
Dehydration before Major Urological Surgery and the Perioperative Pattern of Plasma Creatinine: A Prospective Cohort Series

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Approvals
2.2. Study Population and Design
2.3. Outcome Measures
2.4. Data Collection and Laboratory Tests
2.5. Perioperative Management
2.6. Statistical Analysis
3. Results
3.1. Dehydration
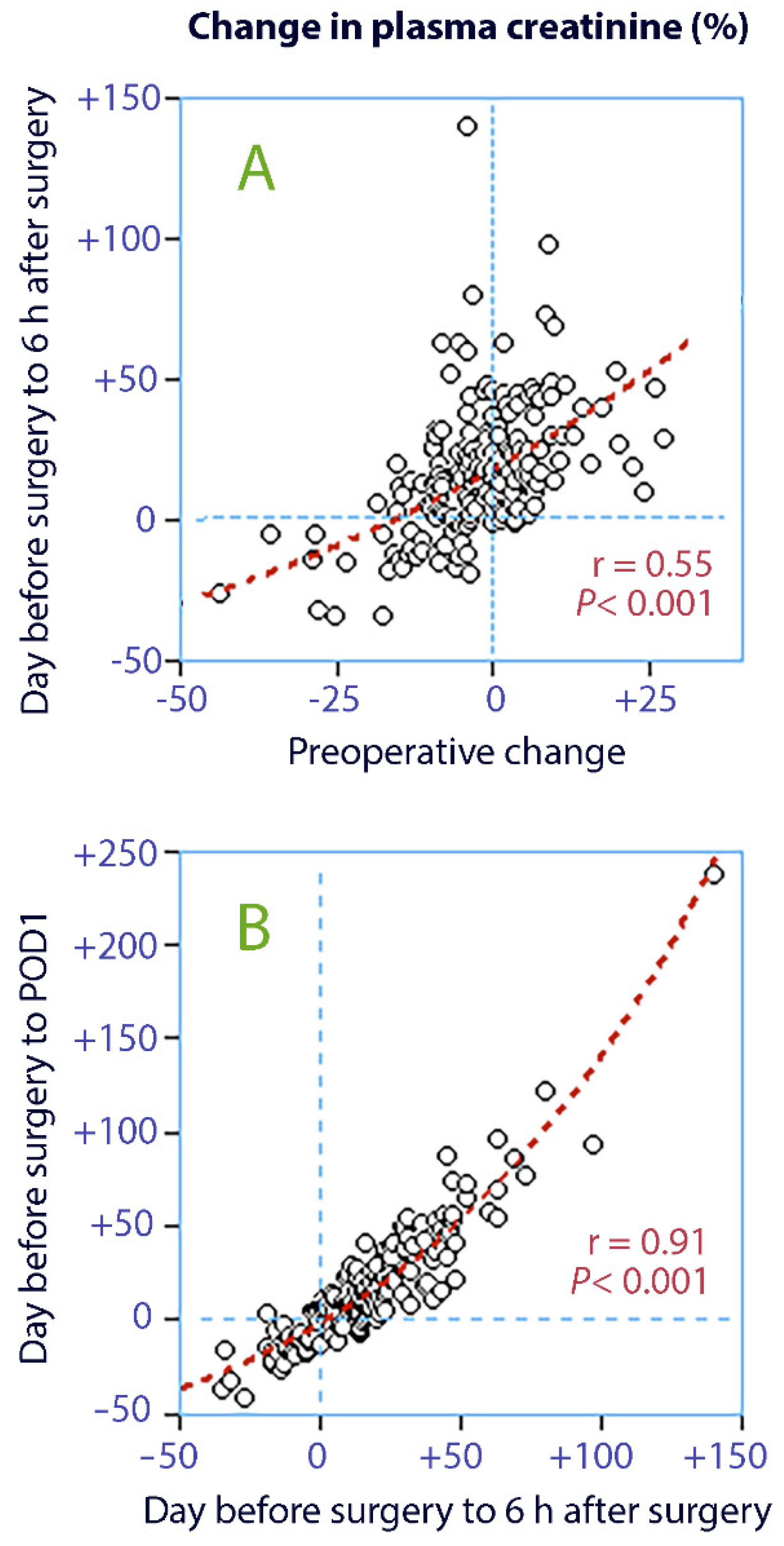
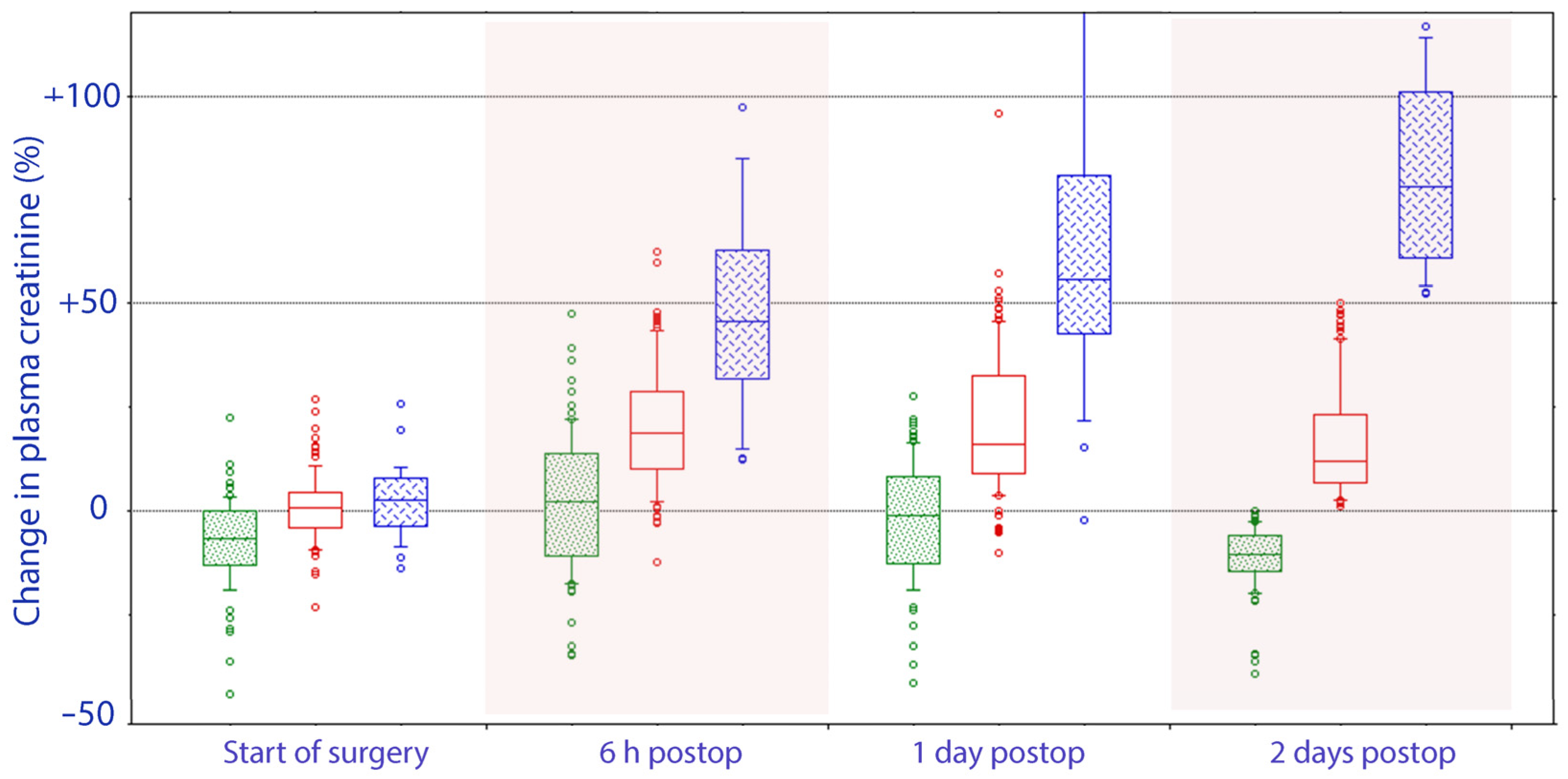
3.2. Trajectory of Plasma Creatinine
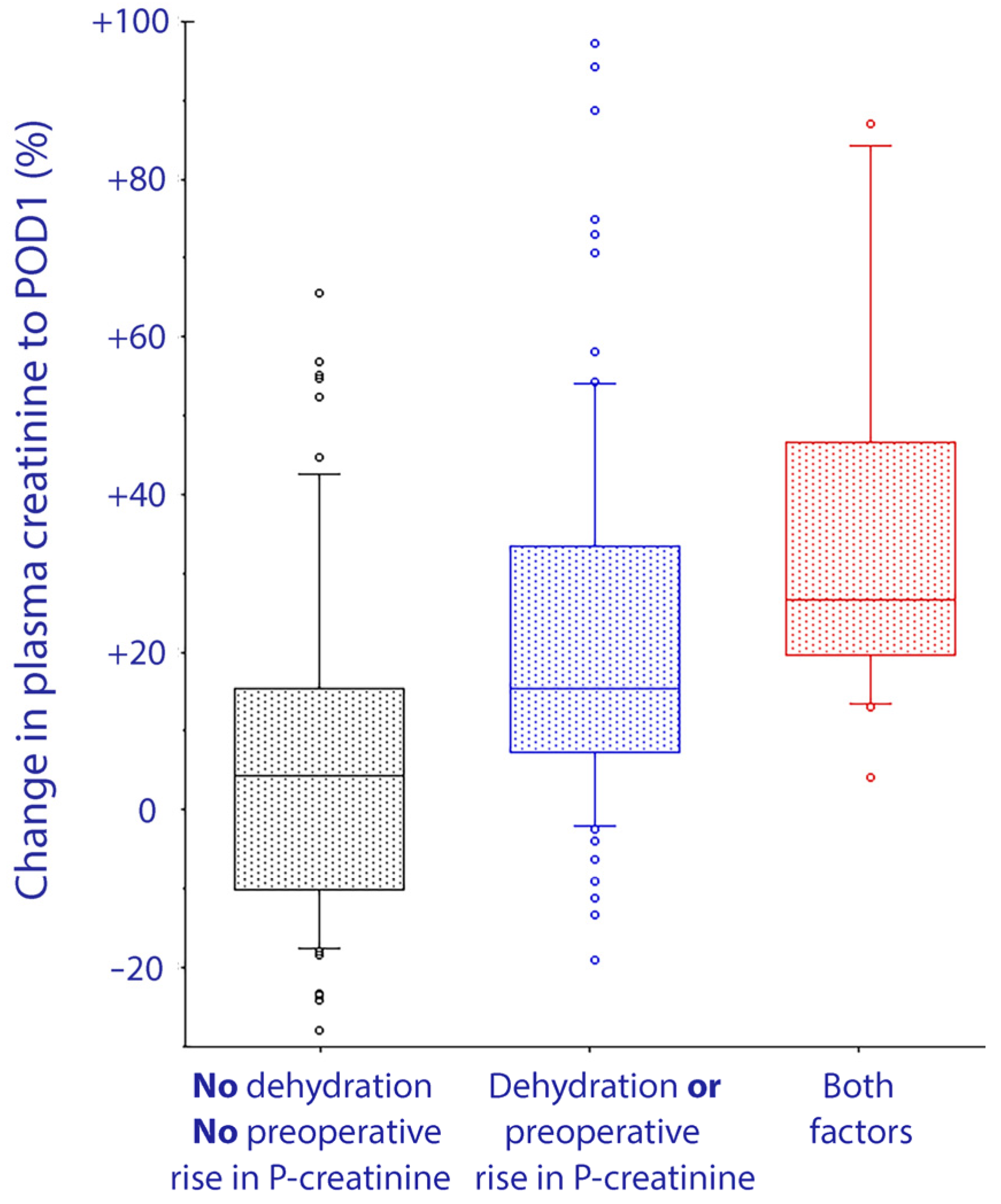
3.3. Risk Factors for Plasma Creatinine Elevation
4. Discussion
4.1. Key Results
4.2. Interpretation
4.3. Literature
4.4. Future Views
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Definitions of Postoperative Complications/Events
Appendix A.1. Gastrointestinal Complications
- Ileus: no evidence of bowel function (no flatus and no passage of stool) with abdominal distension requiring cessation of oral intake and intravenous fluid support by POD 5;
- Constipation: no passage of stool without signs of ileus by POD 5;
- Gastric ulcer: diagnosis made by gastroscopy;
- Anastomotic bowel leak: considered as a complication if requiring surgery or prolonged drainage.
Appendix A.2. Complications of Infections
- Urinary tract infection: temperature >38 °C in the last 24 h and leukocytosis and a prompted urinary analysis that showed bacterial counts >100,000 requiring antibiotics;
- Sepsis: bacterial infection and at least two of the following clinical signs: hypo- or hyperthermia, tachycardia, tachypnea, leukocytopenia or leukocytosis, positive blood culture;
- Pneumonia: temperature >38 °C and leukocytosis and clinical signs of pneumonia, requiring antibiotics;
- Wound infection: pus can be expressed or aspirated, requiring surgical intervention.
Appendix A.3. Wound Complications
- Wound dehiscence: diagnosed clinically and requiring resuturing.
Appendix A.4. Cardiac Events
- Myocardial infarction: increase of the enzyme high-sensitive troponin T above the hospital laboratory’s myocardial infarction threshold (>0.05 µg/L), and either new Q wave changes, or persistent changes in ST-T segments;
- Arrhythmia: confirmed by 12-lead electrocardiography and requiring new medication or electroconversion;
- Congestive heart failure and pulmonary edema: shortness of breath, rales, jugular venous distension, peripheral edema, third heart sound, radiologic signs (cardiomegaly, interstitial or alveolar edema), brain natriuretic peptide value >500 pg/mL and diagnosis requiring diuretics;
- Transient brain natriuretic peptide increase: postoperative serum brain natriuretic peptide values between 100 and 500 pg/mL (considered as minor cardiac event).
Appendix A.5. Thromboembolic Complications
- Pulmonary embolism: evidenced by spiral computerized tomography scanning.
Appendix A.6. Genitourinary Complications
- Renal dysfunction: transient increase of creatinine: creatinine >50% upper limit of normal value;
- Renal failure: severe reduction in glomerular filtration rate (15–29 mL·min−1 × 1.73 m−2) at discharge;
- Urinary leakage: radiologically diagnosed, requiring stenting.
Appendix A.7. Neurological Complications
- Presence of a new focal deficit, confusion/delirium.
References
- Apfel, C.C.; Meyer, A.; Orhan-Sungur, M.; Jalota, L.; Whelan, R.P.; Jukar-Rao, S. Supplemental intravenous crystalloids for the prevention of postoperative nausea and vomiting: Quantitative review. Br. J. Anaesth. 2012, 108, 893–902. [Google Scholar] [CrossRef] [Green Version]
- Cheuvront, S.N.; Kenefick, R.W. Dehydration: Physiology, assessment, and performance effects. Compr. Physiol. 2014, 4, 257–285. [Google Scholar] [PubMed]
- Casa, D.J.; Armstrong, L.E.; Hillman, S.K.; Montain, S.J.; Reiff, R.V.; Rich, B.S.; Roberts, W.O.; Stone, J.A. National athletic trainers’ association position statement: Fluid replacement for athletes. J. Athl. Train. 2000, 35, 212–224. [Google Scholar] [PubMed]
- Hahn, R.G.; Waldreus, N. An aggregate urine analysis tool to detect acute dehydration. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 303–311. [Google Scholar] [CrossRef]
- Ylinenvaara, S.I.; Elisson, O.; Berg, K.; Zdolsek, J.H.; Krook, H.; Hahn, R.G. Preoperative urine-specific gravity and the incidence of complications after hip fracture surgery: A prospective, observational study. Eur. J. Anaesthesiol. 2014, 31, 85–90. [Google Scholar] [CrossRef]
- Hahn, R.G.; Bahlmann, H.; Nilsson, L. Dehydration and fluid volume kinetics before major open abdominal surgery. Acta Anaesthesiol. Scand. 2014, 58, 1258–1266. [Google Scholar] [CrossRef]
- Hahn, R.G. Renal injury during hip fracture surgery: An exploratory study. Anaesthesiol. Intensive Ther. 2015, 47, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Wuethrich, P.Y.; Burkhard, F.C.; Thalmann, G.N.; Stueber, F.; Studer, U.E. Restrictive deferred hydration combined with preemptive norepinephrine infusion during radical cystectomy reduces postoperative complications and hospitalization time: A randomized clinical trial. Anesthesiology 2014, 120, 365–377. [Google Scholar] [CrossRef] [Green Version]
- Bleier, J.I.; Aarons, C.B. Perioperative fluid restriction. Clin. Colon. Rectal Surg. 2013, 26, 197–202. [Google Scholar]
- McCaul, C.; Moran, C.; O’Cronin, D.; Naughton, F.; Geary, M.; Carton, E.; Gardiner, J. Intravenous fluid loading with or without supplementary dextrose does not prevent nausea, vomiting and pain after laparoscopy. Can. J. Anesth. 2003, 50, 440–444. [Google Scholar] [CrossRef]
- Hahn, R.G.; Grankvist, N.; Krizhanovskii, C. Urinary analysis of fluid retention in the general population: A cross-sectional study. PLoS ONE 2016, 11, e0164152. [Google Scholar] [CrossRef]
- Stark, P.A.; Myles, P.S.; Burke, J.A. Development and psychometric evaluation of a postoperative quality of recovery score: The, QoR-15. Anesthesiology 2013, 118, 1332–1340. [Google Scholar] [CrossRef] [Green Version]
- Bennett-Guerrero, E.; Welsby, I.; Dunn, T.J.; Young, L.R.; Wahl, T.A.; Diers, T.L.; Phillips-Bute, B.G.; Newman, M.F.; Mythen, M.G. The use of a postoperative morbidity survey to evaluate patients with prolonged hospitalization after routine, moderate-risk, elective surgery. Anesth. Analg. 1999, 89, 514–519. [Google Scholar] [CrossRef] [Green Version]
- Loffel, L.M.; Kleeb, B.; Burkhard, F.C.; Wuethrich, P.Y. Perioperative use of crystalloids in patients undergoing open radical cystectomy: Balanced, Ringer’s maleate versus a glucose 5%/potassium-based balanced solution: Study protocol for a randomized controlled trial. Trials 2014, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Loffel, L.M.; Burkhard, F.C.; Takala, J.; Wuethrich, P.Y. Impact of a potassium-enriched, chloride-depleted 5% glucose solution on gastrointestinal function after major abdominopelvic surgery: Sesults of a randomized controlled trial. Anesthesiology 2016, 125, 678–689. [Google Scholar] [CrossRef]
- Gan, T.J.; Diemunsch, P.; Habib, A.S.; Kovac, A.; Kranke, P.; Meyer, T.A.; Watcha, M.; Chung, F.; Angus, S.A.A.-C.; Apfel, C.C.; et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth. Analg. 2014, 118, 85–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apfel, C.C.; Laara, E.; Koivuranta, M.; Greim, C.A.; Roewer, N. A simplified risk score for predicting postoperative nausea and vomiting: Conclusions from cross-validations between two centers. Anesthesiology 1999, 91, 693–700. [Google Scholar] [CrossRef] [Green Version]
- Wuethrich, P.Y.; Burkhard, F.C. Improved perioperative outcome with norepinephrine and a restrictive fluid administration during open radical cystectomy and urinary diversion. Urol. Oncol. 2015, 33, 66.e21. [Google Scholar] [CrossRef]
- Brunner, E.; Domhof, S.; Langer, F. Nonparametric, Analysis of Longitudinal, Data in Factorial, Experiments; Wiley: Hoboken, NJ, USA, 2002. [Google Scholar]
- Arnaud, M.J. Mild dehydration: A risk factor of constipation? Eur. J. Clin. Nutr. 2003, 57 (Suppl. 2), S88–S95. [Google Scholar] [CrossRef] [Green Version]
- Engel, D.; Loffel, L.M.; Wuethrich, P.Y.; Hahn, R.G. Preoperative concentrated urine increases the incidence of plasma creatinine elevation after major surgery. Front. Med. 2021, 8, 699969. [Google Scholar] [CrossRef] [PubMed]
- Ekman, L.; Johnson, P.; Hahn, R.G. Signs of Dehydration after Hip, Fracture Surgery: An, Observational Descriptive, Study. Medicina 2020, 56, 361. [Google Scholar] [CrossRef]
- Johnson, E.C.; Munoz, C.X.; Le Bellego, L.; Klein, A.; Casa, D.J.; Maresh, C.M.; Armstrong, L.E. Markers of the hydration process during fluid volume modification in women with habitual high or low daily fluid intakes. Eur. J. Appl. Physiol. 2015, 115, 1067–1074. [Google Scholar] [CrossRef]
- Johnson, P.; Waldreus, N.; Hahn, R.G.; Stenstrom, H.; Sjostrand, F. Fluid retention index predicts the 30-day mortality in geriatric care. Scand. J. Clin. Lab. Investig. 2015, 75, 444–451. [Google Scholar] [CrossRef]
- Hahn, R.G.; Zdolsek, M.; Hasselgren, E.; Zdolsek, J.; Bjorne, H. Fluid volume kinetics of 20% albumin. Br. J. Clin. Pharmacol. 2019, 85, 1303–1311. [Google Scholar] [CrossRef]
- Li, Y.; He, R.; Ying, X.; Hahn, R.G. Dehydration, hemodynamics and fluid volume optimization after induction of general anesthesia. Clinics 2014, 69, 809–816. [Google Scholar] [CrossRef]
- Brandstrup, B.; Møller, A.M. The, Challenge of Perioperative, Fluid Management in Elderly, Patients. Curr. Anesth. Rep. 2019, 9, 406–413. [Google Scholar] [CrossRef]
- Zarbock, A.; Koyner, J.L.; Hoste, E.A.J.; Kellum, J.A. Update on perioperative acute kidney injury. Anesth. Analg. 2018, 127, 1236–1245. [Google Scholar] [CrossRef]
- Bernardi, M.H.; Ristl, R.; Neugebauer, T.; Hiesmayr, M.J.; Druml, W.; Lassnigg, A. Very early changes in serum creatinine are associated with 30-day mortality after cardiac surgery. Eur. J. Anaesthesiol. 2020, 37, 898–907. [Google Scholar] [CrossRef]
- Furrer, M.A.; Schneider, M.P.; Löffel, L.M.; Buckhard, F.C.; Wuethrich, P.Y. Impact of intra-operative fluid and noradrenaline administration on early postoperative renal function after cystectomy and urinary diversion: A retrospective observational cohort study. Eur. J. Anaesthesiol. 2018, 35, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Loffel, L.M.; Bachmann, K.F.; Furrer, M.A.; Wuethrich, P.Y. Impact of intraoperative hypotension on early postoperative acute kidney injury in cystectomy patients—A retrospective cohort analysis. J. Clin. Anesth. 2020, 66, 109906. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Score | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Specific gravity | ≤1.005 | 1.010 | 1.015 | 1.020 | 1.025 | 1.030 |
| Osmolality (mOsmol/kg) | <250 | 250–450 | 450–600 | 600–800 | 800–1000 | >1000 |
| Creatinine (mmol/L) | <4 | 4–7 | 7–12 | 12–17 | 17–25 | >25 |
| Color (shade) | 1 | 2 | 3 | 4 | 5 | 6 |
| All Patients n = 181 | Dehydrated n = 37 | Hydrated n = 144 | p-Value | |
|---|---|---|---|---|
| Type of Surgery | ||||
| Prostate n (%) | 44 (24.3%) | 15 (40.5%) | 29 (20.1%) | 0.005 |
| Bladder n (%) | 50 (27.6%) | 3 (8.1%) | 47 (32.6%) | |
| Kidney n (%) | 51 (28.2%) | 11 (29.7%) | 40 (27.8%) | |
| Other n (%) | 36 (19.9%) | 8 (21.6%) | 28 (19.4%) | |
| Open/minimal invasive n (%) | 130 (72%)/51 (28%) | 23 (62%)/14 (38%) | 107 (74%)/ 37 (26%) | 0.22 |
| Age (years) | 65.0 (56.5–71.0) | 62.0 (51.0–68.0) | 65.5 (56.8–72.0) | 0.04 |
| BMI (kg/height2) | 26.9 (23.9–29.7) | 29.0 (24.2–32.5) | 26.6 (23.9–29.1) | 0.04 |
| ASA 1 n (%) | 9 (5%) | 3 (8.1%) | 6 (4.2%) | 0.16 |
| ASA 2 n (%) | 81 (44.8%) | 21 (56.8%) | 60 (41.7%) | |
| ASA 3 n (%) | 89 (49.2%) | 13 (35.1%) | 76 (52.8%) | |
| ASA 4 n (%) | 2 (1.1%) | 0 (0.0%) | 2 (1.4%) | |
| Ischemic heart disease n (%) | 26 (14.5%) | 3 (8.3%) | 23 (16.1%) ** | 0.30 |
| Hypertension n (%) | 86 (47.5%) | 19 (51.4%) | 67 (46.5%) | 0.71 |
| Diabetes mellitus n (%) | 18 (9.9%) | 5 (13.5%) | 13 (9.0%) | 0.54 |
| Smoking n (%) | 54 (31%) | 17 (45.9%) | 37 (25.6%) | 0.03 |
| GFR > 90 mL/min | 71 (39.7%) | 21 (56.8%) | 50 (35.2%) ** | <0.0001 |
| GFR 60–89 mL/min | 63 (35.2%) | 16 (43.2%) | 47 (33.1%) | |
| GFR < 60 mL/min | 45 (25.1%) | 0 (0.0%) | 45 (31.7%) | |
| Betablocker n (%) | 29 (16.2%) | 7 (18.9%) | 22 (15.5%) ** | 0.62 |
| Calcium antagonists n (%) | 79 (43.6%) | 16 43.2%) | 63 (43.8%) | 1.00 |
| Statins n (%) | 44 (24.3%) | 12 (32.4%) | 32 (22.2%) | 0.20 |
| Aspirin n (%) | 28 (15.6%) | 8 (21.6%) | 20 (14.0%) | 0.31 |
| Diuretics n (%) | 17 (9.4%) | 2 (5.4%) | 15 (10.5%) ** | 0.53 |
| Antidiabetics n (%) | 17 (9.6%) | 5 (13.5%) | 12 (8.5%) ** | 0.35 |
| Hemoglobin + (mmol/L) | 135 (122–144) | 140 (131–144) | 133 (118–143) ** | 0.01 |
| Osmolality + (mosmol/kg) | 288 (284–291) | 288 (285–290) | 288 (283–291) ** | 0.65 |
| Creatinine + (µmol/L) | 84 (70–96) | 73 (65–85) | 85.5 (72–102) * | 0.004 |
| Intraoperative Ringer lactated (mL) | 1300 (1050–2100) | 1800 (1100–2100) | 1300 (1025–2100) | 0.35 |
| Intraoperative Colloids (mL) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.29 |
| Intraoperative packed red blood cells (mL) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.34 |
| Intraoperative fresh frozen plasma (mL) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.21 |
| Blood Loss (mL) | 400 (200–700) | 400 (200–600) | 400 (200–750) | 0.90 |
| Fluid balance on -POD1 (kg) | 0.8 (−2.2–0.1) | 1.0 (−2.7–0.0) | 0.7 (−2.0–0.2) | 0.35 |
| All Patients | Dehydrated | Hydrated | p-Value | |
|---|---|---|---|---|
| n = 181 | n = 37 | n = 144 | ||
| Difference in QoR15 Scores | ||||
| A-Part (questions 1–10) | −25 (−34.0, −15.0) | −26 (−33.5, −16.0) | 24.5 (−35.8, −14.0) | 0.68 |
| B-Part (questions 11–15) | −1.0 (−6.0, 2.0) | −2.0 (−5.0, 0.5) | −1.0 (−6.8, 2.8) | 0.76 |
| Overall (questions 1–15) | −27.0 (−38.0, −14.0) | −28.0 (−36.0, −17.0) | −25.5 (−38.8, −13.0) | 0.55 |
| In-hospital complications | ||||
| Bennett-Guerrero Score | 1.0 (0.0, 1.0) | 1.0 (0.0, 1.0) | 1.0 (0.0, 1.0) | 0.18 |
| Cardiovascular Complications (%) | 5.0 (2.3, 9.2) | 2.7 (0.1, 14.2) | 5.6 (2.4, 10.7) | 0.69 |
| Pulmonary Complications (%) | 2.8 (0.9, 6.3) | 2.7 (0.1, 14.2) | 2.8 (0.8, 7.0) | 1.00 |
| Infections (%) | 11.6 (7.3, 17.2) | 5.4 (0.7, 18.2) | 13.2 (8.1, 19.8) | 0.26 |
| Neurological Complications (%) | 3.9 (1.6, 7.8) | 0.0 (0.0, 9.5) | 4.9 (2.0, 9.8) | 0.35 |
| Renal Complications (%) | 20.4 (14.8, 27.1) | 18.9 (8.0, 35.2) | 20.8 (14.5, 28.4) | 1.00 |
| Gastrointestinal Complications (%) | 9.4 (5.6, 14.6) | 2.7 (0.1, 14.2) | 11.1 (6.5, 17.4) | 0.20 |
| Postoperative Transfusion (%) | 7.7 (4.3, 12.6) | 0.0 (0.0, 9.5) | 9.7 (5.4, 15.8) | 0.08 |
| Deaths (%) | 0.6 (0.0, 3.0) | 0.0 (0.0, 9.5) | 0.7 (0.0, 3.8) | 1.00 |
| Variable | Group | 6h postop. | POD 1 | POD 2 |
|---|---|---|---|---|
| PONV (%) | Dehydrated | 16.2 (6.2, 32) | 21.6 (9.8, 38.2) | 8.1 (1.7, 21.9) |
| Hydrated | 15.3 (9.8, 22.2) | 11.1 (6.5, 17.4) | 10.5 (5.9, 16.6) | |
| Flatus (hours) | Dehydrated | – | 43.2 (27.1, 60.5) | 91.9 (78.1, 98.3) |
| Hydrated | – | 47.6 (38.9, 55.7) | 79.4 (70.1, 84.3) | |
| Defecation * (%) | Dehydrated | – | 2.7 (0.1, 14.2) | 56.8 (39.5, 72.9) |
| Hydrated | – | 11.1 (6.5, 17.4) | 43.0 (34.2, 50.9) | |
| – | p = 0.29 | p = 0.29 |
| Plasma Creatinine (% Change) | Dehydrated (n = 37) | Hydrated (n = 144) | p-Value |
|---|---|---|---|
| 6 h/preop | 20 (13–41) | 13 (1–25) | 0.01 |
| POD 1/preop | 23 (9–39) | 9 (−3–25) | 0.02 |
| POD 2/preop | 12 (−2–42) | 3 (−9–18) | 0.013 |
| Preoperative change in P-creatinine (% change) | |||
| ≥1.0 (n = 82) | <1.0 (n = 102) | ||
| 6 h/preop | 21 (13–36) | 8 (−6–20) | 0.001 |
| POD 1/preop | 18 (9–39) | 6 (−8–21) | 0.001 |
| POD 2/preop | 11 (1–27) | −2 (−12–12) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Löffel, L.M.; Engel, D.A.; Beilstein, C.M.; Hahn, R.G.; Furrer, M.A.; Wuethrich, P.Y. Dehydration before Major Urological Surgery and the Perioperative Pattern of Plasma Creatinine: A Prospective Cohort Series. J. Clin. Med. 2021, 10, 5817. https://doi.org/10.3390/jcm10245817
Löffel LM, Engel DA, Beilstein CM, Hahn RG, Furrer MA, Wuethrich PY. Dehydration before Major Urological Surgery and the Perioperative Pattern of Plasma Creatinine: A Prospective Cohort Series. Journal of Clinical Medicine. 2021; 10(24):5817. https://doi.org/10.3390/jcm10245817
Chicago/Turabian StyleLöffel, Lukas M., Dominique A. Engel, Christian M. Beilstein, Robert G. Hahn, Marc A. Furrer, and Patrick Y. Wuethrich. 2021. "Dehydration before Major Urological Surgery and the Perioperative Pattern of Plasma Creatinine: A Prospective Cohort Series" Journal of Clinical Medicine 10, no. 24: 5817. https://doi.org/10.3390/jcm10245817
APA StyleLöffel, L. M., Engel, D. A., Beilstein, C. M., Hahn, R. G., Furrer, M. A., & Wuethrich, P. Y. (2021). Dehydration before Major Urological Surgery and the Perioperative Pattern of Plasma Creatinine: A Prospective Cohort Series. Journal of Clinical Medicine, 10(24), 5817. https://doi.org/10.3390/jcm10245817