
Real-World Rates of Bleeding, Factor VIII Use, and Quality of Life in Individuals with Severe Haemophilia A Receiving Prophylaxis in a Prospective, Noninterventional Study

 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
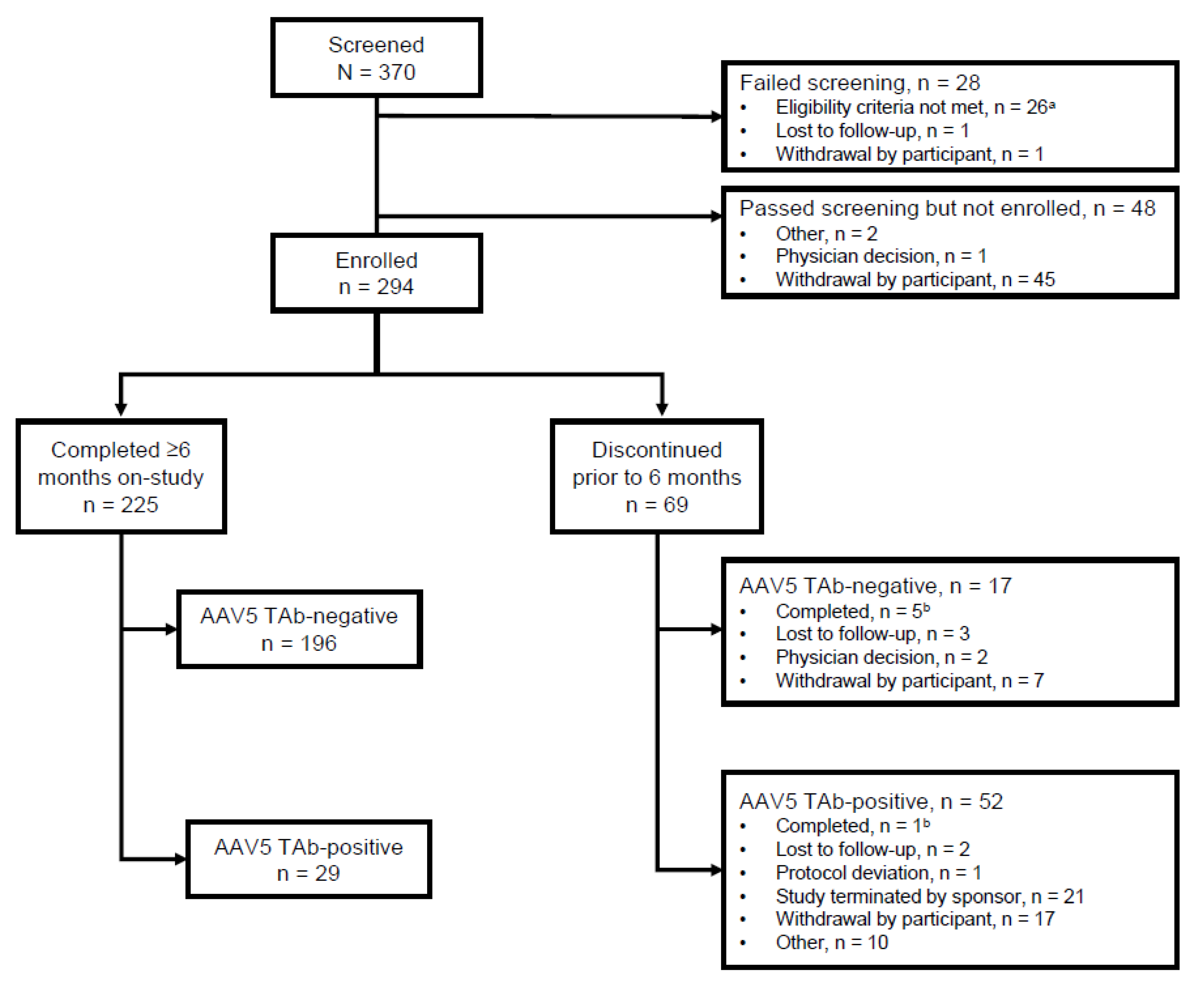
2.1. Study Design and Participants
2.2. Study Assessments and Endpoints
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical Endpoints
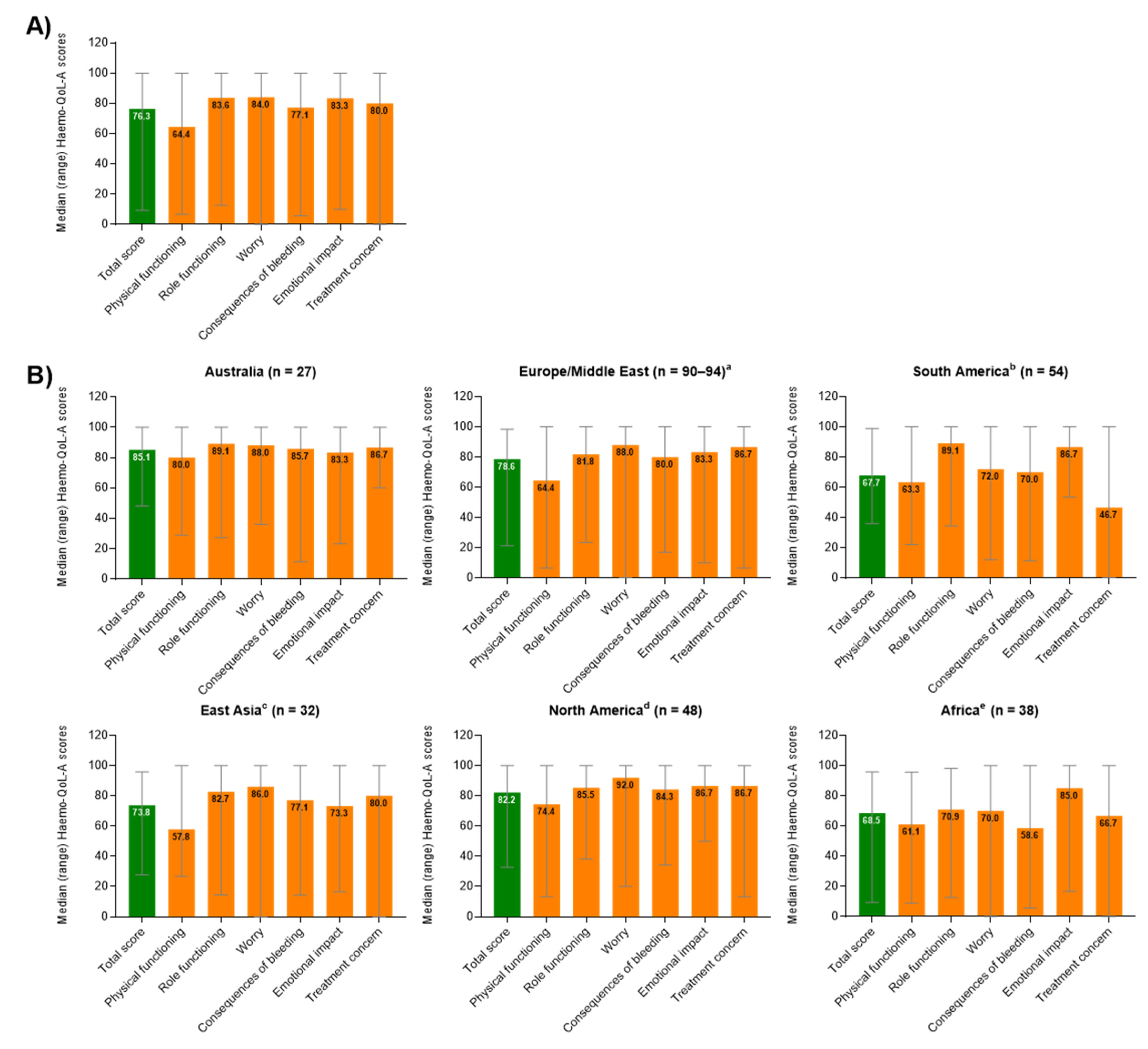
3.3. Patient-Reported Outcomes
3.4. Comparative Analysis among Trial Sites by Region
3.5. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iorio, A.; Stonebraker, J.S.; Chambost, H.; Makris, M.; Coffin, D.; Herr, C.; Germini, F. Establishing the Prevalence and Prevalence at Birth of Hemophilia in Males: A Meta-analytic Approach Using National Registries. Ann. Intern. Med. 2019, 171, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Blanchette, V.S.; Key, N.S.; Ljung, L.R.; Manco-Johnson, M.J.; Van Den Berg, H.M.; Srivastava, A. Definitions in hemophilia: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2014, 12, 1935–1939. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.; Santagostino, E.; Dougall, A.; Kitchen, S.; Sutherland, M.; Pipe, S.W.; Carcao, M.; Mahlangu, J.; Ragni, M.V.; Windyga, J.; et al. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia 2020, 26 (Suppl. 6), 1–158. [Google Scholar] [CrossRef] [PubMed]
- Berntorp, E.; Dolan, G.; Hay, C.; Linari, S.; Santagostino, E.; Tosetto, A.; Castaman, G.; Álvarez-Román, M.; Lopez, R.P.; Oldenburg, J.; et al. European retrospective study of real-life haemophilia treatment. Haemophilia 2017, 23, 105–114. [Google Scholar] [CrossRef]
- Stonebraker, J.S.; Brooker, M.; Amand, R.E.; Farrugia, A.; Srivastava, A. A study of reported factor VIII use around the world. Haemophilia 2010, 16, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Manco-Johnson, M.J.; Soucie, J.M.; Gill, J.C. Joint Outcomes Committee of the Universal Data Collection USHTCN. Prophylaxis usage, bleeding rates, and joint outcomes of hemophilia, 1999 to 2010: A surveillance project. Blood 2017, 129, 2368–2374. [Google Scholar] [CrossRef] [PubMed]
- Bulcha, J.T.; Wang, Y.; Ma, H.; Tai, P.W.L.; Gao, G. Viral vector platforms within the gene therapy landscape. Signal Transduct. Target. Ther. 2021, 6, 53. [Google Scholar] [CrossRef]
- Rentz, A.; Flood, E.; Altisent, C.; Bullinger, M.; Klamroth, R.; Garrido, R.P.; Scharrer, I.; Schramm, W.; Gorina, E.; The Members of the Haemo-QoL-A Steering Committee. Cross-cultural development and psychometric evaluation of a patient-reported health-related quality of life questionnaire for adults with haemophilia. Haemophilia 2008, 14, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Haemo-QoL Study Group. Scoring Manual. Available online: http://haemoqol.de/scoring/manual/ (accessed on 15 December 2020).
- The EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Brooks, R.; EuroQol Group. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- van Genderen, F.R.; Westers, P.; Heijnen, L.; de Kleijn, P.; van den Berg, H.M.; Helders, P.J.M.; van Meeteren, N.L.U. Measuring patients’ perceptions on their functional abilities: Validation of the Haemophilia Activities List. Haemophilia 2006, 12, 36–46. [Google Scholar] [CrossRef]
- Recht, M.; Neufeld, E.J.; Sharma, V.R.; Solem, C.T.; Pickard, A.S.; Gut, R.Z.; Cooper, D.L. Impact of Acute Bleeding on Daily Activities of Patients with Congenital Hemophilia with Inhibitors and Their Caregivers and Families: Observations from the Dosing Observational Study in Hemophilia (DOSE). Value Health 2014, 17, 744–748. [Google Scholar] [CrossRef] [PubMed]
- Reilly Associates. WPAI Scoring. Available online: http://www.reillyassociates.net/WPAI_Scoring.html (accessed on 15 December 2020).
- McLaughlin, P.; Hermans, C.; Asghar, S.; Burke, T.; Nissen, F.; Aizenas, M.; Meier, O.; Dhillon, H.; O’Hara, J. Problem Joints and Their Clinical and Humanistic Burden in Children and Adults with Moderate and Severe Hemophilia a: CHESS Paediatrics and CHESS II [abstract]. Blood 2020, 136 (Suppl. 1), 33–34. [Google Scholar] [CrossRef]
- Burke, T.; Santana, I.R.; Chowdary, P.; Curtis, R.; Khair, K.; Laffan, M.; McLaughin, P.; Noone, D.; O’Mahony, B.; Pasi, J. Examination and Validation of a Patient-centric Joint Metric: “Problem Joint”; Empirical Evidence from the CHESS Paediatrics Dataset [abstract]. Res. Pract. Thromb. Haemost. 2021, 5 (Suppl. 1), 5–6. [Google Scholar]
- Burke, T.; Santana, I.R.; Chowdary, P.; Curtis, R.; Khair, K.; Laffan, M.; McLaughin, P.; Noone, D.; O’Mahony, B.; Pasi, J. Examination and Validation of a Patient-Centric Joint Metric: “Problem Joint”; Empirical Evidence from the CHESS US Dataset [abstract]. Blood 2020, 136 (Suppl. 1), 25–26. [Google Scholar] [CrossRef]
- Kruse-Jarres, R.; Oldenburg, J.; Santagostino, E.; Shima, M.; Kempton, C.L.; Kessler, C.M.; Lehle, M.; Chebon, S.; Bienz, N.S.; Asikanius, E.; et al. Bleeding and safety outcomes in persons with haemophilia A without in-hibitors: Results from a prospective non-interventional study in a real-world setting. Haemophilia 2019, 25, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; McIntosh, K.A.; Squire, S.J.; Yang, M.; Bartholomew, C.; Gue, D.S.; Camp, P.G.; Jackson, S.C. Patient powered prophylaxis: A 12-month study of individualized prophylaxis in adults with severe haemophilia A. Haemophilia 2017, 23, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Ay, C.; Perschy, L.; Rejtö, J.; Kaider, A.; Pabinger, I. Treatment patterns and bleeding outcomes in persons with severe hemophilia A and B in a real-world setting. Ann. Hematol. 2020, 99, 2763–2771. [Google Scholar] [CrossRef] [PubMed]
- Manco-Johnson, M.J.; Sanders, J.; Ewing, N.; Rodriguez, N.; Tarantino, M.; Humphries, T.; TEEN/TWEN Study Group. Consequences of switching from prophylactic treatment to on-demand treatment in late teens and early adults with severe haemophilia A: The TEEN/TWEN study. Haemophilia 2013, 19, 727–735. [Google Scholar] [CrossRef] [PubMed]
- St-Louis, J.; Urajnik, D.J.; Ménard, F.; Cloutier, S.; Klaassen, R.J.; Ritchie, B.; Rivard, G.E.; Warner, M.; Blanchette, V.; Young, N. Generic and disease-specific quality of life among youth and young men with Hemophilia in Canada. BMC Hematol. 2016, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Room, J.; Barker, K. Physical activity levels in men with Haemophilia—A single centre UK survey. Haemophilia 2020, 26, 718–725. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, J.; Martin, A.P.; Nugent, D.; Witkop, M.; Buckner, T.W.; Skinner, M.W.; O’Mahony, B.; Mulhern, B.; Morgan, G.; Li, N.; et al. Evidence of a disability paradox in patient-reported outcomes in haemophilia. Haemophilia 2021, 27, 245–252. [Google Scholar] [CrossRef]
- Di Minno, G.; Santagostino, E.; Morfini, M.; Ettorre, C.; Cultrera, D.; Baldacci, E.; Russo, E.; Gallucci, C. Patient satisfaction and acceptability of an on-demand and on-prophylaxis device for factor VIII delivery in patients with hemophilia A. Patient Prefer. Adherence 2019, 13, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Stonebraker, J.S.; Bolton-Maggs, P.H.B.; Brooker, M.; Evatt, B.; Iorio, A.; Makris, M.; O’Mahony, B.; Skinner, M.W.; Coffin, D.; Pierce, G.F.; et al. The World Federation of Hemophilia Annual Global Survey 1999–2018. Haemophilia 2020, 26, 591–600. [Google Scholar] [CrossRef]
- Bleeding disorders: Making strides towards treatment for all. Lancet Haematol. 2020, 7, E551. [CrossRef]
- Guedes, V.G.; Thomas, S.; Wachholz, P.A.; Souza, S.A.L. Challenges and perspectives in the treatment of patients with haemophilia in Brasil. Rev. Assoc. Med. Bras. (1992) 2018, 64, 872–875. [Google Scholar] [CrossRef]
- Manco-Johnson, M.J.; Lundin, B.; Funk, S.; Peterfy, C.; Raunig, D.; Werk, M.; Kempton, C.L.; Reding, M.T.; Goranov, S.; Gercheva, L.; et al. Effect of late prophylaxis in hemophilia on joint status: A randomized trial. J. Thromb. Haemost. 2017, 15, 2115–2124. [Google Scholar] [CrossRef] [PubMed]
- Diop, S.; Haffar, A.; Mahlangu, J.; Chami, I.; Kitchen, S.; Pierce, G. Improving access to hemophilia care in sub-Saharan Africa by capacity building. Blood Adv. 2019, 3 (Suppl. 1), 1–4. [Google Scholar] [CrossRef] [PubMed]
- Lambert, C.; Meité, N.; Sanogo, I.; Lobet, S.; Adjambri, E.; Eeckhoudt, S.; Hermans, C. Haemophilia in Côte d’Ivoire (the Ivory Coast) in 2017: Extensive data collection as part of the World Federation of Hemophilia’s twinning programme. Haemophilia 2019, 25, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Brennan, Y.; Parikh, S.; McRae, S.; Tran, H. The Australian experience with switching to extended half-life factor VIII and IX concentrates: On behalf of the Australian Haemophilia Centre Directors’ Organisation. Haemophilia 2020, 26, 529–535. [Google Scholar] [CrossRef]
- Guedes, V.G.; Thomas, S.; Farrugia, A.; Wachholz, P.A.; Souza, S.A.L. Perspectives on haemophilia access in Brazil? Haemophilia 2018, 24, e255–e256. [Google Scholar] [CrossRef] [PubMed]
- Mahlangu, J.N.; Naidoo, Y.; Goga, Y.; Vaithlingum, M.; Joubert, J.; Sutton, C.; Potgieter, J.; Cruickshank, A.-L.; Iorio, A. Home therapy for inherited bleeding disorders in South Africa: Results of a modified Delphi consensus process. S. Afr. Med. J. 2019, 109, 639–644. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Kasthuri, R.; Kruse-Jarres, R.; Soni, A.; Kulkarni, R.; Bidlingmaier, C.; Chitlur, M.; Fogarty, P.; Gomez, K.; Holm, P.A.; et al. Global Emerging HEmophilia Panel (GEHEP): A Multinational Collaboration for Advancing Hemophilia Research and Treatment. Transfus. Med. Hemother. 2013, 40, 352–355. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Benbouzid, A.; Belhani, M.; El Andaloussi, M.; Maani, K.; Wali, Y.; El Fegoun, S.B.; Saad, H.A.; Mahlangu, J. HAEMOcare: The First International Epidemiological Study Measuring Burden of Hemophilia in Developing Countries. TH Open 2019, 3, e190–e199. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, B.; Black, C. Expanding Hemophilia Care in Developing Countries. Semin. Thromb. Hemost. 2005, 31, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Nolan, B.; Mahlangu, J.; Perry, D.; Young, G.; Liesner, R.; Konkle, B.; Rangarajan, S.; Brown, S.; Hanabusa, H.; Pasi, K.J.; et al. Long-term safety and efficacy of recombinant factor VIII Fc fusion protein (rFVIIIFc) in subjects with haemophilia A. Haemophilia 2016, 22, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.D.; Schoenig-Diesing, C.; Silvati-Fidell, L.; Wong, W.Y.; Romanov, V. Integrated analysis of safety data from 12 clinical interventional studies of plasma- and albumin-free recombinant factor VIII (rAHF-PFM) in haemophilia A. Haemophilia 2015, 21, 791–798. [Google Scholar] [CrossRef][Green Version]



{kind=link}
{kind=link}
| Parameter | Australia (n = 27) | Europe/ Middle East a (n = 95) | South America b (n = 54) | East Asia c (n = 32) | North America d (n = 48) | Africa e (n = 38) | Overall Enrolled Population (N = 294) |
|---|---|---|---|---|---|---|---|
| Age at enrolment, median (min, max) years | 31.0 (18.0, 71.0) | 33.0 (18.0, 70.0) | 27.0 (18.0, 47.0) | 40.0 (20.0, 66.0) | 32.0 (19.0, 70.0) | 28.0 (18.0, 67.0) | 31.0 (18.0, 71.0) |
| Male sex, n (%) | 27 (100.0) | 95 (100.0) | 54 (100.0) | 32 (100.0) | 48 (100.0) | 38 (100.0) | 294 (100.0) |
| Race, n (%) | |||||||
| Asian | 2 (7.4) | 6 (6.3) | 0 | 32 (100.0) | 2 (4.2) | 0 | 42 (14.3) |
| Black or African American | 0 | 1 (1.1) | 10 (18.5) | 0 | 5 (10.4) | 14 (36.8) | 30 (10.2) |
| White | 24 (88.9) | 65 (68.4) | 44 (81.5) | 0 | 39 (81.3) | 13 (34.2) | 185 (62.9) |
| Other | 1 (3.7) | 0 | 0 | 0 | 0 | 0 | 1 (0.3) |
| Not provided f | 0 | 23 (24.2) | 0 | 0 | 2 (4.2) | 11 (28.9) | 36 (12.2) |
| Hispanic or Latino ethnicity | 1 (3.7) | 2 (2.1) | 0 | 0 | 1 (2.1) | 0 | 4 (1.4) |
| Weight, mean (SD), kg | 83.3 (18.1) | 77.4 (14.9) | 78.9 (20.4) | 61.8 (11.0) | 84.5 (19.6) | 67.9 (18.7) | 79.0 (18.1) |
| History of hepatitis B g, n (%) | 3 (11.1) | 20 (21.1) | 1 (1.9) | 8 (25.0) | 7 (14.6) | 5 (13.2) | 44 (15.0) |
| History of hepatitis C g, n (%) | 12 (44.4) | 43 (45.3) | 12 (22.2) | 20 (62.5) | 24 (50.0) | 7 (18.4) | 118 (40.1) |
| History of HIV, n (%) | 0 | 4 (4.2) | 0 | 0 | 6 (12.5) | 0 | 10 (3.4) |
| Participants with problem joints h, n (%) | 9 (33.3) | 42 (44.2) | 5 (9.3) | 18 (56.3) | 20 (41.7) | 7 (18.4) | 101 (34.4) |
| Number of problem joints h, n (%) | |||||||
| 0 | 18 (66.7) | 53 (55.8) | 49 (90.7) | 14 (43.8) | 28 (58.3) | 31 (81.6) | 193 (65.6) |
| 1 | 3 (11.1) | 14 (14.7) | 5 (9.3) | 11 (34.4) | 6 (12.5) | 6 (15.8) | 45 (15.3) |
| 2 | 3 (11.1) | 9 (9.5) | 0 | 5 (15.6) | 3 (6.3) | 1 (2.6) | 21 (7.1) |
| 3 | 2 (7.4) | 8 (8.4) | 0 | 2 (6.3) | 4 (8.3) | 0 | 16 (5.4) |
| >3 | 1 (3.7) | 11 (11.6) | 0 | 0 | 7 (14.6) | 0 | 19 (6.5) |
| Pre-Baseline n = 225 | On-Study n = 224 | Total Duration n = 224 | |
|---|---|---|---|
| Annualised bleed rate, no. of bleeds/year | |||
| All bleeds | |||
| Mean (SD) | 5.34 (10.1) | 4.81 (6.83) | 5.04 (7.53) |
| Median (range) | 2.00 (0.0, 94.0) | 2.05 (0.0, 37.8) | 2.61 (0.0, 62.7) |
| Treated bleeds | |||
| Mean (SD) | 5.03 (9.35) | 4.33 (6.39) | 4.64 (7.00) |
| Median (range) | 2.00 (0.0, 86.0) | 1.85 (0.0, 37.8) | 2.27 (0.0, 57.8) |
| Treated spontaneous bleeds | |||
| Mean (SD) | 2.98 (6.02) | 1.93 (3.81) | 2.35 (4.14) |
| Median (range) | 0.00 (0.0, 58.0) | 0.00 (0.0, 25.2) | 0.94 (0.0, 39.3) |
| Treated traumatic bleeds | |||
| Mean (SD) | 2.05 (6.81) | 2.40 (4.58) | 2.29 (5.02) |
| Median (range) | 0.00 (0.0, 86.0) | 0.00 (0.0, 31.2) | 0.88 (0.0, 55.9) |
| Treated joint bleeds | |||
| Mean (SD) | 3.74 (7.67) | 2.74 (4.68) | 3.19 (5.41) |
| Median (range) | 2.00 (0.0, 72.0) | 1.21 (0.0, 25.5) | 1.44 (0.0, 47.0) |
| Treated problem joint bleeds | |||
| Mean (SD) | 1.22 (3.69) | 0.66 (2.22) | 0.91 (2.63) |
| Median (range) | 0.00 (0.0, 32.0) | 0.00 (0.0, 20.0) | 0.00 (0.0, 21.4) |
| Pre-Baseline | On-Study | Total Duration | |
|---|---|---|---|
| Mean (SD) annualised FVIII utilisation rate, IU/kg/year | |||
| n | 223 | 222 | 222 |
| All uses | 3937.9 (1799.7) | 3927.7 (1768.1) | 3928.5 (1698.2) |
| Subtypes of usage | |||
| Bleeds | 261.9 (489.0) | 186.7 (287.4) | 219.2 (330.7) |
| Surgery/procedures | 67.1 (411.4) | 57.5 (202.7) | 62.6 (222.1) |
| One-time prophylaxis a | 32.9 (154.6) | 19.2 (68.9) | 25.5 (82.0) |
| Usual prophylaxis b | 3575.9 (1756.9) | 3664.3 (1685.4) | 3621.2 (1637.8) |
| Mean (SD) annualised FVIII infusion rate, no. of infusions/year | |||
| n | 225 | 224 | 224 |
| All uses | 130.5 (45.2) | 131.5 (48.5) | 131.1 (45.2) |
| Subtypes of usage | |||
| Bleeds | 8.19 (15.6) | 5.99 (8.91) | 6.94 (10.3) |
| Surgery/procedures | 1.75 (9.78) | 1.72 (7.12) | 1.77 (6.15) |
| One-time prophylaxis a | 0.96 (4.61) | 0.51 (1.82) | 0.71 (2.34) |
| Usual prophylaxis b | 119.6 (46.8) | 123.3 (48.5) | 121.6 (46.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kenet, G.; Chen, Y.-C.; Lowe, G.; Percy, C.; Tran, H.; von Drygalski, A.; Trossaërt, M.; Reding, M.; Oldenburg, J.; Mingot-Castellano, M.E.; et al. Real-World Rates of Bleeding, Factor VIII Use, and Quality of Life in Individuals with Severe Haemophilia A Receiving Prophylaxis in a Prospective, Noninterventional Study. J. Clin. Med. 2021, 10, 5959. https://doi.org/10.3390/jcm10245959
Kenet G, Chen Y-C, Lowe G, Percy C, Tran H, von Drygalski A, Trossaërt M, Reding M, Oldenburg J, Mingot-Castellano ME, et al. Real-World Rates of Bleeding, Factor VIII Use, and Quality of Life in Individuals with Severe Haemophilia A Receiving Prophylaxis in a Prospective, Noninterventional Study. Journal of Clinical Medicine. 2021; 10(24):5959. https://doi.org/10.3390/jcm10245959
Chicago/Turabian StyleKenet, Gili, Yeu-Chin Chen, Gillian Lowe, Charles Percy, Huyen Tran, Annette von Drygalski, Marc Trossaërt, Mark Reding, Johannes Oldenburg, Maria Eva Mingot-Castellano, and et al. 2021. "Real-World Rates of Bleeding, Factor VIII Use, and Quality of Life in Individuals with Severe Haemophilia A Receiving Prophylaxis in a Prospective, Noninterventional Study" Journal of Clinical Medicine 10, no. 24: 5959. https://doi.org/10.3390/jcm10245959
APA StyleKenet, G., Chen, Y.-C., Lowe, G., Percy, C., Tran, H., von Drygalski, A., Trossaërt, M., Reding, M., Oldenburg, J., Mingot-Castellano, M. E., Park, Y.-S., Peyvandi, F., Ozelo, M. C., Mahlangu, J., Quinn, J., Huang, M., Reddy, D. B., & Kim, B. (2021). Real-World Rates of Bleeding, Factor VIII Use, and Quality of Life in Individuals with Severe Haemophilia A Receiving Prophylaxis in a Prospective, Noninterventional Study. Journal of Clinical Medicine, 10(24), 5959. https://doi.org/10.3390/jcm10245959