
Diagnostic Re-Evaluation and Potential Predictor Factors of Transient and Permanent Congenital Hypothyroidism in Eutopic Thyroid Gland


Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tuli, G.; Munarin, J.; Tessaris, D.; Matarazzo, P.; Einaudi, S.; De Sanctis, L. Incidence of primary congenital hypothyroidism and relationship between diagnostic categories and associated malformations. Endocrine 2021, 71, 122–129. [Google Scholar] [CrossRef]
- van Trotsenburg, P.; Stoupa, A.; Léger, J.; Rohrer, T.; Peters, C.; Fugazzola, L.; Cassio, A.; Heinrichs, C.; Beauloye, V.; Pohlenz, J.; et al. Congenital Hypothyroidism: A 2020–2021 Consensus Guidelines Update—An ENDO-European Reference Network Initiative Endorsed by the European Society for Pediatric Endocrinology and the European Society for Endocrinology. Thyroid 2021, 31, 387–419. [Google Scholar] [CrossRef]
- Nair, P.S.; Sobhakumar, S.; Kailas, L. Diagnostic re-evaluation of children with congenital hypothyroidism. Indian Pediatr. 2010, 47, 757–760. [Google Scholar] [CrossRef] [PubMed]
- Rabbiosi, S.; Vigone, M.C.; Cortinovis, F.; Zamproni, I.; Fugazzola, L.; Persani, L.; Corbetta, C.; Chiumello, G.; Weber, G. Congenital Hypothyroidism With Eutopic Thyroid Gland: Analysis of Clinical and Biochemical Features at Diagnosis and after Re-Evaluation. J. Clin. Endocrinol. Metab. 2013, 98, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.S.; Cho, G.S.; Park, S.H.; Jung, M.H.; Suh, B.K.; Koh, D.G. Earlier re-evaluation may be possible in pediatric patients with eutopic congenital hypothyroidism requiring lower L-thyroxine doses. Ann. Pediatr. Endocrinol. Metab. 2014, 19, 141–145. [Google Scholar] [CrossRef]
- Messina, M.F.; Aversa, T.; Salzano, G.; Zirilli, G.; Sferlazzas, C.; De Luca, F.; Lombardo, F. Early Discrimination between Transient and Permanent Congenital Hypothyroidism in Children with Eutopic Gland. Horm. Res. Paediatr. 2015, 84, 159–164. [Google Scholar] [CrossRef]
- Kara, C.; Günindi, F.; Yılmaz, G.C.; Aydın, M. Transient Congenital Hypothyroidism in Turkey: An Analysis on Frequency and Natural Course. J. Clin. Res. Pediatr. Endocrinol. 2016, 8, 170–179. [Google Scholar] [CrossRef]
- Kang, M.J.; Chung, H.-R.; Oh, Y.-J.; Shim, Y.-S.; Yang, S.; Hwang, I.-T. Three-year follow-up of children with abnormal newborn screening results for congenital hypothyroidism. Pediatr. Neonatol. 2017, 58, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Park, I.S.; Yoon, J.S.; So, C.H.; Lee, H.S.; Hwang, J.S. Predictors of transient congenital hypothyroidism in children with eutopic thyroid gland. Ann. Pediatr. Endocrinol. Metab. 2017, 22, 115–118. [Google Scholar] [CrossRef][Green Version]
- Saba, C.; Guilmin-Crepon, S.; Zénaty, D.; Martinerie, L.; Paulsen, A.; Simon, D.; Storey, C.; Dos Santos, S.; Haignere, J.; Mohamed, D.; et al. Early Determinants of Thyroid Function Outcomes in Children with Congenital Hypothyroidism and a Normally Located Thyroid Gland: A Regional Cohort Study. Thyroid 2018, 28, 959–967. [Google Scholar] [CrossRef]
- Oron, T.; Lazar, L.; Ben-Yishai, S.; Tenenbaum, A.; Yackobovitch-Gavan, M.; Meyerovitch, J.; Phillip, M.; Lebenthal, Y. Permanent vs. Transient Congenital Hypothyroidism: Assessment of Predictive Variables. J. Clin. Endocrinol. Metab. 2018, 103, 4428–4436. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, S.; Hasegawa, Y. Levothyroxine dosages less than 2.4 μg/kg/day at 1 year and 1.3 μg/kg/day at 3 years of age may predict transient congenital hypothyroidism. Clin. Pediatr. Endocrinol. 2019, 28, 127–133. [Google Scholar] [CrossRef]
- Park, E.S.; Yoon, J.Y. Factors associated with permanent hypothyroidism in infants with congenital hypothyroidism. BMC Pediatr. 2019, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Asena, M.; Demiral, M.; Unal, E.; Öcal, M.; Demirbilek, H.; Özbek, M.N. Validity of Six Month L-Thyroxine Dose for Differentiation of Transient or Permanent Congenital Hypothyroidism. J. Clin. Res. Pediatr. Endocrinol. 2020, 12, 275–280. [Google Scholar] [CrossRef]
- Long, W.; Zhou, L.; Wang, Y.; Liu, J.; Wang, H.; Yu, B. Complicated Relationship between Genetic Mutations and Phenotypic Characteristics in Transient and Permanent Congenital Hypothyroidism: Analysis of Pooled Literature Data. Int. J. Endocrinol. 2020, 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-H.; Yang, B.-C.; Li, J.-Y.; Xu, P.; Wang, F. Diagnostic re-evaluation and predictors of congenital hypothyroidism with eutopic thyroid gland in Jiangxi, China. J. Pediatr. Endocrinol. Metab. 2021, 34, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Nagasaki, K.; Sato, H.; Sasaki, S.; Nyuzuki, H.; Shibata, N.; Sawano, K.; Hiroshima, S.; Asami, T. Re-Evaluation of the Prevalence of Permanent Congenital Hypothyroidism in Niigata, Japan: A Retrospective Study. Int. J. Neonatal Screen. 2021, 7, 27. [Google Scholar] [CrossRef]
- Abbasi, F.; Janani, L.; Talebi, M.; Azizi, H.; Hagiri, L.; Rimaz, S. Risk factors for transient and permanent congenital hypothyroidism: A population-based case-control study. Thyroid Res. 2021, 14, 1–7. [Google Scholar] [CrossRef]
- Matejek, N.; Tittel, S.R.; Haberland, H.; Rohrer, T.; Busemann, E.-M.; Jorch, N.; Schwab, K.-O.; Wölfle, J.; Holl, R.W.; Bettendorf, M. Predictors of transient congenital primary hypothyroidism: Data from the German registry for congenital hypothyroidism (AQUAPE “HypoDok”). Eur. J. Nucl. Med. Mol. Imaging 2021, 180, 2401–2408. [Google Scholar] [CrossRef] [PubMed]
- Mehran, L.; Azizi, F.; Mousapour, P.; Cheraghi, L.; Yarahmadi, S.; Amirshekari, G.; Khalili, D. Development of a risk prediction model for early discrimination between permanent and transient congenital hypothyroidism. Endocrine 2021, 73, 1–10. [Google Scholar] [CrossRef]
- Yamamura, H.; Kokumai, T.; Furuya, A.; Suzuki, S.; Tanahashi, Y.; Azuma, H. Increase in doses of levothyroxine at the age of 3 years and above is useful for distinguishing transient and permanent congenital hypothyroidism. Clin. Pediatr. Endocrinol. 2020, 29, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Kemper, A.R.; Grosse, S.D.; Baker, M.; Pollock, A.J.; Hinton, C.F.; Shapira, S.K. Treatment Discontinuation within 3 Years of Levothyroxine Initiation among Children Diagnosed with Congenital Hypothyroidism. J. Pediatr. 2020, 223, 136–140. [Google Scholar] [CrossRef]
- Itonaga, T.; Higuchi, S.; Shimura, K.; Nagasaki, K.; Satoh, M.; Takubo, N.; Takahashi, I.; Sawada, H.; Hasegawa, Y. Levothyroxine Dosage as Predictor of Permanent and Transient Congenital Hypothyroidism: A Multicenter Retrospective Study in Japan. Horm. Res. Paediatr. 2019, 92, 45–51. [Google Scholar] [CrossRef]
- Korzeniewski, S.J.; Grigorescu, V.; Kleyn, M.; Young, W.I.; Birbeck, G.; Todem, D.; Romero, R.; Paneth, N. Transient Hypothyroidism at 3-Year Follow-Up among Cases of Congenital Hypothyroidism Detected by Newborn Screening. J. Pediatr. 2013, 162, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Hashemipour, M.; Hovsepian, S.; Kelishadi, R.; Iranpour, R.; Hadian, R.; Haghighi, S.; Gharapetian, A.; Talaei, M.; Amini, M. Permanent and transient congenital hypothyroidism in Isfahan–Iran. J. Med. Screen. 2009, 16, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Unüvar, T.; Demir, K.; Abacı, A.; Ataş, A.; Büyükgebiz, A.; Böber, E. Monitoring and prognostic evaluation of patients with congenital hypothyroidism treated in a pediatric endocrinology unit. Turk. J. Pediatr. 2013, 55, 384–390. [Google Scholar] [PubMed]
- Unüvar, T.; Demir, K.; Abacı, A.; Büyükgebiz, A.; Böber, E. The Role of Initial Clinical and Laboratory Findings in Infants With Hyperthyrotropinemia to Predict Transient or Permanent Hypothyroidism. J. Clin. Res. Pediatr. Endocrinol. 2013, 5, 170–173. [Google Scholar] [CrossRef]
- Aguiar, L.; Garb, J.; Reiter, E.; Visintainer, P.; Singh, R.; Allen, H.; Tonyushkina, K. Can One Predict Resolution of Neonatal Hyperthyrotropinemia? J. Pediatr. 2016, 174, 71–77.e1. [Google Scholar] [CrossRef]
- Razavi, Z.; Mohammadi, L. Permanent and Transient Congenital Hypothyroidism in Hamadan West Province of Iran. Int. J. Endocrinol. Metab. 2016, 14. [Google Scholar] [CrossRef]
- Fu, C.; Luo, S.; Li, Y.; Li, Q.; Hu, X.; Li, M.; Zhang, Y.; Su, J.; Hu, X.; Chen, Y.; et al. The incidence of congenital hypothyroidism (CH) in Guangxi, China and the predictors of permanent and transient CH. Endocr. Connect. 2017, 6, 926–934. [Google Scholar] [CrossRef][Green Version]
- Habib, A.; Shojazadeh, A.; Molayemat, M.; Habib, A.; Jeddi, M.; Arabsolghar, R.; Nahas, M.; Rahimi, N.; Ardekani, F.M. Prevalence and predictive factors of transient and permanent congenital hypothyroidism in Fars province, Iran. BMC Pediatr. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zdraveska, N.; Zdravkovska, M.; Anastasovska, V.; Sukarova-Angelovska, E.; Kocova, M. Diagnostic re-evaluation of congenital hypothyroidism in Macedonia: Predictors for transient or permanent hypothyroidism. Endocr. Connect. 2018, 7, 278–285. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Permanent CH (PCH) 29 Subjects = 52.7% | Transient CH (TCH) 26 Subjects = 47.3% | p | ||
|---|---|---|---|---|
| Gender | Male | 22 | 12 | 0.02 |
| Female | 7 | 14 | ||
| Gestational Age | At term | 21 | 17 | 0.6 |
| Preterm | 8 | 9 | ||
| Delivery | Vaginal | 15 | 11 | 0.5 |
| Caesarean section | 14 | 15 | ||
| Family history for thyroid disease | 7 | 10 | 0.3 | |
| Neonatal Weight (g) | 2285 ± 156.7 | 2602 ± 129.3 | 0.1 | |
| Neonatal Length (cm) | 47.7 ± 0.76 | 46.3 ± 1.05 | 0.3 | |
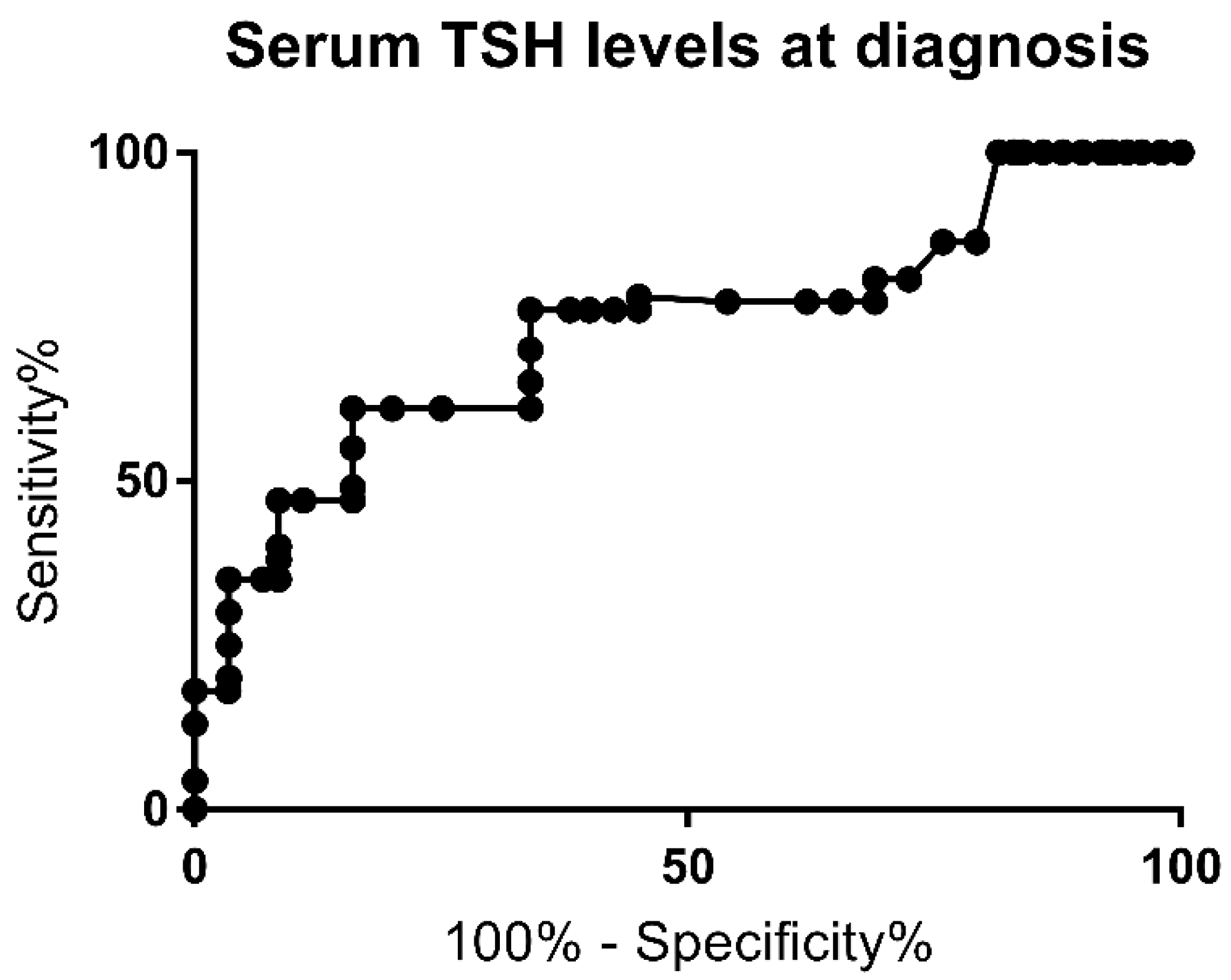
| Blood TSH mcUI/mL | 197.3 ± 44.5 | 55.01 ± 7.33 | 0.009 | |
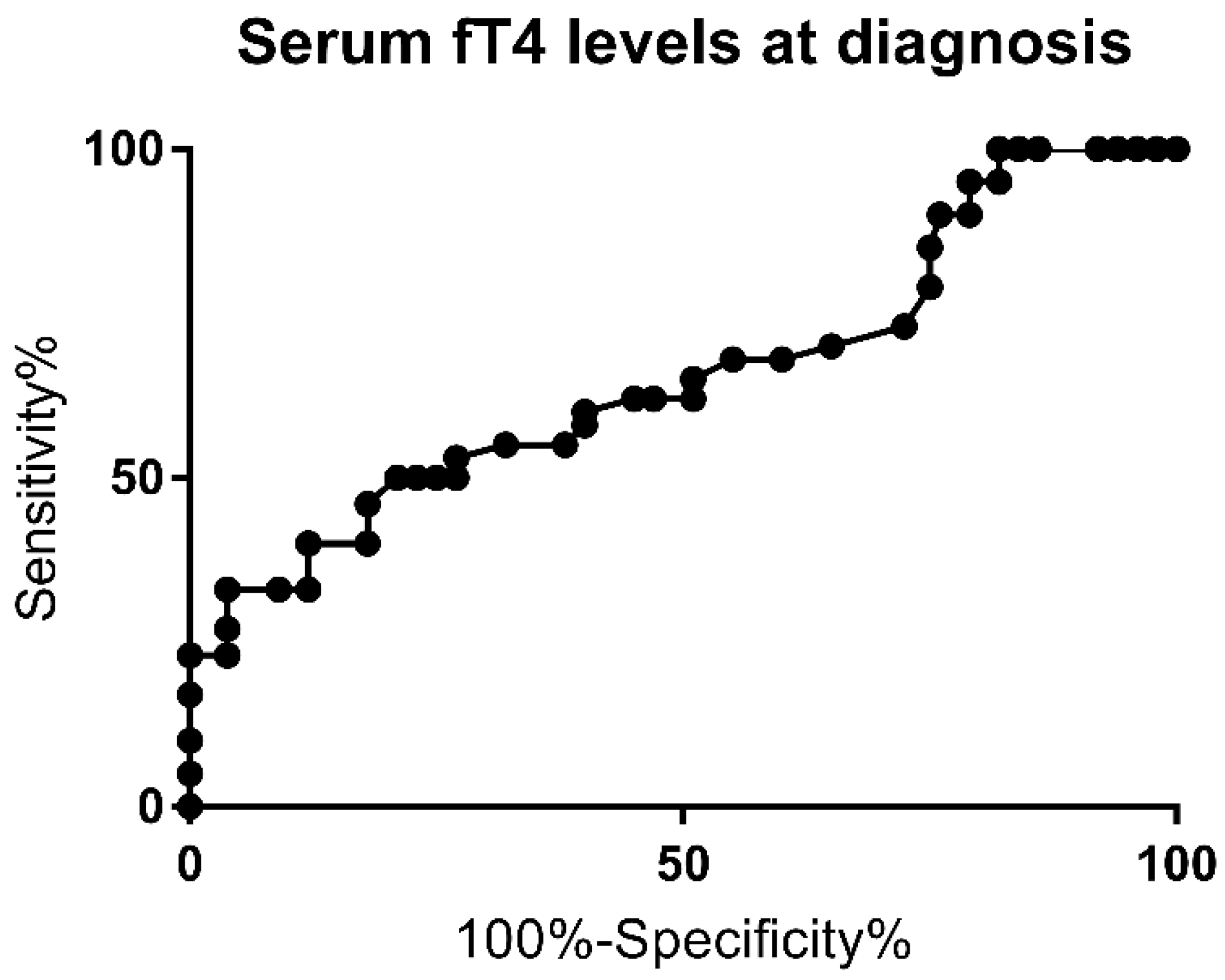
| FT4 pg/mL | 6.92 ± 0.72 | 9.29 ± 1.98 | 0.03 | |
| FT3 pg/mL | 3.75 ± 0.25 | 4.19 ± 0.48 | 0.3 | |
| Levothyroxine initial dose | 8.37 ± 0.43 | 9.13 ± 0.44 | 0.23 | |
| Levothyroxine requirement in the 1st year | 5.12 ± 0.36 | 5.61 ± 0.55 | 0.46 | |
| Levothyroxine requirement in the 2nd year | 2.77 ± 0.19 | 2.74 ± 0.2 | 0.9 | |
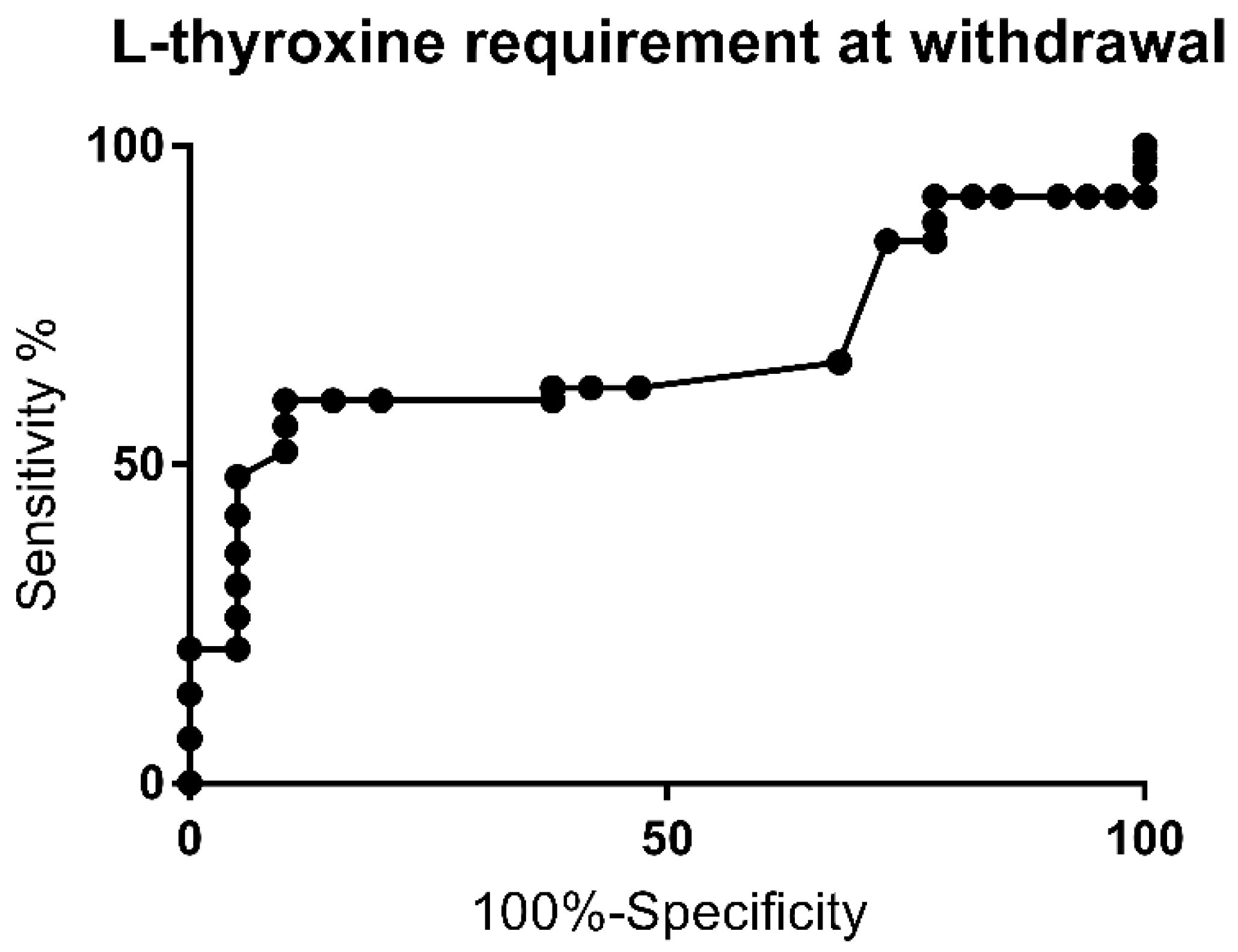
| Levothyroxine requirement at withdrawal | 2.69 ± 0.14 | 2.14 ± 0.19 | 0.02 | |
| TSH mcUI/mL prior to withdrawal | 2.81 ± 0.74 | 1.98 ± 0.27 | 0.2 | |
| FT4 pg/mL prior to withdrawal | 14.53 ± 0.56 | 14.45 ± 0.44 | 0.9 | |
| TSH mcUI/mL after withdrawal | 23.37 ± 13.6 | 4.1 ± 0.31 | 0.007 | |
| FT4 pg/mL after withdrawal | 9.54 ± 1.22 | 13.13 ± 0.33 | 0.004 | |
| Malformations | 15 | 5 | 0.01 | |
| Study | Year | No. of Subjects with Eutopic Thyroid | TCH Rate | Main Findings |
|---|---|---|---|---|
| Nair et al. [3] | 2010 | 23 | 80% | Significant higher TSH in PCH subjects |
| Rabbiosi et al. [4] | 2013 | 84 | 67% | Same clinical outcome in patients with screening TSH values < 20 and >20 mcUI/mL. M/F ratio: 0.88 for TCH vs. 1.23 for PCH (not significant). Malformations rate 12.5% for TCH vs. 13.7% for PCH. |
| Cho et al. [5] | 2014 | 56 | 45% | TSH at diagnosis and levothyroxine requirement found to be predictive. M/F ratio: 0.92 for TCH vs. 0.93 for PCH. |
| Messina et al. [6] | 2015 | 64 | 72% | TSH at diagnosis and levothyroxine requirement found to be predictive. |
| Kara et al. [7] | 2016 | 86 | 73% | Levothyroxine requirement found to be predictive. M/F ratio: 1.7 for TCH vs. 0.7 for PCH. |
| Kang et al. [8] | 2017 | 20 | 50% | TSH at diagnosis and levothyroxine requirement found to be predictive. M/F ratio: 1.3 for TCH vs. 0.6 for PCH. |
| Park et al. [9] | 2017 | 100 | 65% | TSH at diagnosis and levothyroxine requirement. M/F ratio: 1.2 for TCH vs. 1.1 for PCH found to be predictive. |
| Saba et al. [10] | 2018 | 92 | 54% | Levothyroxine requirement found to be predictive. M/F ratio: 1.1 for TCH vs. 1.05 for PCH. |
| Oron et al. [11] | 2018 | 84 | 20% | Levothyroxine requirement found to be predictive. M/F ratio: 1.43 for TCH vs. 0.86 for PCH. |
| Higuchi et al. [12] | 2019 | 30 | 50% | Levothyroxine requirement found to be predictive. M/F ratio: 0.9 for TCH vs. 1.4 for PCH (not significant). |
| Park et al. [13] | 2019 | 80 | 89% | Levothyroxine requirement found to be predictive. M/F ratio: 0.97 for TCH vs. 0.55 for PCH. Malformations rate not reported. |
| Asena et al. [14] | 2020 | 186 | 29% | Levothyroxine requirement found to be predictive. |
| Long et al. [15] | 2020 | 190 | 45% | Mutations related to thyroid dysgenesis are more likely to have PCH. M/F ratio: 1.09 for TCH vs. 1.1 for PCH. (not significant). |
| Chen et al. [16] | 2021 | 508 | 66% | Levothyroxine requirement and familial history of CH found to be predictive. M/F ratio: 1.22 for TCH vs. 1.58 for PCH (not significant). |
| Current study | 2021 | 55 | 47% | M/F ratio: 0.86 for TCH vs. 3.1 for PCH. TSH above 60 mcUI/mL and fT4 inferior to 7.2 pg/mL at diagnosis and levothyroxine requirement above 2.25 mcg/kg/day found to be predictive of PCH. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuli, G.; Munarin, J.; De Sanctis, L. Diagnostic Re-Evaluation and Potential Predictor Factors of Transient and Permanent Congenital Hypothyroidism in Eutopic Thyroid Gland. J. Clin. Med. 2021, 10, 5583. https://doi.org/10.3390/jcm10235583
Tuli G, Munarin J, De Sanctis L. Diagnostic Re-Evaluation and Potential Predictor Factors of Transient and Permanent Congenital Hypothyroidism in Eutopic Thyroid Gland. Journal of Clinical Medicine. 2021; 10(23):5583. https://doi.org/10.3390/jcm10235583
Chicago/Turabian StyleTuli, Gerdi, Jessica Munarin, and Luisa De Sanctis. 2021. "Diagnostic Re-Evaluation and Potential Predictor Factors of Transient and Permanent Congenital Hypothyroidism in Eutopic Thyroid Gland" Journal of Clinical Medicine 10, no. 23: 5583. https://doi.org/10.3390/jcm10235583
APA StyleTuli, G., Munarin, J., & De Sanctis, L. (2021). Diagnostic Re-Evaluation and Potential Predictor Factors of Transient and Permanent Congenital Hypothyroidism in Eutopic Thyroid Gland. Journal of Clinical Medicine, 10(23), 5583. https://doi.org/10.3390/jcm10235583