
Diagnostic, Prognostic, and Therapeutic Value of Droplet Digital PCR (ddPCR) in COVID-19 Patients: A Systematic Review


Abstract
:1. Introduction
2. Results
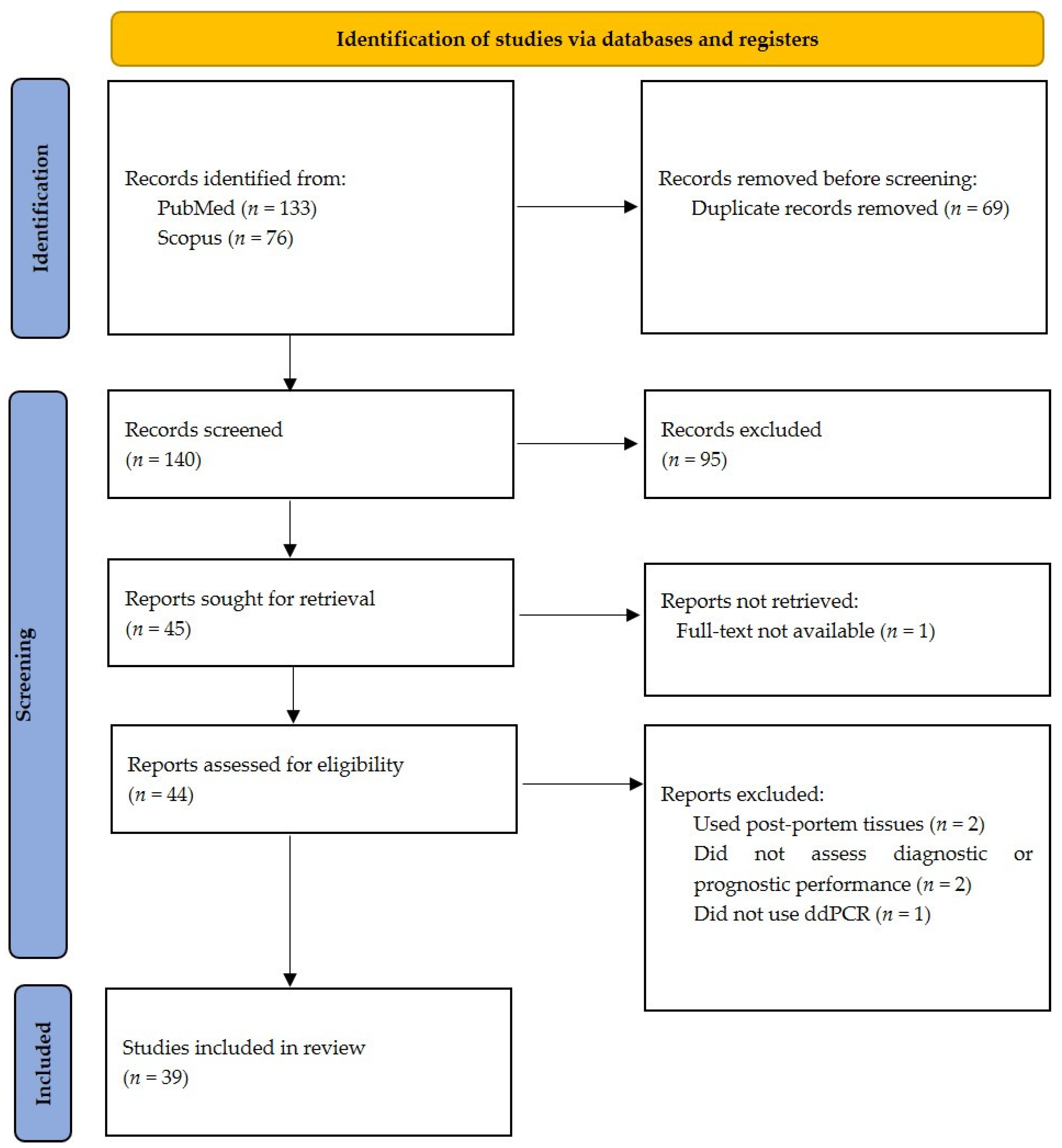
2.1. Literature Search
2.2. Characteristics of Studies
2.3. Diagnostic Performance of Digital PCR
2.4. Prognostic and Therapeutic Value of Digital PCR
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Study Selection
4.3. Data Extraction
4.4. Study Outcomes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mahase, E. COVID-19: WHO Declares Pandemic Because of “Alarming Levels” of Spread, Severity, and Inaction. BMJ 2020, 368, m1036. [Google Scholar] [CrossRef] [Green Version]
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and Influenza Pandemics. Lancet Infect. Dis. 2020, 20, e238–e244. [Google Scholar] [CrossRef]
- Graeden, E.; Carlson, C.; Katz, R. Answering the Right Questions for Policymakers on COVID-19. Lancet Glob. Health 2020, 8, e768–e769. [Google Scholar] [CrossRef]
- Pan, Y.; Zhang, D.; Yang, P.; Poon, L.L.M.; Wang, Q. Viral Load of SARS-CoV-2 in Clinical Samples. Lancet Infect. Dis. 2020, 20, 411–412. [Google Scholar] [CrossRef]
- Fajnzylber, J.; Regan, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Worrall, D.; Giguel, F.; Piechocka-Trocha, A.; Atyeo, C.; et al. SARS-CoV-2 Viral Load Is Associated with Increased Disease Severity and Mortality. Nat. Commun. 2020, 11, 5493. [Google Scholar] [CrossRef]
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community Transmission and Viral Load Kinetics of the SARS-CoV-2 Delta (B.1.617.2) Variant in Vaccinated and Unvaccinated Individuals in the UK: A Prospective, Longitudinal, Cohort Study. Lancet Infect. Dis. 2021, in press. [Google Scholar] [CrossRef]
- Gonçalves, A.; Bertrand, J.; Ke, R.; Comets, E.; Lamballerie, X.; Malvy, D.; Pizzorno, A.; Terrier, O.; Rosa Calatrava, M.; Mentré, F.; et al. Timing of Antiviral Treatment Initiation Is Critical to Reduce SARS-CoV-2 Viral Load. Clin. Pharmacol. Ther. 2020, 9, 509–514. [Google Scholar] [CrossRef]
- Taleghani, N.; Taghipour, F. Diagnosis of COVID-19 for Controlling the Pandemic: A Review of the State-of-the-Art. Biosens. Bioelectron. 2021, 174, 112830. [Google Scholar] [CrossRef]
- Patel, A.; Jernigan, D.B.; 2019-nCoV CDC Response Team; Abdirizak, F.; Abedi, G.; Aggarwal, S.; Albina, D.; Allen, E.; Andersen, L. Initial Public Health Response and Interim Clinical Guidance for the 2019 Novel Coronavirus Outbreak—United States, December 31, 2019–February 4, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 140–146. [Google Scholar] [CrossRef]
- Vasudevan, H.N.; Xu, P.; Servellita, V.; Miller, S.; Liu, L.; Gopez, A.; Chiu, C.Y.; Abate, A.R. Digital Droplet PCR Accurately Quantifies SARS-CoV-2 Viral Load from Crude Lysate without Nucleic Acid Purification. Sci. Rep. 2021, 11, 780. [Google Scholar] [CrossRef]
- Mouliou, D.S.; Gourgoulianis, K.I. False-Positive and False-Negative COVID-19 Cases: Respiratory Prevention and Management Strategies, Vaccination, and Further Perspectives. Expert Rev. Respir. Med. 2021, 15, 993–1002. [Google Scholar] [CrossRef]
- Suo, T.; Liu, X.; Feng, J.; Guo, M.; Hu, W.; Guo, D.; Ullah, H.; Yang, Y.; Zhang, Q.; Wang, X.; et al. DdPCR: A More Accurate Tool for SARS-CoV-2 Detection in Low Viral Load Specimens. Emerg. Microbes Infect. 2020, 9, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Kevadiya, B.D.; Machhi, J.; Herskovitz, J.; Oleynikov, M.D.; Blomberg, W.R.; Bajwa, N.; Soni, D.; Das, S.; Hasan, M.; Patel, M.; et al. Diagnostics for SARS-CoV-2 Infections. Nat. Mater. 2021, 20, 593–605. [Google Scholar] [CrossRef] [PubMed]
- Yüce, M.; Filiztekin, E.; Özkaya, K.G. COVID-19 Diagnosis—A Review of Current Methods. Biosens. Bioelectron. 2021, 172, 112752. [Google Scholar] [CrossRef] [PubMed]
- Mohamadian, M.; Chiti, H.; Shoghli, A.; Biglari, S.; Parsamanesh, N.; Esmaeilzadeh, A. COVID-19: Virology, Biology and Novel Laboratory Diagnosis. J. Gene Med. 2021, 23, e3303. [Google Scholar] [CrossRef]
- Taylor, S.C.; Laperriere, G.; Germain, H. Droplet Digital PCR versus QPCR for Gene Expression Analysis with Low Abundant Targets: From Variable Nonsense to Publication Quality Data. Sci. Rep. 2017, 7, 2409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Jiang, Y.; Cao, X.; Liu, C.; Zhang, N.; Shi, D. Droplet Digital PCR as an Emerging Tool in Detecting Pathogens Nucleic Acids in Infectious Diseases. Clin. Chim. Acta 2021, 517, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Liu, C.; Tong, H.; Chen, Y.; Liu, K. Principles of Digital PCR and Its Applications in Current Obstetrical and Gynecological Diseases. Am. J. Transl. Res. 2019, 11, 7209–7222. [Google Scholar] [PubMed]
- Park, C.; Lee, J.; UI Hassan, Z.; Ku, K.B.; Kim, S.-J.; Kim, H.G.; Park, E.C.; Park, G.-S.; Park, D.; Baek, S.-H.; et al. Comparison of Digital PCR and Quantitative PCR with Various SARS-CoV-2 Primer-Probe Sets. J. Microbiol. Biotechnol. 2021, 31, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Wang, G.; Long, X.; Hou, H.; Wei, J.; Cao, Y.; Tan, J.; Liu, W.; Huang, L.; Meng, F.; et al. Dynamics of Blood Viral Load Is Strongly Associated with Clinical Outcomes in Coronavirus Disease 2019 (COVID-19) Patients. J. Mol. Diagn. 2021, 23, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Dang, Y.; Liu, N.; Tan, C.; Feng, Y.; Yuan, X.; Fan, D.; Peng, Y.; Jin, R.; Guo, Y.; Lou, J. Comparison of Qualitative and Quantitative Analyses of COVID-19 Clinical Samples. Clin. Chim. Acta 2020, 510, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Zhou, J.; Niu, C.; Wang, Q.; Pan, Y.; Sheng, S.; Wang, X.; Zhang, Y.; Yang, J.; Liu, M.; et al. Highly Accurate and Sensitive Diagnostic Detection of SARS-CoV-2 by Digital PCR. Talanta 2021, 224, 121726. [Google Scholar] [CrossRef]
- Hu, X.; Zhu, L.; Luo, Y.; Zhao, Q.; Tan, C.; Chen, X.; Zhang, H.; Hu, X.; Lu, L.; Xiao, Y.; et al. Evaluation of the Clinical Performance of Single-, Dual-, and Triple-Target SARS-CoV-2 RT-QPCR Methods. Clin. Chim. Acta 2020, 511, 143–148. [Google Scholar] [CrossRef]
- Jiang, Y.; Wang, H.; Hao, S.; Chen, Y.; He, J.; Liu, Y.; Chen, L.; Yu, Y.; Hua, S. Digital PCR Is a Sensitive New Technique for SARS-CoV-2 Detection in Clinical Applications. Clin. Chim. Acta 2020, 511, 346–351. [Google Scholar] [CrossRef]
- Liu, C.; Shi, Q.; Peng, M.; Lu, R.; Li, H.; Cai, Y.; Chen, J.; Xu, J.; Shen, B. Evaluation of Droplet Digital PCR for Quantification of SARS-CoV-2 Virus in Discharged COVID-19 Patients. Aging 2020, 12, 20997–21003. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Feng, J.; Zhang, Q.; Guo, D.; Zhang, L.; Suo, T.; Hu, W.; Guo, M.; Wang, X.; Huang, Z.; et al. Analytical Comparisons of SARS-COV-2 Detection by QRT-PCR and DdPCR with Multiple Primer/Probe Sets. Emerg. Microbes Infect. 2020, 9, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Nyaruaba, R.; Li, C.; Mwaliko, C.; Mwau, M.; Odiwuor, N.; Muturi, E.; Muema, C.; Xiong, J.; Li, J.; Yu, J.; et al. Developing Multiplex DdPCR Assays for SARS-CoV-2 Detection Based on Probe Mix and Amplitude Based Multiplexing. Expert Rev. Mol. Diagn. 2021, 21, 119–129. [Google Scholar] [CrossRef]
- Sun, Y.; Ding, C.; Chen, Q.; Xie, J.; Yu, J.; Shi, Y.; Jiang, C.; Zhang, Z.; He, H.; Ge, Y.; et al. Digital PCR Assay for the Effective Detection of COVID-19 Patients with SARS-CoV-2 Low Viral Load. J. Virol. Methods 2021, 295, 114185. [Google Scholar] [CrossRef]
- Yin, H.; Wu, Z.; Shi, N.; Qi, Y.; Jian, X.; Zhou, L.; Tong, Y.; Cheng, Z.; Zhao, J.; Mao, H. Ultrafast Multiplexed Detection of SARS-CoV-2 RNA Using a Rapid Droplet Digital PCR System. Biosens. Bioelectron. 2021, 188, 113282. [Google Scholar] [CrossRef]
- Yu, F.; Yan, L.; Wang, N.; Yang, S.; Wang, L.; Tang, Y.; Gao, G.; Wang, S.; Ma, C.; Xie, R.; et al. Quantitative Detection and Viral Load Analysis of SARS-CoV-2 in Infected Patients. Clin. Infect. Dis. 2020, 71, 793–798. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Dai, C.; Wang, H.; Gao, Y.; Li, T.; Fang, Y.; Shen, Z.; Chen, L.; Chen, Z.; Ma, X.; et al. Analysis and Validation of a Highly Sensitive One-Step Nested Quantitative Real-Time Polymerase Chain Reaction Assay for Specific Detection of Severe Acute Respiratory Syndrome Coronavirus 2. Virol. J. 2020, 17, 197. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.B.; Choi, H.; Lee, G.D.; Lee, J.; Lee, S.; Kim, Y.; Cho, S.-Y.; Lee, D.-G.; Kim, M. Analytical and Clinical Performance of Droplet Digital PCR in the Detection and Quantification of SARS-CoV-2. Mol. Diagn. Ther. 2021, 25, 617–628. [Google Scholar] [CrossRef]
- Lee, C.-J.; Shin, W.; Mun, S.; Yu, M.; Choi, Y.-B.; Kim, D.H.; Han, K. Diagnostic Evaluation of QRT-PCR-Based Kit and DPCR-Based Kit for COVID-19. Genes Genom. 2021, 43, 1277–1288. [Google Scholar] [CrossRef]
- Alteri, C.; Cento, V.; Antonello, M.; Colagrossi, L.; Merli, M.; Ughi, N.; Renica, S.; Matarazzo, E.; Di Ruscio, F.; Tartaglione, L.; et al. Detection and Quantification of SARS-CoV-2 by Droplet Digital PCR in Real-Time PCR Negative Nasopharyngeal Swabs from Suspected COVID-19 Patients. PLoS ONE 2020, 15, e0236311. [Google Scholar] [CrossRef] [PubMed]
- Cassinari, K.; Alessandri-Gradt, E.; Chambon, P.; Charbonnier, F.; Gracias, S.; Beaussire, L.; Alexandre, K.; Sarafan-Vasseur, N.; Houdayer, C.; Etienne, M.; et al. Assessment of Multiplex Digital Droplet RT-PCR as a Diagnostic Tool for SARS-CoV-2 Detection in Nasopharyngeal Swabs and Saliva Samples. Clin. Chem. 2021, 67, 736–741. [Google Scholar] [CrossRef]
- Cento, V.; Renica, S.; Matarazzo, E.; Antonello, M.; Colagrossi, L.; Di Ruscio, F.; Pani, A.; Fanti, D.; Vismara, C.; Puoti, M.; et al. Frontline Screening for SARS-CoV-2 Infection at Emergency Department Admission by Third Generation Rapid Antigen Test: Can We Spare RT-QPCR? Viruses 2021, 13, 818. [Google Scholar] [CrossRef]
- Colagrossi, L.; Antonello, M.; Renica, S.; Merli, M.; Matarazzo, E.; Travi, G.; Vecchi, M.; Colombo, J.; Muscatello, A.; Grasselli, G.; et al. SARS-CoV-2 RNA in Plasma Samples of COVID-19 Affected Individuals: A Cross-Sectional Proof-of-Concept Study. BMC Infect. Dis. 2021, 21, 184. [Google Scholar] [CrossRef]
- De Kock, R.; Baselmans, M.; Scharnhorst, V.; Deiman, B. Sensitive Detection and Quantification of SARS-CoV-2 by Multiplex Droplet Digital RT-PCR. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 807–813. [Google Scholar] [CrossRef]
- Falzone, L.; Musso, N.; Gattuso, G.; Bongiorno, D.; Palermo, C.; Scalia, G.; Libra, M.; Stefani, S. Sensitivity Assessment of Droplet Digital PCR for SARS-CoV-2 Detection. Int. J. Mol. Med. 2020, 46, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Marchio, A.; Batejat, C.; Vanhomwegen, J.; Feher, M.; Grassin, Q.; Chazal, M.; Raulin, O.; Farges-Berth, A.; Reibel, F.; Estève, V.; et al. DdPCR Increases Detection of SARS-CoV-2 RNA in Patients with Low Viral Loads. Arch. Virol. 2021, 166, 2529–2540. [Google Scholar] [CrossRef]
- Martin, A.; Storto, A.; Le Hingrat, Q.; Collin, G.; André, B.; Mallory, A.; Dangla, R.; Descamps, D.; Visseaux, B.; Gossner, O. High-Sensitivity SARS-CoV-2 Group Testing by Digital PCR among Symptomatic Patients in Hospital Settings. J. Clin. Virol. 2021, 141, 104895. [Google Scholar] [CrossRef]
- Mio, C.; Cifù, A.; Marzinotto, S.; Marcon, B.; Pipan, C.; Damante, G.; Curcio, F. Validation of a One-Step Reverse Transcription-Droplet Digital PCR (RT-DdPCR) Approach to Detect and Quantify SARS-CoV-2 RNA in Nasopharyngeal Swabs. Dis. Markers 2021, 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Sabbatinelli, J.; Giuliani, A.; Matacchione, G.; Latini, S.; Laprovitera, N.; Pomponio, G.; Ferrarini, A.; Svegliati Baroni, S.; Pavani, M.; Moretti, M.; et al. Decreased Serum Levels of the Inflammaging Marker MiR-146a Are Associated with Clinical Non-Response to Tocilizumab in COVID-19 Patients. Mech. Ageing Dev. 2021, 193, 111413. [Google Scholar] [CrossRef] [PubMed]
- Scutari, R.; Piermatteo, L.; Manuelli, M.C.; Iannetta, M.; Salpini, R.; Bertoli, A.; Alteri, C.; Saccomandi, P.; Bellocchi, M.C.; Malagnino, V.; et al. Long-Term SARS-CoV-2 Infection Associated with Viral Dissemination in Different Body Fluids Including Bile in Two Patients with Acute Cholecystitis. Life 2020, 10, 302. [Google Scholar] [CrossRef]
- Szwebel, T.-A.; Veyer, D.; Robillard, N.; Eshagh, D.; Canoui, E.; Bruneau, T.; Contejean, A.; Azoulay, C.; Serrano, T.; Hueso, T.; et al. Usefulness of Plasma SARS-CoV-2 RNA Quantification by Droplet-Based Digital PCR to Monitor Treatment Against COVID-19 in a B-Cell Lymphoma Patient. Stem Cell Rev. Rep. 2021, 17, 296–299. [Google Scholar] [CrossRef]
- Tedim, A.P.; Almansa, R.; Domínguez-Gil, M.; González-Rivera, M.; Micheloud, D.; Ryan, P.; Méndez, R.; Blanca-López, N.; Pérez-García, F.; Bustamante, E.; et al. Comparison of Real-time and Droplet Digital PCR to Detect and Quantify SARS-CoV-2 RNA in Plasma. Eur. J. Clin. Investig. 2021, 51, e13501. [Google Scholar] [CrossRef]
- Veyer, D.; Kernéis, S.; Poulet, G.; Wack, M.; Robillard, N.; Taly, V.; L’Honneur, A.-S.; Rozenberg, F.; Laurent-Puig, P.; Bélec, L.; et al. Highly Sensitive Quantification of Plasma Severe Acute Respiratory Syndrome Coronavirus 2 RNA Sheds Light on Its Potential Clinical Value. Clin. Infect. Dis. 2020, 73, e2890–e2897. [Google Scholar] [CrossRef] [PubMed]
- Abasiyanik, M.F.; Flood, B.; Lin, J.; Ozcan, S.; Rouhani, S.J.; Pyzer, A.; Trujillo, J.; Zhen, C.; Wu, P.; Jumic, S.; et al. Sensitive Detection and Quantification of SARS-CoV-2 in Saliva. Sci. Rep. 2021, 11, 12425. [Google Scholar] [CrossRef]
- Bermejo-Martin, J.F.; González-Rivera, M.; Almansa, R.; Micheloud, D.; Tedim, A.P.; Domínguez-Gil, M.; Resino, S.; Martín-Fernández, M.; Ryan Murua, P.; Pérez-García, F.; et al. Viral RNA Load in Plasma Is Associated with Critical Illness and a Dysregulated Host Response in COVID-19. Crit. Care 2020, 24, 691. [Google Scholar] [CrossRef] [PubMed]
- Gniazdowski, V.; Paul Morris, C.; Wohl, S.; Mehoke, T.; Ramakrishnan, S.; Thielen, P.; Powell, H.; Smith, B.; Armstrong, D.T.; Herrera, M.; et al. Repeated Coronavirus Disease 2019 Molecular Testing: Correlation of Severe Acute Respiratory Syndrome Coronavirus 2 Culture With Molecular Assays and Cycle Thresholds. Clin. Infect. Dis. 2021, 73, e860–e869. [Google Scholar] [CrossRef]
- Poggio, P.; Songia, P.; Vavassori, C.; Ricci, V.; Banfi, C.; Barbieri, S.S.; Garoffolo, G.; Myasoedova, V.A.; Piacentini, L.; Raucci, A.; et al. Digital PCR for High Sensitivity Viral Detection in False-Negative SARS-CoV-2 Patients. Sci. Rep. 2021, 11, 4310. [Google Scholar] [CrossRef] [PubMed]
- Ram-Mohan, N.; Kim, D.; Zudock, E.J.; Hashemi, M.M.; Tjandra, K.C.; Rogers, A.J.; Blish, C.A.; Nadeau, K.C.; Newberry, J.A.; Quinn, J.V.; et al. SARS-CoV-2 RNAemia Predicts Clinical Deterioration and Extrapulmonary Complications from COVID-19. Clin. Infect. Dis. 2021, in press. [Google Scholar] [CrossRef]
- Savela, E.S.; Winnett, A.; Romano, A.E.; Porter, M.K.; Shelby, N.; Akana, R.; Ji, J.; Cooper, M.M.; Schlenker, N.W.; Reyes, J.A.; et al. Quantitative SARS-CoV-2 Viral-Load Curves in Paired Saliva and Nasal Swabs Inform. Appropriate Respiratory Sampling Site and Analytical Test. Sensitivity Required for Earliest Viral Detection. medRxiv 2021. [Google Scholar] [CrossRef]
- Xu, J.; Kirtek, T.; Xu, Y.; Zheng, H.; Yao, H.; Ostman, E.; Oliver, D.; Malter, J.S.; Gagan, J.R.; SoRelle, J.A. Digital Droplet PCR for SARS-CoV-2 Resolves Borderline Cases. Am. J. Clin. Pathol. 2021, 155, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Rosas, A.; Benitez-Guerrero, T.; Corona-Cervantes, K.; Vélez-Ixta, J.M.; Zavala-Torres, N.G.; Cuenca-Leija, J.; Martínez-Pichardo, S.; Landero-Montes-de-Oca, M.E.; Bastida-González, F.G.; Zárate-Segura, P.B.; et al. Study of Perinatal Transmission of SARS-CoV-2 in a Mexican Public Hospital. Int. J. Infect. Dis. 2021, 113, 225–232. [Google Scholar] [CrossRef]
- Duong, K.; Ou, J.; Li, Z.; Lv, Z.; Dong, H.; Hu, T.; Zhang, Y.; Hanna, A.; Gordon, S.; Crynen, G.; et al. Increased Sensitivity Using Real-Time DPCR for Detection of SARS-CoV-2. BioTechniques 2021, 70, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Au, W.Y.; Cheung, P.P.H. Diagnostic Performances of Common Nucleic Acid Tests for SARS-CoV-2 in Hospitals and Clinics: A Systematic Review and Meta-Analysis. Lancet Microbe 2021, 12, e704–e714. [Google Scholar] [CrossRef]
- Kojabad, A.A.; Farzanehpour, M.; Galeh, H.E.G.; Dorostkar, R.; Jafarpour, A.; Bolandian, M.; Nodooshan, M.M. Droplet Digital PCR of Viral DNA/RNA, Current Progress, Challenges, and Future Perspectives. J. Med. Virol. 2021, 93, 4182–4197. [Google Scholar] [CrossRef]
- Zhao, Y.; Xia, Q.; Yin, Y.; Wang, Z. Comparison of Droplet Digital PCR and Quantitative PCR Assays for Quantitative Detection of Xanthomonas Citri Subsp. Citri. PLoS ONE 2016, 11, e0159004. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Pan, H.; Xu, X.; Lv, P.; Wang, X.; Zhao, Z. Droplet Digital PCR (DdPCR) for the Detection and Quantification of Ureaplasma Spp. BMC Infect. Dis. 2021, 21, 804. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yao, H.; Xu, X.; Zhang, P.; Zhang, M.; Shao, J.; Xiao, Y.; Wang, H. Limits of Detection of 6 Approved RT–PCR Kits for the Novel SARS-Coronavirus-2 (SARS-CoV-2). Clin. Chem. 2020, 66, 977–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokkoris, V.; Vukicevich, E.; Richards, A.; Thomsen, C.; Hart, M.M. Challenges Using Droplet Digital PCR for Environmental Samples. Appl. Microbiol. 2021, 1, 74–88. [Google Scholar] [CrossRef]
- Sanders, R.; Mason, D.J.; Foy, C.A.; Huggett, J.F. Evaluation of Digital PCR for Absolute RNA Quantification. PLoS ONE 2013, 8, e75296. [Google Scholar] [CrossRef] [PubMed]
- Colozza-Gama, G.A.; Callegari, F.; Bešič, N.; de J Paniza, A.C.; Cerutti, J.M. Machine Learning Algorithm Improved Automated Droplet Classification of DdPCR for Detection of BRAF V600E in Paraffin-Embedded Samples. Sci. Rep. 2021, 11, 12648. [Google Scholar] [CrossRef] [PubMed]
- Kilic, T.; Weissleder, R.; Lee, H. Molecular and Immunological Diagnostic Tests of COVID-19: Current Status and Challenges. Iscience 2020, 23, 101406. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Odiwuor, N.; Xiong, J.; Sun, L.; Nyaruaba, R.O.; Wei, H.; Tanner, N.A. Rapid Molecular Detection of SARS-CoV-2 (COVID-19) Virus RNA Using Colorimetric LAMP. medRxiv 2020. [Google Scholar] [CrossRef]
- Li, L.; Tan, C.; Zeng, J.; Luo, C.; Hu, S.; Peng, Y.; Li, W.; Xie, Z.; Ling, Y.; Zhang, X.; et al. Analysis of Viral Load in Different Specimen Types and Serum Antibody Levels of COVID-19 Patients. J. Transl. Med. 2021, 19, 30. [Google Scholar] [CrossRef] [PubMed]
- Boehm, E.; Kronig, I.; Neher, R.A.; Eckerle, I.; Vetter, P.; Kaiser, L. Novel SARS-CoV-2 Variants: The Pandemics within the Pandemic. Clin. Microbiol. Infect. 2021, 27, 1109–1117. [Google Scholar] [CrossRef]
- Heijnen, L.; Elsinga, G.; de Graaf, M.; Molenkamp, R.; Koopmans, M.P.G.; Medema, G. Droplet Digital RT-PCR to Detect SARS-CoV-2 Signature Mutations of Variants of Concern in Wastewater. Sci. Total Environ. 2021, 799, 149456. [Google Scholar] [CrossRef]
- Perchetti, G.A.; Zhu, H.; Mills, M.G.; Shrestha, L.; Wagner, C.; Bakhash, S.M.; Lin, M.J.; Xie, H.; Huang, M.; Mathias, P.; et al. Specific Allelic Discrimination of N501Y and Other SARS-CoV-2 Mutations by DdPCR Detects B.1.1.7 Lineage in Washington State. J. Med. Virol. 2021, 93, 5931–5941. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wohlin, C. Guidelines for Snowballing in Systematic Literature Studies and a Replication in Software Engineering. In Proceedings of the 18th International Conference on Evaluation and Assessment in Software Engineering—EASE ’14, London, UK, 13–14 May 2014; ACM Press: London, UK; New York, NY, USA, 2014; pp. 1–10. [Google Scholar]



{kind=link}
{kind=link}
| First Author (Year) | Number of Patients (Samples) | Sources of Samples | Summary of Results | |
|---|---|---|---|---|
| Patients (Samples) | Controls | |||
| Abasiyanik et al. (2020) [48] | 166 | N/A | Nasopharyngeal swabs Saliva |
|
| Alteri et al. (2020) [34] | 55 (100) | N/A | Nasopharyngeal swabs |
|
| Cassinari et al. (2021) [35] | 130 | N/A | Nasopharyngeal swabs Saliva |
|
| Cento et al. (2021) [36] | 960 (960) | N/A | Nasopharyngeal swabs |
|
| Chen et al. (2021) [20] | 52 (87) | N/A | Blood Oropharyngeal swabs |
|
| Dang et al. (2020) [21] | 30 (117) | 61 | Pharyngeal swabs Sputum |
|
| de Kock et al. (2020) [38] | 5 samples | 5 samples | Nasopharyngeal swabs |
|
| Dong et al. (2021) [22] | 103 (196) | N/A | Pharyngeal swabs |
|
| Duong et al. (2021) [56] | 20 (60) | 12 | Nasopharyngeal swabs |
|
| Falzone et al. (2020) [39] | 1 (multiple dilutions) | 1 (multiple dilutions) | Nasopharyngeal swabs |
|
| Gniazdowski et al. (2020) [50] | 185 | N/A | Nasopharyngeal swabs |
|
| Jiang et al. (2020) [24] | 10 (32) | N/A | Nasopharyngeal swabs Oropharyngeal swabs Blood |
|
| Kim et al. (2021) [32] | 366 samples | N/A | Nasopharyngeal swabs Sputum samples Blood samples |
|
| Lee et al. (2021) [33] | 20 | 20 | Pharyngeal swabs Sputum samples |
|
| Liu et al. (2020) [25] | 43 (74) | N/A | Stool samples Sputum samples Throat swabs |
|
| Liu et al. (2020) [26] * | N/A | N/A | Nasopharyngeal swabs |
|
| Marchio et al. (2021) [40] | 208 samples | N/A | Nasopharyngeal swabs |
|
| Martin et al. (2021) [41] | 448 samples | N/A | Nasopharyngeal swabs |
|
| Mio et al. (2021) [42] | 90 | N/A | Nasopharyngeal swabs |
|
| Nyaruaba et al. (2020) [27] | 94 samples | N/A | Oropharyngeal swabs |
|
| Park et al. (2021) [19] | 5 (8) | N/A | Nasopharyngeal swabs Oropharyngeal swabs |
|
| Poggio et al. (2021) [51] | 64 | N/A | Nasopharyngeal swabs |
|
| Ramirez-Rosas et al. (2021) [55] | 404 samples | N/A | Nasopharyngeal swabs Colostrum samples |
|
| Savela et al. (2021) [53] | 7 (105) | N/A | Saliva Nasopharyngeal swabs |
|
| Scutari et al. (2020) [44] | 2 | N/A | Nasopharyngeal swabs Rectal swabs Urine Bile Plasma |
|
| Sun et al. (2021) [28] | 21 | 6 | Throat swabs Sputum swabs Anal swabs |
|
| Suo et al. (2020) [12] | 77 | N/A | Throat swabs |
|
| Szwebel et al. (2021) [45] | 1 | N/A | Nasopharyngeal swabs BAL Plasma |
|
| Tedim et al. (2021) [46] | 90 | N/A | Nasopharyngeal swabs Plasma |
|
| Xu et al. (2021) [54] | 30 samples | 30 samples | Nasopharyngeal swabs |
|
| Yin et al. (2021) [29] | 6 | 3 | Throat swabs |
|
| Yu et al. (2020) [30] | 76 (323) | N/A | Nasal swabs Throat swabs Sputum Blood Urine |
|
| Zhang et al. (2020) [31] | 24 (34) | N/A | Throat swabs Anal swabs Sputum Blood |
|
| Author (Year) | Number of Samples | Source of Sample | Summary of Results | |
|---|---|---|---|---|
| Patients (Samples) | Controls | |||
| Bermejo-Martin et al. (2020) [49] | 250 | N/A | Plasma |
|
| Chen et al. (2021) [20] | 52 (87) | N/A | Plasma Oropharyngeal swabs |
|
| Colagrossi et al. (2021) [37] | 41 | N/A | Nasopharyngeal swabs BAL Plasma |
|
| Hu et al. (2020) [23] | 47 | N/A | Throat swabs Deep sputum |
|
| Ram-Mohan et al. (2021) [52] | 191 | N/A | Nasopharyngeal swabs Plasma |
|
| Sabbatinelli et al. (2021) [43] | 30 | N/A | Serum |
|
| Szwebel et al. (2021) [45] | 1 | N/A | Nasopharyngeal swabs BAL Plasma |
|
| Tedim et al. (2021) [46] | 90 | N/A | Nasopharyngeal swabs Plasma |
|
| Veyer et al. (2020) [47] | 58 | 12 | Plasma |
|
| Yu et al. (2020) [30] | 76 (323) | N/A | Nasal swabs Throat swabs Sputum Blood Urine |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishak, A.; AlRawashdeh, M.M.; Esagian, S.M.; Nikas, I.P. Diagnostic, Prognostic, and Therapeutic Value of Droplet Digital PCR (ddPCR) in COVID-19 Patients: A Systematic Review. J. Clin. Med. 2021, 10, 5712. https://doi.org/10.3390/jcm10235712
Ishak A, AlRawashdeh MM, Esagian SM, Nikas IP. Diagnostic, Prognostic, and Therapeutic Value of Droplet Digital PCR (ddPCR) in COVID-19 Patients: A Systematic Review. Journal of Clinical Medicine. 2021; 10(23):5712. https://doi.org/10.3390/jcm10235712
Chicago/Turabian StyleIshak, Angela, Mousa M. AlRawashdeh, Stepan M. Esagian, and Ilias P. Nikas. 2021. "Diagnostic, Prognostic, and Therapeutic Value of Droplet Digital PCR (ddPCR) in COVID-19 Patients: A Systematic Review" Journal of Clinical Medicine 10, no. 23: 5712. https://doi.org/10.3390/jcm10235712
APA StyleIshak, A., AlRawashdeh, M. M., Esagian, S. M., & Nikas, I. P. (2021). Diagnostic, Prognostic, and Therapeutic Value of Droplet Digital PCR (ddPCR) in COVID-19 Patients: A Systematic Review. Journal of Clinical Medicine, 10(23), 5712. https://doi.org/10.3390/jcm10235712