
Long-Term Preservation of Renal Function in Septic Shock Burn Patients Requiring Renal Replacement Therapy for Acute Kidney Injury

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and In-Hospital AKI Management
2.2. In-Hospital Burn and AKI Management
2.3. Technical Aspects of CRRT and CPFA-CRRT Treatment
2.4. Nephrological Follow-Up after Discharge
2.5. Study of Urine Protein Profile and Determination of Normalized Radio Isotopic GFR (NRI–GFR)
2.6. Statistical Analysis
3. Results
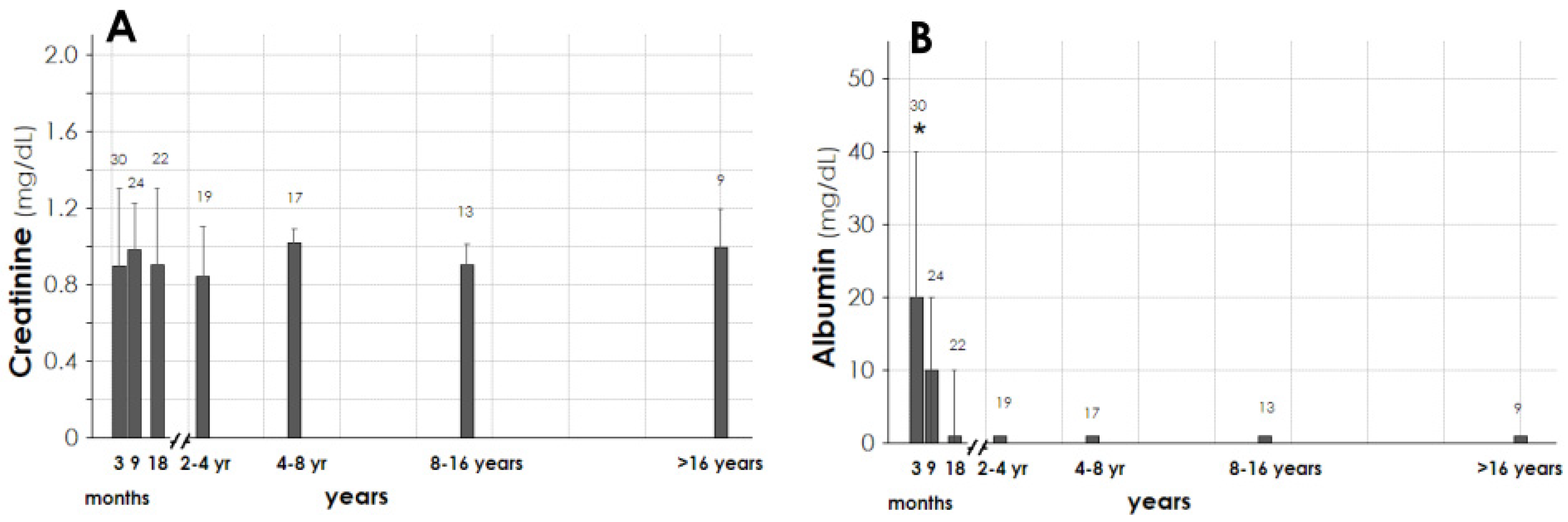
3.1. Baseline Characteristics of Patients and Long-Term Outcome of Creatinine and Urine Albumin
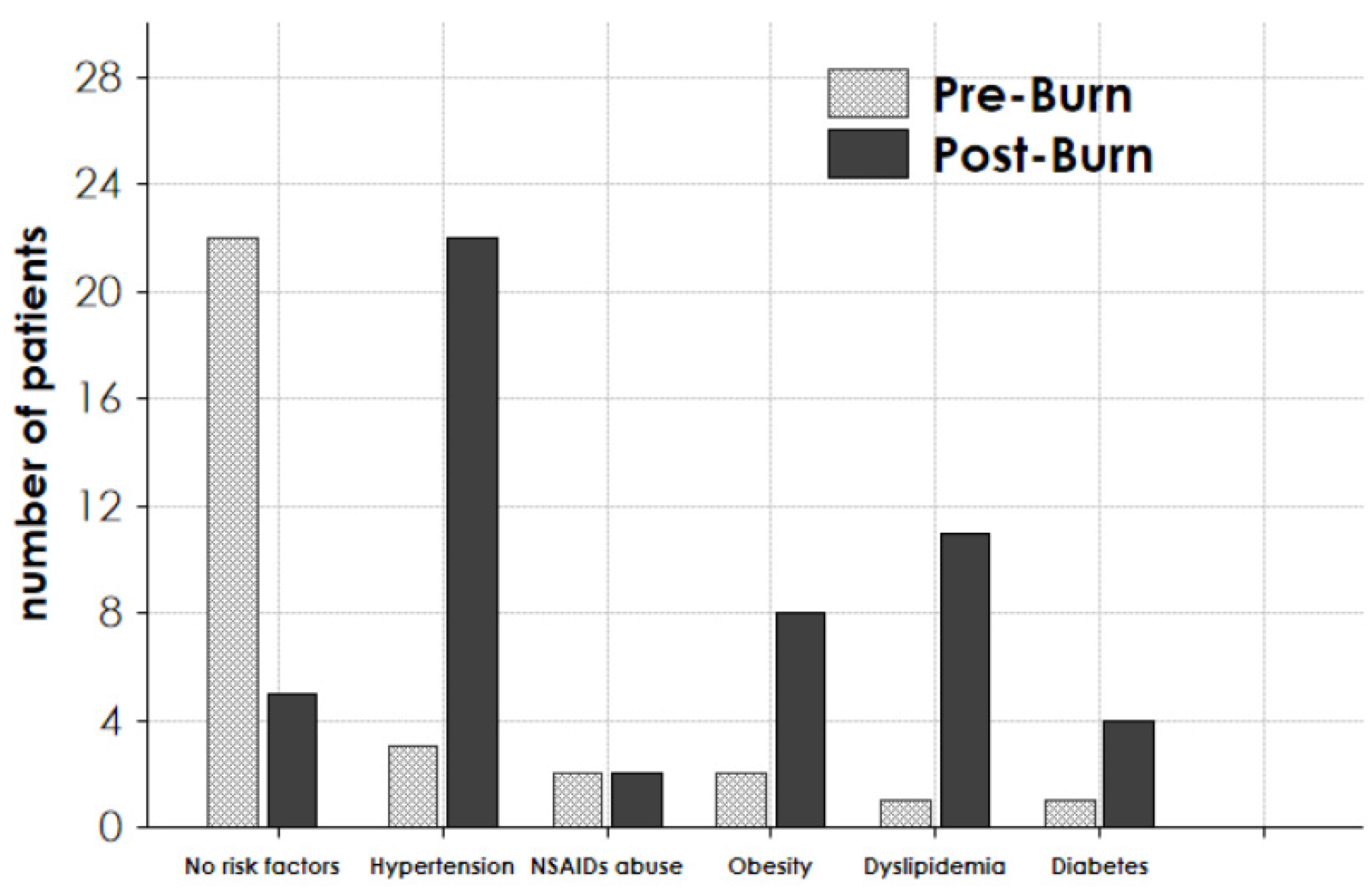
3.2. Risk Factors for the Development of CKD
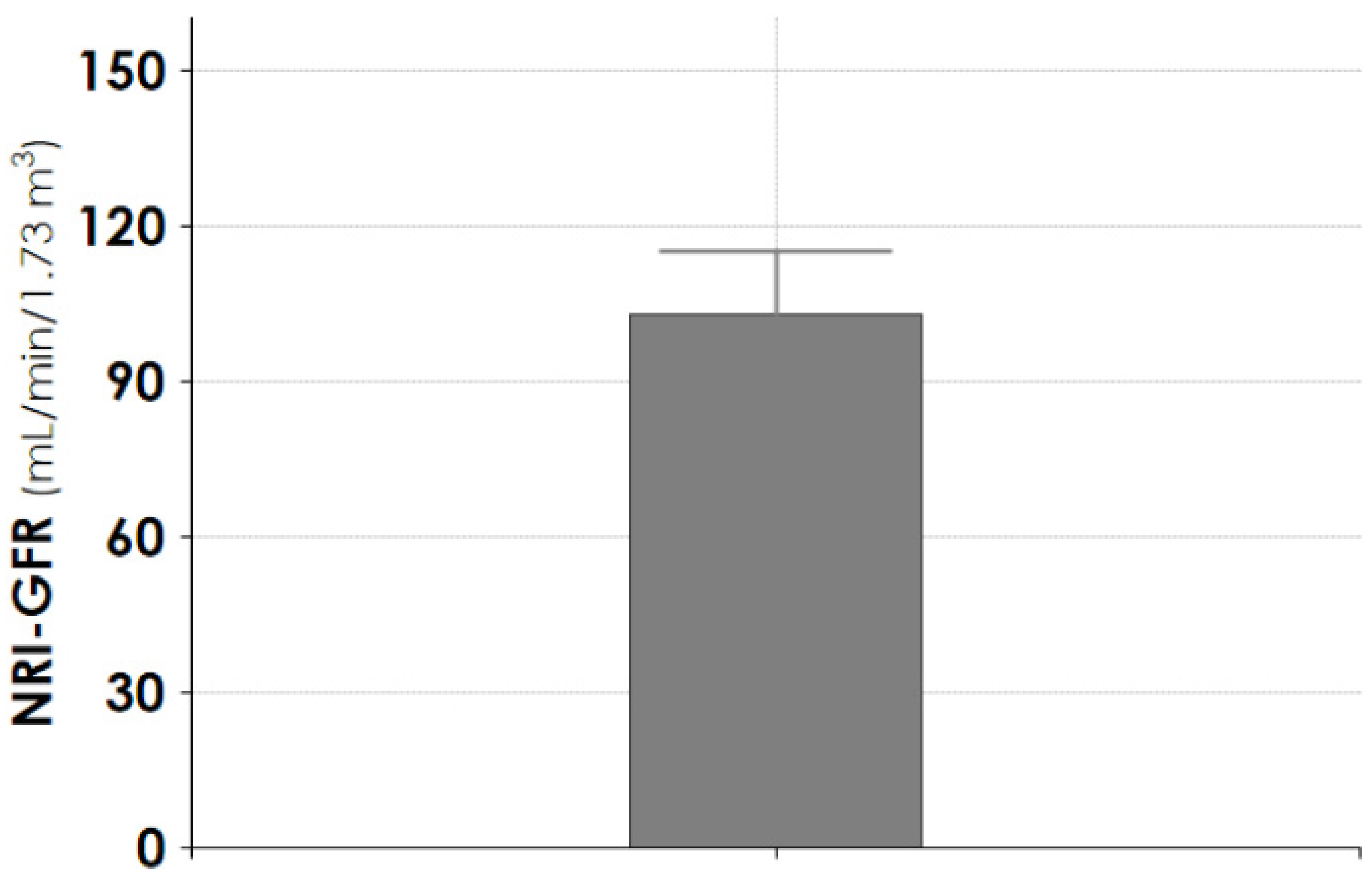
3.3. Study of Long-Term Glomerular Function and Glomerular/Tubular Protein Markers in CPFA-CRRT Patients
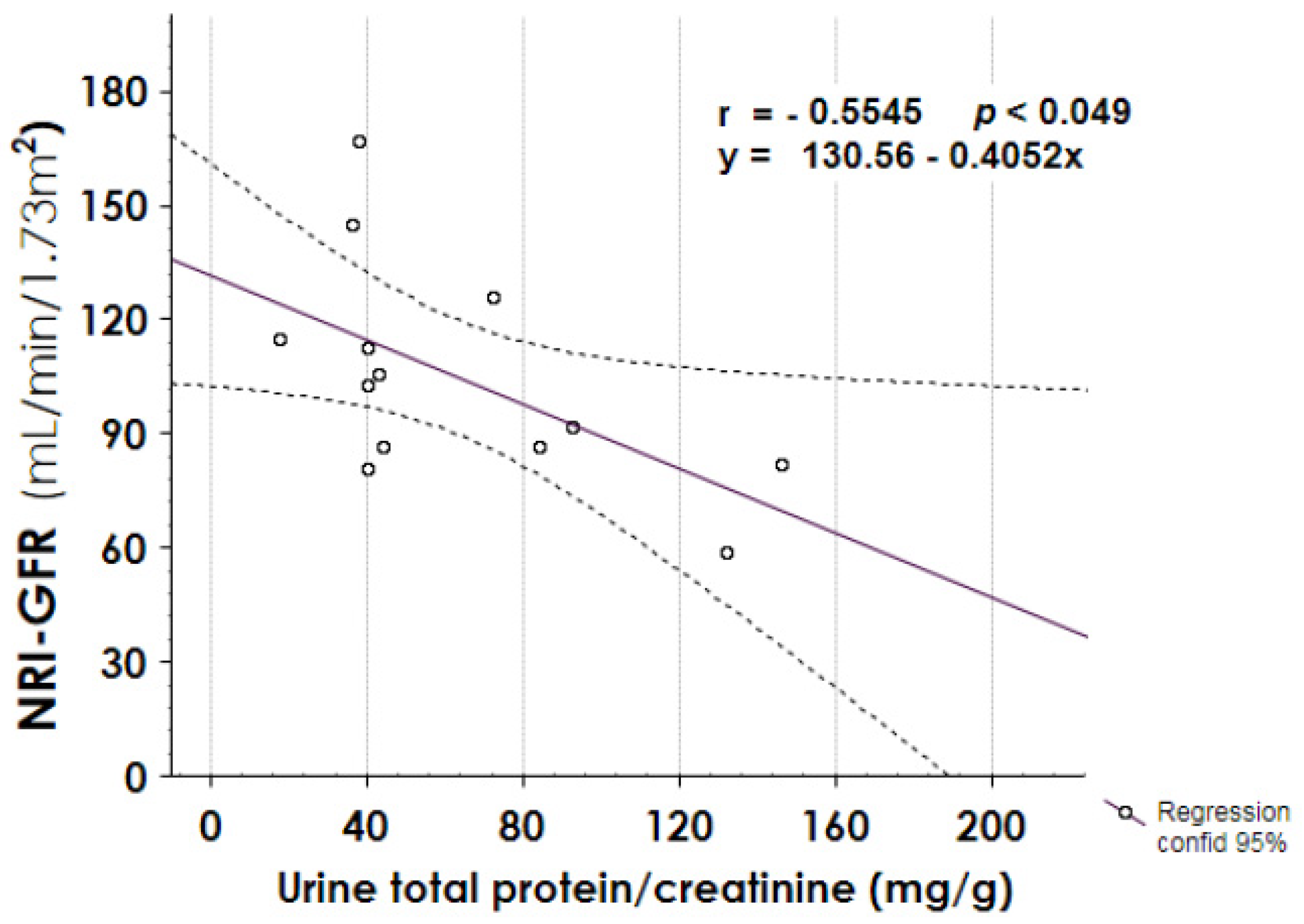
3.4. Relationship between Proteinuria, AKI Severity, and NRI-GFR in CPFA-CRRT Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fortrie, G.; de Geus, H.R.H.; Betjes, M.G.H. The aftermath of acute kidney injury: A narrative review of long-term mortality and renal function. Crit. Care 2019, 23, 24. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Kimmel, P.L. Acute kidney injury and chronic kidney disease: An integrated clinical syndrome. Kidney Int. 2012, 82, 516–524. [Google Scholar] [CrossRef]
- Yoon, J.; Kim, Y.; Kym, D.; Hur, J.; Yim, H.; Cho, Y.-S.; Chun, W. Subgroup analysis of continuous renal replacement therapy in severely burned patients. PLoS ONE 2017, 12, e0189057. [Google Scholar] [CrossRef]
- Helanterä, I.; Koljonen, V.; Finne, P.; Tukiainen, E.; Gissler, M. The risk for end-stage renal disease is increased after burn. Burns 2016, 42, 316–321. [Google Scholar] [CrossRef]
- Folkestad, T.; Brurberg, K.G.; Nordhuus, K.M.; Tveiten, C.K.; Guttormsen, A.B.; Os, I.; Beitland, S. Acute kidney injury in burn patients admitted to the intensive care unit: A systematic review and me-ta-analysis. Crit. Care 2020, 24, 2. [Google Scholar] [CrossRef]
- Yu, H.; Cooper, E.; Settle, J.; Meadows, T. Urinary protein profiles after burn injury. Burns 1983, 9, 339–349. [Google Scholar] [CrossRef]
- Mariano, F.; Gangemi, E.N.; Bergamo, D.; Hollo, Z.; Stella, M.; Triolo, G. Burns and Acute Kidney Failure in Management of Acute Kidney, Problems, 1st ed.; Jorres, A., Ronco, C., Kellum, J.A., Eds.; Springer: Berlin, Germany, 2010; pp. 429–438. [Google Scholar]
- Neyra, J.A.; Li, X.; Yessayan, L.; Adams-Huet, B.; Yee, J.; Toto, R.D. Acute Kidney Injury in critical illness study group: Dipstick albuminuria and acute kidney injury recovery in critically ill septic patients. Nephrology 2016, 21, 512–518. [Google Scholar] [CrossRef]
- Verma, S.K.; Molitoris, B.A. Renal endothelial injury and microvascular dysfunction in acute kidney injury. Semin. Nephrol. 2015, 35, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Peerapornratana, S.; Manrique-Caballero, C.L.; Gómez, H.; Kellum, J.A. Acute kidney injury from sepsis: Current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int. 2019, 96, 1083–1099. [Google Scholar] [CrossRef]
- Holm, C.; Horbrand, F.; von Donnersmarck, G.H.; Muhlbauer, W. Acute renal failure in severely burned patients. Burns 1999, 25, 171–178. [Google Scholar] [CrossRef]
- Tremblay, R.; Ethier, J.; Quérin, S.; Béroniade, V.; Falardeau, P.; Leblanc, M. Veno-venous continuous renal replacement therapy for burned patients with acute renal failure. Burns 2000, 26, 638–643. [Google Scholar] [CrossRef]
- Mustonen, K.-M.; Vuola, J. Acute renal failure in intensive care burn patients (ARF in burn patients). J. Burn Care Res. 2008, 29, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Brusselaers, N.; Monstrey, S.; Colpaert, K.; Decruyenaere, J.; Blot, S.I.; Hoste, E.A.J. Outcome of acute kidney injury in severe burns: A systematic review and meta-analysis. Intensiv. Care Med. 2010, 36, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Mariano, F.; Tedeschi, L.; Morselli, M.; Stella, M.; Triolo, G. Normal citratemia and metabolic tolerance of citrate anticoagulation for hemodiafiltration in severe septic shock burn patients. Intensiv. Care Med. 2010, 36, 1735–1743. [Google Scholar] [CrossRef]
- Thalji, S.Z.; Kothari, A.N.; Kuo, P.C.; Mosier, M.J. Acute kidney injury in burn patients: Clinically significant over the initial hospitalization and 1 year after injury: An original retrospective cohort study. Ann. Surg. 2017, 266, 376–382. [Google Scholar] [CrossRef]
- Rakkolainen, I.; Mustonen, K.-M.; Vuola, J. Long-Term outcome after renal replacement therapy in severe burns. J. Burn Care Res. 2020, 41, 866–870. [Google Scholar] [CrossRef]
- Mariano, F.; Tetta, C.; Stella, M.; Biolino, P.; Miletto, A.; Triolo, G. Regional citrate anticoagulation in critically Ill patients treated with plasma filtration and adsorption. Blood Purif. 2004, 22, 313–319. [Google Scholar] [CrossRef]
- Mariano, F.; Morselli, M.; Hollo, Z.; Agostini, F.; Stella, M.; Biancone, L. Citrate pharmacokinetics at high levels of circuit citratemia during coupled plasma filtration adsorption. Nephrol. Dial. Transplant. 2015, 30, 1911–1919. [Google Scholar] [CrossRef] [PubMed]
- Mariano, F.; Hollo’, Z.; Depetris, N.; Malvasio, V.; Mella, A.; Bergamo, D.; Pensa, A.; Berardino, M.; Stella, M.; Biancone, L. Coupled-plasma filtration and adsorption for severe burn patients with septic shock and acute kidney injury treated with renal replacement therapy. Burns 2020, 46, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Lameire, N.; KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: A KDIGO summary (Part 1). Crit. Care 2013, 17, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Regeniter, A.; Freidank, H.; Dickenmann, M.; Boesken, W.H.; Siede, W.H. Evaluation of proteinuria and GFR to diagnose and classify kidney disease: Systematic review and proof of concept. Eur. J. Intern. Med. 2009, 20, 556–561. [Google Scholar] [CrossRef]
- Bastard, J.P.; Fellahi, S.; Regeniter, A.; Capeau, J.; Ronco, P.; Plaisier, E. Aside from acute renal failure cases, are urinary markers of glomerular and tubular function useful in clinical practice? Clin. Biochem. 2019, 65, 1–6. [Google Scholar] [CrossRef]
- Fleming, J.S.; Zivanovic, M.A.; Blake, G.M.; Burniston, M.; Cosgriff, P.S. British Nuclear Medicine Society: Guidelines for the measurement of glomerular filtration rate using plasma sampling. Nucl. Med. Commun. 2004, 25, 759–769. [Google Scholar] [CrossRef]
- Findlay, M.; Donaldson, K.; Robertson, S.; Almond, A.; Flynn, R.; Isles, C. Chronic kidney disease rather than illness severity predicts medium- to long-term mortality and renal outcome after acute kidney injury. Nephrol. Dial. Transplant. 2015, 30, 594–598. [Google Scholar] [CrossRef]
- Chawla, L.S.; Seneff, M.G.; Nelson, D.R.; Williams, M.; Levy, H.; Kimmel, P.L.; Macias, W.L. Elevated plasma concentrations of IL-6 and elevated apache ii score predict acute kidney injury in patients with severe sepsis. Clin. J. Am. Soc. Nephrol. 2007, 2, 22–30. [Google Scholar] [CrossRef]
- Coca, S.G.; King, J.T.; Rosenthal, R.A.; Perkal, M.F.; Parikh, C.R. The duration of postoperative acute kidney injury is an ad-ditional parameter predicting long-term survival in diabetic veterans. Kidney Int. 2010, 78, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Siew, E.D.; Abdel-Kader, K.; Perkins, A.M.; Greevy, R.A.; Parr, S.K.; Horner, J.; Vincz, A.J.; Denton, J.; Wilson, O.D.; Hung, A.M.; et al. Timing of recovery from moderate to severe AKI and the risk for future loss of kidney function. Am. J. Kidney Dis. 2020, 75, 204–213. [Google Scholar] [CrossRef]
- Soltani, A.; Karsidag, S.; Garner, W. A ten-year experience with hemodialysis in burn patients at Los Angeles County + USC Medical Center. J. Burn Care Res. 2009, 30, 832–835. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.K.; Lundy, J.B.; Matson, J.R.; Renz, E.M.; White, C.; King, B.T.; Barillo, D.J.; Jones, J.; Cancio, L.C.; Blackbourne, L.H.; et al. Continuous venovenous hemofiltration in severely burned patients with acute kidney injury: A cohort study. Crit. Care 2009, 13, R62. [Google Scholar] [CrossRef]
- Stoumpos, S.; Mark, P.B.; McQuarrie, E.P.; Traynor, J.P.; Geddes, C.C. Continued monitoring of acute kidney injury survivors might not be necessary in those regaining an estimated glomerular filtration rate >60 mL/min at 1 year. Nephrol. Dial. Transplant. 2017, 32, 81–88. [Google Scholar] [CrossRef][Green Version]
- Hsu, C.-Y.; Hsu, R.; Yang, J.; Ordonez, J.D.; Zheng, S.; Go, A.S. Elevated BP after AKI. J. Am. Soc. Nephrol. 2016, 27, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Jeschke, M.G.; Gauglitz, G.G.; Kulp, G.A.; Finnerty, C.C.; Williams, F.N.; Kraft, R.; Suman, O.E.; Mlcak, R.P.; Herndon, D.N. Long-Term persistance of the pathophysiologic response to severe burn injury. PLoS ONE 2011, 6, e21245. [Google Scholar] [CrossRef]
- Thomas, G.; Sehgal, A.R.; Kashyap, S.R.; Srinivas, T.R.; Kirwan, J.P.; Navaneethan, S.D. Metabolic syndrome and kidney disease: A systematic review and meta-analysis. Clin. J. Am. Soc. Nephrol. 2011, 6, 2364–2373. [Google Scholar] [CrossRef]
- Hu, J.Y.; Meng, X.C.; Han, J.; Xiang, F.; Fang, Y.D.; Wu, J.; Peng, Y.Z.; Wu, Y.Z.; Huang, Y.S.; Luo, Q.Z. Relation between proteinuria and acute kidney injury in patients with severe burns. Crit. Care 2012, 16, R172. [Google Scholar] [CrossRef] [PubMed]
- Schiavon, M.; Di Landro, D.; Baldo, M.; De Silvestro, G.; Chiarelli, A. A study of renal damage in seriously burned patients. Burn. Incl. Therm. Inj. 1988, 14, 107–112. [Google Scholar] [CrossRef]
- Vlachou, E.; Gosling, P.; Moiemen, N. Microalbuminuria: A marker of endothelial dysfunction in thermal injury. Burns 2006, 32, 1009–1016. [Google Scholar] [CrossRef]
- Mariano, F.; Camussi, G. Unravelling the enigma of proteinuria in burn patients. Crit. Care 2012, 16, 184. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mariano, F.; Cantaluppi, V.; Stella, M.; Romanazzi, G.M.; Assenzio, B.; Cairo, M.; Biancone, L.; Triolo, G.; Ranieri, V.M.; Camussi, G. Circulating plasma factors induce tubular and glomerular alterations in septic burns patients. Crit. Care 2008, 12, R42. [Google Scholar] [CrossRef]
- Oudemans-van, S.; Heleen, M. Circulating pro-apoptotic mediators in burn septic acute renal failure. Crit. Care 2008, 12, 126. [Google Scholar] [CrossRef] [PubMed]
- Parr, S.K.; Matheny, M.; Abdel-Kader, K.; Greevy, R.A.; Bian, A.; Fly, J.; Chen, G.; Speroff, T.; Hung, A.M.; Ikizler, T.; et al. Acute kidney injury is a risk factor for subsequent proteinuria. Kidney Int. 2018, 93, 460–469. [Google Scholar] [CrossRef]
- Berg, L.; Meyer, S.; Ipaktchi, R.; Vogt, P.M.; Müller, A.; de Zwaan, M. Psychosocial distress at different time intervals after burn injury. Psychother. Psychosom. Med. Psychol. 2017, 67, 231–239. [Google Scholar] [PubMed]
- Vincent, J.-L. Recent negative clinical trials in septic patients: Maybe a good thing? Minerva Anestesiol. 2015, 81, 122–124. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All RRT Patients | CRRT Patients | CRRT-CFFA Patients | p | |
|---|---|---|---|---|
| Patients (n) | 40 | 21 | 19 | - |
| Cumulative follow-up time (months) | 4067 | 1728 | 2339 | - |
| Gender ratio (male/female) | 29/11 | 13/8 | 16/3 | 0.11 |
| Age (years) | 52.0 (43.2–68.0) | 67.0 (53.0–74.0) | 46.0 (30.0–51.0) | 0.01 |
| Age at follow-up end (years) | 63.0 (49.0–73.0) | 74.0 (59.6–81.0) | 52.0 (44.3–62.0) | 0.01 |
| Follow-up time (median, months) | 84 (44–173) | 54 (36–159) | 101 (68–206) | 0.07 |
| Mortality (%, n) | 25.0%, 10 | 43.0%, 9 | 5.3%, 1 | 0.02 |
| Total body surface area (%) | 37.5 (22.5–50.0) | 30.0 (20.0–40.0) | 45.0 (35.0–60.0) | 0.01 |
| Baux index | 0.32 (0.16–0.62) | 0.43 (0.13–0.61) | 0.30 (0.19–0.63) | 0.70 |
| Septic shock (%, n) | 95.0%, 38 | 95.0%, 19 | 100%, 19 | 0.35 |
| Mechanical ventilation (%, n) | 97.5%, 39 | 95.2 %, 20 | 100%, 19 | 0.54 |
| SOFA score (at 1st day of treatment) | 10 (9–12.5) | 10 (9–12) | 10 (9–13) | 0.73 |
| CRRT/CPFA-CRRT duration (days) | 9.0 (5.50–21.5) | 8.0 (5.0–29.0) | 10.0 (7.0–20.0) | 0.58 |
| Citrate anticoagulation (%, n) | 70.0%, 28 | 80.9%, 17 | 57.8%, 11 | 0.08 |
| Plasma creatinine (at the start, mg/dL) | 2.2 (1.3–3.0) | 2.4 (2.2–3.1) | 1.4 (0.9–2.2) | 0.01 |
| Plasma creatinine (at the end, mg/dL) | 1.3 (0.9–1.8) | 1.3 (1.1–1.9) | 1.1 (0.7–1.7) | 0.06 |
| Plasma creatinine (at the peak, mg/dL) | 2.4 (1.4–3.1) | 2.9 (2.2–3.4) | 1.8 (1.1–2.7) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mariano, F.; De Biase, C.; Hollo, Z.; Deambrosis, I.; Davit, A.; Mella, A.; Bergamo, D.; Maffei, S.; Rumbolo, F.; Papaleo, A.; et al. Long-Term Preservation of Renal Function in Septic Shock Burn Patients Requiring Renal Replacement Therapy for Acute Kidney Injury. J. Clin. Med. 2021, 10, 5760. https://doi.org/10.3390/jcm10245760
Mariano F, De Biase C, Hollo Z, Deambrosis I, Davit A, Mella A, Bergamo D, Maffei S, Rumbolo F, Papaleo A, et al. Long-Term Preservation of Renal Function in Septic Shock Burn Patients Requiring Renal Replacement Therapy for Acute Kidney Injury. Journal of Clinical Medicine. 2021; 10(24):5760. https://doi.org/10.3390/jcm10245760
Chicago/Turabian StyleMariano, Filippo, Consuelo De Biase, Zsuzsanna Hollo, Ilaria Deambrosis, Annalisa Davit, Alberto Mella, Daniela Bergamo, Stefano Maffei, Francesca Rumbolo, Alberto Papaleo, and et al. 2021. "Long-Term Preservation of Renal Function in Septic Shock Burn Patients Requiring Renal Replacement Therapy for Acute Kidney Injury" Journal of Clinical Medicine 10, no. 24: 5760. https://doi.org/10.3390/jcm10245760
APA StyleMariano, F., De Biase, C., Hollo, Z., Deambrosis, I., Davit, A., Mella, A., Bergamo, D., Maffei, S., Rumbolo, F., Papaleo, A., Stella, M., & Biancone, L. (2021). Long-Term Preservation of Renal Function in Septic Shock Burn Patients Requiring Renal Replacement Therapy for Acute Kidney Injury. Journal of Clinical Medicine, 10(24), 5760. https://doi.org/10.3390/jcm10245760