
Risk Due to ABO Incompatibility and Donor-Recipient Weight Mismatch in Living Donor Kidney Transplantation: A National Cohort Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
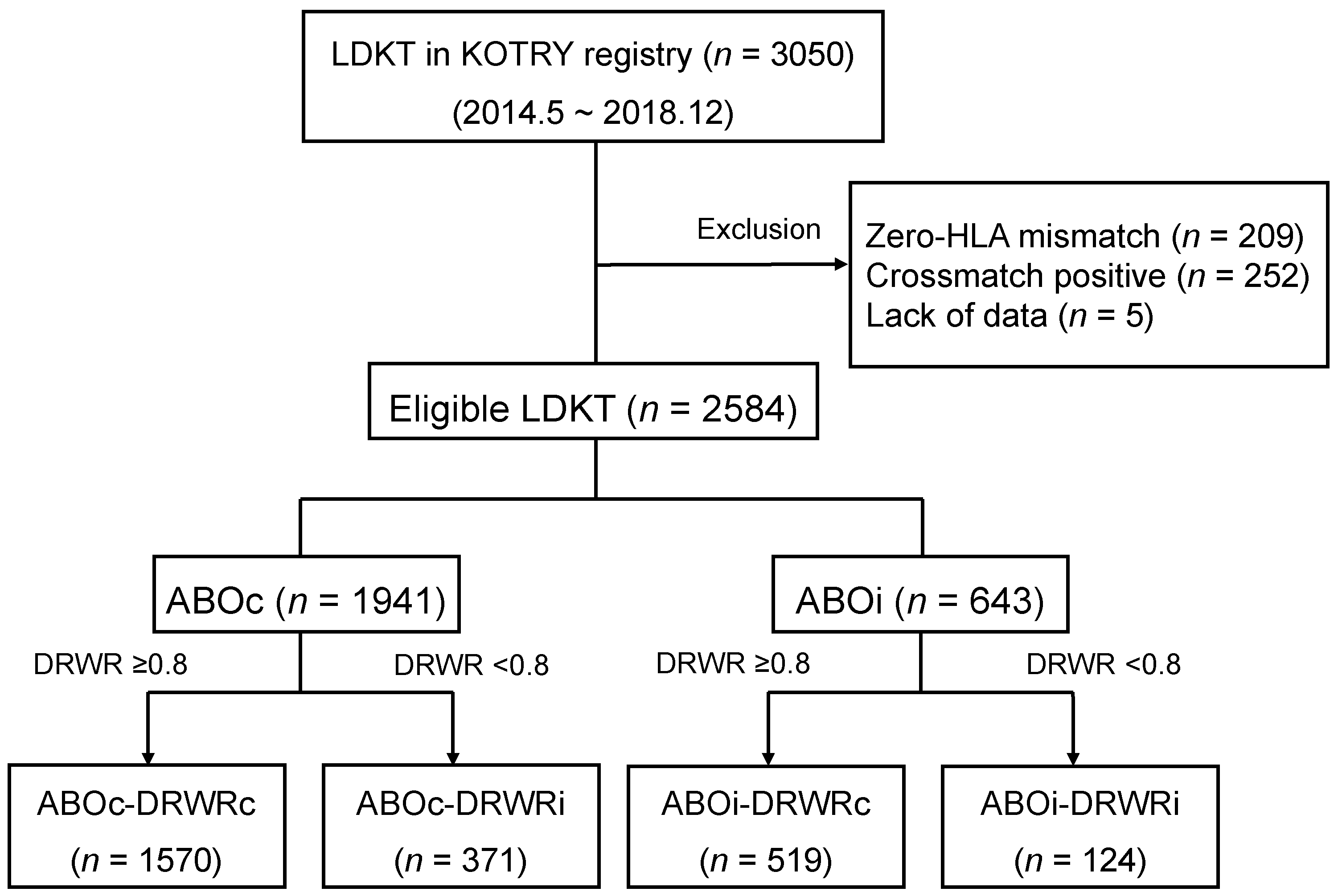
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
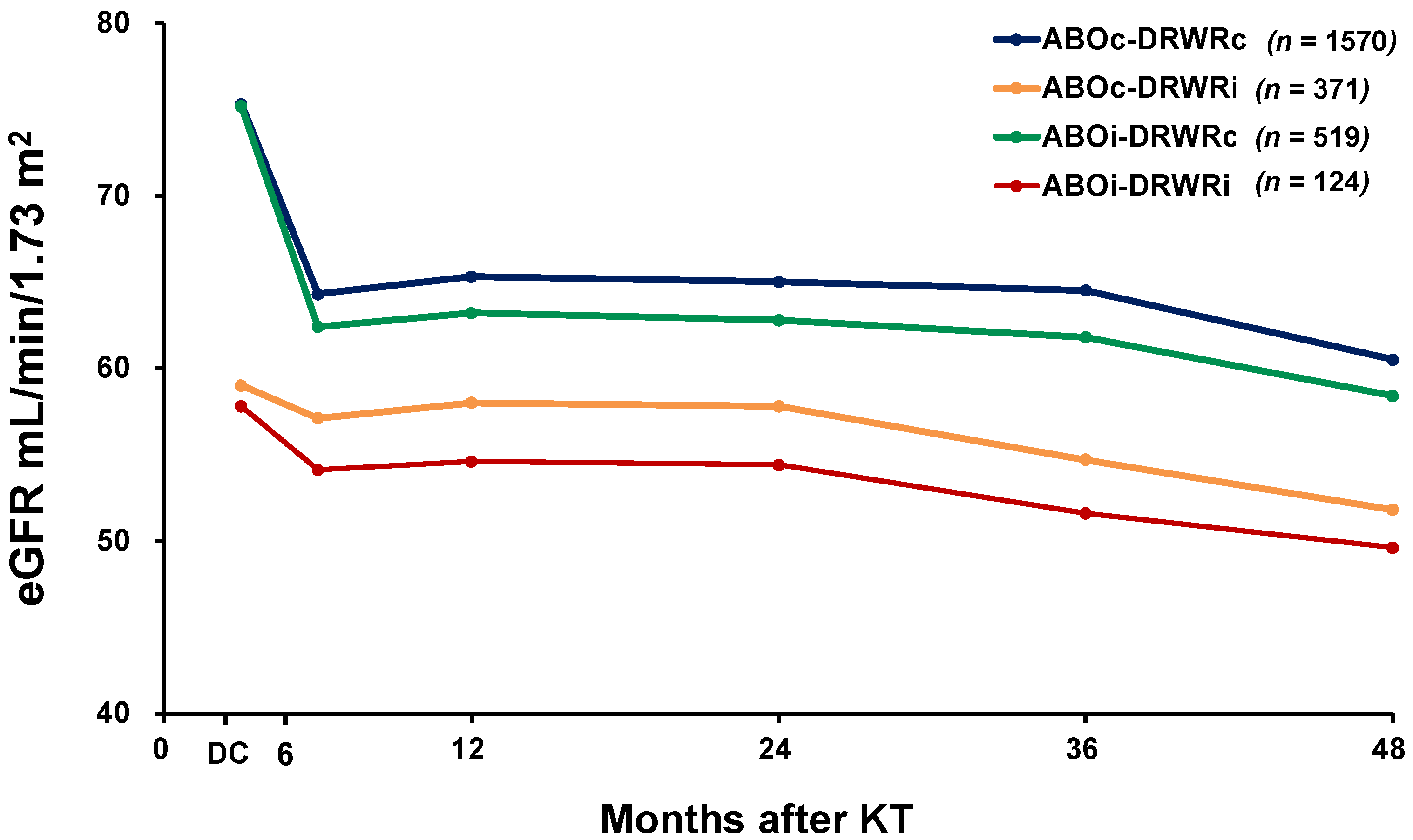
3.2. Graft Function
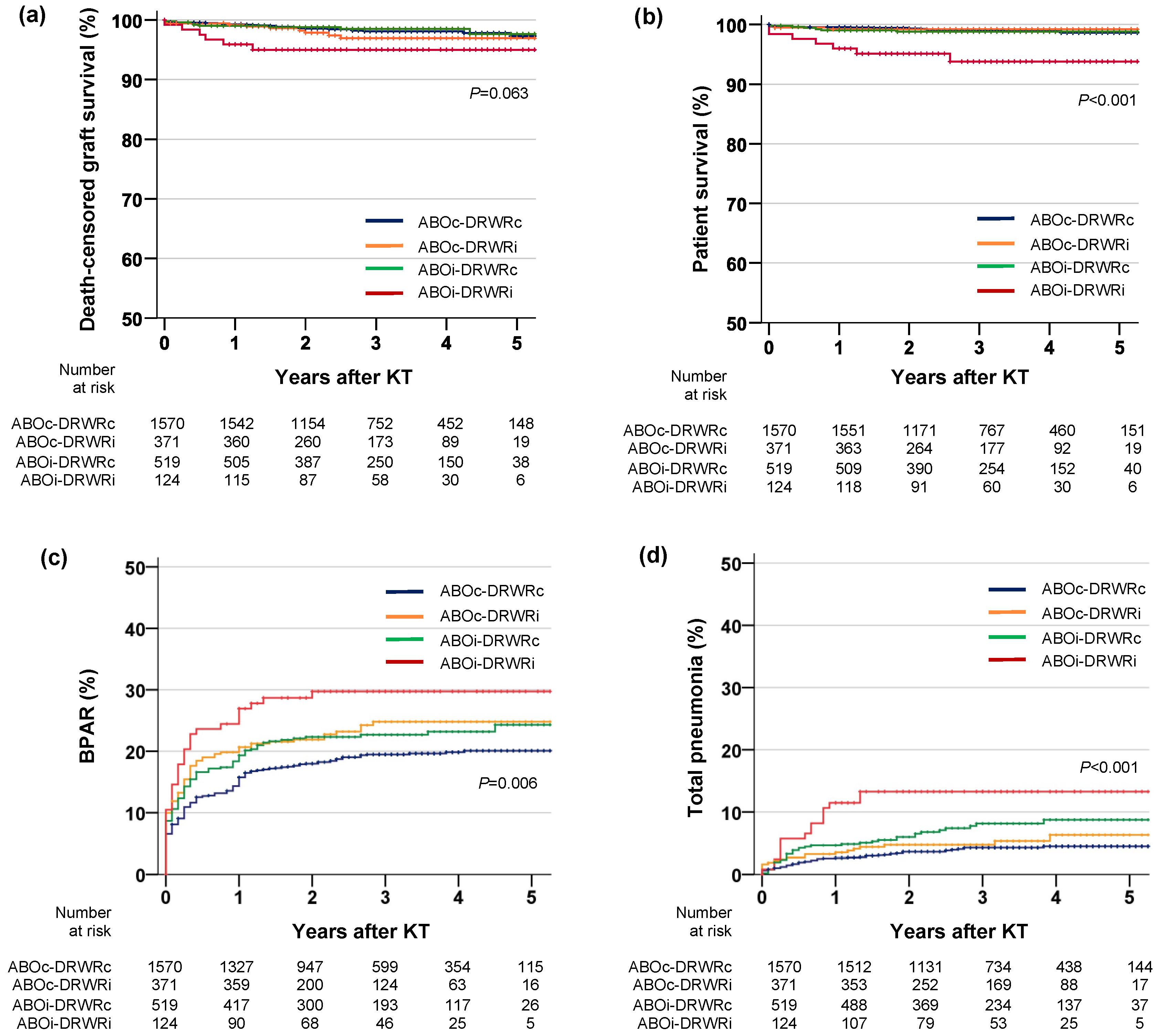
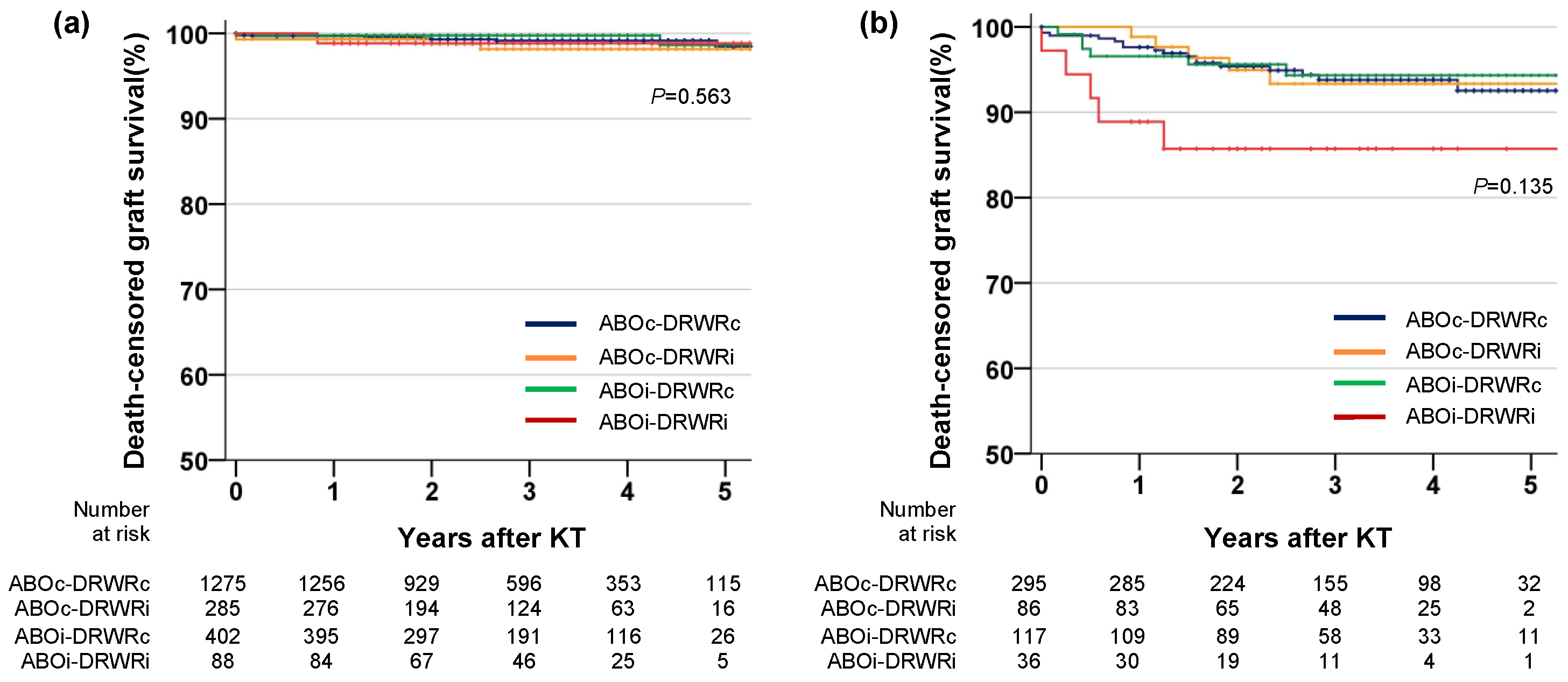
3.3. Graft Survival
3.4. Patient Survival
3.5. Biopsy-Proven Acute Rejection
3.6. Infection
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic review: Kidney transplantation compared with dialysis in clinically relevant outcomes. Am. J. Transplant. 2011, 11, 2093–2109. [Google Scholar] [CrossRef]
- Takahashi, K.; Saito, K.; Takahara, S.; Okuyama, A.; Tanabe, K.; Toma, H.; Uchida, K.; Hasegawa, A.; Yoshimura, N.; Kamiryo, Y.; et al. Excellent long-term outcome of ABO-incompatible living donor kidney transplantation in Japan. Am. J. Transplant. 2004, 4, 1089–1096. [Google Scholar] [CrossRef]
- Speer, C.; Kälble, F.; Nusshag, C.; da Silva, L.P.; Schaier, M.; Becker, L.E.; Klein, K.; Sommerer, C.; Beimler, J.; Leo, A.; et al. Outcomes and complications following ABO-incompatible kidney transplantation performed after desensitization by semi-selective immunoadsorption—A retrospective study. Transpl. Int. 2019, 32, 1286–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Weerd, A.E.; Betjes, M.G.H. ABO-incompatible kidney transplant outcomes: A meta-analysis. Clin. J. Am. Soc. Nephrol. 2018, 13, 1234. [Google Scholar] [CrossRef] [PubMed]
- Song, S.H.; Lee, J.; Kim, B.S.; Kim, S.; Lee, J.G.; Jeong, H.J.; Kim, Y.S.; Kim, M.S.; Kim, H.O.; Kim, S.I.; et al. Successful launch of an ABO-incompatible kidney transplantation program to overcome the shortage of compatible living donors: Experience at a single center. Clin. Nephrol. 2017, 88, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Opelz, G.; Morath, C.; Süsal, C.; Tran, T.H.; Zeier, M.; Döhler, B. Three-year outcomes following 1420 ABO-incompatible living-donor kidney transplants performed after ABO antibody reduction: Results from 101 centers. Transplantation 2015, 99, 400. [Google Scholar] [CrossRef]
- Kong, J.M.; Ahn, J.; Park, J.B.; Chung, B.-H.; Yang, J.; Kim, J.K.; Huh, K.H.; Kim, J.M. ABO incompatible living donor kidney transplantation in Korea: Highly uniform protocols and good medium-term outcome. Clin. Transplant. 2013, 27, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, J.R.; Berger, J.C.; Warren, D.S.; James, N.T.; Montgomery, R.A.; Segev, D.L. Outcomes of ABO-incompatible kidney transplantation in the United States. Transplantation 2012, 93, 603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genberg, H.; Kumlien, G.; Wennberg, L.; Tyden, G. The efficacy of antigen-specific immunoadsorption and rebound of anti-A/B antibodies in ABO-incompatible kidney transplantation. Nephrol. Dial. Transplant. 2011, 26, 2394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scurt, F.G.; Ewert, L.; Mertens, P.R.; Haller, H.; Schmidt, B.M.W.; Chatzikyrkou, C. Clinical outcomes after ABO-incompatible renal transplantation: A systematic review and meta-analysis. Lancet 2019, 393, 2059–2072. [Google Scholar] [CrossRef]
- Massie, A.B.; Orandi, B.J.; Waldram, M.M.; Luo, X.; Nguyen, A.Q.; Montgomery, R.A.; Lentine, K.L.; Segev, D.L. Impact of ABO-incompatible living donor kidney transplantation on patient survival. Am. J. Kidney Dis. 2020, 76, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, V.A.; Brenner, B.M. The clinical importance of nephron mass. J. Am. Soc. Nephrol. 2010, 21, 898–910. [Google Scholar] [CrossRef] [Green Version]
- Azuma, H.; Nadeau, K.; Mackenzie, H.S.; Brenner, B.M.; Tilney, N.L. Nephron mass modulates the hemodynamic, cellular, and molecular response of the rat renal allograft1. Transplantation 1997, 63, 519–528. [Google Scholar] [CrossRef]
- Brenner, B.M.; Milford, E.L. Nephron underdosing: A programmed cause of chronic renal allograft failure. Am. J. Kidney Dis. 1993, 21, 66–72. [Google Scholar] [CrossRef]
- McNamara, B.; Diouf, B.; Hughson, M.; Hoy, W.; Bertram, J.F. Associations between age, body size and nephron number with individual glomerular volumes in urban West African males. Nephrol. Dial. Transplant. 2009, 24, 1500–1506. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.J.; Kiberd, B.A.; Alwayn, I.P.; Odutayo, A.; Tennankore, K.K. Donor-recipient weight and sex mismatch and the risk of graft loss in renal transplantation. Clin. J. Am. Soc. Nephrol. 2017, 12, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.J.; Smits, G.; Wiseman, A.C. Long-term impact of donor-recipient size mismatching in deceased donor kidney transplantation and in expanded criteria donor recipients. Transplantation 2010, 90, 867–874. [Google Scholar] [CrossRef]
- Giral, M.; Foucher, Y.; Karam, G.; Labrune, Y.; Kessler, M.; de Ligny, B.H.; Büchler, M.; Bayle, F.; Meyer, C.; Trehet, N.; et al. Kidney and recipient weight incompatibility reduces long-term graft survival. J. Am. Soc. Nephrol. 2010, 21, 1022–1029. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Moon, J.I.; Kim, D.K.; Kim, S.I.; Park, K. Ratio of donor kidney weight to recipient bodyweight as an index of graft function. Lancet 2001, 357, 1180–1181. [Google Scholar] [CrossRef]
- Yang, J.; Jeong, J.C.; Lee, J.; Kim, Y.H.; Paik, H.C.; Kim, J.-J.; Park, H.-Y.; Kim, M.S.; Ahn, C. Design and methods of the Korean organ transplantation registry. Transplant. Direct 2017, 3, e191. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Kim, D.G.; Lee, J.; Kim, M.S.; Kwon, O.J.; Jung, C.W.; Lee, K.W.; Yang, J.; Ahn, C.; Huh, K.H. The Korean organ transplantation registry study group outcomes of ABO-incompatible kidney transplantation in older patients: A national cohort study. Transpl. Int. 2021, 34, 290–301. [Google Scholar] [CrossRef] [PubMed]
- Buttigieg, J.; Ali, H.; Sharma, A.; Halawa, A. Positive Luminex and negative flow cytometry in kidney transplantation: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2018, 34, 1950–1960. [Google Scholar] [CrossRef] [PubMed]
- Van den Hoogen, M.W.; Kamburova, E.G.; Baas, M.C.; Steenbergen, E.J.; Florquin, S.M.; Koenen, H.J.P.; Hilbrands, L.B. Rituximab as induction therapy after renal transplantation: A randomized, double-blind, placebo-controlled study of efficacy and safety. Am. J. Transplant. 2015, 15, 407. [Google Scholar] [CrossRef]
- Ko, E.J.; Yu, J.H.; Yang, C.W.; Chung, B.H. The Korean organ transplantation registry study group clinical outcomes of ABO- and HLA-incompatible kidney transplantation: A nationwide cohort study. Transpl. Int. 2017, 30, 1215–1225. [Google Scholar] [CrossRef] [PubMed]
- El-Agroudy, A.E.; Hassan, N.A.; Bakr, M.A.; Foda, M.A.; Shokeir, A.A.; Shehab el-Dein, A.B. Effect of donor/recipient body weight mismatch on patient and graft outcome in living-donor kidney transplantation. Am. J. Nephrol. 2003, 23, 294. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Snyder, J.J.; Gilbertson, D. Inadequate donor size in cadaver kidney transplantation. J. Am. Soc. Nephrol. 2002, 13, 2152–2159. [Google Scholar] [CrossRef]
- Arshad, A.; Hodson, J.; Chappelow, I.; Nath, J.; Sharif, A. The influence of donor to recipient size matching on kidney transplant outcomes. Transplant. Direct 2018, 4, e391. [Google Scholar] [CrossRef] [PubMed]
- Massie, A.B.; Leanza, J.; Fahmy, L.M.; Chow, E.; Desai, N.M.; Luo, X.; King, E.A.; Bowring, M.; Segev, D.L. A risk index for living donor kidney transplantation. Am. J. Transplant. 2016, 16, 2077–2084. [Google Scholar] [CrossRef] [Green Version]
- Sureshkumar, K.K.; Chopra, B.; Josephson, M.A.; Shah, P.B.; McGill, R.L. Recipient obesity and kidney transplant outcomes: A mate-kidney analysis. Am. J. Kidney Dis. 2021, 78, 501–510.e1. [Google Scholar] [CrossRef]
- Yacoub, R.; Nadkarni, G.N.; Cravedi, P.; He, J.C.; Delaney, V.B.; Kent, R.; Chauhan, K.N.; Coca, S.G.; Florman, S.S.; Heeger, P.S.; et al. Analysis of OPTN/UNOS registry suggests the number of HLA matches and not mismatches is a stronger independent predictor of kidney transplant survival. Kidney Int. 2018, 93, 482–490. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | ABOc-DRWRc (n = 1570) | ABOc-DRWRi (n = 371) | ABOi-DRWRc (n = 519) | ABOi-DRWRi (n = 124) | p |
|---|---|---|---|---|---|
| Age, years | 47.6 ± 12.2 | 47.1 ± 10.7 | 47.6 ± 12.5 | 49.8 ± 9.2 | 0.192 |
| Sex, male | 847 (53.9) | 345 (93.0) | 277 (53.4) | 116 (93.5) | <0.001 |
| BMI, kg/m2 | 22.5 ± 3.3 | 26.6 ± 3.4 | 22.3 ± 3.3 | 26.3 ± 3.6 | <0.001 |
| Donor age, years | 45.6 ± 12.2 | 48.0 ± 9.9 | 47.0 ± 12.1 | 47.6 ± 9.7 | 0.001 |
| Donor sex, male | 804 (51.2) | 30 (8.1) | 261 (50.3) | 8 (6.5) | <0.001 |
| Donor BMI, kg/m2 | 24.7 ± 3.1 | 22.2 ± 2.4 | 24.5 ± 3.2 | 22.1 ± 2.3 | <0.001 |
| Recipient-donor relationship | <0.001 | ||||
| Unrelated | 596 (38.0) | 213 (57.4) | 278 (53.6) | 98 (79.0) | |
| Related | 974 (62.0) | 158 (42.6) | 241 (46.4) | 26 (21.0) | |
| Recipient-donor relationship-detail | <0.001 | ||||
| Spouse | 487 (31.0) | 195 (52.6) | 248 (47.8) | 91 (73.4) | |
| Parent | 280 (17.8) | 61 (16.4) | 91 (17.5) | 10 (8.1) | |
| Offspring | 345 (22.0) | 28 (7.5) | 79 (15.2) | 7 (5.6) | |
| Sibling | 349 (22.3) | 69 (18.6) | 71 (13.7) | 9 (7.3) | |
| Other unrelated | 109 (6.9) | 18 (4.9) | 30 (5.8) | 7 (5.6) | |
| Number of HLA mismatch (for A/B/DR) | 3.6 ± 1.4 | 3.9 ± 1.5 | 3.9 ± 1.5 | 4.3 ± 1.4 | <0.001 |
| Cause of ESRD | 0.001 | ||||
| Diabetes | 343 (21.8) | 120 (32.3) | 126 (24.3) | 40 (32.3) | |
| Hypertension | 214 (13.6) | 51 (13.7) | 61 (11.8) | 21 (16.9) | |
| Glomerular disease | 568 (36.2) | 100 (27.0) | 181 (34.9) | 33 (26.6) | |
| PCKD | 74 (4.7) | 22 (5.9) | 30 (5.8) | 8 (6.5) | |
| Other disease | 48 (3.1) | 4 (1.1) | 19 (3.7) | 3 (2.4) | |
| Unknown | 323 (20.6) | 74 (19.9) | 102 (19.7) | 19 (15.3) | |
| Dialysis duration, months | 17.8 ± 35.7 | 14.5 ± 34.5 | 17.7 ± 36.3 | 11.5 ± 23.4 | 0.110 |
| Retransplantation | 114 (7.3) | 7 (1.9) | 28 (5.4) | 3 (2.4) | <0.001 |
| Diabetes | 441 (28.1) | 147 (39.6) | 162 (31.2) | 53 (42.7) | <0.001 |
| Hypertension | 1388 (88.4) | 348 (93.8) | 467 (90.0) | 121 (97.6) | <0.001 |
| CVD | 134 (8.5) | 48 (12.9) | 43 (8.3) | 13 (10.5) | 0.050 |
| XM-DSA+ | 84 (5.4) | 6 (1.6) | 50 (9.6) | 8 (6.5) | <0.001 |
| Induction agent | 0.330 | ||||
| IL-2 receptor antibody | 1390 (88.5) | 339 (91.4) | 463 (89.2) | 107 (86.3) | |
| Anti-thymocyte globulin | 180 (11.5) | 32 (8.6) | 56 (10.8) | 17 (13.7) |
| Univariable Cox | Multivariable Cox | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p | HR (95% CI) | p |
| For death-censored graft survival a | ||||
| ABOi vs. ABOc | 1.18 (0.64–2.19) | 0.601 | 1.10 (0.59–2.04) | 0.770 |
| DRWRi vs. DRWRc | 1.87 (1.02–3.43) | 0.042 | 1.75 (0.95–3.23) | 0.074 |
| ABOc-DRWRc | Reference | Reference | ||
| ABOc-DRWRi | 1.46 (0.69–3.10) | 0.327 | 1.32 (0.62–2.83) | 0.469 |
| ABOi-DRWRc | 0.90 (0.41–1.98) | 0.791 | 0.82 (0.37–1.81) | 0.624 |
| ABOi-DRWRi | 2.94 (1.21–7.12) | 0.017 | 2.73 (1.11–6.70) | 0.028 |
| For patient survival b | ||||
| ABOi vs. ABOc | 2.18 (1.07–4.45) | 0.032 | 1.65 (0.79–3.42) | 0.181 |
| DRWRi vs. DRWRc | 2.05 (0.96–4.34) | 0.063 | 1.64 (0.75–3.59) | 0.214 |
| ABOc-DRWRc | Reference | Reference | ||
| ABOc-DRWRi | 0.86 (0.25–2.97) | 0.813 | 0.67 (0.19–2.35) | 0.533 |
| ABOi-DRWRc | 1.21 (0.47–3.12) | 0.693 | 0.93 (0.35–2.42) | 0.875 |
| ABOi-DRWRi | 6.02 (2.46–14.77) | <0.001 | 3.55 (1.39–9.04) | 0.008 |
| For BPAR c | ||||
| ABOi vs. ABOc | 1.24 (1.03–1.50) | 0.024 | 1.14 (0.94–1.38) | 0.190 |
| DRWRi vs. DRWRc | 1.31 (1.07–1.60) | 0.009 | 1.05 (0.84–1.31) | 0.661 |
| ABOc-DRWRc | Reference | Reference | ||
| ABOc-DRWRi | 1.29 (1.02–1.64) | 0.037 | 1.02 (0.79–1.32) | 0.879 |
| ABOi-DRWRc | 1.23 (0.99–1.52) | 0.060 | 1.11 (0.89–1.38) | 0.355 |
| ABOi-DRWRi | 1.66 (1.17–2.34) | 0.004 | 1.27 (0.88–1.82) | 0.203 |
| For pneumonia d | ||||
| ABOi vs. ABOc | 2.08 (1.47–2.93) | <0.001 | 2.02 (1.42–2.87) | <0.001 |
| DRWRi vs. DRWRc | 1.53 (1.04–2.25) | 0.030 | 1.28 (0.85–1.94) | 0.235 |
| ABOc-DRWRc | Reference | Reference | ||
| ABOc-DRWRi | 1.34 (0.80–2.25) | 0.262 | 1.15 (0.67–1.97) | 0.605 |
| ABOi-DRWRc | 1.91 (1.27–2.86) | 0.002 | 1.87 (1.24–2.82) | 0.003 |
| ABOi-DRWRi | 3.53 (2.04–6.12) | <0.001 | 2.94 (1.64–5.57) | <0.001 |
| Variables | ABOc-DRWRc (n = 1570) | ABOc-DRWRi (n = 371) | ABOi-DRWRc (n = 519) | ABOi-DRWRi (n = 124) | p |
|---|---|---|---|---|---|
| Total infections | 321 (20.4) | 85 (22.9) | 118 (22.7) | 30 (24.2) | 0.480 |
| Urinary tract infection | 152 (9.7) | 37 (10.0) | 66 (12.7) | 9 (7.3) | 0.155 |
| Bacterial pneumonia | 21 (1.3) | 8 (2.2) | 10 (1.9) | 9 (7.6) | <0.001 |
| Bacteremia | 6 (0.4) | 4 (1.1) | 6 (1.2) | 2 (1.6) | 0.106 |
| Viral infection | 142 (9.0) | 37 (10.0) | 44 (8.5) | 17 (13.7) | 0.308 |
| Viral pneumonia | 6 (0.4) | 2 (0.5) | 9 (1.7) | 4 (3.2) | 0.001 |
| Fungal infection | 11 (0.7) | 3 (0.8) | 7 (1.3) | 2 (1.6) | 0.451 |
| Pneumocystis jiroveci pneumonia | 8 (0.5) | 2 (0.5) | 7 (1.3) | 4 (3.2) | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.Y.; Cha, S.H.; Kim, S.H.; Jeong, K.H.; Chung, K.Y.; Cho, H.R.; Lee, J.; Huh, K.H.; Yang, J.; Kim, M.S.; et al. Risk Due to ABO Incompatibility and Donor-Recipient Weight Mismatch in Living Donor Kidney Transplantation: A National Cohort Study. J. Clin. Med. 2021, 10, 5674. https://doi.org/10.3390/jcm10235674
Lee JY, Cha SH, Kim SH, Jeong KH, Chung KY, Cho HR, Lee J, Huh KH, Yang J, Kim MS, et al. Risk Due to ABO Incompatibility and Donor-Recipient Weight Mismatch in Living Donor Kidney Transplantation: A National Cohort Study. Journal of Clinical Medicine. 2021; 10(23):5674. https://doi.org/10.3390/jcm10235674
Chicago/Turabian StyleLee, Jun Young, Sung Hwan Cha, Sung Hwa Kim, Kyung Hwan Jeong, Ku Yong Chung, Hong Rae Cho, Juhan Lee, Kyu Ha Huh, Jaeseok Yang, Myoung Soo Kim, and et al. 2021. "Risk Due to ABO Incompatibility and Donor-Recipient Weight Mismatch in Living Donor Kidney Transplantation: A National Cohort Study" Journal of Clinical Medicine 10, no. 23: 5674. https://doi.org/10.3390/jcm10235674
APA StyleLee, J. Y., Cha, S. H., Kim, S. H., Jeong, K. H., Chung, K. Y., Cho, H. R., Lee, J., Huh, K. H., Yang, J., Kim, M. S., Kim, D. G., & on behalf of the Korean Organ Transplantation Registry Study Group. (2021). Risk Due to ABO Incompatibility and Donor-Recipient Weight Mismatch in Living Donor Kidney Transplantation: A National Cohort Study. Journal of Clinical Medicine, 10(23), 5674. https://doi.org/10.3390/jcm10235674