
Incidence of Venous Thromboembolism in Multiple Myeloma Patients across Different Regimens: Role of Procoagulant Microparticles and Cytokine Release

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection and Storage
2.2. Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kristinsson, S.Y.; Fears, T.R.; Gridley, G.; Turesson, I.; Mellqvist, U.H.; Björkholm, M.; Landgren, O. Deep vein thrombosis after monoclonal gammopathy of undetermined significance and multiple myeloma. Blood 2008, 112, 3582–3586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gogia, A.; Sikka, M.; Sharma, S.; Rusia, U. Hemostatic Abnormalities in Multiple Myeloma Patients. Asian Pac. J. Cancer Prev. 2018, 19, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Castelli, R.; Gualtierotti, R.; Orofino, N.; Losurdo, A.; Gandolfi, S.; Cugno, M. Current and emerging treatment options for patients with relapsed myeloma. Clin. Med. Insights Oncol. 2013, 7, 209–219. [Google Scholar] [CrossRef]
- Castelli, R.; Orofino, N.; Losurdo, A.; Gualtierotti, R.; Cugno, M. Choosing treatment options for patients with relapsed/refractory multiple myeloma. Expert Rev. Anticancer Ther. 2014, 14, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Castelli, R.; Pantaleo, G.; Gallipoli, P.; Gidaro, A.; Arquati, M.; Wu, M.A.; Lambertenghi Deliliers, G. Salvage therapy with bortezomib and dexamethasone in elderly patients with relapsed/refractory multiple myeloma. Anticancer Drugs 2015, 26, 1078–1082. [Google Scholar] [CrossRef]
- Tiong, I.S.; Rodgers, S.E.; Lee, C.H.; McRae, S.J. Baseline and treatment-related changes in thrombin generation in patients with multiple myeloma. Leuk. Lymphoma 2017, 58, 941–949. [Google Scholar] [CrossRef]
- Zangari, M.; Berno, T.; Zhan, F.; Tricot, G.; Fink, L. Mechanisms of thrombosis in paraproteinemias: The effects of immunomodulatory drugs. Semin. Thromb. Hemost. 2012, 38, 768–779. [Google Scholar] [CrossRef]
- Cini, M.; Zamagni, E.; Valdré, L.; Palareti, G.; Patriarca, F.; Tacchetti, P.; Cavo, M. Thalidomide-dexamethasone as up-front therapy for patients with newly diagnosed multiple myeloma: Thrombophilic alterations, thrombotic complications, and thromboprophylaxis with low-dose warfarin. Eur. J. Haematol. 2010, 84, 484–492. [Google Scholar] [CrossRef]
- Crowely, M.P.; Quinn, S.; Coleman, E.; Eustace, J.A.; Gilligan, O.M.; Shea, S.I. Differing coagulation profiles of patients with monoclonal gammopathy of undetermined significance and multiple myeloma. J. Thromb. Thrombolysis 2015, 39, 245–249. [Google Scholar] [CrossRef]
- Colombo, R.; Gallipoli, P.; Castelli, R. Thrombosis, and hemostatic abnormalities in hematological malignancies. Clin. Lymphoma Myeloma Leuk. 2014, 14, 441–450. [Google Scholar] [CrossRef]
- Zifkos, K.; Dubois, C.; Schäfer, K. Extracellular Vesicles and Thrombosis: Update on the Clinical and Experimental Evidence. Int. J. Mol. Sci. 2021, 22, 9317. [Google Scholar] [CrossRef]
- Auwerda, J.J.; Sonneveld, P.; de Maat, M.P.; Leebeek, F.W. Prothrombotic coagulation abnormalities in patients with newly diagnosed multiple myeloma. Haematologica 2007, 92, 279–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najem, M.Y.; Couturaud, F.; Lemarié, C.A. Cytokine and chemokine regulation of venous thromboembolism. J. Thromb. Haemost. 2020, 18, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Shet, A.S.; Aras, O.; Gupta, K.; Hass, M.J.; Rausch, D.J.; Saba, N.; Koopmeiners, L.; Key, N.S.; Hebbel, R.P. Sickle blood contains tissue factor-positive microparticles derived from endothelial cells and monocytes. Blood 2003, 102, 2678–2683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubiczkova, L.; Sedlarikova, L.; Hajek, R.; Sevcikova, S. TGF-β—An excellent servant but a bad master. J. Transl. Med. 2012, 10, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, T.; Kristensen, S.R.; Gregersen, H.; Teodorescu, E.M.; Pedersen, S. Prothrombotic abnormalities in patients with multiple myeloma and monoclonal gammopathy of undetermined significance. Thromb. Res. 2021, 202, 108–118. [Google Scholar] [CrossRef]
- Auwerda, J.J.; Yuana, Y.; Osanto, S.; de Maat, M.P.; Sonneveld, P.; Bertina, R.M.; Leebeek, F.W. Microparticle-associated tissue factor activity and venous thrombosis in multiple myeloma. Thromb. Haemost. 2011, 105, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, R.; Sakamoto, A.; Yamaguchi, R.; Haraguchi, M.; Narahara, S.; Sugiuchi, H.; Yamaguchi, Y. Di-(2-Ethylhexyl) Phthalate Promotes Release of Tissue Factor-Bearing Microparticles From Macrophages via the TGFβ1/Smad/PAI-1 Signaling Pathway. Am. J. Med. Sci. 2019, 357, 492–506. [Google Scholar] [CrossRef]
- Kadota, T.; Fujita, Y.; Yoshioka, Y.; Araya, J.; Kuwano, K.; Ochiya, T. Emerging role of extracellular vesicles as a senescenceassociated secretory phenotype: Insights into the pathophysiology of lung diseases. Mol. Asp. Med. 2018, 60, 92–103. [Google Scholar] [CrossRef]
- Braga, W.M.; Atanackovic, D.; Colleoni, G.W. The Role of Regulatory T Cells and TH17 Cells in Multiple Myeloma. J. Immunol. Res. 2012, 2012, 293479. [Google Scholar] [CrossRef]
- Bettelli, E.; Carrier, Y.; Gao, W.; Korn, T.; Strom, T.B.; Oukka, M.; Weiner, H.L.; Kuchroo, V.K. Reciprocal developmental pathways for the generation of pathogenic effector TH17 and regulatory T cells. Nature 2006, 441, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Hadjiaggelidou, C.; Mandala, E.; Terpos, E.; Yiannaki, E.; Markala, D.; Triantafyllou, T.; Papatheodorou, A.; Gkastari, V.; Verrou, E.; Papanikolaou, A.; et al. Evaluation of regulatory T cells (Tregs) alterations in patients with multiple myeloma treated with bortezomib or lenalidomide plus dexamethasone: Correlations with treatment outcome. Ann. Hematol. 2019, 98, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Castelli, R.; Cannavò, A.; Conforti, F.; Grava, G.; Cortelezzi, A. Immunomodulatory drugs in multiple myeloma: From molecular mechanisms of action to clinical practice. Immunopharmacol. Immunotoxicol. 2012, 34, 740–753. [Google Scholar] [CrossRef] [PubMed]
- Galustian, C.; Meyer, B.; Labarthe, M.C.; Dredge, K.; Klaschka, D.; Henry, J.; Todryk, S.; Chen, R.; Muller, G.; Stirling, D.; et al. The anti-cancer agents lenalidomide and pomalidomide inhibit the proliferation and function of T regulatory cells. Cancer Immunol. Immunother. 2009, 58, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V.; Blood, E.; Vesole, D.; Fonseca, R.; Greipp, P.R.; Eastern Cooperative Oncology Group. Phase III clinical trial of thalidomide plus dexamethasone compared with dexamethasone alone in newly diagnosed multiple myeloma: A clinical trial coordinated by the Eastern Cooperative Oncology Group. J. Clin. Oncol. 2006, 24, 431–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palumbo, A.; Rajkumar, S.V.; Dimopoulos, M.A.; Richardson, P.G.; San Miguel, J.; Barlogie, B.; Harousseau, J.; Zonder, J.A.; Cavo, M.; Zangari, M.; et al. Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia 2008, 22, 414–423. [Google Scholar] [CrossRef] [Green Version]
- Rajkumar, S.V.; Jacobus, S.; Callander, N.S.; Fonseca, R.; Vesole, D.H.; Williams, M.E.; Abonour, R.; Siegel, D.S.; Katz, M.; Greipp, P.R.; et al. Lenalidomide plus high-dose dexamethasone versus lenalidomide plus low-dose dexamethasone as initial therapy for newly diagnosed multiple myeloma: An open-label randomised controlled trial. Lancet Oncol. 2010, 11, 29–37, Erratum in Lancet Oncol. 2010, 11, 14. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| A. Whole Population | B. Dexamethasone and Bortezomib | C. IMiDs | D. Watch and Waits Smoldering MM | p Value B vs. C | p Value B vs. D | p Value C vs. D | |
|---|---|---|---|---|---|---|---|
| Age [years] | 74 (70–82) | 68 (67–73.5) | 80 (74–82) | 72 (70–80) | <0.001 | 0.025 | 0.002 |
| Number of patients with thrombosis/number of patients | 14/123 | 10/29 | 4/63 | 0/31 | 0.002 | 0.017 | 0.3 |
| ● Melphalan, Prednisone and Thalidomide (MPT) | 4/32 | ||||||
| ● Lenalidomide | 0/31 | ||||||
| Median follow-up [months] | 12 (10–16) | 12 (8–13) | 12 (8–13) | 20 (12–32) | |||
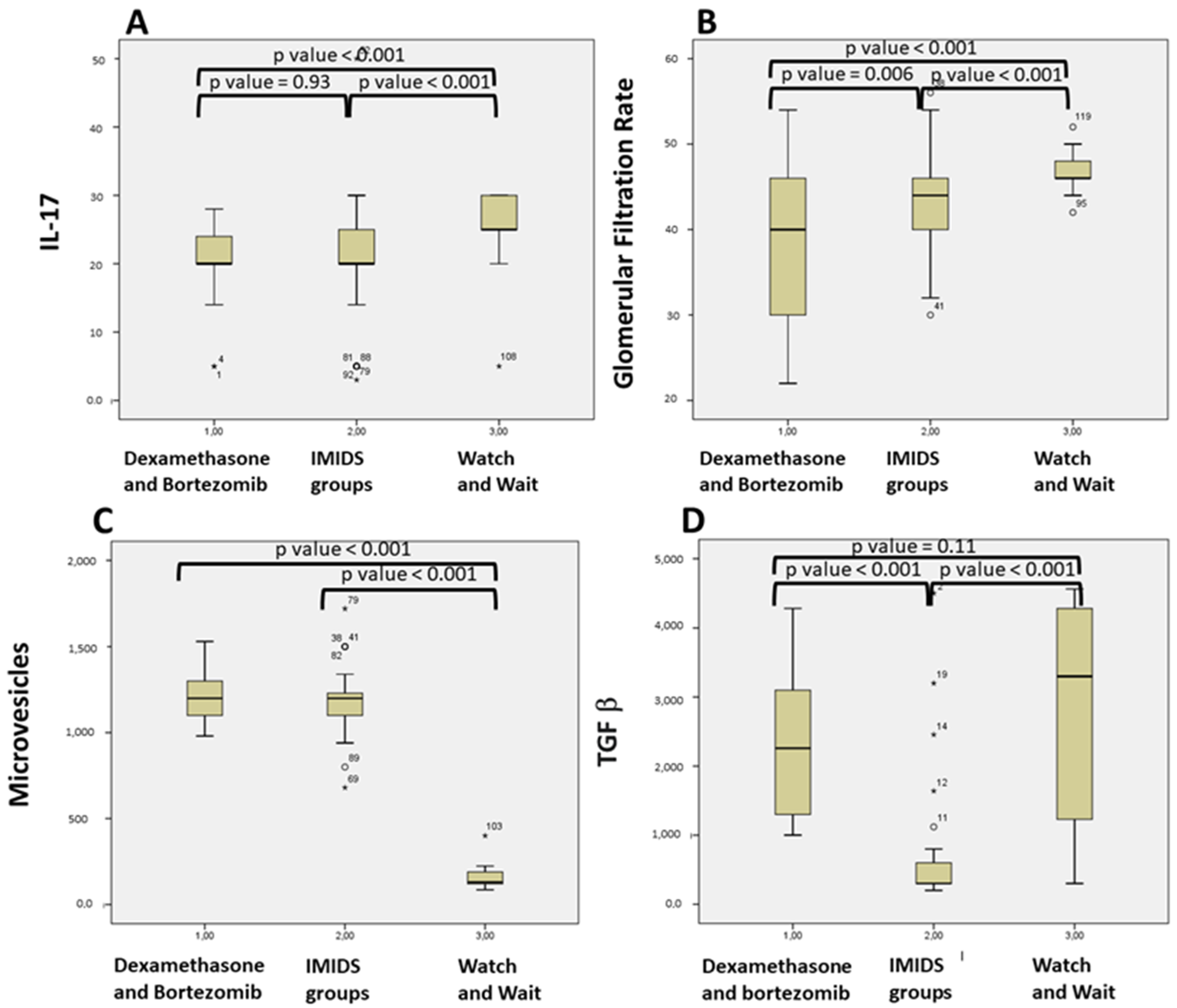
| Microvescicles [N/mL] | 1100 (400–1200) | 1200 (1100–1300) | 1200 (1100–1230) | 130 (120–190) | 0.83 | <0.001 | <0.001 |
| Hemoglobin [g/dL] | 10.2 (9.6–11.3) | 10.4 (9.4–11.4) | 10.4 (9.6–11.4) | 10 (9.7–10.7) | 0.65 | 0.77 | 0.4 |
| Glomerular Filtration Rate (eGFR) [mL/min/1.73 m2] | 46 (40–48) | 40 (30–46) | 44 (40–46) | 46 (46–48) | 0.006 | <0.001 | <0.001 |
| Number of patients with Chronic kidney disease (CKD) Stage 3a: 45 to 59 [mL/min/1.73 m2] eGFR | 68 | 9 | 30 | 29 | 0.17 | <0.001 | <0.001 |
| Number of patients with CKD Stage 3b: 30 to 44 [mL/min/1.73 m2] eGFR | 49 | 20 | 33 | 2 | 0.17 | <0.001 | <0.001 |
| Platelets [×109/L] | 187,000 (142,000–210,000) | 203,000 (126,000–230,000) | 178,000 (142,000–203,000) | 164,000 (123,000–242,500) | 0.27 | 0.9 | 0.9 |
| Activated Partial Thromboplastin Time (aPTT) | 1.02 (0.96–1.08) | 1 (0.96–1.06) | 1.03 (0.97–1.06) | 1.01 (0.97–1.08) | 0.91 | 0.95 | 0.97 |
| International Normalized Ratio (INR) | 1 (0.95–1.05 | 1.01 (0.95–1.03) | 0.99 (0.96–1.03) | 1.01 (0.95–1.05) | 0.97 | 0.91 | 0.93 |
| TNF-α [pg/mL] | 1 (1–2) | 2 (1–2) | 2 (1–2) | 1 (1–2) | 0.14 | 0.029 | 0.14 |
| IL-17 [pg/mL] | 20 (20–25) | 20 (18–24) | 20 (20–25) | 25 (25–30) | 0.93 | <0.001 | <0.001 |
| TGF-β pg/mL | 1100 (300–2456) | 2259 (1290–3150) | 300 (300–600) | 3300 (1200–4280) | <0.001 | 0.11 | <0.001 |
| Monoclonal protein level [g/dL] | 3 (2.6–3.5) | 2.6 (2.4–3.5) | 3 (3–3.5) | 3 (3–3.5) | 0.037 | 0.1 | 0.97 |
| IL-10 [pg/mL] | 12 (6–35) | 6 (2–10) | 25 (7–60) | 12 (12–12) | <0.001 | <0.001 | 0.266 |
| A. Whole Population | B. Patients with Thrombosis | C. Patients without Thrombosis | p Value Univariate | p Value Multivariate Cox Proportional Hazard Model | Odds Ratio Multivariate | |
|---|---|---|---|---|---|---|
| Age [years] | 74 (70–82) | 71.5 (67.75–77.25) | 74 (70–82) | 0.713 | ||
| Number of patients | 123 | 14 | 109 | |||
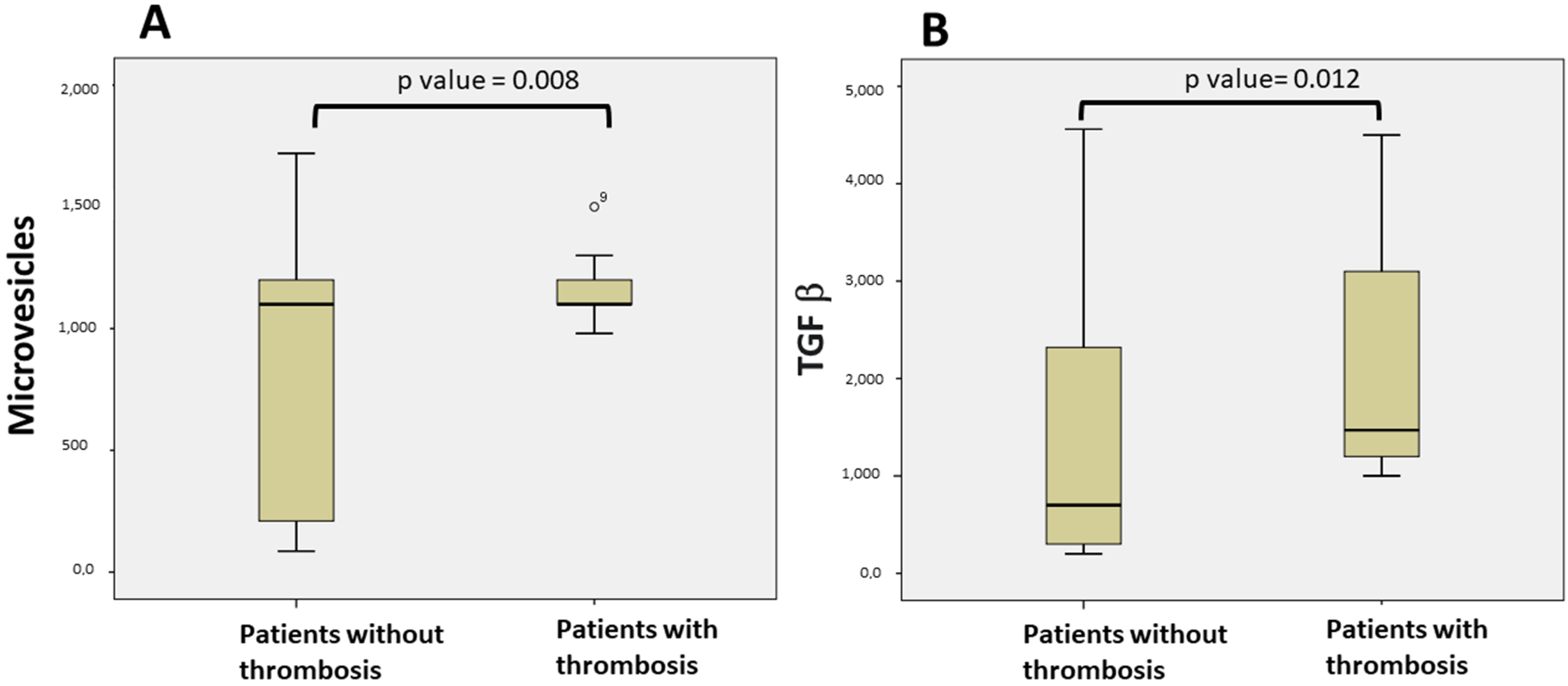
| Microvescicles [N/mL] | 1100 (400–1200) | 1100 (1087–1200) | 1100 (200–1200) | 0.008 | 0.001 | 0.003 (0.001–0.005) |
| TNF α [pg/mL] | 1 (1–2) | 1.5 (1–2) | 1 (1–2) | 0.228 | ||
| IL-17 [pg/mL] | 20 (20–25) | 20 (14–21.25) | 20 (20–25) | 0.085 | ||
| TGF-β ng/mL | 1100 (300–2456) | 1470 (1180–3145) | 700 (300–2360) | 0.012 | 0.003 | 0.001 (0–0.003) |
| IL-10 [pg/mL] | 12 (6–35) | 7.5 (4.25–13.5) | 12 (6.5–36) | 0.181 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gidaro, A.; Manetti, R.; Delitala, A.P.; Soloski, M.J.; Lambertenghi Deliliers, G.; Castro, D.; Soldini, D.; Castelli, R. Incidence of Venous Thromboembolism in Multiple Myeloma Patients across Different Regimens: Role of Procoagulant Microparticles and Cytokine Release. J. Clin. Med. 2022, 11, 2720. https://doi.org/10.3390/jcm11102720
Gidaro A, Manetti R, Delitala AP, Soloski MJ, Lambertenghi Deliliers G, Castro D, Soldini D, Castelli R. Incidence of Venous Thromboembolism in Multiple Myeloma Patients across Different Regimens: Role of Procoagulant Microparticles and Cytokine Release. Journal of Clinical Medicine. 2022; 11(10):2720. https://doi.org/10.3390/jcm11102720
Chicago/Turabian StyleGidaro, Antonio, Roberto Manetti, Alessandro Palmerio Delitala, Mark Jon Soloski, Giorgio Lambertenghi Deliliers, Dante Castro, Davide Soldini, and Roberto Castelli. 2022. "Incidence of Venous Thromboembolism in Multiple Myeloma Patients across Different Regimens: Role of Procoagulant Microparticles and Cytokine Release" Journal of Clinical Medicine 11, no. 10: 2720. https://doi.org/10.3390/jcm11102720
APA StyleGidaro, A., Manetti, R., Delitala, A. P., Soloski, M. J., Lambertenghi Deliliers, G., Castro, D., Soldini, D., & Castelli, R. (2022). Incidence of Venous Thromboembolism in Multiple Myeloma Patients across Different Regimens: Role of Procoagulant Microparticles and Cytokine Release. Journal of Clinical Medicine, 11(10), 2720. https://doi.org/10.3390/jcm11102720