
Setting for “Normal” Serum Ferritin Levels in Patients with Transfusion-Dependent Thalassemia: Our Current Strategy


 ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Biochemical Assays
2.3. Iron Overload Assessment
2.4. Diagnostic Criteria
- -
- Hypogonadism: no spontaneous puberty or failure to proceed through puberty after the age of 16 years; after puberty, in females, loss of menses before the age 45 years and in males reduced libido, impotence, low levels of gonadotropin, and free and total testosterone;
- -
- Hypothyroidism: high serum thyrotropin concentration and normal or reduced free thyroxine levels (primary form), normal or low serum thyrotropin concentration, and reduced free thyroxine levels (central form);
- -
- Hypoparathyroidism: low serum calcium concentration, increased serum phosphate, low serum parathyroid hormone or, if normal, inappropriate for the calcium level;
- -
- Diabetes mellitus: fasting plasma glucose ≥ 126 mg/dL or 2-h plasma glucose ≥ 200 mg/dL during an oral glucose tolerance test or in patients with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥ 200 mg/dL [29].
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Serum Ferritin and Clinical Correlates
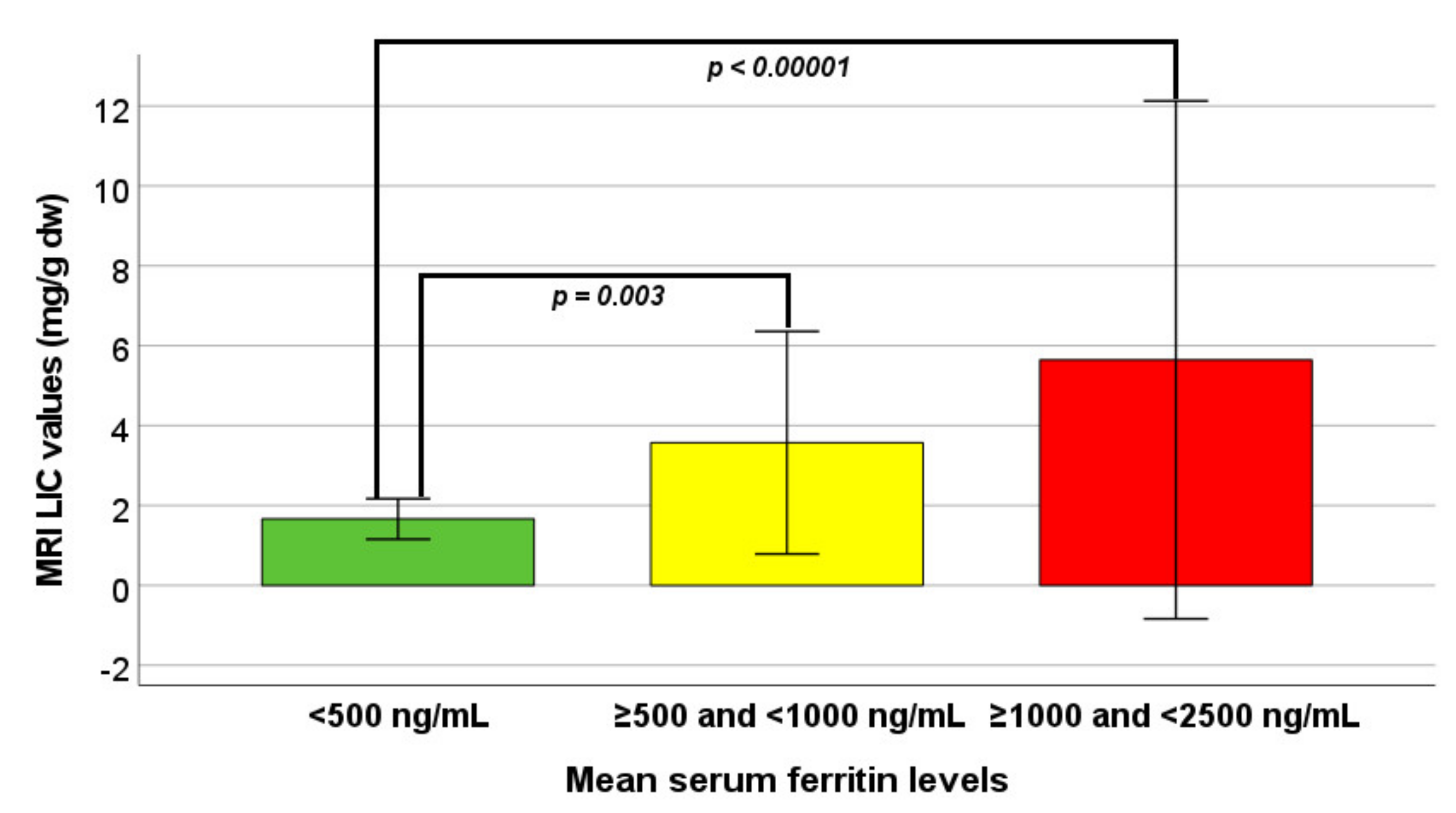
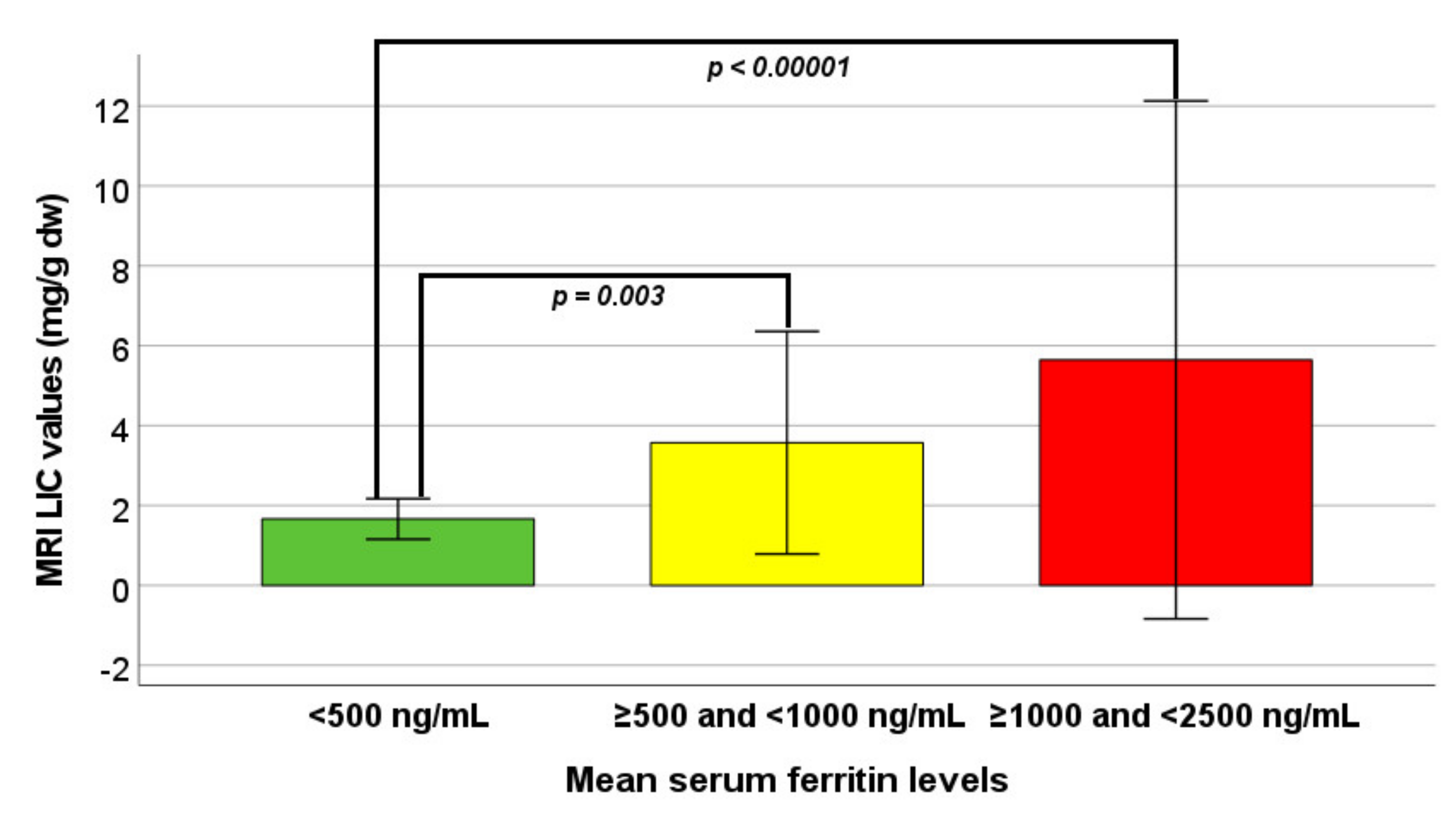
3.3. Serum Ferritin and Iron Overload
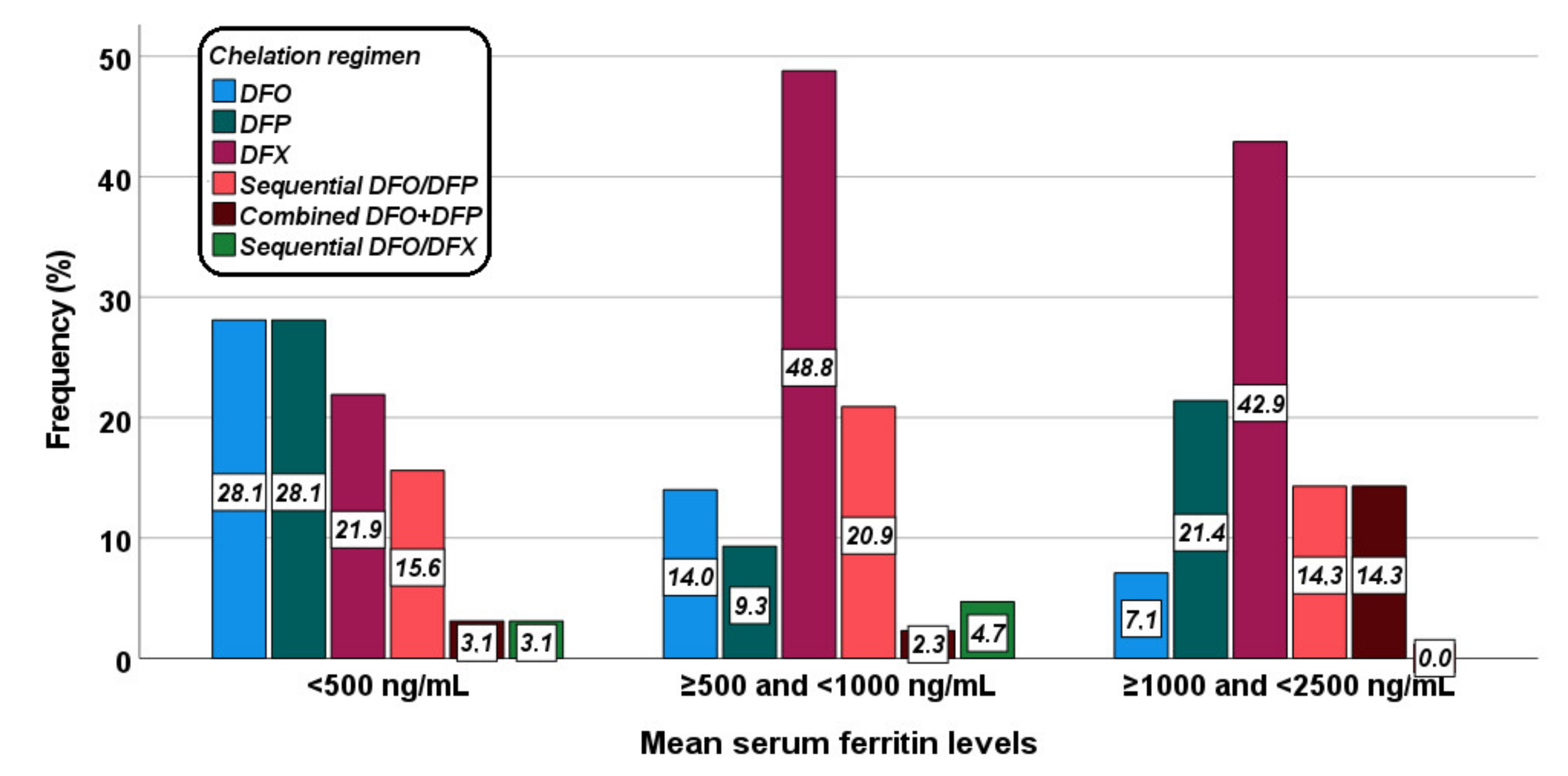
3.4. Serum Ferritin and Chelation Therapy
3.5. Patients with Serum Ferritin Levels ≥ 2500 ng/mL
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pepe, A.; Meloni, A.; Rossi, G.; Midiri, M.; Missere, M.; Valeri, G.; Sorrentino, F.; D’Ascola, D.G.; Spasiano, A.; Filosa, A.; et al. Prediction of cardiac complications for thalassemia major in the widespread cardiac magnetic resonance era: A prospective multicentre study by a multi-parametric approach. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Pepe, A.; Pistoia, L.; Gamberini, M.R.; Cuccia, L.; Peluso, A.; Messina, G.; Spasiano, A.; Allo, M.; Bisconte, M.G.; Putti, M.C.; et al. The Close Link of Pancreatic Iron With Glucose Metabolism and With Cardiac Complications in Thalassemia Major: A Large, Multicenter Observational Study. Diabetes Care 2020, 43, 2830–2839. [Google Scholar] [CrossRef]
- Borgna-Pignatti, C.; Rugolotto, S.; De Stefano, P.; Zhao, H.; Cappellini, M.D.; Del Vecchio, G.C.; Romeo, M.A.; Forni, G.L.; Gamberini, M.R.; Ghilardi, R.; et al. Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine. Haematologica 2004, 89, 1187–1193. [Google Scholar] [PubMed]
- Modell, B.; Khan, M.; Darlison, M.; Westwood, M.A.; Ingram, D.; Pennell, D.J. Improved survival of thalassaemia major in the UK and relation to T2* cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2008, 10, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, M.A.; Galanello, R.; Dessi, C.; Smith, G.C.; Westwood, M.A.; Agus, A.; Roughton, M.; Assomull, R.; Nair, S.V.; Walker, J.M.; et al. A randomized, placebo-controlled, double-blind trial of the effect of combined therapy with deferoxamine and deferiprone on myocardial iron in thalassemia major using cardiovascular magnetic resonance. Circulation 2007, 115, 1876–1884. [Google Scholar] [CrossRef] [PubMed]
- Pennell, D.J.; Berdoukas, V.; Karagiorga, M.; Ladis, V.; Piga, A.; Aessopos, A.; Gotsis, E.D.; Tanner, M.A.; Smith, G.C.; Westwood, M.A.; et al. Randomized controlled trial of deferiprone or deferoxamine in beta-thalassemia major patients with asymptomatic myocardial siderosis. Blood 2006, 107, 3738–3744. [Google Scholar] [CrossRef] [Green Version]
- Berdoukas, V.; Chouliaras, G.; Moraitis, P.; Zannikos, K.; Berdoussi, E.; Ladis, V. The efficacy of iron chelator regimes in reducing cardiac and hepatic iron in patients with thalassaemia major: A clinical observational study. J. Cardiovasc. Magn. Reson. 2009, 11, 20. [Google Scholar] [CrossRef] [Green Version]
- Pennell, D.J.; Porter, J.B.; Piga, A.; Lai, Y.; El-Beshlawy, A.; Belhoul, K.M.; Elalfy, M.; Yesilipek, A.; Kilinc, Y.; Lawniczek, T.; et al. A 1-year randomized controlled trial of deferasirox vs. deferoxamine for myocardial iron removal in beta-thalassemia major (CORDELIA). Blood 2014, 123, 1447–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, A.; Meloni, A.; Rossi, G.; Cuccia, L.; D’Ascola, G.D.; Santodirocco, M.; Cianciulli, P.; Caruso, V.; Romeo, M.A.; Filosa, A.; et al. Cardiac and hepatic iron and ejection fraction in thalassemia major: Multicentre prospective comparison of combined deferiprone and deferoxamine therapy against deferiprone or deferoxamine monotherapy. J. Cardiovasc. Magn. Reson. 2013, 15, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, A.; Meloni, A.; Pistoia, L.; Cuccia, L.; Gamberini, M.R.; Lisi, R.; D’Ascola, D.G.; Rosso, R.; Allo, M.; Spasiano, A.; et al. MRI multicentre prospective survey in thalassaemia major patients treated with deferasirox versus deferiprone and desferrioxamine. Br. J. Haematol. 2018, 183, 783–795. [Google Scholar] [CrossRef] [Green Version]
- Noetzli, L.J.; Mittelman, S.D.; Watanabe, R.M.; Coates, T.D.; Wood, J.C. Pancreatic iron and glucose dysregulation in thalassemia major. Am. J. Hematol. 2012, 87, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Meloni, A.; Restaino, G.; Missere, M.; De Marchi, D.; Positano, V.; Valeri, G.; Giuseppe D’Ascola, D.; Peluso, A.; Caterina Putti, M.; Lendini, M.; et al. Pancreatic iron overload by T2* MRI in a large cohort of well treated thalassemia major patients: Can it tell us heart iron distribution and function? Am. J. Hematol. 2015, 90, E189–E190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, B.A.; O’Sullivan, C.; Jarritt, P.H.; Porter, J.B. Value of sequential monitoring of left ventricular ejection fraction in the management of thalassemia major. Blood 2004, 104, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Gabutti, V.; Piga, A. Results of long-term iron-chelating therapy. Acta Haematol. 1996, 95, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Olivieri, N.F.; Nathan, D.G.; MacMillan, J.H.; Wayne, A.S.; Liu, P.P.; McGee, A.; Martin, M.; Koren, G.; Cohen, A.R. Survival in medically treated patients with homozygous beta-thalassemia. N. Engl. J. Med. 1994, 331, 574–578. [Google Scholar] [CrossRef]
- Musallam, K.M.; Angastiniotis, M.; Eleftheriou, A.; Porter, J.B. Cross-talk between available guidelines for the management of patients with beta-thalassemia major. Acta Haematol. 2013, 130, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Pepe, A.; Positano, V.; Santarelli, F.; Sorrentino, F.; Cracolici, E.; De Marchi, D.; Maggio, A.; Midiri, M.; Landini, L.; Lombardi, M. Multislice multiecho T2* cardiovascular magnetic resonance for detection of the heterogeneous distribution of myocardial iron overload. J. Magn. Reson. Imaging 2006, 23, 662–668. [Google Scholar] [CrossRef]
- Ramazzotti, A.; Pepe, A.; Positano, V.; Rossi, G.; De Marchi, D.; Brizi, M.G.; Luciani, A.; Midiri, M.; Sallustio, G.; Valeri, G.; et al. Multicenter validation of the magnetic resonance t2* technique for segmental and global quantification of myocardial iron. J. Magn. Reson. Imaging 2009, 30, 62–68. [Google Scholar] [CrossRef]
- Meloni, A.; De Marchi, D.; Pistoia, L.; Grassedonio, E.; Peritore, G.; Preziosi, P.; Restaino, G.; Righi, R.; Riva, A.; Renne, S.; et al. Multicenter validation of the magnetic resonance T2* technique for quantification of pancreatic iron. Eur. Radiol. 2019, 29, 2246–2252. [Google Scholar] [CrossRef] [PubMed]
- Positano, V.; Salani, B.; Pepe, A.; Santarelli, M.F.; De Marchi, D.; Ramazzotti, A.; Favilli, B.; Cracolici, E.; Midiri, M.; Cianciulli, P.; et al. Improved T2* assessment in liver iron overload by magnetic resonance imaging. Magn. Reson. Imaging 2009, 27, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Restaino, G.; Meloni, A.; Positano, V.; Missere, M.; Rossi, G.; Calandriello, L.; Keilberg, P.; Mattioni, O.; Maggio, A.; Lombardi, M.; et al. Regional and global pancreatic T*(2) MRI for iron overload assessment in a large cohort of healthy subjects: Normal values and correlation with age and gender. Magn. Reson. Med. 2011, 65, 764–769. [Google Scholar] [CrossRef] [PubMed]
- Meloni, A.; Positano, V.; Pepe, A.; Rossi, G.; Dell’Amico, M.; Salvatori, C.; Keilberg, P.; Filosa, A.; Sallustio, G.; Midiri, M.; et al. Preferential patterns of myocardial iron overload by multislice multiecho T*2 CMR in thalassemia major patients. Magn. Reson. Med. 2010, 64, 211–219. [Google Scholar] [CrossRef]
- Positano, V.; Pepe, A.; Santarelli, M.F.; Scattini, B.; De Marchi, D.; Ramazzotti, A.; Forni, G.; Borgna-Pignatti, C.; Lai, M.E.; Midiri, M.; et al. Standardized T2* map of normal human heart in vivo to correct T2* segmental artefacts. NMR Biomed. 2007, 20, 578–590. [Google Scholar] [CrossRef] [PubMed]
- Meloni, A.; Luciani, A.; Positano, V.; De Marchi, D.; Valeri, G.; Restaino, G.; Cracolici, E.; Caruso, V.; Dell’amico, M.C.; Favilli, B.; et al. Single region of interest versus multislice T2* MRI approach for the quantification of hepatic iron overload. J. Magn. Reson. Imaging 2011, 33, 348–355. [Google Scholar] [CrossRef]
- Meloni, A.; Rienhoff, H.Y., Jr.; Jones, A.; Pepe, A.; Lombardi, M.; Wood, J.C. The use of appropriate calibration curves corrects for systematic differences in liver R2* values measured using different software packages. Br. J. Haematol. 2013, 161, 888–891. [Google Scholar] [CrossRef] [PubMed]
- Wood, J.C.; Enriquez, C.; Ghugre, N.; Tyzka, J.M.; Carson, S.; Nelson, M.D.; Coates, T.D. MRI R2 and R2* mapping accurately estimates hepatic iron concentration in transfusion-dependent thalassemia and sickle cell disease patients. Blood 2005, 106, 1460–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meloni, A.; De Marchi, D.; Positano, V.; Neri, M.G.; Mangione, M.; Keilberg, P.; Lendini, M.; Cirotto, C.; Pepe, A. Accurate estimate of pancreatic T2* values: How to deal with fat infiltration. Abdom. Imaging 2015, 40, 3129–3136. [Google Scholar] [CrossRef]
- Meloni, A.; Positano, V.; Ruffo, G.B.; Spasiano, A.; D’Ascola, D.G.; Peluso, A.; Keilberg, P.; Restaino, G.; Valeri, G.; Renne, S.; et al. Improvement of heart iron with preserved patterns of iron store by CMR-guided chelation therapy. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 325–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Standards of Medical Care in Diabetes—2011. Diabetes Care 2011, 34 (Suppl. S1), S11–S61. [CrossRef] [Green Version]
- WHO. Prevention and Management of Osteoporosis; World Health Organization: Geneva, Switzerland, 2003; Volume 921, pp. 1–164. [Google Scholar]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Buxton, A.E.; Calkins, H.; Callans, D.J.; DiMarco, J.P.; Fisher, J.D.; Greene, H.L.; Haines, D.E.; Hayes, D.L.; Heidenreich, P.A.; Miller, J.M.; et al. ACC/AHA/HRS 2006 key data elements and definitions for electrophysiological studies and procedures: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (ACC/AHA/HRS Writing Committee to Develop Data Standards on Electrophysiology). Circulation 2006, 114, 2534–2570. [Google Scholar]
- Angelucci, E.; Brittenham, G.M.; McLaren, C.E.; Ripalti, M.; Baronciani, D.; Giardini, C.; Galimberti, M.; Polchi, P.; Lucarelli, G. Hepatic iron concentration and total body iron stores in thalassemia major. N. Engl. J. Med. 2000, 343, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Positano, V.; Meloni, A.; Santarelli, M.F.; Gerardi, C.; Bitti, P.P.; Cirotto, C.; De Marchi, D.; Salvatori, C.; Landini, L.; Pepe, A. Fast generation of T2* maps in the entire range of clinical interest: Application to thalassemia major patients. Comput. Biol. Med. 2015, 56, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Ricchi, P.; Ammirabile, M.; Spasiano, A.; Costantini, S.; Cinque, P.; Di Matola, T.; Pagano, L.; Prossomariti, L. Combined chelation therapy in thalassemia major with deferiprone and desferrioxamine: A retrospective study. Eur. J. Haematol. 2010, 85, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Pepe, A.; Meloni, A.; Rossi, G.; Dell’Amico, M.C.; Spasiano, A.; Capra, M.; Cianciulli, P.; Caruso, V.; Favilli, B.; Cracolici, E.; et al. A T2* MRI prospective survey on heart iron in thalassemia major patients treated with deferasirox versus deferiprone and desferrioxamine in monotherapy. J. Cardiovasc. Magn. Reson. 2011, 13, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Farmaki, K.; Tzoumari, I.; Pappa, C.; Chouliaras, G.; Berdoukas, V. Normalisation of total body iron load with very intensive combined chelation reverses cardiac and endocrine complications of thalassaemia major. Br. J. Haematol. 2010, 148, 466–475. [Google Scholar] [CrossRef]
- Kolnagou, A.; Kleanthous, M.; Kontoghiorghes, G.J. Efficacy, compliance and toxicity factors are affecting the rate of normalization of body iron stores in thalassemia patients using the deferiprone and deferoxamine combination therapy. Hemoglobin 2011, 35, 186–198. [Google Scholar] [CrossRef] [PubMed]
- Pinna, F.; Carta, R.; Morittu, M.; Dessi, C.; Moi, P.; Leoni, G.; Foschini, M.L.; Defraia, E.; Zappu, A.; Origa, R. Thalassemia Major: Who Is Afraid of Serum Ferritin below 500 mug/l? Acta Haematol. 2015, 134, 183–184. [Google Scholar] [CrossRef]
- Jehn, M.; Clark, J.M.; Guallar, E. Serum ferritin and risk of the metabolic syndrome in U.S. adults. Diabetes Care 2004, 27, 2422–2428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricchi, P.; Meloni, A.; Spasiano, A.; Costantini, S.; Pepe, A.; Cinque, P.; Filosa, A. The impact of liver steatosis on the ability of serum ferritin levels to be predictive of liver iron concentration in non-transfusion-dependent thalassaemia patients. Br. J. Haematol. 2018, 180, 721–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponticelli, C.; Musallam, K.M.; Cianciulli, P.; Cappellini, M.D. Renal complications in transfusion-dependent beta thalassaemia. Blood Rev. 2010, 24, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Ang, A.L.; Shah, F.T.; Davis, B.A.; Thomas, A.; Murugachandran, G.; Kumuradevan, J.; Garbowksi, M.W.; Porter, J.B. Deferiprone is Associated with Lower Serum Ferritin (SF) Relative to Liver Iron Concentration (LIC) Than Deferoxamine and Deferasirox- Implications for Clinical Practice. Blood 2010, 116, 4246. [Google Scholar] [CrossRef]
- Pennell, D.J.; Udelson, J.E.; Arai, A.E.; Bozkurt, B.; Cohen, A.R.; Galanello, R.; Hoffman, T.M.; Kiernan, M.S.; Lerakis, S.; Piga, A.; et al. Cardiovascular function and treatment in beta-thalassemia major: A consensus statement from the American Heart Association. Circulation 2013, 128, 281–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, F.T.; Porter, J.B.; Sadasivam, N.; Kaya, B.; Moon, J.C.; Velangi, M.; Ako, E.; Pancham, S. Guidelines for the monitoring and management of iron overload in patients with haemoglobinopathies and rare anaemias. Br. J. Haematol. 2021. [Google Scholar] [CrossRef]
- Taher, A.T.; Musallam, K.M.; Cappellini, M.D. beta-Thalassemias. N. Engl. J. Med. 2021, 384, 727–743. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Mean Serum Ferritin < 500 ng/mL (N = 32) | Mean Serum Ferritin ≥ 500 and <1000 ng/mL (N = 43) | Mean Serum Ferritin ≥ 1000 and <2500 ng/mL (N = 28) | p | |
|---|---|---|---|---|
| Demographic and clinical characteristics | ||||
| Age (years) | 41.87 ± 7.78 | 39.88 ± 8.93 | 38.15 ± 10.74 | 0.292 |
| Females, N (%) | 17 (53.1) | 26 (60.5) | 16 (57.1) | 0.817 |
| Regular transfusions starting age (months) | 16.47 ± 18.08 | 13.28 ± 13.96 | 19.79 ± 28.96 | 0.192 |
| Chelation starting age (years) | 7.33 ± 5.12 | 5.82 ± 4.38 | 6.27 ± 6.76 | 0.255 |
| Genotype, N (%) | 0.998 | |||
| β+β+ | 5 (15.6) | 7 (16.3) | 5 (17.9) | |
| β0β+ | 15 (46.9) | 20 (46.5) | 12 (42.9) | |
| β0β0 | 12 (37.5) | 16 (37.2) | 11 (39.3) | |
| Splenectomy, N (%) | 21 (65.6) | 22 (51.2) | 13 (46.4) | 0.283 |
| HCV infection, N (%) | 0.515 | |||
| Negative | 10 (31.3) | 11 (25.6) | 10 (35.7) | |
| Spontaneously eradicated | 11 (34.4) | 15 (34.9) | 8 (28.6) | |
| Eradicated after treatment | 5 (15.6) | 14 (32.6) | 6 (24.0) | |
| Chronic | 6 (18.8) | 3 (7.0) | 4 (14.3) | |
| Hematological parameters | ||||
| Mean hemoglobin (g/dL) | 9.93 ± 0.34 | 9.78 ± 0.38 | 9.78 ± 0.41 | 0.265 |
| Alanine aminotransferase (U/L) | 31.59 ± 28.07 | 21.63 ± 11.07 | 29.04 ± 20.31 | 0.274 |
| Aspartate aminotransferase (U/L) | 29.25 ± 24.15 | 22.23 ± 8.67 | 25.32 ± 10.12 | 0.274 |
| Gamma-glutamyl transpeptidase (U/L) | 29.59 ± 23.29 | 21.35 ± 18.11 | 29.11 ± 17.47 | 0.053 |
| Creatinine (mg/dL | 0.67 ± 0.16 | 0.67 ± 0.14 | 1.02 ± 1.26 | 0.243 |
| Uric acid (mg/dL) | 4.47 ± 0.96 | 4.02 ± 1.03 | 4.34 ± 0.81 | 0.155 |
| Total cholesterol (mg/dL) | 106.71 ± 27.86 | 111.51 ± 25.95 | 115.39 ± 28.75 | 0.487 |
| Triglycerides (mg/dL) | 91.43 ± 42.47 | 99.37 ± 44.30 | 140.59 ± 92.43 | 0.025 |
| High-density lipoprotein cholesterol (mg/dL) | 38.15 ± 14.65 | 41.34 ± 13.26 | 36.87 ± 13.52 | 0.408 |
| Complications | ||||
| Hepatic cirrhosis, N (%) | 0 (0.0) | 2 (4.7) | 0 (0.0) | 0.241 |
| Hypogonadism, N (%) | 17 (53.1) | 23 (53.5) | 12 (42.9) | 0.639 |
| Hypothyroidism, N (%) | 7 (21.9) | 11 (25.6) | 7 (25.0) | 0.929 |
| Hypoparathyroidism, N (%) | 1 (3.1) | 1 (2.3) | 1 (3.6) | 0.951 |
| Diabetes mellitus, N (%) | 5 (15.6) | 3 (7.0) | 3 (10.7) | 0.487 |
| Osteopenia/osteoporosis, N (%) | 24 (75.0) | 33 (76.7) | 21 (75.0) | 0.979 |
| Hearing loss, N (%) | 7 (21.9) | 11/32 (26.1) | 6/26 (23.2) | 0.904 |
| Ophthalmic diseases, N (%) | 0 (0.0) | 0/41 (0.0) | 0/25 (0.0) | - |
| Heart failure, N (%) | 1 (3.1) | 0 (0.0) | 0 (0.0) | 0.326 |
| Arrhythmias, N (%) | 2 (6.3) | 1 (2.3) | 1 (3.6) | 0.681 |
| Mean Serum Ferritin < 500 ng/mL (N = 25) | Mean Serum Ferritin ≥ 500 and <1000 ng/mL (N = 37) | Mean Serum Ferritin ≥ 1000 and <2500 ng/mL (N = 23) | p | |
|---|---|---|---|---|
| MRI LIC (mg/g dw) | 1.67 ± 0.51 | 3.57 ± 2.79 | 5.65 ± 6.48 | <0.0001 |
| MRI LIC ≥ 3 mg/g dw, N (%) | 1 (4.0) | 14 (37.8) | 11 (47.8) | 0.002 |
| Global pancreas T2* (ms) | 9.34 ± 8.24 | 11.29 ± 8.29 | 9.92 ± 8.72 | 0.479 |
| Global pancreas T2* < 26 ms, N (%) | 23 (92.0) | 34 (91.9) | 20 (87.0) | 0.783 |
| Global heart T2* (ms) | 42.51 ± 4.75 | 38.79 ± 8.16 | 34.91 ± 11.64 | 0.048 |
| Global heart T2* < 20 ms, N (%) | 0 (0.0) | 1 (2.7) | 4 (17.4) | 0.021 |
| Mean Serum Ferritin Levels | MRI LIC | Global Pancreas T2* | Global Heart T2* | |
|---|---|---|---|---|
| DFO therapy (N = 14) | ||||
| Mean value | 608.14 ± 326.68 ng/mL | 1.88 ± 1.03 mg/g dw | 8.63 ± 5.39 ms | 40.71 ± 7.43 ms |
| Correlation with ferritin | R = 0.697 p = 0.006 | R = −0.341 p = 0.233 | R = −0.393 p = 0.164 | |
| DFP therapy (N = 15) | ||||
| Mean value | 838.67 ± 612.19 ng/mL | 5.08 ± 4.17 mg/g dw | 8.37 ± 6.49 ms | 40.48 ± 4.79 ms |
| Correlation with ferritin | R = 0.463 p = 0.082 | R = 0.297 p = 0.282 | R = 0.145 p = 0.606 | |
| DFX therapy (N = 32) | ||||
| Mean value | 875.06 ± 468.48 ng/mL | 4.12 ± 5.52 mg/g dw | 13.74 ± 10.64 ms | 38.44 ± 9.54 ms |
| Correlation with ferritin | R = 0.491 p = 0.004 | R = −0.092 p = 0.623 | R = −0.243 p = 0.181 | |
| Sequential or combined DFO/DFP (N = 21) | ||||
| Mean value | 863.57 ± 510.39 ng/mL | 3.10 ± 2.20 mg/g dw | 7.47 ± 4.43 ms | 37.09 ± 11.09 ms |
| Correlation with ferritin | R = 0.443 p = 0.044 | R = 0.045 p = 0.847 | R = −0.622 p = 0.003 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spasiano, A.; Meloni, A.; Costantini, S.; Quaia, E.; Cademartiri, F.; Cinque, P.; Pepe, A.; Ricchi, P. Setting for “Normal” Serum Ferritin Levels in Patients with Transfusion-Dependent Thalassemia: Our Current Strategy. J. Clin. Med. 2021, 10, 5985. https://doi.org/10.3390/jcm10245985
Spasiano A, Meloni A, Costantini S, Quaia E, Cademartiri F, Cinque P, Pepe A, Ricchi P. Setting for “Normal” Serum Ferritin Levels in Patients with Transfusion-Dependent Thalassemia: Our Current Strategy. Journal of Clinical Medicine. 2021; 10(24):5985. https://doi.org/10.3390/jcm10245985
Chicago/Turabian StyleSpasiano, Anna, Antonella Meloni, Silvia Costantini, Emilio Quaia, Filippo Cademartiri, Patrizia Cinque, Alessia Pepe, and Paolo Ricchi. 2021. "Setting for “Normal” Serum Ferritin Levels in Patients with Transfusion-Dependent Thalassemia: Our Current Strategy" Journal of Clinical Medicine 10, no. 24: 5985. https://doi.org/10.3390/jcm10245985
APA StyleSpasiano, A., Meloni, A., Costantini, S., Quaia, E., Cademartiri, F., Cinque, P., Pepe, A., & Ricchi, P. (2021). Setting for “Normal” Serum Ferritin Levels in Patients with Transfusion-Dependent Thalassemia: Our Current Strategy. Journal of Clinical Medicine, 10(24), 5985. https://doi.org/10.3390/jcm10245985