
Outcome after Thrombectomy of Acute M1 and Carotid-T Occlusions with Involvement of the Corticospinal Tract in Postinterventional Imaging

 , ,
, ,
Abstract
:1. Introduction
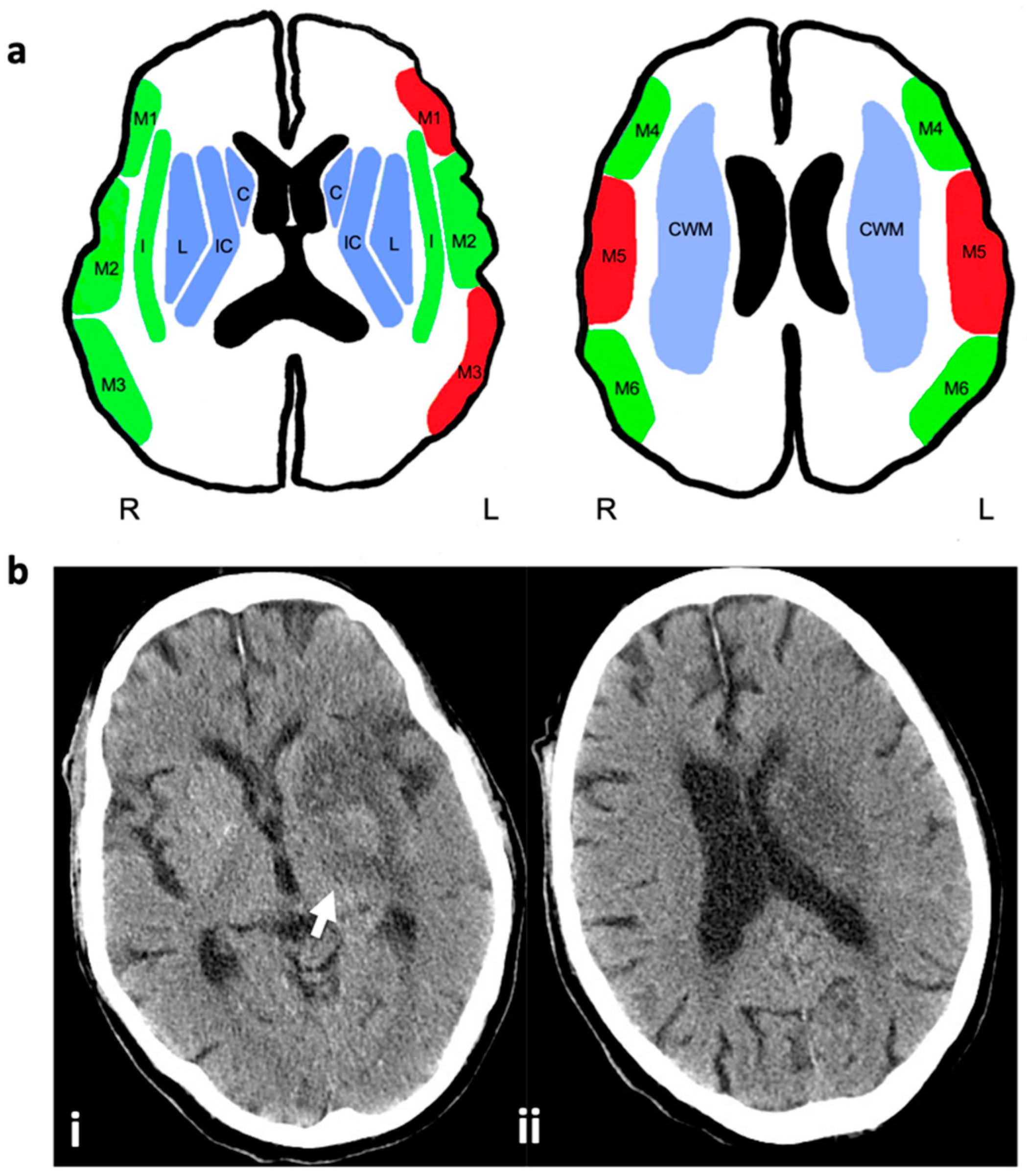
2. Materials and Methods
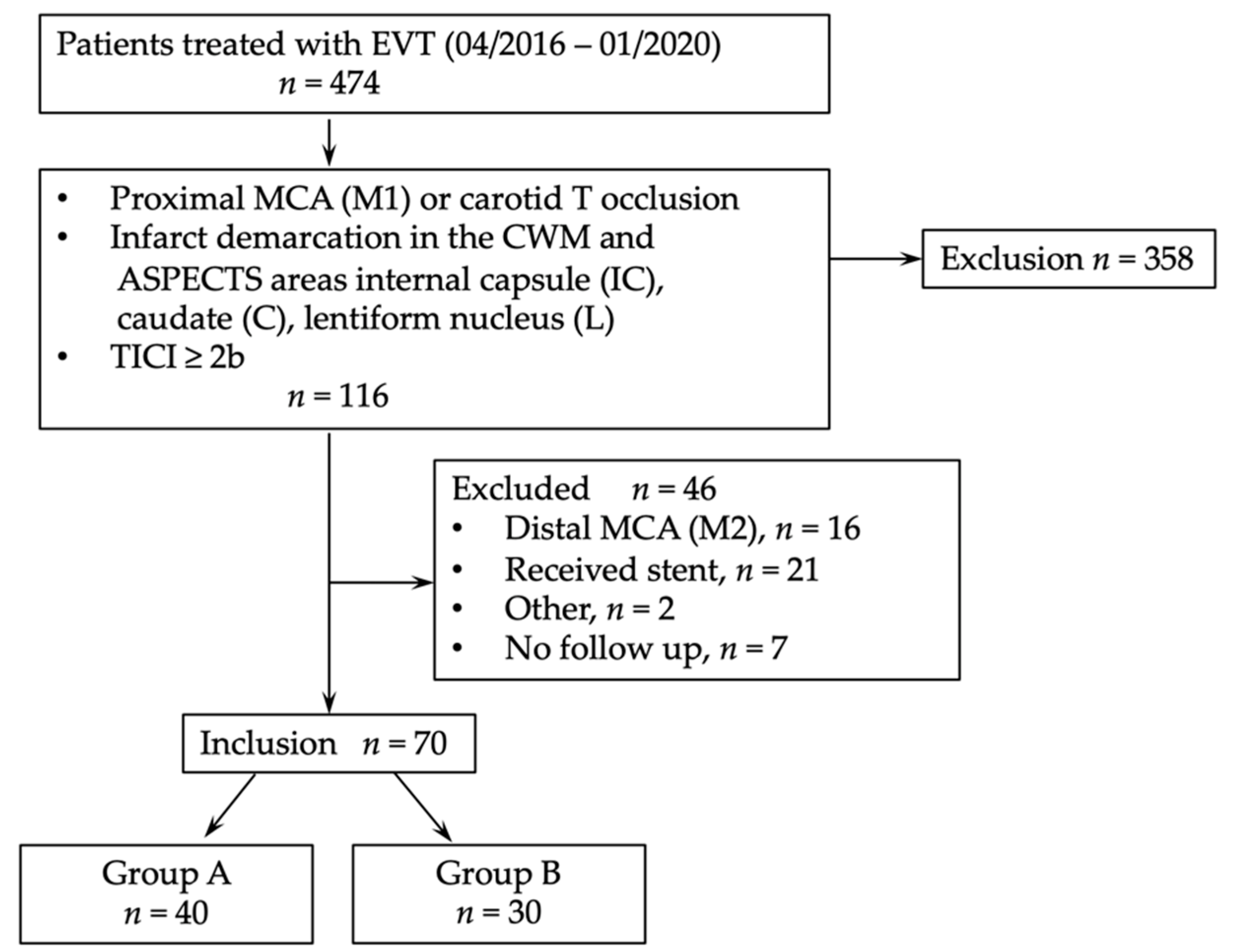
2.1. Study Design
2.2. Statistical Analysis
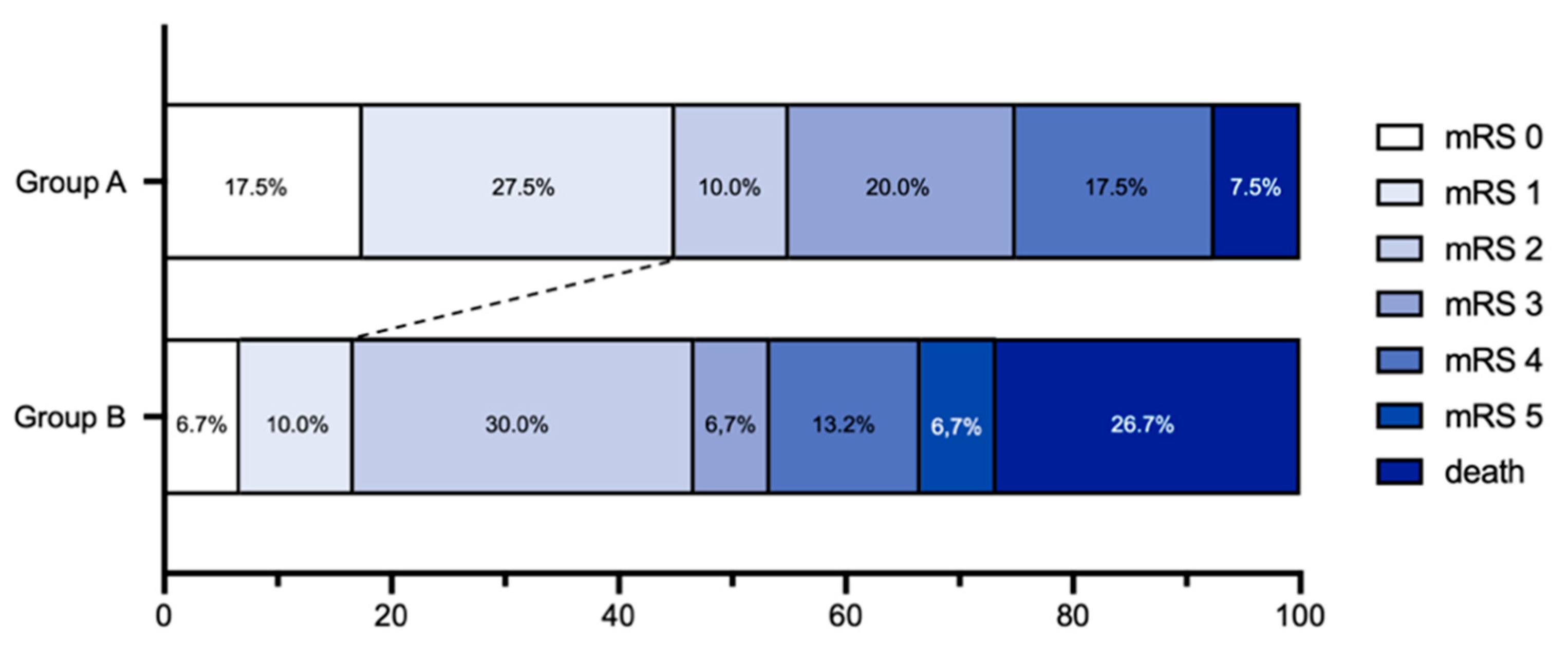
3. Results
3.1. Impacts of Cortical Lesions
3.2. ASPECTS Score
3.3. Safety Outcome
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Dippel, D.W.; Majoie, C.B.; Roos, Y.B.; van der Lugt, A.; van Oostenbrugge, R.J.; van Zwam, W.H.; Lingsma, H.F.; Koudstaal, P.J.; Treurniet, K.M.; van den Berg, L.A.; et al. Influence of Device Choice on the Effect of Intra-Arterial Treatment for Acute Ischemic Stroke in MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands). Stroke 2016, 47, 2574–2581. [Google Scholar] [CrossRef] [Green Version]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [Green Version]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; San Román, L.; Serena, J.; Abilleira, S.; Ribó, M.; et al. Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef] [Green Version]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.-C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-Retriever Thrombectomy after Intravenous t-PA vs. t-PA Alone in Stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.V.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular Therapy for Ischemic Stroke with Perfusion-Imaging Selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [Green Version]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and Reliability of a Quantitative Computed Tomography Score in Predicting Outcome of Hyperacute Stroke before Thrombolytic Therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef]
- Prabhakaran, S.; Zarahn, E.; Riley, C.; Speizer, A.; Chong, J.Y.; Lazar, R.M.; Marshall, R.S.; Krakauer, J.W. Inter-Individual Variability in the Capacity for Motor Recovery after Ischemic Stroke. Neurorehabil. Neural Repair 2008, 22, 64–71. [Google Scholar] [CrossRef]
- Román, L.S.; Menon, B.K.; Blasco, J.; Hernández-Pérez, M.; Dávalos, A.; Majoie, C.B.L.M.; Campbell, B.C.V.; Guillemin, F.; Lingsma, H.; Anxionnat, R.; et al. Imaging Features and Safety and Efficacy of Endovascular Stroke Treatment: A Meta-Analysis of Individual Patient-Level Data. Lancet Neurol. 2018, 17, 895–904. [Google Scholar] [CrossRef] [Green Version]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Berndt, M.T.; Pürner, D.; Maegerlein, C.; Wunderlich, S.; Friedrich, B.; Zimmer, C.; Sepp, D.; Kaesmacher, J.; Boeckh-Behrens, T. Basal Ganglia versus Peripheral Infarcts: Predictive Value of Early Fiber Alterations. AJNR Am. J. Neuroradiol. 2021, 42, 264–270. [Google Scholar] [CrossRef]
- Kleine, J.F.; Kaesmacher, M.; Wiestler, B.; Kaesmacher, J. Tissue-Selective Salvage of the White Matter by Successful Endovascular Stroke Therapy. Stroke 2017, 48, 2776–2783. [Google Scholar] [CrossRef]
- Almekhlafi, M.A.; Hill, M.D.; Roos, Y.M.; Campbell, B.C.V.; Muir, K.W.; Demchuk, A.M.; Bracard, S.; Gomis, M.; Guillemin, F.; Jovin, T.G.; et al. Stroke Laterality Did Not Modify Outcomes in the HERMES Meta-Analysis of Individual Patient Data of 7 Trials. Stroke 2019, 50, 2118–2124. [Google Scholar] [CrossRef]
- Laredo, C.; Zhao, Y.; Rudilosso, S.; Renú, A.; Pariente, J.C.; Chamorro, Á.; Urra, X. Prognostic Significance of Infarct Size and Location: The Case of Insular Stroke. Sci. Rep. 2018, 8, 9498. [Google Scholar] [CrossRef]
- Baek, B.H.; Yoon, W.; Lee, Y.Y.; Park, I.; Kim, S.K. Impact of Isolated Basal Ganglia Infarction at Pretreatment DWI on Outcomes after Endovascular Thrombectomy in Acute Anterior Circulation Stroke. Neuroradiology 2019, 61, 89–96. [Google Scholar] [CrossRef]
- Boers, A.M.M.; Jansen, I.G.H.; Beenen, L.F.M.; Devlin, T.G.; San Roman, L.; Heo, J.H.; Ribó, M.; Brown, S.; Almekhlafi, M.A.; Liebeskind, D.S.; et al. Association of Follow-up Infarct Volume with Functional Outcome in Acute Ischemic Stroke: A Pooled Analysis of Seven Randomized Trials. J. Neurointerv. Surg 2018, 10, 1137–1142. [Google Scholar] [CrossRef] [Green Version]
- Zaidat, O.O.; Yoo, A.J.; Khatri, P.; Tomsick, T.A.; von Kummer, R.; Saver, J.L.; Marks, M.P.; Prabhakaran, S.; Kallmes, D.F.; Fitzsimmons, B.-F.M.; et al. Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke: A Consensus Statement. Stroke 2013, 44, 2650–2663. [Google Scholar] [CrossRef] [Green Version]
- Von Kummer, R.; Broderick, J.P.; Campbell, B.C.V.; Demchuk, A.; Goyal, M.; Hill, M.D.; Treurniet, K.M.; Majoie, C.B.L.M.; Marquering, H.A.; Mazya, M.V.; et al. The Heidelberg Bleeding Classification: Classification of Bleeding Events After Ischemic Stroke and Reperfusion Therapy. Stroke 2015, 46, 2981–2986. [Google Scholar] [CrossRef] [Green Version]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular Thrombectomy after Large-Vessel Ischaemic Stroke: A Meta-Analysis of Individual Patient Data from Five Randomised Trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Fuhrer, H.; Forner, L.; Pruellage, P.; Weber, S.; Beume, L.-A.; Schacht, H.; Egger, K.; Bardutzky, J.; Weiller, C.; Urbach, H.; et al. Long-Term Outcome Changes after Mechanical Thrombectomy for Anterior Circulation Acute Ischemic Stroke. J. Neurol. 2020, 267, 1026–1034. [Google Scholar] [CrossRef]
- Golsari, A.; Cheng, B.; Sobesky, J.; Schellinger, P.D.; Fiehler, J.; Gerloff, C.; Thomalla, G. Stroke Lesion Volumes and Outcome Are Not Different in Hemispheric Stroke Side Treated with Intravenous Thrombolysis Based on Magnetic Resonance Imaging Criteria. Stroke 2015, 46, 1004–1008. [Google Scholar] [CrossRef] [Green Version]
- Ospel, J.M.; Menon, B.K.; Qiu, W.; Kashani, N.; Mayank, A.; Singh, N.; Cimflova, P.; Marko, M.; Nogueira, R.G.; McTaggart, R.A.; et al. A Detailed Analysis of Infarct Patterns and Volumes at 24-Hour Noncontrast CT and Diffusion-Weighted MRI in Acute Ischemic Stroke Due to Large Vessel Occlusion: Results from the ESCAPE-NA1 Trial. Radiology 2021, 300, 152–159. [Google Scholar] [CrossRef]
- Khan, M.; Baird, G.L.; Goddeau, R.P.; Silver, B.; Henninger, N. Alberta Stroke Program Early CT Score Infarct Location Predicts Outcome Following M2 Occlusion. Front. Neurol 2017, 8, 98. [Google Scholar] [CrossRef] [Green Version]
- Sampaio-Baptista, C.; Johansen-Berg, H. White Matter Plasticity in the Adult Brain. Neuron 2017, 96, 1239–1251. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, B.; Lobsien, D.; Maegerlein, C.; Wunderlich, S.; Zimmer, C.; Kaesmacher, J.; Kleine, J. Distance to Thrombus in Acute Middle Cerebral Artery Stroke Predicts Basal Ganglia Infarction after Mechanical Thrombectomy. Oncotarget 2016, 7, 85813–85818. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.L.; Lindenberg, R.; Alexander, M.P.; Schlaug, G. Lesion Load of the Corticospinal Tract Predicts Motor Impairment in Chronic Stroke. Stroke 2010, 41, 910–915. [Google Scholar] [CrossRef] [Green Version]
- Heit, J.J.; Sussman, E.S.; Wintermark, M. Perfusion Computed Tomography in Acute Ischemic Stroke. Radiol. Clin. N. Am. 2019, 57, 1109–1116. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Seymour, J.; Cairns, J.; Keir, S.; Lewis, S.; Sandercock, P. Immediate Computed Tomography Scanning of Acute Stroke Is Cost-Effective and Improves Quality of Life. Stroke 2004, 35, 2477–2483. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.V.; Majoie, C.B.L.M.; Albers, G.W.; Menon, B.K.; Yassi, N.; Sharma, G.; van Zwam, W.H.; van Oostenbrugge, R.J.; Demchuk, A.M.; Guillemin, F.; et al. Penumbral Imaging and Functional Outcome in Patients with Anterior Circulation Ischaemic Stroke Treated with Endovascular Thrombectomy versus Medical Therapy: A Meta-Analysis of Individual Patient-Level Data. Lancet Neurol. 2019, 18, 46–55. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| n (%) Overall | n (%) Group A | n (%) Group B | p-Value | |
|---|---|---|---|---|
| n = 70 | n = 40 | n = 30 | ||
| Age (y; mean ± SD) | 71.8 ± 13.20 | 71.4 ± 13.81 | 72.4 ± 12.54 | |
| Male | 32 (45.7) | 17 (42.5) | 15 (50.0) | 0.533 |
| Secondary transferred to EVT | 33 (47.1) | 20 (50.0) | 13 (43.3) | 0.580 |
| IVT | 43 (61.4) | 27 (67.5) | 16 (53.3) | 0.228 |
| Length of stay (d; mean ± SD) | 11.7 ± 8.69 | 12.5 ± 10.07 | 10.7 ± 6.46 | 0.592 |
| NIHSS baseline (median, IQR) | 14 (10–18) | 11.5 (9–17) | 16 (12–19) | 0.005 |
| mRS baseline (median, IQR) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 0.222 |
| Living status prior stroke | ||||
| Home | 63 (90.0) | 37 (92.5) | 26 (86.7) | 0.420 |
| Nursing at home | 1 (1.4) | 0 (0) | 1 (3.3) | 0.245 |
| Nursing home | 6 (8.6) | 3 (7.5) | 3 (10.0) | 0.712 |
| Risk factors | ||||
| Smoking | 10 (14.3) | 6 (15.0) | 4 (13.3) | 0.844 |
| Hypertension | 55 (78.6) | 30 (75.0) | 25 (83.3) | 0.400 |
| Dyslipidemia | 9 (12.9) | 4 (10.0) | 5 (16.7) | 0.410 |
| Diabetes | 11 (15.7) | 6 (15.0) | 5 (16.7) | 0.850 |
| Atrial fibrillation | 44 (62.9) | 28 (70.0) | 16 (53.3) | 0.153 |
| TOAST | ||||
| Large-artery atheroslerosis | 6 (8.6) | 2 (5.0) | 4 (13.4) | 0.218 |
| Cardioembolism | 46 (65.7) | 28 (70.0) | 18 (60.0) | 0.383 |
| Other | 18 (25.7) | 10 (25.0) | 8 (26.6) | 0.776 |
| Occlusion Side Left | 37 (52.9) | 18 (45.0) | 19 (63.3) | 0.128 |
| Occlusion localisation | ||||
| M1 | 58 (82.9) | 32 (80.0) | 26 (86.7) | 0.464 |
| Carotid-T | 12 (17.1) | 8 (20.0) | 4 (13.3) | 0.464 |
| TICI | ||||
| 2b | 34 (48.6) | 19 (47.5) | 15 (50.0) | 0.856 |
| 2c | 7 (10.0) | 3 (7.5) | 4 (13.3) | 0.421 |
| 3 | 29 (41.4) | 18 (45.0) | 11 (36.7) | 0.484 |
| Symptom onset to endovascular reperfusion (h; mean ± SD) | 10.9 ± 39.71 | 6.2 ± 4.00 | 17.3 ± 60.84 | 0.586 |
| Groin puncture to endovascular reperfusion (h; mean ± SD) | 0.8 ± 0.48 | 0.8 ± 0.48 | 0.8 ± 0.48 | 0.826 |
| n (%) Overall | n (%) Group A | n (%) Group B | p-Value | |
|---|---|---|---|---|
| n = 70 | n = 40 | n = 30 | ||
| Living status discharge | ||||
| Home | 21 (30.0) | 14 (35.0) | 7 (23.3) | 0.113 |
| Rehab | 35 (50.0) | 20 (50) | 15 (50.0) | 1.000 |
| Nursing home | 1 (1.4) | 1 (2.5) | 0 (0) | 0.383 |
| Hospital | 6 (8.6) | 2 (5.0) | 4 (13.3) | 0.218 |
| Dead | 7 (10) | 3 (7.5) | 4 (13.3) | 0.421 |
| Living status 90 d FU | ||||
| Home | 41 (58.6) | 24 (60.0) | 17 (56.7) | 0.779 |
| Nursing at home | 6 (8.6) | 4 (10.0) | 2 (6.65) | 0.622 |
| Nursing home | 5 (7.1) | 4 (10.0) | 1 (3.3) | 0.284 |
| Rehab | 5 (7.1) | 3 (7.5) | 2 (6.65) | 0.893 |
| Hospital | 2 (2.9) | 2 (5.0) | 0 (0) | 0.214 |
| Dead | 11 (15.7) | 3 (7.5) | 8 (26.7) | 0.029 |
| NIHSS (median, IQR) | ||||
| After 24 h | 8 (3–15) | 4.5 (3–10) | 13 (7–21) | 0.001 |
| At discharge | 2 (0–8) | 1 (0–5) | 5.5 (2–12) | 0.002 |
| mRS (median, IQR) | ||||
| At discharge | 2.5 (1–4) | 1.5 (1–4) | 4 (2–5) | 0.013 |
| After 90 d | 2 (1–4) | 2 (1–4) | 3 (2–6) | 0.021 |
| mRS outcome after 90 d | ||||
| Good outcome (mRS 0–2) | 36 (51.4) | 22 (55.0) | 14 (46.7) | 0.581 |
| Excellent outcome (mRS 0–1) | 23 (32.9) | 18 (45.0) | 5 (16.7) | 0.013 |
| Symptomatic intracranial haemorrhage | 3 (4.3) | 0 (0) | 3 (10.0) | 0.052 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reitz, S.C.; Gerhard, E.; Breuer, S.; Bohmann, F.O.; Pfeilschifter, W.; Berkefeld, J. Outcome after Thrombectomy of Acute M1 and Carotid-T Occlusions with Involvement of the Corticospinal Tract in Postinterventional Imaging. J. Clin. Med. 2022, 11, 2823. https://doi.org/10.3390/jcm11102823
Reitz SC, Gerhard E, Breuer S, Bohmann FO, Pfeilschifter W, Berkefeld J. Outcome after Thrombectomy of Acute M1 and Carotid-T Occlusions with Involvement of the Corticospinal Tract in Postinterventional Imaging. Journal of Clinical Medicine. 2022; 11(10):2823. https://doi.org/10.3390/jcm11102823
Chicago/Turabian StyleReitz, Sarah Christina, Ellen Gerhard, Stella Breuer, Ferdinand Oliver Bohmann, Waltraud Pfeilschifter, and Joachim Berkefeld. 2022. "Outcome after Thrombectomy of Acute M1 and Carotid-T Occlusions with Involvement of the Corticospinal Tract in Postinterventional Imaging" Journal of Clinical Medicine 11, no. 10: 2823. https://doi.org/10.3390/jcm11102823
APA StyleReitz, S. C., Gerhard, E., Breuer, S., Bohmann, F. O., Pfeilschifter, W., & Berkefeld, J. (2022). Outcome after Thrombectomy of Acute M1 and Carotid-T Occlusions with Involvement of the Corticospinal Tract in Postinterventional Imaging. Journal of Clinical Medicine, 11(10), 2823. https://doi.org/10.3390/jcm11102823