarseth, J.H.; Myhr, K.M. Depression and anxiety amongst multiple sclerosis patients. Eur. J. Neurol. 2008, 15, 239–245. [Google Scholar] [CrossRef]
- Minden, S.L.; Frankel, D.; Hadden, L.; Perloff, J.; Srinath, K.P.; Hoaglin, D.C. The Sonya Slifka longitudinal multiple sclerosis study: Methods and sample characteristics. Mult. Scler. 2006, 12, 24–38. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Smith, A. Symbol Digit Modalities Test: Manual; Western Psychological Services: Los Angeles, CA, USA, 1982. [Google Scholar]
- Łojek, E.; Stańczak, J. Kalifornijski Test Uczenia się językowego (CVLT); Psychological Test Laboratory of the Polish Psychological Association: Warsaw, Poland, 2010. [Google Scholar]
- Benedict, R.H. Brief Visuospatial Memory Test—Revised: Professional Manual; FPAR Inc.: Odessa, FL, USA, 1997. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Gruszczak, A.; Bartosik-Psujek, H.; Pocińska, K.; Stelmasiak, Z. Analiza walidacyjna wybranych aspektów psychometrycznych polskiej wersji Zmodyfikowanej Skali Wpływu Zmęczenia (Modifed Fatigue Impact Scale)—Wyniki wstępne. Neurol. Neurochir. Pol. 2009, 43, 148–154. [Google Scholar] [PubMed]
- Polat, S.; Öksüzler, F.Y.; Öksüzler, M.; Kabakci, A.G.; Yücel, A.H. Morphometric MRI Study of the Brain Ventricles in Healthy Turkish Subjects. Int. J. Morphol. 2019, 37, 554–560. [Google Scholar] [CrossRef]
- Eshaghi, A.; Marinescu, R.V.; Young, A.; Firth, N.C.; Prados, F.; Cardoso, M.J.; Tur, C.; De Angelis, F.; Cawley, N.; Brownlee, W.J.; et al. Progression of regional grey matter atrophy in multiple sclerosis. Brain 2018, 141, 1665–1677. [Google Scholar] [CrossRef] [PubMed]
- Houtchens, M.K.; Benedict, R.; Killiany, R.; Sharma, J.; Jaisani, Z.; Singh, B.; Weinstock-Guttman, B.; Guttmann, C.R.; Bakshi, R. Thalamic atrophy and cognition in multiple sclerosis. Neurology 2007, 69, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- Cifelli, A.; Arridge, M.; Jezzard, P.; Esiri, M.M.; Palace, J.; Matthews, P.M. Thalamic neurodegeneration in multiple sclerosis. Ann. Neurol. 2002, 52, 650–653. [Google Scholar] [CrossRef]
- Preul, C.; Hund-Georgiadis, M.; Forstmann, B.U.; Lohmann, G. Characterization of cortical thickness and ventricular width in normal aging: A morphometric study at 3 Tesla. J. Magn. Reson. Imaging 2006, 24, 513–519. [Google Scholar] [CrossRef]
- Chiaravalloti, N.D.; DeLuca, J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008, 7, 1139–1151. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Bruce, J.M.; Dwyer, M.; Abdelrahman, N.; Hussein, S.; Weinstock-Guttman, B.; Garg, N.; Munschauer, F.; Zivadinov, R. Neocortical Atrophy, Third Ventricular Width, and Cognitive Dysfunction in Multiple Sclerosis. Arch. Neurol. 2006, 63, 1301–1306. [Google Scholar] [CrossRef]
- Papathanasiou, A.; Messinis, L.; Zampakis, P.; Panagiotakis, G.; Gourzis, P.; Georgiou, V.; Papathanasopoulos, P. Thalamic atrophy predicts cognitive impairment in relapsing remitting multiple sclerosis. Effect on instrumental activities of daily living and employment status. J. Neurol. Sci. 2015, 358, 236–242. [Google Scholar] [CrossRef]
- Heesen, C.; Schulz, K.; Fiehler, J.; Von der Mark, U.; Otte, C.; Jung, R.; Poettgen, J.; Krieger, T.; Gold, S. Correlates of cognitive dysfunction in multiple sclerosis. Brain, Behav. Immun. 2010, 24, 1148–1155. [Google Scholar] [CrossRef]
- Amato, M.P.; Portaccio, E.; Goretti, B.; Zipoli, V.; Hakiki, B.; Giannini, M.; Pastò, L.; Razzolini, L. Cognitive impairment in early stages of multiple sclerosis. Neurol. Sci. 2010, 31, 211–214. [Google Scholar] [CrossRef] [PubMed]
- da Silva, A.M.; Cavaco, S.; Moreira, I.; Bettencourt, A.; Santos, E.; Pinto, C.; Gonçalves, A.; Coutinho, M.E.; Samões, R.; Dias, C.C.; et al. Cognitive reserve in multiple sclerosis: Protective effects of education. Mult. Scler. J. 2015, 21, 1312–1321. [Google Scholar] [CrossRef] [PubMed]
- Karadayi, H.; Arisoy, O.; Altunrende, B.; Boztaş, M.H.; Sercan, M. The relationship of cognitive impairment with neurological and psychiatric variables in multiple sclerosis patients. Int. J. Psychiatry Clin. Pract. 2014, 18, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Hänninen, K.; Viitala, M.; Paavilainen, T.; Karhu, J.O.; Rinne, J.; Koikkalainen, J.; Lötjönen, J.; Soilu-Hänninen, M. Thalamic Atrophy Predicts 5-Year Disability Progression in Multiple Sclerosis. Front. Neurol. 2020, 11, 606. [Google Scholar] [CrossRef] [PubMed]
- Tovar-Moll, F.; Evangelou, I.; Chiu, A.; Richert, N.; Ostuni, J.; Ohayon, J.; Auh, S.; Ehrmantraut, M.; Talagala, S.; McFarland, H.; et al. Thalamic Involvement and Its Impact on Clinical Disability in Patients with Multiple Sclerosis: A Diffusion Tensor Imaging Study at 3T. Am. J. Neuroradiol. 2009, 30, 1380–1386. [Google Scholar] [CrossRef] [PubMed]
- Stuke, H.; Hanken, K.; Hirsch, J.; Klein, J.; Wittig, F.; Kastrup, A.; Hildebrandt, H. Cross-Sectional and Longitudinal Relationships between Depressive Symptoms and Brain Atrophy in MS Patients. Front. Hum. Neurosci. 2016, 10, 622. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Bakshi, R.; Simon, J.H.; Priore, R.; Miller, C.; Munschauer, F. Frontal cortex atrophy predicts cognitive impairment in multiple sclerosis. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 44–51. [Google Scholar] [CrossRef]
- Bernitsas, E.; Yarraguntla, K.; Bao, F.; Sood, R.; Santiago-Martinez, C.; Govindan, R.; Khan, O.; Seraji-Bozorgzad, N. Structural and Neuronal Integrity Measures of Fatigue Severity in Multiple Sclerosis. Brain Sci. 2017, 7, 102. [Google Scholar] [CrossRef]
- Voskuhl, R.R.; Patel, K.; Paul, F.; Gold, S.M.; Scheel, M.; Kuchling, J.; Cooper, G.; Asseyer, S.; Chien, C.; Brandt, A.U.; et al. Sex differences in brain atrophy in multiple sclerosis. Biol. Sex Differ. 2020, 11, 49. [Google Scholar] [CrossRef]
- Müller, M.; Esser, R.; Kötter, K.; Voss, J.; Müller, A.; Stellmes, P. Third ventricular enlargement in early stages of multiple sclerosis is a predictor of motor and neuropsychological deficits: A cross-sectional study. BMJ Open 2013, 3, e003582. [Google Scholar] [CrossRef]
- Turner, B.; Ramli, N.; Blumhardt, L.D.; Jaspan, T. Ventricular enlargement in multiple sclerosis: A comparison of three-dimensional and linear MRI estimates. Neuroradiology 2001, 43, 608–614. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | MS Group n = 93 | HPs Group n = 150 | p |
|---|---|---|---|
| Age (years) | 0.02 | ||
| median (25–75th percentiles) | 41 (33–50) | 37 (29–48) | |
| range | 20–67 | 18–64 | |
| Female-to-male ratio | 67:26 | 109:41 | 0.97 |
| Education (years) | 0.11 | ||
| median (25–75th percentiles) | 13 (12–17) | 15 (12–17) | |
| range | 8–18 | 8–21 | |
| Disease duration (years) | |||
| median (25–75th percentiles) | 9 (4–16) | ||
| range | 0.1–44 | ||
| Disease course, n (%) | |||
| RRMS | 60 (64.5) | ||
| SPMS | 25 (26.9) | ||
| PPMS | 8 (8.60) | ||
| EDSS | |||
| median (25–75th percentiles) | 3.0 (2.0–4.0) | ||
| range | 1.0–7.5 |
| MS Group | HPs Group | Cohen’s d | p | |
|---|---|---|---|---|
| SDMT, median | 41 | 49 | 0.64 | <0.0001 |
| (25–75th percentiles) | (31–50) | (42–55) | ||
| CVLT, mean ± SD | 49.9 ± 11.5 | 54.1 ± 10.3 | 0.39 | 0.003 |
| BVMT-R, median | 24 | 29 | 0.48 | 0.003 |
| (25–75th percentiles) | (18–30) | (24–32) |
| F = 31.34; SE = 0.53; Corrected R2 = 0.63; p < 0.000001 | ||||
|---|---|---|---|---|
| β | SE_β | t | p | |
| age | −0.32 | 0.08 | −4.20 | 0.00006 |
| 3VW | −0.31 | 0.07 | −4.24 | 0.00006 |
| education | 0.23 | 0.07 | 3.19 | 0.002 |
| EDSS | −0.21 | 0.08 | −2.70 | 0.008 |
| MFIS | −0.16 | 0.07 | −2.18 | 0.03 |
| F = 12.21; SE = 1.42; Corrected R2 = 0.27; p < 0.000001 | ||||
|---|---|---|---|---|
| β | SE_β | t | p | |
| age | 0.26 | 0.11 | 2.34 | 0.02 |
| duration of the disease | 0.24 | 0.11 | 2.25 | 0.03 |
| 3VW | 0.22 | 0.09 | 2.29 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guenter, W.; Betscher, E.; Bonek, R. Predictive Value of the Third Ventricle Width for Neurological Status in Multiple Sclerosis. J. Clin. Med. 2022, 11, 2841. https://doi.org/10.3390/jcm11102841
Guenter W, Betscher E, Bonek R. Predictive Value of the Third Ventricle Width for Neurological Status in Multiple Sclerosis. Journal of Clinical Medicine. 2022; 11(10):2841. https://doi.org/10.3390/jcm11102841
Chicago/Turabian StyleGuenter, Wojciech, Ewa Betscher, and Robert Bonek. 2022. "Predictive Value of the Third Ventricle Width for Neurological Status in Multiple Sclerosis" Journal of Clinical Medicine 11, no. 10: 2841. https://doi.org/10.3390/jcm11102841
APA StyleGuenter, W., Betscher, E., & Bonek, R. (2022). Predictive Value of the Third Ventricle Width for Neurological Status in Multiple Sclerosis. Journal of Clinical Medicine, 11(10), 2841. https://doi.org/10.3390/jcm11102841