
Analysis of the Different Lymphatic Drainage Patterns during Sentinel Lymph Node Biopsy for Skin Melanoma

 ,
, 
 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.1.1. Patients Included
2.1.2. Exclusion Criteria
2.2. Outcome
2.3. Interventions
2.4. Satisical Analysis
3. Results
- sex: 77.28% male (111) and 32.72% female (54);
- median age and standard deviation: 62 ± 15.15
- The Breslow depth was reported in 157 cases (95.15%), the higher number of patients had a stage II of Breslow (48.4%) and a stage III (27.4%) (Table 1).
- The T classification of melanoma, based on the thickness of the primary tumor and presence or absence of ulceration, is reported in 156 patients (94.23%), the higher number of patients have a stage T1b (32.7%) and T2a (29.5%) (Table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Depth | Number of Patients (%) |
|---|---|---|
| Stage I | 0.75 mm or less | 18 (11.4%) |
| Stage II | 0.76 mm–1.50 mm | 76 (48.4%) |
| Stage III | 1.51 mm–4.00 mm | 43 (27.4%) |
| Stage IV | >4 mm | 20 (12.8%) |
| Stage | Depth of Melanoma | Number of Patients (%) |
|---|---|---|
| T1b | ≤1.0 mm in thickness with ulceration or mitoses ≥1/mm2 | 51 (32.7%) |
| T2a | 1.01–2.0 mm in thickness without ulceration | 46 (29.5%) |
| T2b | 1.01–2.0 mm in thickness with ulceration | 11 (7.0%) |
| T3a | 2.01–4.0 mm in thickness with ulceration | 14 (9.0%) |
| T3b | 2.01–4.0 mm in thickness without ulceration | 18 (11.5%) |
| T4a | >4.0 mm in thickness without ulceration | 5 (3.2%) |
| T4b | >4.0 mm in thickness with ulceration | 11 (7.0%) |
3.1. Data and Analysis
- regions draining at least 90% of the time into the same group of lymph nodes were considered homogeneous;
- regions of the lateral wall of the abdomen and gluteus, considering the low number of cases, and not presenting a significantly heterogeneous pattern were classified as homogeneous;
- regions that were shown to have multiple and/or bilateral drainage in significant numbers were identified as heterogeneous.
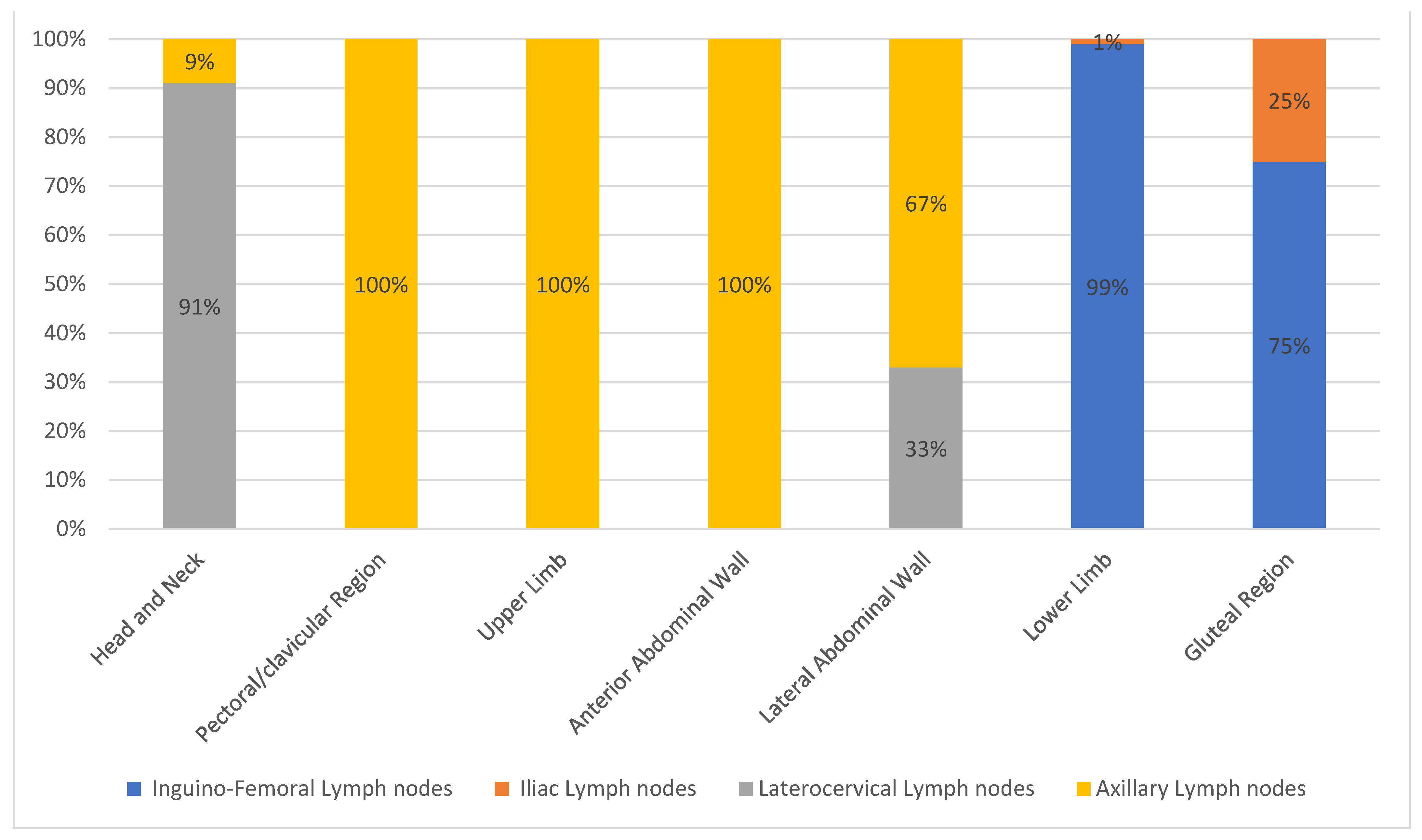
3.1.1. Homogeneous Drainage Group
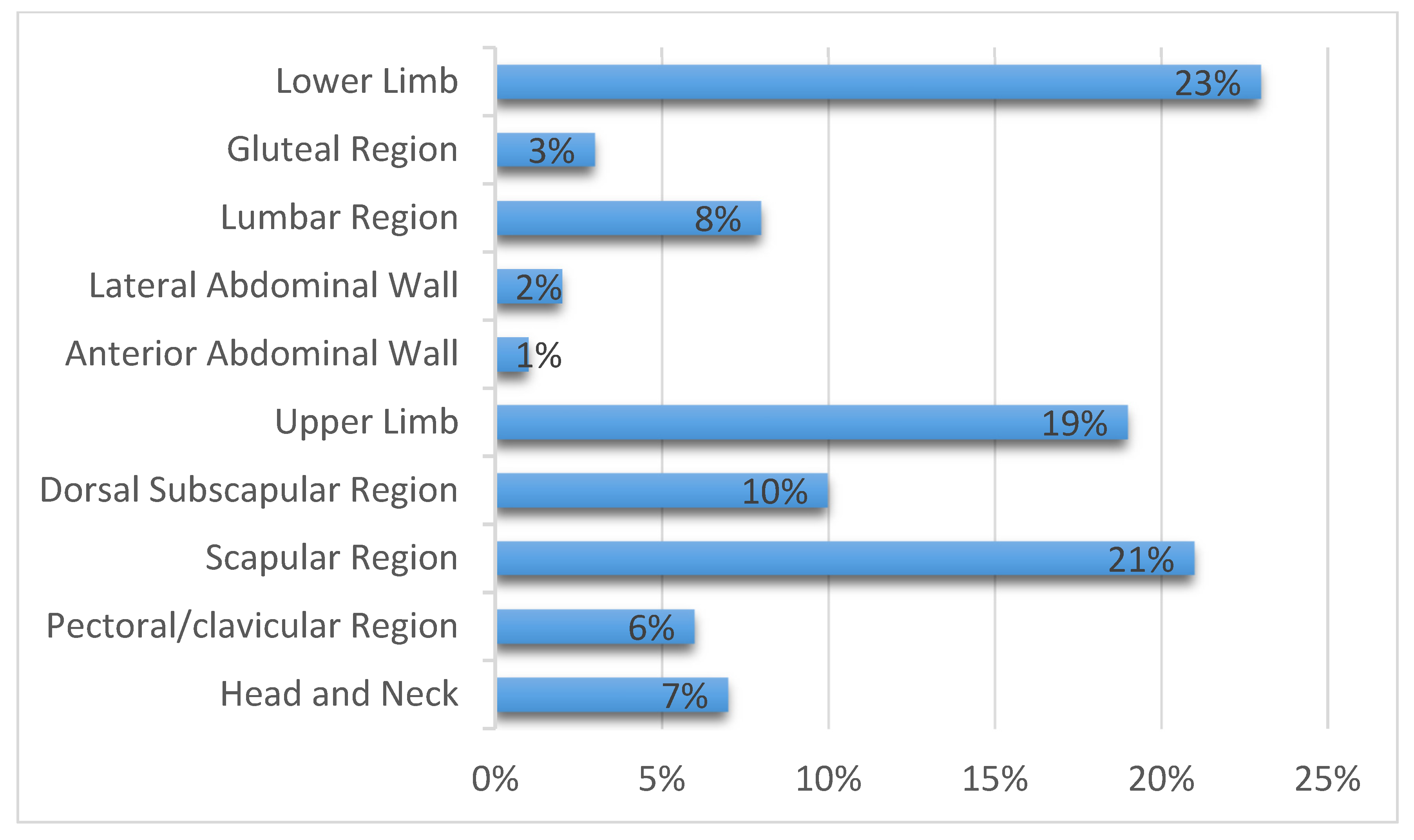
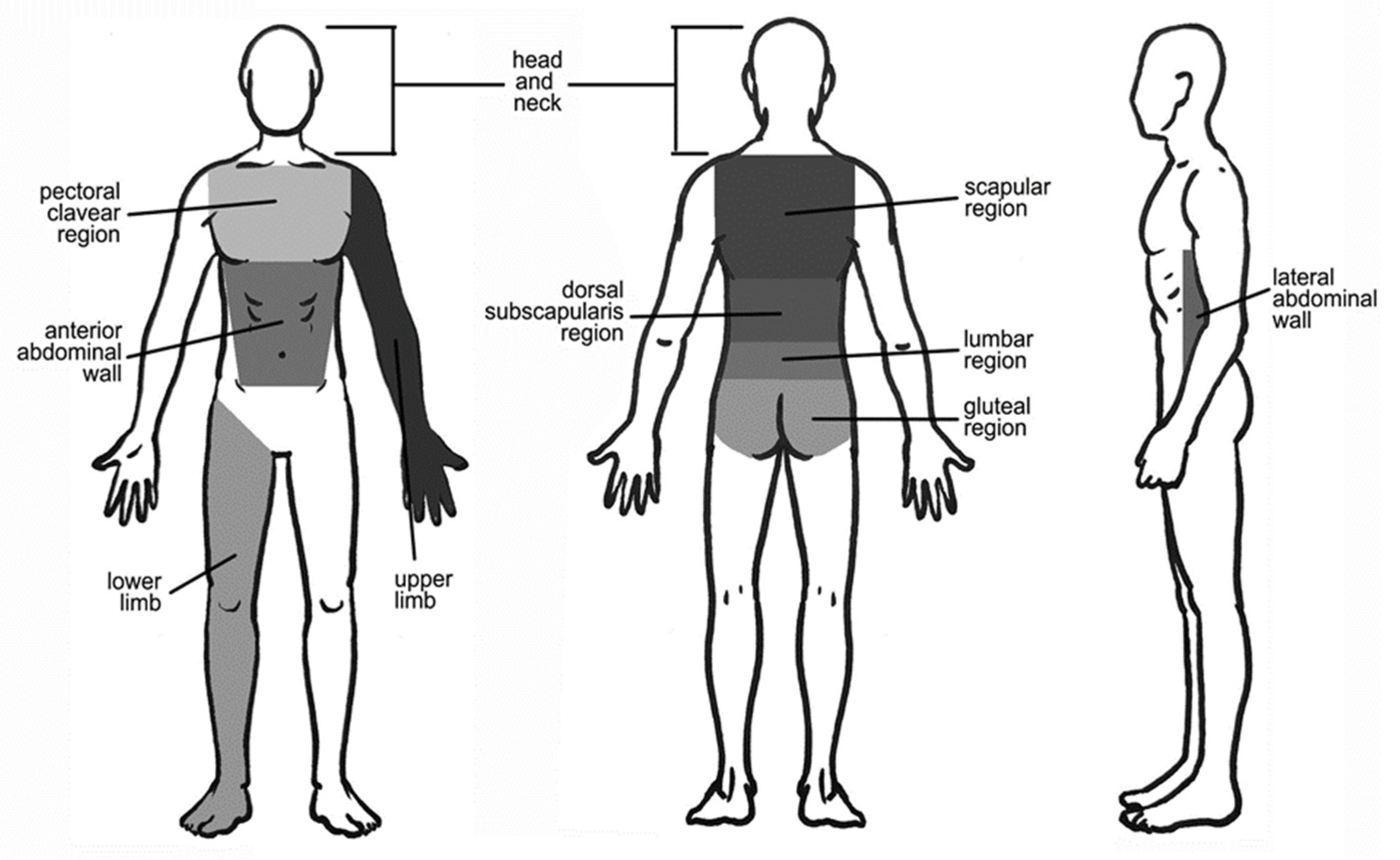
- Head and neck. Twelve cutaneous melanomas were located in this region (7.27% of all included patients) (Figure 1). The greatest number of cutaneous melanomas drained into the laterocervical lymph nodes (91.17%) and only one patient drained into the axilla (8.3%) (Figure 3). The pT evaluation reported two pT1b, three pT2a, three pT3b, one pT4a, and one pT4b case(s); in two cases the pT evaluation was not reported (Table 3).
- Pectoral/clavicular region. In this area, 11 cutaneous melanomas were located (6.66% of all included patients) (Figure 1) and, in all cases, the lymphatic drainage was at the level of the homolateral axillary lymph nodes (100%) (Figure 3). In this group, two pT1b, three pT2a, one pT2b, one pT3a, one pT3b, and two pT4b cases were reported; in one case pT evaluation was not reported (Table 3).
- Upper limb. In this region, 32 cutaneous melanomas were localized (19.39% of all included patients) (Figure 1) and in all cases the lymphatic drainage was at the level of the homolateral axillary lymph nodes (100%) (Figure 3). At this level, the location was as reported in Table 3.
- Arm. In twenty-seven patients, the cases were five pT1b, eight pT2a, seven pT2b, two pT3a, two pT3b, and two pT4b. In one case, pT evaluation was not reported.
- Forearm. Five patients were reported in this group: one case of pT1b, pT2b, pT3a, and pT3b, respectively. In one case, pT assessment was not reported.
- Lower limb. Here, 38 cutaneous melanomas were localized (23.03% of all included patients) (Figure 1) and in all cases the lymphatic drainage was at the level of the homolateral iliac–femoral lymph nodes (100%) (Figure 3). By means of a functional, not simply anatomical, assessment, it is possible to consider these two lymph node stations, iliac and femoral, as a single drainage group: the iliac–femoral lymph nodes.At this level, the location was as seen in Table 3.
- Thigh. In this region there were 16 patients with SLNB at the homolateral inguinal–femoral lymph node. The pT assessment was pT1b in six cases and pT2a in five cases, with one case of pT3a, two cases of pT3b and two cases of pT4b.
- Knee. One patient with SLNB at the homolateral inguinal–femoral lymph node. This patient had a pT1b stage.
- Calf. Sixteen patients with SLNB to the homolateral inguinal–femoral lymph node and also at the iliac lymph node in three cases (18.75%). In these patients with SBLN at the iliac lymph node the pT evaluation was pT1b in two cases and pT3a in one case; in patients with only SBLN at the homolateral inguinal–femoral lymph node, there were two cases of pT1b, seven cases of pT2a, and two cases of pT3a and pT4b.
- Foot. Five patients with SLNB at the homolateral inguinal–femoral lymph node. In these patients, the pT assessment was a pT1b in three cases and a pT3a in one case; in one case no pT assessment was reported.
- Gluteal region. In this area, four cutaneous melanomas were located (2.42% of all included patients) (Figure 1) and in three cases the lymphatic drainage was to the homolateral inguinal–femoral lymph nodes (75%); only in one patient was drainage to the iliac lymph node reported (25%) (Figure 2). In this group, three pT1b were reported, and in one case pT evaluation was not reported (Table 3). According to the above functional evaluation, it can be stated that the drainage of cutaneous melanomas of the gluteal region was in 100% of the cases at the iliac–femoral lymph nodes.
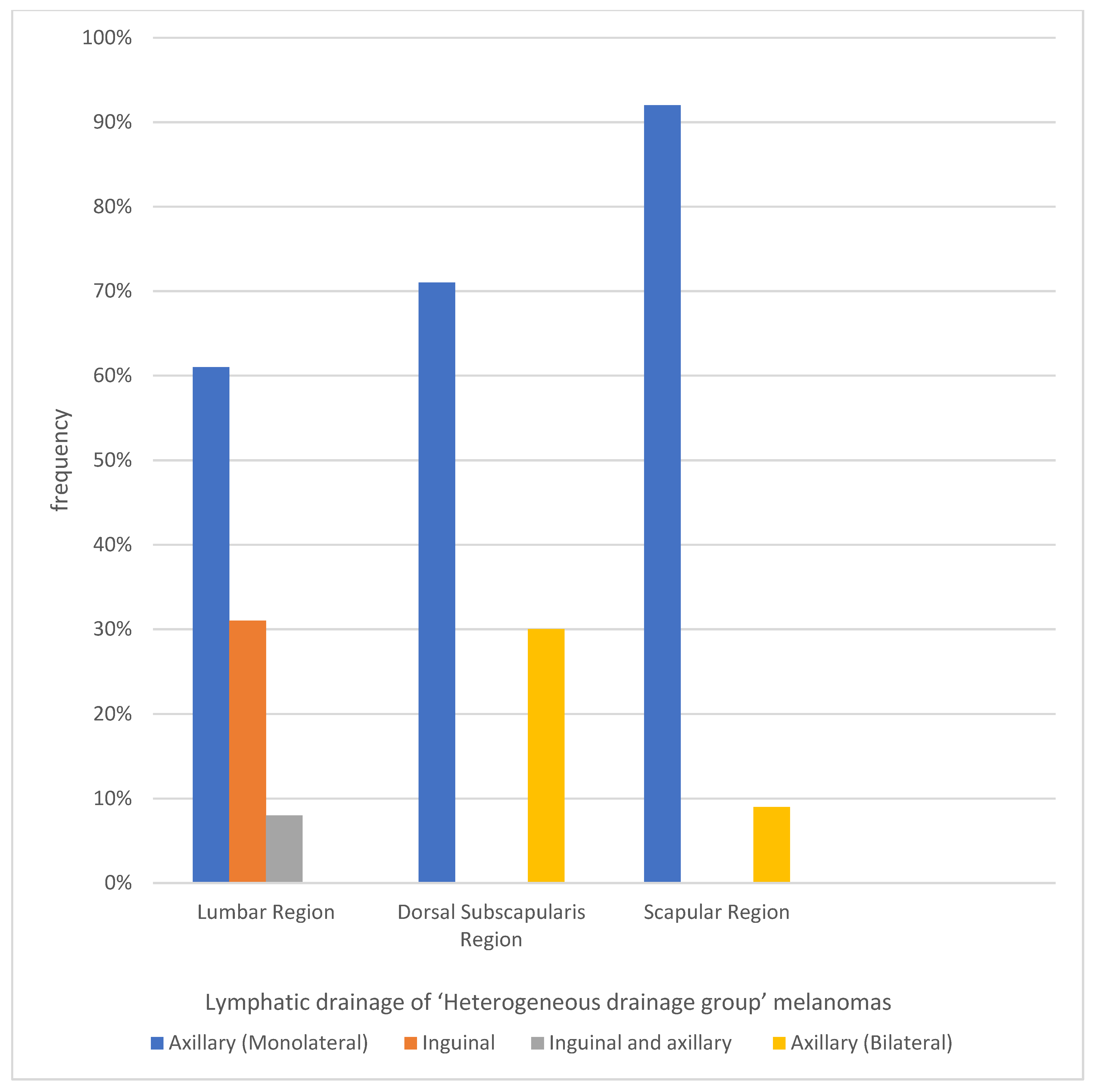
3.1.2. Heterogeneous Drainage Group
- Lumbar region. In this area, 13 cutaneous melanomas were located (7.88% of all included patients) (Figure 1). Lymphatic drainage was very heterogeneous: eight patients to axillary lymph nodes only (61.53%), one patient to axillary and inguinal lymph nodes (7.69%), and four patients to inguinal level only (30.77%) (Figure 4). In this group, five pT1b, two pT2a, two pT3a, and two pT4a cases were reported; pT evaluation was not reported in two cases (Table 3).
- Dorsal subscapularis region. Seventeen cutaneous melanomas were localized to this region (10.3% of all included patients) (Figure 1). The skin melanoma drained into the homolateral (70.59%) or bilateral (29.41%) axillary lymph nodes (Figure 4). The pT evaluation reported three pT1b, four pT2a, two pT2b, two pT3a, three pT3b, and two pT4a cases; in one case the pT evaluation was not reported (Table 3).
- Scapular region. Thirty-five cutaneous melanomas were located in this region (21.21% of all included patients) (Figure 1). Drainage of the skin melanoma was to the homolateral axillary region in 91.43% of the cases; bilateral drainage was reported in only three cases (8.57%) (Figure 4). The pT evaluation reported eight pT1b, nine pT2a, one pT2b, three pT3a, four pT3b, two pT4a, and six pT4b cases. In one case the pT evaluation was not reported (Table 3).
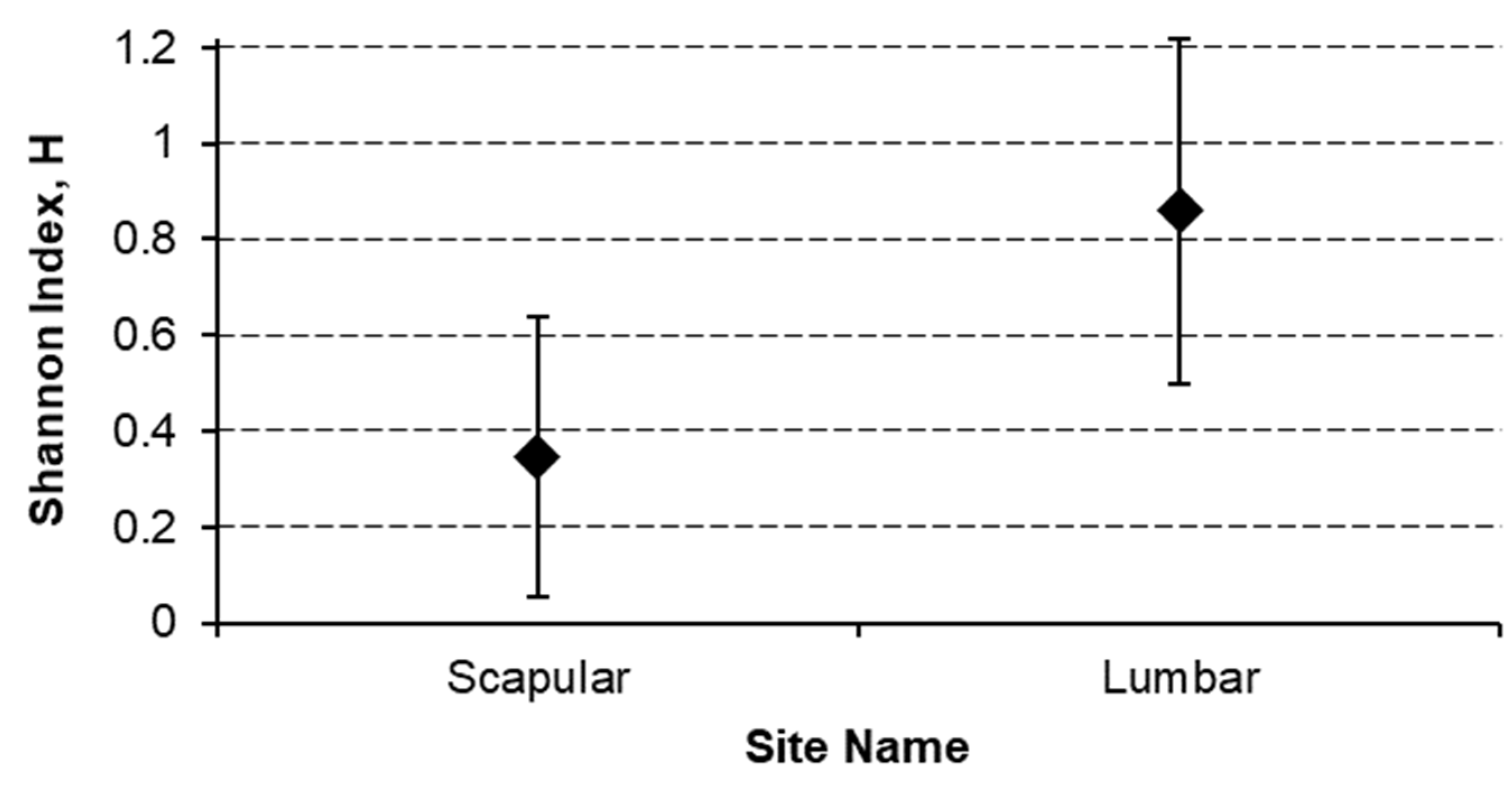
- Lumbar region has a most significant (p < 0.01) heterogeneous site of lymph node region drainage with a Shannon index of 0.876 (CI 0.500–1.217) with respect to the 0.347 (CI 0.055–0.639) of the Scapular region (Figure 5).
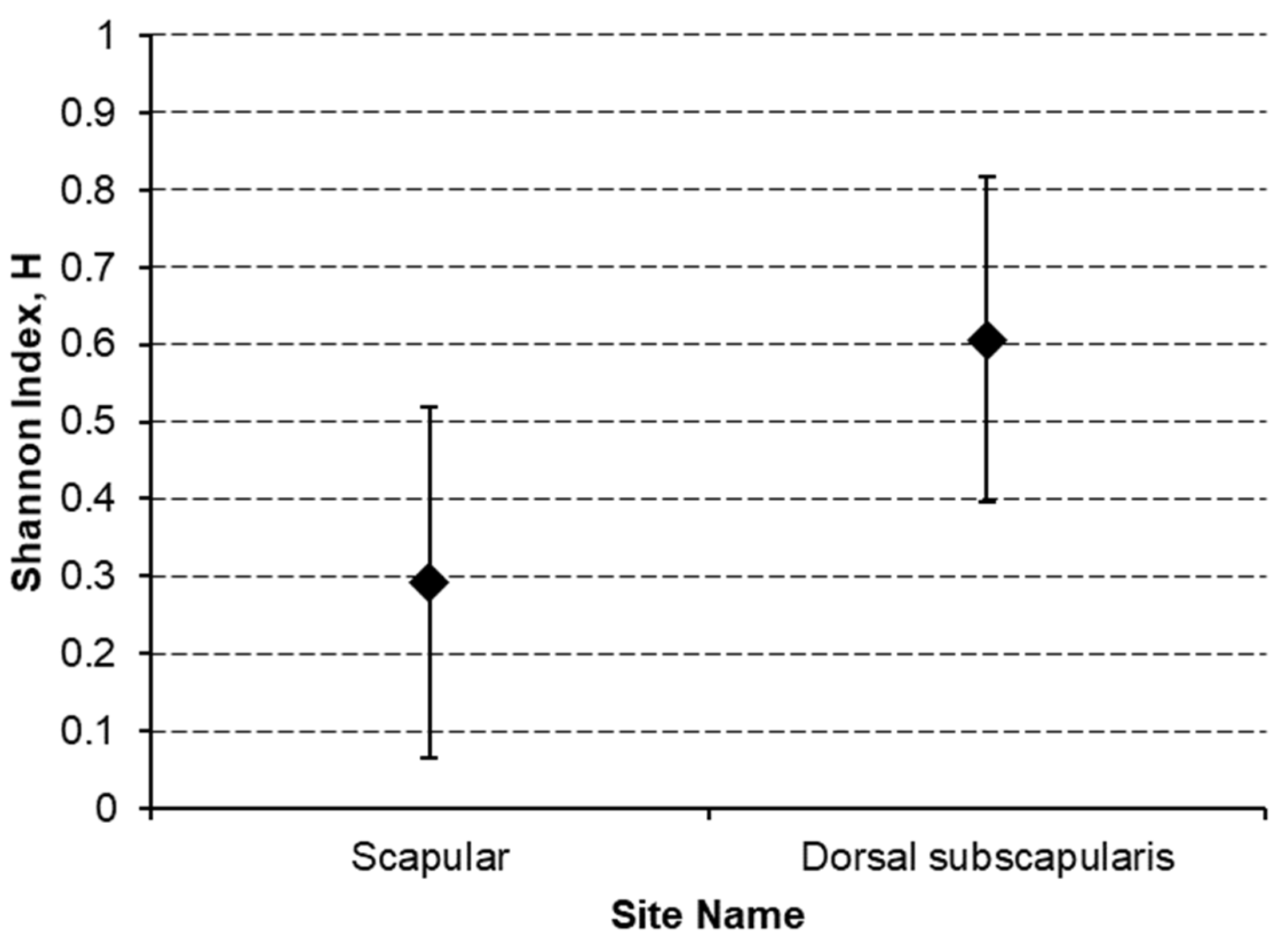
- Dorsal subscapularis region presented the most significantly (p < 0.05) heterogeneous lymphatic laterality drainage (homolateral vs. bilateral) with a Shannon index of 0.606 (CI 0.395–0.816) against the 0.293 (CI 0.065–0.520) of the Scapular region (Figure 6).
4. Discussion
- Pattern 1: it separates lymphatic channels draining to the axilla directly, bypassing the TIS node.
- Pattern 2: lymphatic channels draining first to the TIS node, then to a homolateral axillary node.
- Pattern 3: lymphatic channels draining to the TIS and the axilla, as well as separate channels that drain to the axillary nodes and bypassed the TIS nodes.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sappey, M.P.C. Anatomie, Physiologie, Pathologie des Vaisseaux Lymphatiques Consideres chez L’homme at les Vertebres, A; Delahaye et E. Lacrosnier: Paris, France, 1874. [Google Scholar]
- Tanis, P.J.; Nieweg, O.E.; Valdès Olmos, R.A.; Rutgers, E.J.T.; Kroon, B.B.R. History of sentinel node and validation of the technique. Breast Cancer Res. 2001, 3, 109–112. [Google Scholar] [CrossRef]
- Reynolds, H.M.; Walker, C.G.; Dunbar, P.R.; O’Sullivan, M.J.; Uren, R.F.; Thompson, J.F.; Smith, N.P. Functional anatomy of the lymphatics draining the skin: A detailed statistical analysis. J. Anat. 2010, 216, 344–355. [Google Scholar] [CrossRef]
- Uren, R.F.; Howman-Giles, R.; Thompson, J.F.; McCarthy, W.H.; Quinn, M.J.; Roberts, J.M.; Shaw, H.M. Interval nodes: The forgotten sentinel nodes in patients with melanoma. Arch Surg. 2000, 135, 1168–1172. [Google Scholar] [CrossRef]
- Sugarbaker, E.V.; McBride, C.M. Melanoma of the trunk: The results of surgical excision and anatomic guidelines for predicting nodal metastasis. Surgery 1976, 80, 22–30. [Google Scholar]
- Uren, R.F.; Hoefnagal, C.A. Lymphoscintigraphy. In Textbook of Melanoma; Thompson, J.F., Morton, D.L., Kroon, B.B.R., Eds.; Taylor & Francis: London, UK; New York, NY, USA, 2004. [Google Scholar]
- Manca, G.; Romanini, A.; Rubello, D.; Mazzarri, S.; Boni, G.; Chiacchio, S.; Tredici, M.; Duce, V.; Tardelli, E.; Volterrani, D.; et al. A critical reappraisal of false negative sentinel lymph node biopsy in melanoma. Q. J. Nucl. Med. Mol. Imaging 2014, 58, 105–113. [Google Scholar] [PubMed]
- Suami, H.; Scaglioni, M.F. Anatomy of the Lymphatic System and the Lymphosome Concept with Reference to Lymphedema. Semin. Plast. Surg. 2018, 32, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Leong, S.P.; Achtem, T.A.; Habib, F.A.; Steinmetz, I.; Morita, E.; Allen, R.E.; Kashani-Sabet, M.; Sagebiel, R. Discordancy between clinical predictions vs lymphoscintigraphic and intraoperative mapping of sentinel lymph node drainage of primary melanoma. Arch. Dermatol. 1999, 135, 1472–1476. [Google Scholar] [CrossRef]
- Marone, U.; Aloj, L.; Di Monta, G.; Caracò, C. Lymphoscintigraphy defines new lymphatic pathways from cutaneous melanoma site: Clinical implications and surgical management. Radiol. Res. Pract. 2011, 2011, 817043. [Google Scholar] [CrossRef]
- Lo, M.C.I.; White, S.H.; Nunney, I.; Skrypniuk, J.; Heaton, M.J.; Moncrieff, M.D.S. A feasibility study of indocyanine green fluorescence mapping for sentinel lymph node detection in cutaneous melanoma. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 137–171. [Google Scholar] [CrossRef] [PubMed]
- Nieweg, O.E.; Tanis, P.J.; Leong, S.P.L. Anatomy and Physiology of Lymphatic Circulation: Application to Lymphatic Mapping. In Atlas of Lymphoscintigraphy and Sentinel Node Mapping; Mariani, G., Vidal-Sicart, S., Valdés Olmos, R., Eds.; Springer: Cham, Switzerland, 2020; pp. 1–6. ISBN 978-3-030-45296-4. [Google Scholar]
- Reynolds, H.M.; Dunbar, P.R.; Uren, R.F.; Blackett, S.A.; Thompson, J.F.; Smith, N.P. Three-dimensional visualisation of lymphatic drainage patterns in patients with cutaneous melanoma. Lancet Oncol. 2007, 8, 806–812. [Google Scholar] [CrossRef]
- Wagner, J.D.; Park, H.M.; Coleman, J.J., III; Love, C.; Hayes, J.T. Cervical sentinel lymph node biopsy for melanomas of the head and neck and upper thorax. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 313–321. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Veenstra, H.J.; Klop, W.M.C.; Speijers, M.J.; Lohuis, P.J.; Nieweg, O.E.; Hoekstra, H.J.; Balm, A.J. Lymphatic Drainage Patterns from Melanomas on the Shoulder or Upper Trunk to Cervical Lymph Nodes and Implications for the Extent of Neck Dissection. Ann. Surg. Oncol. 2012, 19, 3906–3912. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, S.A.; Dengel, L.T.; Hranjec, T.; Slingluff, C.L., Jr. A triangular intermuscular space sentinel node in melanoma: Association with axillary lymphatic drainage. Ann. Surg. Oncol. 2010, 17, 2465–2470. [Google Scholar] [CrossRef]
- Uren, R.F.; Howman-Giles, R.; Thompson, J.F.; Quinn, M.J.; O’Brien, C.; Shaw, H.M.; Bosch, C.M.; McCarthy, W.H. Lymphatic drainage to triangular intermuscular space lymph nodes in melanoma on the back. J. Nucl. Med. 1996, 37, 964–966. [Google Scholar]
- Herbert, G.S.; Beshlian, K.M. The triangular intermuscular space as a site of lymph node metastasis in melanoma of the back. Ann. Plast. Surg. 2010, 64, 52–54. [Google Scholar] [CrossRef]
- Saralaya, V.; Joy, T.; Madhyastha, S.; Vadgaonkar, R.; Saralaya, S. Abnormal branching of the axillary artery: Subscapular common trunk: A case report. Int. J. Morphol. 2008, 26, 963–966. [Google Scholar] [CrossRef]
- Tverskoi, A.V.; Morozov, V.N.; Petrichko, S.A.; Pushkarskiy, V.V.; Parichuk, A.S. Rare Branching Pattern of the Subscapular Artery. J. Morphol. Sci. 2018, 35, 167–169. [Google Scholar] [CrossRef]
- Dimovelis, I.; Michalinos, A.; Spartalis, E.; Athanasiadis, G.; Skandalakis, P.; Troupis, T. Tetrafurcation of the subscapular artery. Anatomical and clinical implications. Folia Morphol. 2017, 76, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Bonmarchand, A.; Coquerel-Beghin, D.; Duval-Modeste, A.B.; Duparc, F.; Auquit-Auckbur, I. Anatomy of the cutaneous lymphatic system of the trunk: A clinico-anatomical study of 90 cutaneous melanomas. Surg. Radiol. Anat. 2018, 40, 3–13. [Google Scholar] [CrossRef]
- Rickenbacher, J.; Landolt, A.M.; Theiler, K.; Scheier, H.; Siegfried, J. Outline of the Lymphatic System of the Back. In Applied Anatomy of the Back; Springer: Berlin/Heidelberg, Germany, 1985; pp. 113–117. ISBN 978-3-662-05793-3. [Google Scholar]
- Bluemel, C.; Herrmann, K.; Giammarile, F.; Nieweg, O.E.; Dubreuil, J.; Testori, A.; Audisio, R.A.; Zoras, O.; Lassmann, M.; Chakera, A.H.; et al. EANM practice guidelines for lymphoscintigraphy and sentinel lymph node biopsy in melanoma. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1750–1766. [Google Scholar] [CrossRef]
- Suami, H. Lymphosome concept: Anatomical study of the lymphatic system. J. Surg. Oncol. 2017, 115, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Suami, H.; Taylor, G.I.; Pan, W.R. A new radiographic cadaver injection technique for investigating the lymphatic system. Plast. Reconstr. Surg. 2005, 115, 2007–2013. [Google Scholar] [CrossRef] [PubMed]
- Porter, G.A.; Ross, M.I.; Berman, R.S.; Lee, J.E.; Mansfield, P.F.; Gershenwald, J.E. Significance of multiple nodal basin drainage in truncal melanoma patients undergoing sentinel lymph node biopsy. Ann. Surg. Oncol. 2000, 7, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, R.E.; Panageas, K.; Busam, K.J.; Brady, M.S. Prognostic implications of multiple lymphatic basin drainage in patients with truncal melanoma. J. Clin. Oncol. 2005, 23, 518–524. [Google Scholar] [CrossRef]







| pT1b | pT2a | pT2 | pT3a | pT3b | pT4a | pT4b | Not Reported | |
|---|---|---|---|---|---|---|---|---|
| Head and Neck | 2 | 3 | 0 | 0 | 3 | 1 | 1 | 2 |
| Pectoral/clavicular Region | 2 | 3 | 1 | 1 | 1 | 0 | 2 | 1 |
| Upper Limb (Arm/Forearm) | 5/1 | 8/0 | 7/1 | 2/1 | 2/1 | 0/0 | 2/0 | 1/1 |
| Anterior Abdominal Wall | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Lateral Abdominal Wall | 0 | 2 | 0 | 0 | 1 | 0 | 0 | 0 |
| Lower Limb (Thigh/Knee/Calf/Foot) | 6/1/4/3 | 5/0/7/0 | 0/0/0/0 | 1/0/3/1 | 2/0/0/0 | 0/0/0/0 | 2/0/2/0 | 0/0/0/1 |
| Gluteal Region | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Lumbar Region | 5 | 2 | 0 | 2 | 0 | 2 | 0 | 2 |
| Dorsal Subscapularis Region | 3 | 4 | 2 | 2 | 3 | 2 | 0 | 1 |
| Scapular Region | 8 | 9 | 1 | 3 | 4 | 2 | 6 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirocchi, R.; Metaj, G.; Cicoletti, M.; Arcangeli, F.; De Sol, A.; Poli, G.; Bruzzone, P.; Gioia, S.; Anagnostou, C.; Loreti, F.; et al. Analysis of the Different Lymphatic Drainage Patterns during Sentinel Lymph Node Biopsy for Skin Melanoma. J. Clin. Med. 2021, 10, 5544. https://doi.org/10.3390/jcm10235544
Cirocchi R, Metaj G, Cicoletti M, Arcangeli F, De Sol A, Poli G, Bruzzone P, Gioia S, Anagnostou C, Loreti F, et al. Analysis of the Different Lymphatic Drainage Patterns during Sentinel Lymph Node Biopsy for Skin Melanoma. Journal of Clinical Medicine. 2021; 10(23):5544. https://doi.org/10.3390/jcm10235544
Chicago/Turabian StyleCirocchi, Roberto, Giulio Metaj, Michela Cicoletti, Fabrizio Arcangeli, Angelo De Sol, Giulia Poli, Paolo Bruzzone, Sara Gioia, Christos Anagnostou, Fabio Loreti, and et al. 2021. "Analysis of the Different Lymphatic Drainage Patterns during Sentinel Lymph Node Biopsy for Skin Melanoma" Journal of Clinical Medicine 10, no. 23: 5544. https://doi.org/10.3390/jcm10235544
APA StyleCirocchi, R., Metaj, G., Cicoletti, M., Arcangeli, F., De Sol, A., Poli, G., Bruzzone, P., Gioia, S., Anagnostou, C., Loreti, F., Francesconi, S., Ricci, L., Laurenti, M. E., Capotorti, A., Artico, M., D’Andrea, V., Henry, B. M., Fedeli, P., & Carlini, L. (2021). Analysis of the Different Lymphatic Drainage Patterns during Sentinel Lymph Node Biopsy for Skin Melanoma. Journal of Clinical Medicine, 10(23), 5544. https://doi.org/10.3390/jcm10235544