
Effect of Intra-Articular Injection of Platelet-Rich Plasma on the Serum Levels of Osteoarthritic Biomarkers in Patients with Unilateral Knee Osteoarthritis

 , , ,
, , ,
Abstract
:1. Introduction
Aim of the Study
2. Materials and Methods
2.1. Study Approval
2.2. Outcome Measures
2.3. PRP Preparation and Administration
2.4. Blood Sampling
2.5. Multiplex Assay for Cytokine/Chemokine and Matrix Metalloproteinase Quantification
2.6. Enzyme-Linked Immunosorbent Assay (ELISA) Measurement of Human Collagen Type 2, BMP2, TIMP1, TIMP2, TGF Beta 1 and COMP
2.7. Statistical Analysis
3. Results
3.1. Clinical Outcomes
3.2. Laboratory Outcomes
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Abramson, S.B.; Attur, M. Developments in the scientific understanding of osteoarthritis. Arthritis Res. Ther. 2009, 11, 227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tchetina, E.V. Developmental Mechanisms in Articular Cartilage Degradation in Osteoarthritis. Arthritis 2010, 2011, 683970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- dos Santos, R.G.; Santos, G.S.; Alkass, N.; Chiesa, T.L.; Azzini, G.O.; da Fonseca, L.F.; dos Santos, A.F.; Rodrigues, B.L.; Mosaner, T.; Lana, J.F. The regenerative mechanisms of platelet-rich plasma: A review. Cytokine 2021, 144, 155560. [Google Scholar] [CrossRef] [PubMed]
- Collins, T.; Alexander, D.; Barkatali, B. Platelet-rich plasma: A narrative review. EFORT Open Rev. 2021, 6, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Gato-Calvo, L.; Magalhães, J.; Ruiz-Romero, C.; Blanco, F.J.; Burguera, E.F. Platelet-rich plasma in osteoarthritis treatment: Review of current evidence. Ther. Adv. Chronic Dis. 2019, 10, 2040622319825567. [Google Scholar] [CrossRef] [Green Version]
- Hohmann, E.; Tetsworth, K.; Glatt, V. Is platelet-rich plasma effective for the treatment of knee osteoarthritis? A systematic review and meta-analysis of level 1 and 2 randomized controlled trials. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 955–967. [Google Scholar] [CrossRef]
- Altman, R.; Asch, E.; Bloch, D.; Bole, G.; Borenstein, D.; Brandt, K.; Christy, W.; Cooke, T.D.; Greenwald, R.; Hochberg, M.; et al. Development of criteria for the classification and reporting of osteoarthritis: Classification of osteoarthritis of the knee. Arthritis Rheum. 1986, 29, 1039–1049. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status in-strument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteo-arthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Boonstra, A.M.; Preuper, H.R.S.; Reneman, M.F.; Posthumus, J.B.; Stewart, R.E. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. Int. J. Rehabil. Res. 2008, 31, 165–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaková, T.; Rosocha, J.; Lacko, M.; Harvanová, D.; Gharaibeh, A. Treatment of Knee Joint Osteoarthritis with Autologous Platelet-Rich Plasma in Comparison with Hyaluronic Acid. Am. J. Phys. Med. Rehabil. 2012, 91, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Primorac, D.; Molnar, V.; Rod, E.; Jeleč, Ž.; Čukelj, F.; Matišić, V.; Vrdoljak, T.; Hudetz, D.; Hajsok, H.; Borić, I. Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic Considerations. Genes 2020, 11, 854. [Google Scholar] [CrossRef]
- Bauer, D.; Hunter, D.; Abramson, S.; Attur, M.; Corr, M.; Felson, D.; Heinegård, D.; Jordan, J.; Kepler, T.; Lane, N.; et al. Classification of osteoarthritis biomarkers: A proposed approach. Osteoarthr. Cartil. 2006, 14, 723–727. [Google Scholar] [CrossRef] [Green Version]
- Kumavat, R.; Kumar, V.; Malhotra, R.; Pandit, H.; Jones, E.; Ponchel, F.; Biswas, S. Biomarkers of Joint Damage in Osteoarthritis: Current Status and Future Directions. Mediat. Inflamm. 2021, 2021, 5574582. [Google Scholar] [CrossRef] [PubMed]
- Mariani, E.; Canella, V.; Cattini, L.; Kon, E.; Marcacci, M.; Di Matteo, B.; Pulsatelli, L.; Filardo, G. Leukocyte-Rich Plate-let-Rich Plasma Injections Do Not Up-Modulate Intra-Articular Pro-Inflammatory Cytokines in the Osteoarthritic Knee. PLoS ONE 2016, 11, e0156137. [Google Scholar] [CrossRef]
- Fawzy, R.M.; Hashaad, N.I.; Mansour, A.I. Decrease of serum biomarker of type II Collagen degradation (Coll2-1) by intra-articular injection of an autologous plasma-rich-platelet in patients with unilateral primary knee osteoarthritis. Eur. J. Rheumatol. 2017, 4, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Kuculmez, O.; Sirin, F.B.; Sarikaya, N.O.; Kocyigi, H. Effect of platelet-rich plasma on serum and urine biomarkers in patients with knee osteoarthritis. Int. J. Clin. Exp. Med. 2020, 13, 5040–5049. [Google Scholar]
- Lychagin, A.; Lipina, M.; Garkavi, A.; Islaieh, O.; Timashev, P.; Ashmore, K.; Kon, E. Intraosseous injections of platelet rich plasma for knee bone marrow lesions treatment: One year follow-up. Int. Orthop. 2021, 45, 355–363. [Google Scholar] [CrossRef]
- Henrotin, Y.; Chevalier, X.; Deberg, M.; Balblanc, J.; Richette, P.; Mulleman, D.; Maillet, B.; Rannou, F.; Piroth, C.; Mathieu, P.; et al. Early decrease of serum biomarkers of type II collagen degradation (Coll2-1) and joint inflammation (Coll2-1 NO2) by hyaluronic acid intra-articular injections in patients with knee osteoarthritis: A research study part of the Biovisco study. J. Orthop. Res. 2013, 31, 901–907. [Google Scholar] [CrossRef]
- Riegger, J.; Rehm, M.; Büchele, G.; Brenner, H.; Günther, K.-P.; Rothenbacher, D.; Brenner, R.E. Serum Cartilage Oligomeric Matrix Protein in Late-Stage Osteoarthritis: Association with Clinical Features, Renal Function, and Cardiovascular Biomarkers. J. Clin. Med. 2020, 9, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bi, X. Correlation of serum cartilage oligomeric matrix protein with knee osteoarthritis diagnosis: A meta-analysis. J. Orthop. Surg. Res. 2018, 13, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, W.; Liu, Y.; Hou, R.; Yin, R. Correlation of Bone Morphogenetic Protein-2 Levels in Serum and Synovial Fluid with Disease Severity of Knee Osteoarthritis. Med. Sci. Monit. 2015, 21, 363–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, E.N.B.; Vitters, E.L.; Van Lent, P.L.; Van De Loo, F.A.; Berg, W.B.V.D.; Van Der Kraan, P.M. Elevated extracellular matrix production and degradation upon bone morphogenetic protein-2 (BMP-2) stimulation point toward a role for BMP-2 in cartilage repair and remodeling. Arthritis Res. Ther. 2007, 9, R102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaud, M.; Balardy, L.; Moulis, G.; Gaudin, C.; Peyrot, C.; Vellas, B.; Cesari, M.; Nourhashemi, F. Proinflammatory Cytokines, Aging, and Age-Related Diseases. J. Am. Med. Dir. Assoc. 2013, 14, 877–882. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | OA Group (n = 36) |
|---|---|
| Age (years) | 53.4 (±7.7) |
| Female/Male | 22/14 |
| BMI (kg/m2) | 29.1 (±3.4) |
| KL grade of OA (I/II/III/IV) | 5/19/12/0 |
| Variables | Baseline | 3-Month Follow Up | p Value |
|---|---|---|---|
| VAS | 6.5 (±1.4) | 3.3 (±1.8) | p < 0.001 |
| WOMAC | |||
| Pain | 8.8 (±3.1) | 3.6 (±2.4) | p < 0.001 |
| Stiffness | 2.9 (±2.1) | 1.2 (±1.5) | p < 0.001 |
| Function | 23.9 (±9.6) | 13.2 (±8.4) | p < 0.001 |
| Total | 32.8 (±11.9) | 18.1 (±11.6) | p < 0.001 |
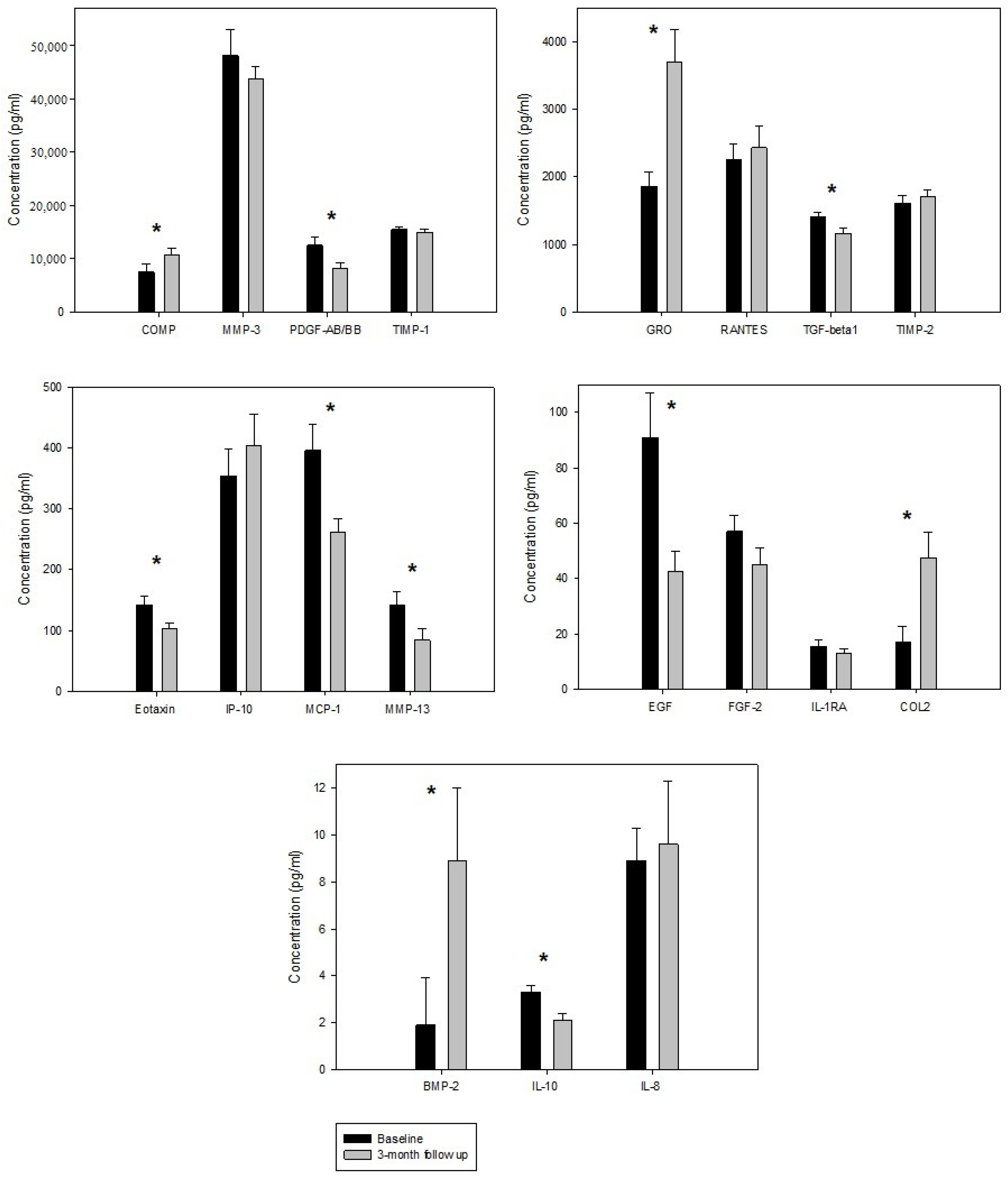
| Biomarker | Baseline | 3-Month Follow Up | p Value |
|---|---|---|---|
| BMP-2 | 1.9 (±2.0) | 8.9 (±3.1) | p = 0.011 |
| COMP | 7545.1 (±1428.4) | 10,716.3 (±1174.4) | p = 0.046 |
| EGF | 90.9 (±16.2) | 42.6 (±7.4) | p = 0.030 |
| Eotaxin | 141.6 (±14.1) | 103.1 (±9.9) | p = 0.039 |
| FGF-2 | 57.1 (±5.8) | 45.2 (±5.9) | p = 0.119 |
| GRO | 1860.4 (±213.6) | 3708 (±477.7) | p = 0.002 |
| IL-10 | 3.3 (±0.3) | 2.1 (±0.3) | p = 0.002 |
| IL-1RA | 15.5 (±2.2) | 13.1 (±1.7) | p = 0.485 |
| IL-8 | 8.9 (±1.4) | 9.6 (±2.7) | p = 0.537 |
| IP-10 | 354.9 (±42.8) | 404 (±50.5) | p = 0.632 |
| Collagen 2 | 17.1 (±5.6) | 47.4 (±9.5) | p = 0.022 |
| MCP-1 | 396.1 (±43.4) | 262.7 (±21.6) | p = 0.007 |
| MMP-13 | 141.7 (±22.1) | 84.2 (±19.6) | p = 0.005 |
| MMP-3 | 48,084.3 (±4858.3) | 43,737.8 (±2298.4) | p = 0.630 |
| PDGF-AB/BB | 12,513.9 (±1501.2) | 8287.7 (±923.8) | p = 0.027 |
| RANTES | 2250.3 (±240.4) | 2434.3 (±313.2) | p = 0.995 |
| TGF-β1 | 1402.4 (±74.1) | 1165.8 (±73.4) | p = 0.026 |
| TIMP1 | 15,497.7 (±542.8) | 14,958.9 (±568.2) | p = 0.240 |
| TIMP2 | 1612.7 (±107.0) | 1710.2 (±97.2) | p = 0.252 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lacko, M.; Harvanová, D.; Slovinská, L.; Matuška, M.; Balog, M.; Lacková, A.; Špaková, T.; Rosocha, J. Effect of Intra-Articular Injection of Platelet-Rich Plasma on the Serum Levels of Osteoarthritic Biomarkers in Patients with Unilateral Knee Osteoarthritis. J. Clin. Med. 2021, 10, 5801. https://doi.org/10.3390/jcm10245801
Lacko M, Harvanová D, Slovinská L, Matuška M, Balog M, Lacková A, Špaková T, Rosocha J. Effect of Intra-Articular Injection of Platelet-Rich Plasma on the Serum Levels of Osteoarthritic Biomarkers in Patients with Unilateral Knee Osteoarthritis. Journal of Clinical Medicine. 2021; 10(24):5801. https://doi.org/10.3390/jcm10245801
Chicago/Turabian StyleLacko, Marek, Denisa Harvanová, Lucia Slovinská, Martin Matuška, Marek Balog, Antónia Lacková, Timea Špaková, and Ján Rosocha. 2021. "Effect of Intra-Articular Injection of Platelet-Rich Plasma on the Serum Levels of Osteoarthritic Biomarkers in Patients with Unilateral Knee Osteoarthritis" Journal of Clinical Medicine 10, no. 24: 5801. https://doi.org/10.3390/jcm10245801
APA StyleLacko, M., Harvanová, D., Slovinská, L., Matuška, M., Balog, M., Lacková, A., Špaková, T., & Rosocha, J. (2021). Effect of Intra-Articular Injection of Platelet-Rich Plasma on the Serum Levels of Osteoarthritic Biomarkers in Patients with Unilateral Knee Osteoarthritis. Journal of Clinical Medicine, 10(24), 5801. https://doi.org/10.3390/jcm10245801