
Kinematic Parameters Following Pilon Fracture Treatment with the Ilizarov Method

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
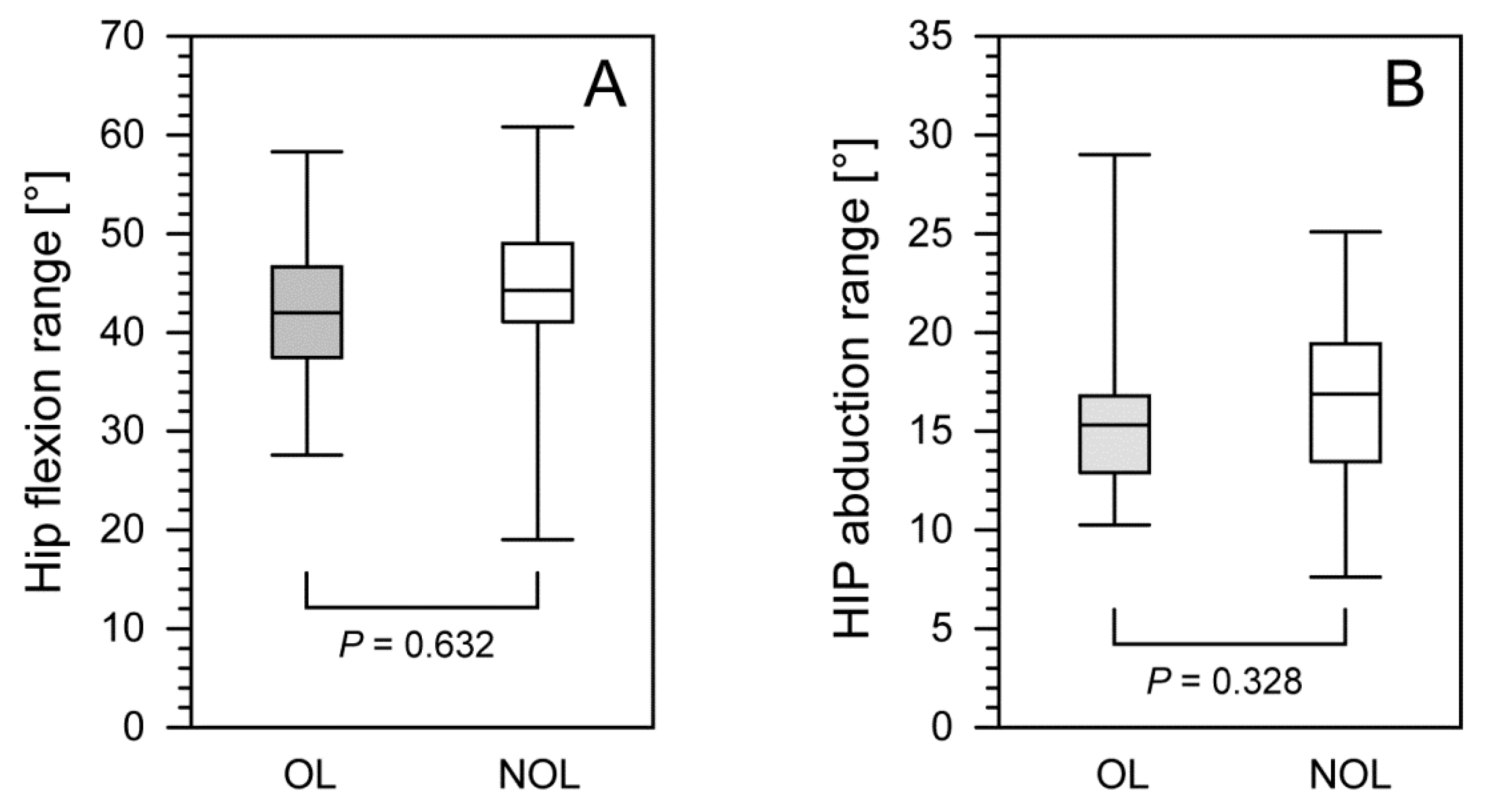
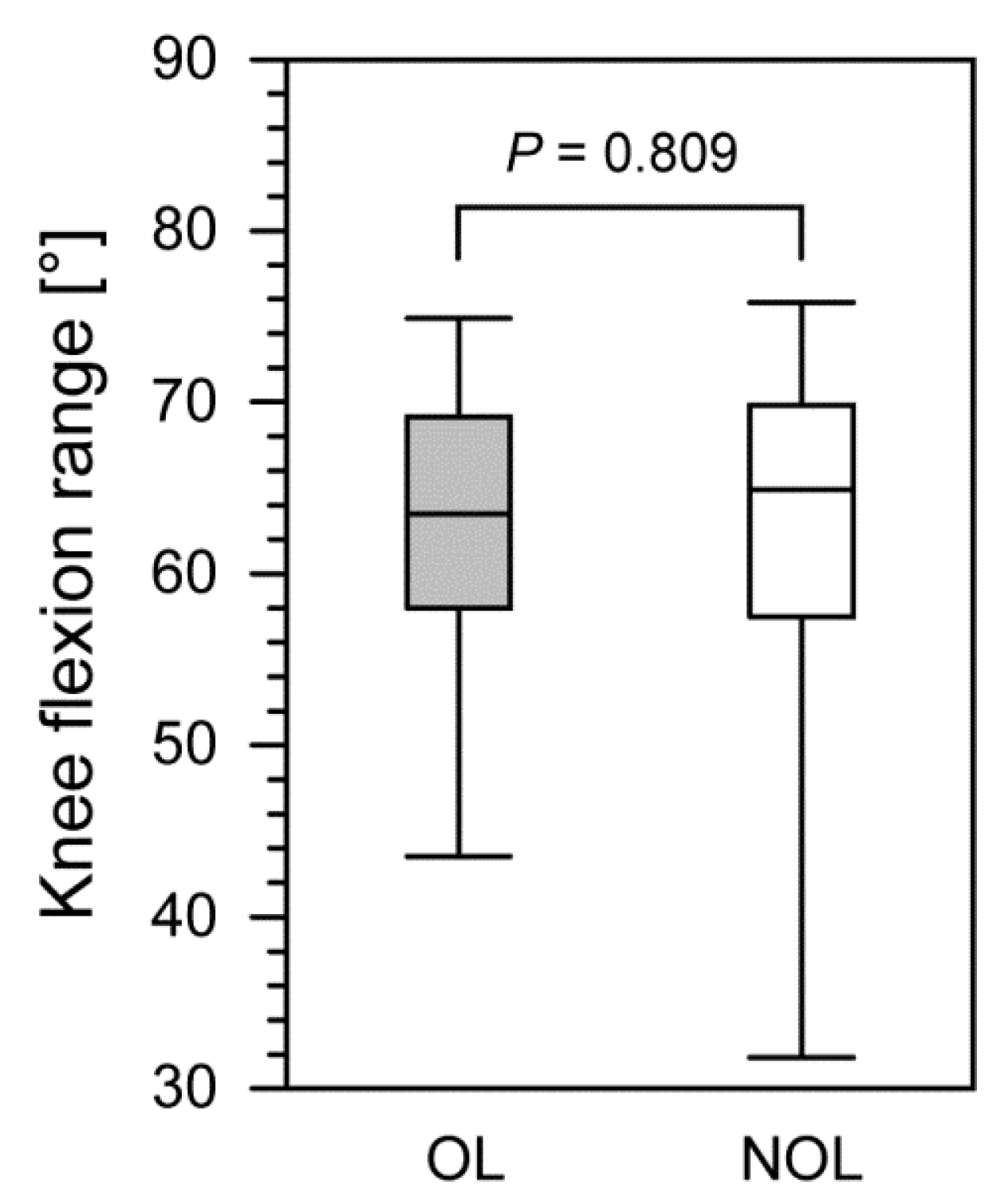
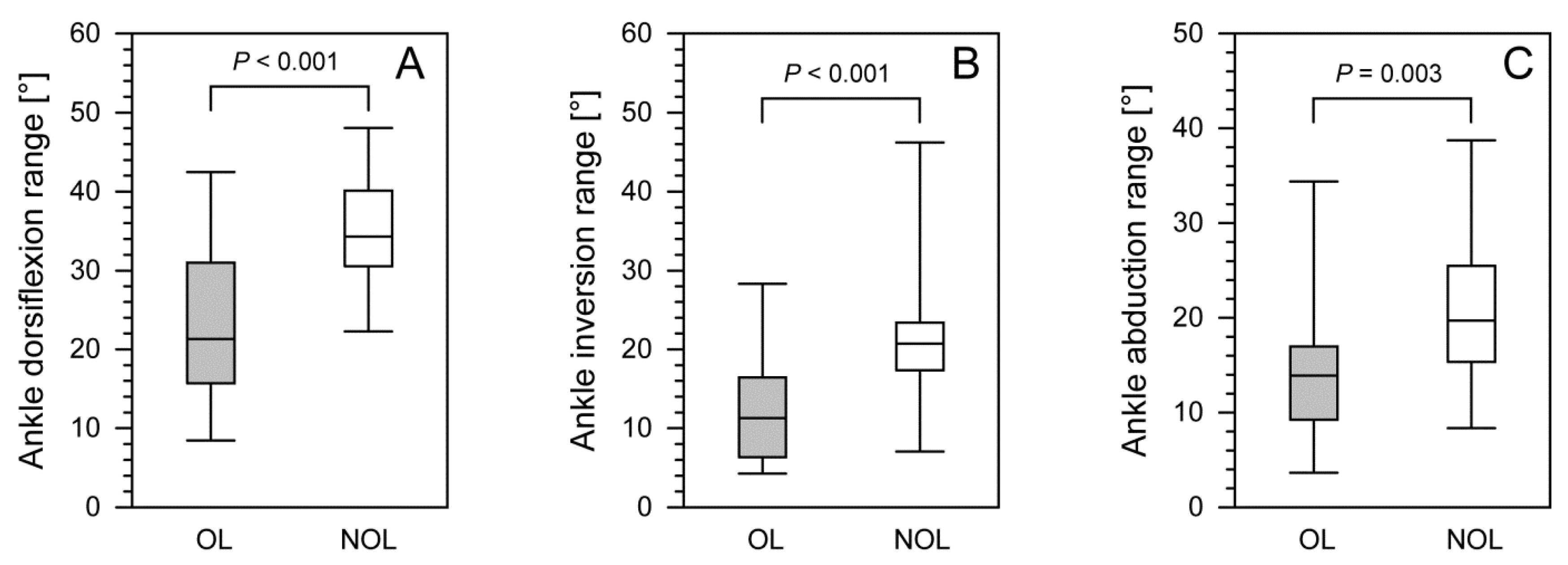
- Following pilon fracture treatment with the Ilizarov method, we observed no differences in terms of knee or hip joint mobility between the OL and the NOL, whereas the range of motion in the ankle joint of the OL was significantly limited.
- The treatment of pilon fractures with the Ilizarov method does not ensure the complete normalization of ankle joint kinematic parameters. Therefore, intense personalized rehabilitation of the ankle joint is recommended.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papadokostakis, G.; Kontakis, G.; Giannoudis, P.; Hadjipavlou, A. External fixation devices in the treatment of fractures of the tibial plafond: A systematic review of the literature. J. Bone Joint Surg. Br. 2008, 90, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Villaseñor, L.E.V.; Leyva, M.A.O.; Flores, R.R.; López, J.L.H. Clinical outcome of a bilateral tibial pylon fracture treated with a minimally invasive technique. Acta Ortop. Mex. 2009, 23, 163–166. [Google Scholar]
- Okcu, G.; Aktuglu, K. Intra-articular fractures of the tibial plafond. A comparison of the results using articulated and ring external fixators. J. Bone Joint Surg. Br. 2004, 86, 868–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Balderas, A.; Beltrán-Cota, E.R.; Ruiz-Barrios, J.M.; Caldera-Barbosa, O. Results of the treatment of high energy tibial pylon fractures. Acta Ortop Mex. 2013, 27, 363–366. [Google Scholar]
- Závitkovský, P.; Malkus, T. Fractures of the tibial pylon: Treatment options and outcomes. Acta Chir. Orthop. Traumatol. Cech. 2004, 71, 228–236. [Google Scholar]
- Aktuğlu, K.; Ozsoy, M.H.; Yensel, U. Treatment of displaced pylon fractures with circular external fixators of Ilizarov. Foot Ankle Int. 1998, 19, 208–216. [Google Scholar] [CrossRef]
- Bastian, L.; Blauth, M.; Thermann, H.; Tscherne, H. Various therapy concepts in severe fractures of the tibial pilon (type C injuries). A comparative study. Unfallchirurg 1995, 98, 551–558. [Google Scholar]
- Zheng, Y.; Zhang, J.-D.; Shen, J.-M.; Chen, J.-J.; Toy, L.; Huang, F.-J. A Modified 2-Stage Treatment for AO/OTA 43-C1 Pilon Fractures Accompanied by Distal Fibular and Posterior Lip of the Distal Tibia Fracture. J. Foot Ankle Surg. 2020, 59, 972–978. [Google Scholar] [CrossRef]
- Campbell, S.T.; Goodnough, L.H.; Salazar, B.; Lucas, J.F.; Bishop, J.A.; Gardner, M.J. How do pilon fractures heal? An analysis of dual plating and bridging callus formation. Injury 2020, 51, 1655–1661. [Google Scholar] [CrossRef]
- Malik-Tabassum, K.; Pillai, K.; Hussain, Y.; Bleibleh, S.; Babu, S.; Giannoudis, P.V.; Tosounidis, T.H. Post-operative outcomes of open reduction and internal fixation versus circular external fixation in treatment of tibial plafond fractures: A systematic review and meta-analysis. Injury 2020, 51, 1448–1456. [Google Scholar] [CrossRef]
- Falzarano, G.; Pica, G.; Medici, A.; Rollo, G.; Bisaccia, M.; Cioffi, R.; Pavone, M.; Meccariello, L. Foot Loading and Gait Analysis Evaluation of Nonarticular Tibial Pilon Fracture: A Comparison of Three Surgical Techniques. J. Foot Ankle Surg. 2018, 57, 894–898. [Google Scholar] [CrossRef] [PubMed]
- Jansen, H.; Fenwick, A.; Doht, S.; Frey, S.; Meffert, R. Clinical outcome and changes in gait pattern after pilon fractures. Int. Orthop. 2013, 37, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morasiewicz, P.; Konieczny, G.; Dejnek, M.; Urbański, W.; Dragan, S.Ł.; Kulej, M.; Pawik, Ł. Assessment of the distribution of load on the lower limbs and balance before and after ankle arthrodesis with the Ilizarov method. Sci. Rep. 2018, 8, 15693. [Google Scholar] [CrossRef] [PubMed]
- Pawik, Ł.; Wietecki, P.; Leśkow, A.; Pajchert Kozłowska, A.; Żarek, S.; Górski, R.; Pawik, M.; Fink-Lwow, F.; Urbański, W.; Morasiewicz, P. Gait Symmetry Analysis in Patients after Treatment of Pilon Fractures by the Ilizarov Method. Symmetry 2021, 13, 349. [Google Scholar] [CrossRef]
- Veilleux, L.N.; Robert, M.; Ballaz, L.; Lemay, M.; Rauch, F. Gait analysis using a force-measuring gangway: Intrasession repeatability in healthy adults. J. Musculoskelet. Neuronal Interact. 2011, 11, 27–33. [Google Scholar] [PubMed]
- Bhave, A.; Paley, D.; Herzenberg, J.E. Improvement in gait parameters after lengthening for the treatment of limb-length discrepancy. J. Bone Jt. Surg. Ser. A. 1999, 81, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Morasiewicz, M.; Koprowski, P.; Wrzosek, Z.; Dragan, S. Gait analysis in patients after lengthening and correction of tibia with Ilizarov technique. Physiotheraphy 2010, 18, 9–18. [Google Scholar] [CrossRef]
- Saraph, V.; Zwick, E.B.; Steinwender, G.; Auner, C.; Schneider, F.; Linhart, W. Leg lengthening as part of gait improvement surgery in cerebral palsy: An evaluation using gait analysis. Gait Posture 2006, 23, 83–90. [Google Scholar] [CrossRef]
- Manjra, M.A.; Naude, J.; Birkholtz, F.; Glatt, V.; Tetsworth, K.; Hohmann, E. The relationship between gait and functional outcomes in patients treated with circular external fixation for malunited tibial fractures. Gait Posture 2019, 68, 569–574. [Google Scholar] [CrossRef]
- Koczewski, P.; Urban, F.; Jóźwiak, M. Analysis of some gait parameters at different stages of leg lengthening using the Ilizarov technique. Chir. Narzadow Ruchu Ortop. Pol. 2004, 69, 393–397. [Google Scholar]
- Vidyadhara, S.; Rao, S.K. Ilizarov treatment of complex tibial pilon fractures. Int. Orthop. 2006, 30, 113–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osman, W.; Alaya, Z.; Kaziz, H.; Hassini, L.; Braiki, M.; Naouar, N.; Laaziz, M.; Ayeche, B. Treatment of high-energy pilon fractures using the ilizarov treatment. Pan. Afr. Med. J. 2017, 27, 199. [Google Scholar] [CrossRef] [PubMed]
- Fırat, A.; Tecimel, O.; Işık, C.; Ozdemir, M.; Oçgüder, A.; Bozkurt, M. Ilizarov external fixator in the management of tibial pilon fractures: Ankle hinged vs ankle fixed frame. Eklem Hastalik. Cerrahisi 2013, 24, 133–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos, T.; Karlsson, J.; Eriksson, B.I.; Nistor, L. Treatment of distal tibial fractures with the Ilizarov external fixator—A prospective observational study in 39 consecutive patients. BMC Musculoskelet. Disord. 2013, 14, 30. [Google Scholar] [CrossRef] [Green Version]
- Bańkosz, Z.; Winiarski, S.; Lanzoni, I.M. Gender differences in kinematic parameters of topspin forehand and backhand in table tennis. Int. J. Environ. Res. Public Health 2020, 17, 5742. [Google Scholar] [CrossRef]
- Bańkosz, Z.; Winiarski, S. Kinematic parameters of topspin forehand in table tennis and their inter-and intra-individual variability. J. Sport Sci. Med. 2020, 19, 138–148. [Google Scholar]
- Struzik, A.; Konieczny, G.; Grzesik, K.; Stawarz, M.; Winiarski, S.; Rokita, A. Relationship between lower limbs kinematic variables and effectiveness of sprint during maximum velocity phase. Acta Bioeng. Biomech. 2015, 17, 131–138. [Google Scholar] [CrossRef]
- Struzik, A.; Konieczny, G.; Stawarz, M.; Grzesik, K.; Winiarski, S.; Rokita, A. Relationship between Lower Limb Angular Kinematic Variables and the Effectiveness of Sprinting during the Acceleration Phase. Appl. Bionics Biomech. 2016, 2016, 748070. [Google Scholar] [CrossRef] [Green Version]
- Cichy, B.; Wilk, M. Gait analysis in osteoarthritis of the hip. Med. Sci. Monit. 2006, 12, 507–513. [Google Scholar]
- Shrader, M.W.; Draganich, L.F.; Pottenger, L.A.; Piotrowski, G.A. Effects of knee pain relief in osteoarthritis on gait and stair-stepping. Clin. Orthop. Relat. Res. 2004, 421, 188–193. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients after Surgery (n = 23) | |
|---|---|
| Minimum hip flexion, OL [°] | −12.4 [(−23.80)–(−4.0)] |
| Minimum hip flexion, NOL [°] | −13.3 [(−19.70)–(−2.8)] |
| p-value | 0.911 |
| Maximum hip flexion, OL [°] | 29.7 (21.3–40.9) |
| Maximum hip flexion, NOL [°] | 31.6 (10.8–46.7) |
| p-value | 0.551 |
| Hip flexion range, OL [°] | 42.0 (29.0–57.9) |
| Hip flexion range, NOL [°] | 44.3 (20.9–60.5) |
| p-value | 0.632 |
| Minimum hip abduction, OL [°] | −8.1 [(−14.1)–(−0.7)] |
| Minimum hip abduction, NOL [°] | −8.3 [(−17.4)–(−2.7)] |
| p-value | 0.746 |
| Maximum hip abduction, OL [°] | 7.1 (1.8–17.4) |
| Maximum hip abduction, NOL [°] | 7.2 (0.1–17.5) |
| p-value | 0.575 |
| Hip abduction range, OL [°] | 15.3 (10.3–27.3) |
| Hip abduction range, NOL [°] | 16.9 (8.1–24.6) |
| p-value | 0.328 |
| Patients after Surgery (n = 23) | |
|---|---|
| Minimum knee flexion, OL [°] | −3.0 [(−7.5)–(−0.1)] |
| Minimum knee flexion, NOL [°] | −0.5 [(−20.4)–0.1] |
| p-value | 0.127 |
| Maximum knee flexion, OL [°] | 58.6 (38.0–72.9) |
| Maximum knee flexion, NOL [°] | 63.5 (21.6–74.7) |
| p-value | 0.878 |
| Knee flexion range, OL [°] | 63.5 (44.2–74.9) |
| Knee flexion range, NOL [°] | 64.9 (32.8–75.7) |
| p-value | 0.809 |
| Patients after Surgery (n = 23) | |
|---|---|
| Minimum ankle dorsiflexion, OL [°] | −14.3 [(−33.5)–(−3.5)] |
| Minimum ankle dorsiflexion, NOL [°] | −23.2 [(−32.8)–(−8.4)] |
| p-value | 0.011 |
| Maximum ankle dorsiflexion, OL [°] | 7.2 (2.2–16.8) |
| Maximum ankle dorsiflexion, NOL [°] | 12.8 (4.5–24.4) |
| p-value | <0.001 |
| Ankle dorsiflexion range, OL [°] | 21.3 (8.6–41.8) |
| Ankle dorsiflexion range, NOL [°] | 34.3 (22.4–47.1) |
| p-value | <0.001 |
| Minimum ankle inversion, OL [°] | −4.8 [(−16.2)–(−1.0)] |
| Minimum ankle inversion, NOL [°] | −7.4 [18.8–(−4.5)] |
| p-value | 0.005 |
| Maximum ankle inversion, OL [°] | 7.2 (0.7–15.8) |
| Maximum ankle inversion, NOL [°] | 11.9 (1.3–33.7) |
| p-value | 0.011 |
| Ankle inversion range, OL [°] | 11.3 (4.3–26.9) |
| Ankle inversion range, NOL [°] | 20.7 (7.6–42.1) |
| p-value | <0.001 |
| Minimum ankle abduction, OL [°] | −8.0 [(−28.40–(−2.4)] |
| Minimum ankle abduction, NOL [°] | −13.2 [(−33.1)–(−6.0)] |
| p-value | 0.004 |
| Maximum ankle abduction, OL [°] | 4.4 (0.8–17.2) |
| Maximum ankle abduction, NOL [°] | 6.8 (2.7–13.0) |
| p-value | 0.051 |
| Ankle abduction range, OL [°] | 13.9 (4.4–32.9) |
| Ankle abduction range, NOL [°] | 19.7 (9.6–37.2) |
| p-value | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wietecki, P.; Pawik, Ł.; Fink-Lwow, F.; Leśkow, A.; Górski, R.; Pawik, M.; Olech, J.; Klepacki, K.; Kuliński, P.; Reichert, P.; et al. Kinematic Parameters Following Pilon Fracture Treatment with the Ilizarov Method. J. Clin. Med. 2022, 11, 2763. https://doi.org/10.3390/jcm11102763
Wietecki P, Pawik Ł, Fink-Lwow F, Leśkow A, Górski R, Pawik M, Olech J, Klepacki K, Kuliński P, Reichert P, et al. Kinematic Parameters Following Pilon Fracture Treatment with the Ilizarov Method. Journal of Clinical Medicine. 2022; 11(10):2763. https://doi.org/10.3390/jcm11102763
Chicago/Turabian StyleWietecki, Paweł, Łukasz Pawik, Felicja Fink-Lwow, Artur Leśkow, Radosław Górski, Malwina Pawik, Jarosław Olech, Krzysztof Klepacki, Patryk Kuliński, Paweł Reichert, and et al. 2022. "Kinematic Parameters Following Pilon Fracture Treatment with the Ilizarov Method" Journal of Clinical Medicine 11, no. 10: 2763. https://doi.org/10.3390/jcm11102763
APA StyleWietecki, P., Pawik, Ł., Fink-Lwow, F., Leśkow, A., Górski, R., Pawik, M., Olech, J., Klepacki, K., Kuliński, P., Reichert, P., & Morasiewicz, P. (2022). Kinematic Parameters Following Pilon Fracture Treatment with the Ilizarov Method. Journal of Clinical Medicine, 11(10), 2763. https://doi.org/10.3390/jcm11102763