
Photodynamic Therapy in the Treatment of Vulvar Lichen Sclerosus: A Systematic Review of the Literature



Abstract
:1. Introduction
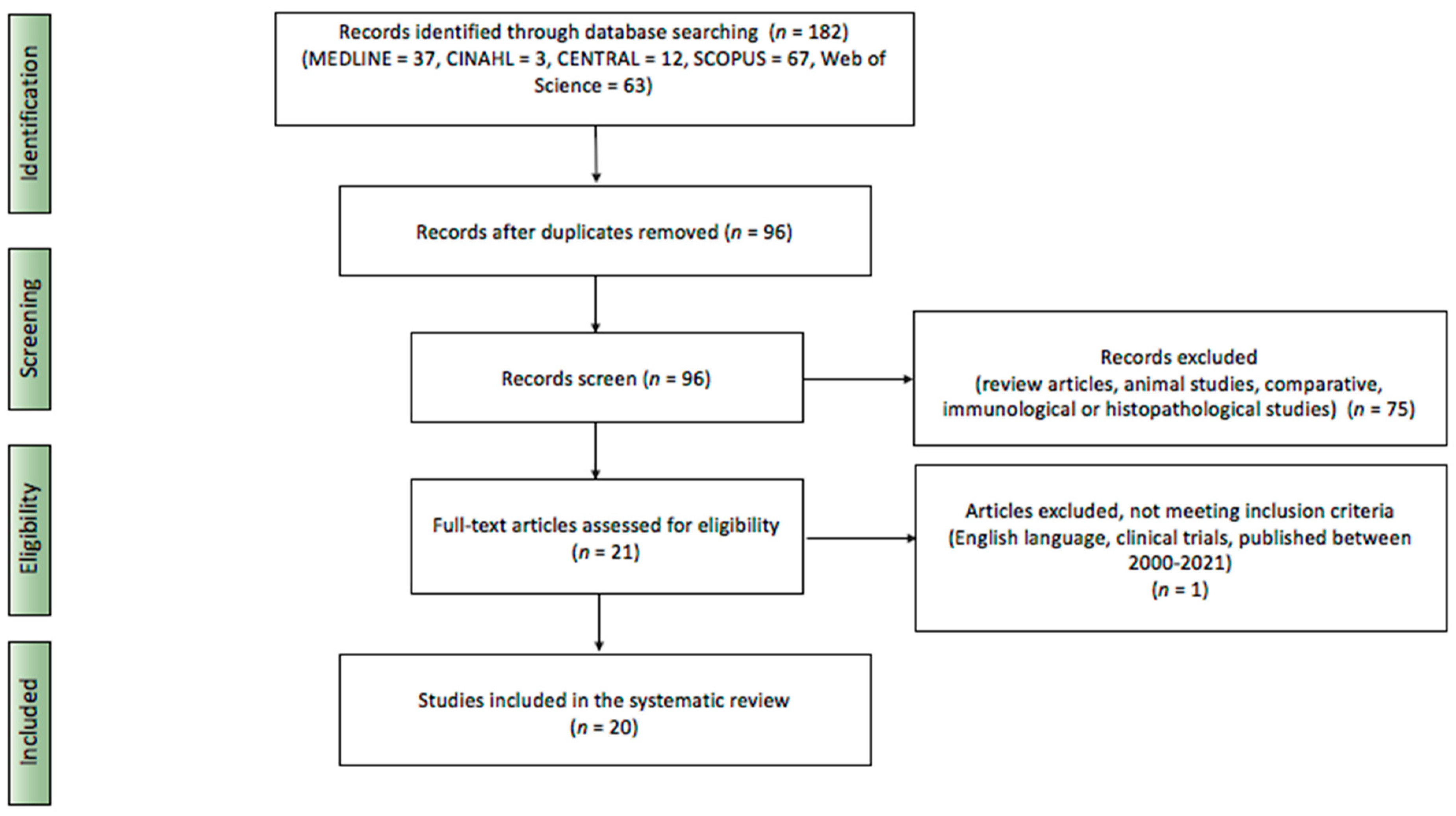
2. Materials and Methods
3. Results
3.1. Characteristics of Included Studies
3.2. Photodynamic Therapy Parameters of Included Studies
3.3. Main Outcomes
3.4. Adverse Effects
3.5. Recurrences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darier, J. Lichen plan sclereux. Ann. Dermatol. Syph. 1892, 23, 833–887. [Google Scholar]
- Fistarol, S.K.; Itin, P.H. Diagnosis and treatment of lichen sclerosus: An update. Am. J. Clin. Dermatol. 2013, 14, 27–47. [Google Scholar] [CrossRef] [Green Version]
- Tran, D.A.; Tan, X.; Macri, C.J.; Goldstein, A.T.; Fu, S.W. Lichen Sclerosus: An autoimmunopathogenic and genomic enigma with emerging genetic and immune targets. Int. J. Biol. Sci. 2019, 15, 1429–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campolmi, P.; Cannarozzo, G.; Bennardo, L.; Clementi, A.; Sannino, M.; Nisticò, S. Fractional Micro-Ablative CO2 Laser as Therapy in Penile Lichen Sclerosus: CO2 Laser to Treat Penile Lichen Sclerosus. J. Lasers Med Sci. 2021, 12, e61. [Google Scholar] [CrossRef]
- Jabłonowska, O.; Woźniacka, A.; Żebrowska, A. Lichen sclerosus. Dermatol. Rev. Przegląd Dermatol. 2021, 108, 126–136. [Google Scholar] [CrossRef]
- Melnick, L.E.; Steuer, A.B.; Bieber, A.K.; Wong, P.W.; Pomeranz, M.K. Lichen sclerosus among women in the United States. Int. J. Women’s Dermatol. 2020, 6, 260–262. [Google Scholar] [CrossRef]
- Cooper, S.M.; Ali, I.; Baldo, M.; Wojnarowska, F. The association of lichen sclerosus and erosive lichen planus of the vulva with autoimmune disease: A case-control study. Arch. Dermatol. 2008, 144, 1432–1435. [Google Scholar] [CrossRef]
- Kirtschig, G. Lichen Sclerosus-Presentation, Diagnosis and Management. Dtsch. Ärzteblatt Int. 2016, 113, 337–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirtschig, G.; Becker, K.; Günthert, A.; Jasaitiene, D.; Cooper, S.; Chi, C.C.; Kreuter, A.; Rall, K.K.; Aberer, W.; Riechardt, S.; et al. Evidence-based (S3) Guideline on (anogenital) Lichen sclerosus. J. Eur. Acad. Dermatol. Venereol. 2015, 29, e1–e43. [Google Scholar] [CrossRef]
- Dinh, H.; Purcell, S.M.; Chung, C.; Zaenglein, A.L. Pediatric Lichen Sclerosus: A Review of the Literature and Management Recommendations. J. Clin. Aesthet. Dermatol. 2016, 9, 49–54. [Google Scholar] [PubMed]
- Singh, N.; Ghatage, P. Etiology, Clinical Features, and Diagnosis of Vulvar Lichen Sclerosus: A Scoping Review. Obstet. Gynecol. Int. 2020, 2020, 7480754. [Google Scholar] [CrossRef] [PubMed]
- Kwok, R.; Shah, T.T.; Minhas, S. Recent advances in understanding and managing Lichen Sclerosus. F1000Research 2020, 9, F1000. [Google Scholar] [CrossRef] [PubMed]
- Paulis, G.; Berardesca, E. Lichen sclerosus: The role of oxidative stress in the pathogenesis of the disease and its possible transformation into carcinoma. Res. Rep. Urol. 2019, 11, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Spekreijse, J.J.; Streng, B.M.M.; Vermeulen, R.F.M.; Voss, F.O.; Vermaat, H.; van Beurden, M. The risk of developing squamous cell carcinoma in patients with anogenital lichen sclerosis: A systematic review. Gynecol. Oncol. 2020, 157, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Ishikawa, O.; Asano, Y.; Sato, S.; Jinnin, M.; Takehara, K.; Fujimoto, M.; Yamamoto, T.; Ihn, H. Diagnostic criteria, severity classification and guidelines of lichen sclerosus et atrophicus. J. Dermatol. 2018, 45, 891–897. [Google Scholar] [CrossRef] [Green Version]
- Errichetti, E.; Lallas, A.; Apalla, Z.; Di Stefani, A.; Stinco, G. Dermoscopy of Morphea and Cutaneous Lichen Sclerosus: Clinicopathological Correlation Study and Comparative Analysis. Dermatology 2017, 233, 462–470. [Google Scholar] [CrossRef]
- Ankad, B.S.; Beergouder, S.L. Dermoscopic patterns in lichen sclerosus: A report of three cases. Indian Dermatol. Online J. 2015, 6, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Van de Nieuwenhof, H.P.; Meeuwis, K.A.; Nieboer, T.E.; Vergeer, M.C.; Massuger, L.F.; De Hullu, J.A. The effect of vulvar lichen sclerosus on quality of life and sexual functioning. J. Psychosom. Obstet. Gynaecol. 2010, 31, 279–284. [Google Scholar] [CrossRef]
- Felmingham, C.; Chan, L.; Doyle, L.W.; Veysey, E. The Vulval Disease Quality of Life Index in women with vulval lichen sclerosus correlates with clinician and symptom scores. Australas. J. Dermatol. 2020, 61, 110–118. [Google Scholar] [CrossRef]
- Akel, R.; Fuller, C. Updates in lichen sclerosis: British Association of Dermatologists guidelines for the management of lichen sclerosus 2018. Br. J. Dermatol. 2018, 178, 823–824. [Google Scholar] [CrossRef]
- Krapf, J.M.; Mitchell, L.; Holton, M.A.; Goldstein, A.T. Vulvar Lichen Sclerosus: Current Perspectives. Int. J. Women’s Health 2020, 12, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, F.M.; Tatnall, F.M.; Velangi, S.S.; Bunker, C.B.; Kumar, A.; Brackenbury, F.; Mohd Mustapa, M.F.; Exton, L.S. British Association of Dermatologists guidelines for the management of lichen sclerosus, 2018. Br. J. Dermatol. 2018, 178, 839–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eshtiaghi, P.; Sadownik, L.A. Fact or Fiction? Adipose-Derived Stem Cells and Platelet-Rich Plasma for the Treatment of Vulvar Lichen Sclerosus. J. Low. Genit. Tract Dis. 2019, 23, 65–70. [Google Scholar] [CrossRef]
- Del Duca, E.; Manfredini, M.; Petrini, N.; Farnetani, F.; Chester, J.; Bennardo, L.; Schipani, G.; Tamburi, F.; Sannino, M.; Cannarozzo, G.; et al. Daylight photodynamic therapy with 5-aminolevulinic acid 5% gel for the treatment of mild-to-moderate inflammatory acne. Ital. J. Dermatol. Venerol. 2021, 156, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Gunaydin, G.; Gedik, M.E.; Ayan, S. Photodynamic Therapy for the Treatment and Diagnosis of Cancer-A Review of the Current Clinical Status. Front. Chem. 2021, 9, 686303. [Google Scholar] [CrossRef]
- Biniszkiewicz, T.; Olejek, A.; Kozak-Darmas, I.; Sieroń, A. Therapeutic effects of 5-ALA-induced photodynamic therapy in vulvar lichen sclerosus. Photodiagnosis Photodyn. Ther. 2005, 2, 157–160. [Google Scholar] [CrossRef]
- Romero, A.; Hernández-Núñez, A.; Córdoba-Guijarro, S.; Arias-Palomo, D.; Borbujo-Martínez, J. Treatment of recalcitrant erosive vulvar lichen sclerosus with photodynamic therapy. J. Am. Acad. Dermatol. 2007, 57, 46–47. [Google Scholar] [CrossRef]
- Sotiriou, E.; Panagiotidou, D.; Ioannidis, D. An open trial of 5-aminolevulinic acid photodynamic therapy for vulvar lichen sclerosus. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 141, 187–188. [Google Scholar] [CrossRef]
- Sotiriou, E.; Apalla, Z.; Patsatsi, A.; Panagiotidou, D. Recalcitrant vulvar lichen sclerosis treated with aminolevulinic acid-photodynamic therapy: A report of five cases. J. Eur. Acad. Dermatol. Venereol. 2008, 22, 1398–1399. [Google Scholar] [CrossRef]
- Vano-Galvan, S.; Fernandez-Guarino, M.; Beà-Ardebol, S.; Perez, B.; Harto, A.; Jaen, P. Successful treatment of erosive vulvar lichen sclerosus with methylaminolaevulinic acid and laser-mediated photodynamic therapy. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 71–72. [Google Scholar] [CrossRef]
- Zawislak, A.A.; McCluggage, W.G.; Donnelly, R.F.; Maxwell, P.; Price, J.H.; Dobbs, S.P.; McClelland, H.R.; Woolfson, A.D.; Mccarron, P.A. Response of vulval lichen sclerosus and squamous hyperplasia to photodynamic treatment using sustained topical delivery of aminolevulinic acid from a novel bioadhesive patch system. Photodermatol. Photoimmunol. Photomed. 2009, 25, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Skrzypulec, V.; Olejek, A.; Drosdzol, A.; Nowosielski, K.; Kozak-Darmas, I.; Wloch, S. Sexual functions and depressive symptoms after photodynamic therapy for vulvar lichen sclerosus in postmenopausal women from the Upper Silesian Region of Poland. J. Sex. Med. 2009, 6, 3395–3400. [Google Scholar] [CrossRef] [PubMed]
- Osiecka, B.J.; Nockowski, P.; Jurczyszyn, K.; Ziólkowski, P. Photodynamic therapy of vulvar lichen sclerosus et atrophicus in a woman with hypothyreosis—Case report. Photodiagnosis Photodyn. Ther. 2012, 9, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Imbernón-Moya, A.; Martínez-Pérez, M.; Churruca-Grijelmo, M.; Lobato-Berezo, A.; Vargas-Laguna, E.; Fernández-Cogolludo, E.; Aguilar-Martínez, A.; Gallego-Valdés, M.Á. Photodynamic therapy as a therapeutic alternative in vulvar lichen sclerosus: Series of 8 cases. Photodermatol. Photoimmunol. Photomed. 2016, 32, 307–310. [Google Scholar] [CrossRef]
- Osiecka, B.J.; Jurczyszyn, K.; Nockowski, P.; Murawski, M.; Ziółkowski, P. Photodynamic therapy with green light for the treatment of vulvar lichen sclerosus—Preliminary results. Photodiagnosis Photodyn. Ther. 2017, 17, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Maździarz, A.; Osuch, B.; Kowalska, M.; Nalewczyńska, A.; Śpiewankiewicz, B. Photodynamic therapy in the treatment of vulvar lichen sclerosus. Photodiagnosis Photodyn. Ther. 2017, 19, 135–139. [Google Scholar] [CrossRef]
- Olejek, A.; Gabriel, I.; Bilska-Janosik, A.; Kozak-Darmas, I.; Kawczyk-Krupka, A. ALA-Photodynamic treatment in Lichen sclerosus-clinical and immunological outcome focusing on the assesment of antinuclear antibodies. Photodiagnosis Photodyn. Ther. 2017, 18, 128–132. [Google Scholar] [CrossRef]
- Lan, T.; Zou, Y.; Hamblin, M.R.; Yin, R. 5-Aminolevulinic acid photodynamic therapy in refractory vulvar lichen sclerosus et atrophicus: Series of ten cases. Photodiagnosis Photodyn. Ther. 2018, 21, 234–238. [Google Scholar] [CrossRef]
- Maździarz, A. Successful pregnancy and delivery following selective use of photodynamic therapy in treatment of cervix and vulvar diseases. Photodiagnosis Photodyn. Ther. 2019, 28, 65–68. [Google Scholar] [CrossRef]
- Zhang, F.; Li, D.; Shi, L.; Gu, Y.; Xu, Y. 5-ALA-photodynamic therapy in refractory vulvar lichen sclerosus et atrophicus. Int. J. Clin. Exp. Pathol. 2020, 13, 3100–3110. [Google Scholar]
- Li, Z.; Wang, Y.; Wang, J.; Li, S.; Xiao, Z.; Feng, Y.; Gu, J.; Li, J.; Peng, X.; Li, C.; et al. Evaluation of the efficacy of 5-aminolevulinic acid photodynamic therapy for the treatment of vulvar lichen sclerosus. Photodiagnosis Photodyn. Ther. 2020, 29, 101596. [Google Scholar] [CrossRef]
- Cao, Y.; Zhang, G.; Wang, P.; Li, C.; Wang, X. Treatment of Hyperkeratotic Vulvar Lichen Sclerosus with combination of holmium laser therapy and ALA-PDT: Case report. Photodiagnosis Photodyn. Ther. 2020, 31, 101762. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Hao, J.; Wang, Y.; Liu, Y.; Xu, T. Clinical and Dermoscopic Assessment of Vulvar Lichen Sclerosus after 5-Aminolevulinic Acid Photodynamic Therapy: A Prospective Study. Photodiagnosis Photodyn. Ther. 2021, 33, 102109. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Li, D.; Shi, L.; Gu, Y.; Xu, Y.; Wu, C. Efficacy of 5-Aminolevulinic Acid (ALA)-Photodynamic Therapy (PDT) in Refractory Vulvar Lichen Sclerosus: Preliminary Results. Med. Sci. Monit. 2021, 27, e927406. [Google Scholar] [CrossRef]
- Zielińska, A.; Maździarz, A.; Abdalla, N.; Sawicki, W.; Dmoch-Gajzlerska, E. Does HPV infection have impact on results of photodynamic treatment of vulvar lichen sclerosus? Photodiagnosis Photodyn. Ther. 2021, 34, 102138. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.; Khachemoune, A. An update on topical photodynamic therapy for clinical dermatologists. J. Dermatol. Treat. 2019, 30, 732–744. [Google Scholar] [CrossRef]
- Kennedy, J.C.; Pottier, R.H.; Pross, D.C. Photodynamic therapy with endogenous protoporphyrin IX: Basic principles and present clinical experience. J. Photochem. Photobiol. B Biol. 1990, 6, 143–148. [Google Scholar] [CrossRef]
- Corazza, M.; Schettini, N.; Zedde, P.; Borghi, A. Vulvar Lichen Sclerosus from Pathophysiology to Therapeutic Approaches: Evidence and Prospects. Biomedicines 2021, 9, 950. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.T.; Creasey, A.; Pfau, R.; Phillips, D.; Burrows, L.J. A double-blind, randomized controlled trial of clobetasol versus pimecrolimus in patients with vulvar lichen sclerosus. J. Am. Acad. Dermatol. 2011, 64, 99–104. [Google Scholar] [CrossRef]
- Renaud-Vilmer, C.; Cavelier-Balloy, B.; Porcher, R.; Dubertret, L. Vulvar lichen sclerosus: Effect of long-term topical application of a potent steroid on the course of the disease. Arch. Dermatol. 2004, 140, 709–712. [Google Scholar] [CrossRef] [Green Version]
- Shi, L.; Miao, F.; Zhang, L.L.; Zhang, G.L.; Wang, P.R.; Ji, J.; Wang, X.J.; Huang, Z.; Wang, H.W.; Wang, X.L. Comparison of 5-Aminolevulinic Acid Photodynamic Therapy and Clobetasol Propionate in Treatment of Vulvar Lichen Sclerosus. Acta Derm.-Venereol. 2016, 96, 684–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Declercq, A.; Güvenç, C.; De Haes, P. Proposition of standardized protocol for photodynamic therapy for vulvar lichen sclerosus. J. Dermatolog. Treat. 2020, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| No. | Study | Type of Study | Number of Patients/Patients’ Age | Previous Treatment of VLS | Photosensitizer: Type/Time of Incubation | PDT Characteristic: Light/Wavelength/Power Density | Number of Treatment/Time Interval | Outcome | Adverse Effect |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Biniszkiewicz et al. (2005) [26] | Prospective cohort | 24 women/ 58 years on average | Not reported | 20% 5-ALA/115 min | Coherent/630 nm, 180 J/cm2, 700 mW/cm2 | 3–6 therapy cycles/14-day interval | -remission of subjective symptoms in 23 patients -maintenance of the subjective symptoms in one patient | minimal local toxicity: vulvar erythema |
| 2 | Romero et al. (2007) [27] | Case report | One woman/ 61 years | Surgical treatment, topical corticosteroids, topical tacrolimus 0.1%, hydroxychloroquine 200 mg/day, oral prednisone 0.5 mg/kg/day | 20% 5-ALA/2 h | Noncoherent 633 nm red light, 30 J/cm2, 80 mW/cm2 | Two treatments/1-month interval | -almost total reduction of subjective symptoms; -marked improvement of objective symptoms; -improvement of sexual life | Moderate pain during irradiation |
| 3 | Sotiriou et al. (2008) [28] | Case series | 10 women/ 54.6 years on average | Topical corticosteroids, pimecrolimus ointment | 20% 5-ALA/4 h | Noncoherent 570–670 nm red light, 40 J/cm2, 80 mW/cm | Two treatments/2-week interval | -minor improvement of clinical signs in nine patients; -no improvement in one patient; -remission or reduction of subjective symptoms in all of the patients | Burning and stinging sensation during treatment; erythema up to 1 week after irradiation |
| 4 | Sotiriou et al. (2008) [29] | Case series | Five women/ 61.4 years on average | Topical corticosteroids, tacrolimus ointment 0.1% | 20% 5-ALA/3 h | Noncoherent 570–670 nm red light, 40 J/cm2, 80 mW/cm2 | One session | -significant reduction of subjective signs in all patients; -no resolution of histopathological features; -mean duration of reduction of symptoms 4.6 months | Burning sensation during the procedure, local erythema 3–5 days after therapy |
| 5 | Vano-Galvan et al. (2008) [30] | Case report | One woman/ 68 years | Topical 0.1% halcinonide once daily, tacrolimus 60.1% ointment, oral prednisone 0.5 mg/kg/day | MAL/2 h | Coherent, 585 nm, 7 mm, 6 ms, 9 J/cm2 | Three cycles/a one-month interval | -marked clinical improvement, -almost total reduction of subjective symptoms | Intense pain during the procedure |
| 6 | Zawiślak et al. (2009) [31] | Prospective cohort | Eight women/ Age not reported | Not reported | Bioadhesive patch system with ALA/4–6 h | Noncoherent 630 nm red light, 100 J/cm2 | Two sessions/2–15-week intervals | -marked decrease of subjective symptoms; -no resolution of histopathological features | Intense pain during first 3 min of irradiation; post-treatment pain lasting for at least 24 h |
| 7 | Skrzypulec et al. (2009) [32] | Prospective cohort | 37 women/ 50–70 years (59.98 years on average) | Not reported | 5% ALA/4–5 h | Coherent 635 nm, 80 J/cm2, 40–70 mW/cm2 | Six cycles/2-week interval | -reduction in the severity of symptoms in 28 patients; -no negative influence on sexual life; -beneficial effect on depressive disorders | Lubrication disorders |
| 8 | Osiecka et al. (2012) [33] | Case report | One woman/ 30 years | Clobetasol propionate, tacrolimus | 20% 5-ALA/4 h | Noncoherent 630 nm red light, 150 J/cm2, 100 mW/cm2 | a total of six sessions; the first two separated by 4 weeks; the 3rd performed 6 months after starting treatment; the 4th after another 6 weeks; no information about the 5th and 6th sessions is available | -complete remission of objective and subjective symptoms, except few days in the perimenstrual period | Marked itching during the first treatment, burning within 24 h after the first irradiation |
| 9 | Imbernón-Moya et al. (2016) [34] | Case series | Eight women/ seven women > 60 years One woman: 38 years | Topical corticosteroids, topical calcineurin inhibitors | MAL/3 h | Noncoherent 630 nm red light, 37 J/cm2, 70 mW/cm2 | 1–3 treatments/6–12 months interval | -significant improvement in subjective symptoms and quality of life in all cases; -lack of improvement in clinical presentation in all cases | Mild erythema, edema, burning, urinary problems |
| 10 | Osiecka et al. (2017) [35] | Prospective cohort | 11 women/ 30–66 years (48 on average) | Topical corticosteroids, estrogens, topical calcineurin inhibitors | 20% 5-ALA/5 h | Noncoherent 540 ± 15 nm green light, 62.5 J/cm2, 85 mW/cm2; fractionated—2 min irradiation, then 1 min pause | Three treatments/2-week interval | -complete resolution of objective symptoms in 5/5 patients 2 months after PDT; -complete resolution of subjective symptoms 2 months after PDT in 9/11 women, one remaining in moderate intensity, the other one in low intensity | Itching as the main symptom, weak or moderate pain, mild edema, and erythema |
| 11 | Maździarz et al. (2017) [36] | Prospective cohort | 102 women/ 19–85 years (55.08 on average) | Topical corticosteroids | 5% 5-ALA with 2% DMSO/3 h | Noncoherent 590–760 nm, 120 J/cm2, 204 mW/cm2 | 10 applications/one-week interval | -complete or partial remission in 87% of patients, -decrease in the number of objective signs (improvement rate 100%—70% in 60.78% of patients, around 50% in 16.67% of patients, 30% in 9.8%, less than 30% in 12.75%) | Paresthesia during irradiation in 39 patients, in 12 patients swelling for a few hours |
| 12 | Olejek et al. (2017) [37] | Prospective, controlled cohort | 100 women/ 57 years on average in the first group (n = 40) and 58.5 years on average in the second group (n = 60) | Not reported | 10% ALA with 20% DMSO/3 h | First group: coherent 630 nm red light Second group: 580–1400 nm 100 J/cm2; 40–80 mW/cm2 | 10 applications/one-week interval | -significant reduction of subjective symptoms in 92% patients, -in 8% of patients’ symptoms of the same or worse intensity | No visible side effects |
| 13 | Lan et al. (2018) [38] | Case series | 10 women/ 51 years on average | Topical corticosteroids, topical calcineurin inhibitors, cryosurgery | 10% 5-ALA/3 h | Noncoherent 635 ± 15 nm red light, 100 J/cm2, 100 mW/cm2 | Three sessions/2-week interval | -resolution of subjective symptoms in 10 patients, -complete resolution of sexual dysfunction; -improvement of quality of life; -significant decrease of lesion size; -no recurrences during the observation period | Short-term pain, burning, erythema, and edema during and after irradiation |
| 14 | Maździarz (2019) [39] | Prospective cohort | Two women/ 22 and 23 years | Topical corticosteroids | 5% 5-ALA with 2% DMSO/3 h | Noncoherent 590–760 nm, 120 J/cm2, 204 mW/cm2 | 10 applications/one-week interval | remission of vulvar lesions and negative HPV DNA results in one patient | Short-term pain and burning sensation |
| 15 | Zhang (2020) [40] | Case series | 30 women/ 48.23 years on average | Topical corticosteroids, vitamin E, Haijisin | 20% 5-ALA/3 h | Noncoherent 631–635 nm red light, 60–90 mW/cm2 | Three sessions/ 2-week interval | -total resolution of pruritus in 25 patients, improvement in three patients, -complete resolution of pain in 28 patients, mild to moderate pain in two patients -total resolution of sexual dysfunction in 26 patients, moderate to severe sexual intercourse persisting in 4 patients | Short-term pain, burning, erythema, and edema |
| 16 | Li et al. (2020) [41] | Prospective cohort | 10 women/ 35.4 years on average | Topical corticosteroids | 20% 5-ALA/3 h | Coherent 635 nm red light, 80 J/cm2, 80 mW/cm2 | 4–9 sessions, depending on the condition | -significant reduction in objective and subjective symptoms of VLS and improvement in quality of life -no recurrence of lesions 3 months after PDT -recurrence of lesions 6 months after PDT in two patients | -mild to moderate pain in eight women undergoing PDT -burning sensation, swelling, erythema in six women, lasting up to 5 days after irradiation |
| 17 | Cao et al. (2020) [42] | Case report | One woman/ 72 years | Clobetasol propionate 0.5% cream | 10% 5-ALA/3 h | Noncoherent 635 nm red light, 100 J/cm2, 200 mW/cm2 | Three treatments at 2-week intervals, then after one month, a holmium laser treatment in combination with the last PDT | -VLS areas reduced and thinned after three PDT treatments -almost complete remission after last combined laser + PDT treatment -relief of subjective symptoms -no recurrence of lesions after 1 year of follow-up -satisfaction of patients with the treatment | Mild swelling and erythema after each treatment, moderate pain |
| 18 | Liu et al. (2021) [43] | Prospective cohort | 24 women/ 21–61 years (45 years on average) | Not reported | 20% 5-ALA/3 h | Noncoherent 633 nm red light, 60 mW/cm2 | Six treatments/2-week intervals | -significant remission of clinical signs -gradual alleviation of subjective symptoms with subsequent PDT treatments -marked improvement of the dermoscopic features | -in 19 cases, transient complaints of pain (<24 h) -in seven cases, erosions healed within one week after PDT |
| 19 | Zhang et al. (2021) [44] | Prospective cohort | 30 women/ 48.2 years on average | Topical corticosteroids, vitamin E cream | 20% 5-ALA/3 h | Noncoherent 635 nm red light, 100–150 J/cm2, 60–90 mW/cm2 | Three sessions/2-week interval | -significant reduction of objective signs -improvement of histopathological findings -significant reduction of sexual dysfunctions, considerable improvement of patients’ quality of life -recurrence of lesions in three patients at 6 months follow-up | -pain and burning sensation gradually subsiding 3 to 48 h after the procedure -slight erythema and swelling for up to 4 days after PDT |
| 20 | Zielińska et al. (2021) [45] | Prospective cohort | 73 women/ 9–81 years (54.1 years on average) | Not reported | 5% 5-ALA with 2% DMSO/2 h | Noncoherent 630 nm, 120 J/cm2 204 mW/cm2 | a full cycle of 10 treatments once a week; if necessary, the cycle was repeated after 3 months (one cycle: 37 women, two cycles: 30 women, three cycles: six women) | -resolution of subjective symptoms in all patients -histopathological remission in two patients -clinical remission without histopathological remission in 55 patients -no significant influence of HPV infection on the number of procedures -no relevant correlation between duration of clinical remission and HPV status | 32 patients reported paresthesia during PDT that resolved after treatment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerkowicz, A.; Szczepanik-Kułak, P.; Krasowska, D. Photodynamic Therapy in the Treatment of Vulvar Lichen Sclerosus: A Systematic Review of the Literature. J. Clin. Med. 2021, 10, 5491. https://doi.org/10.3390/jcm10235491
Gerkowicz A, Szczepanik-Kułak P, Krasowska D. Photodynamic Therapy in the Treatment of Vulvar Lichen Sclerosus: A Systematic Review of the Literature. Journal of Clinical Medicine. 2021; 10(23):5491. https://doi.org/10.3390/jcm10235491
Chicago/Turabian StyleGerkowicz, Agnieszka, Paulina Szczepanik-Kułak, and Dorota Krasowska. 2021. "Photodynamic Therapy in the Treatment of Vulvar Lichen Sclerosus: A Systematic Review of the Literature" Journal of Clinical Medicine 10, no. 23: 5491. https://doi.org/10.3390/jcm10235491
APA StyleGerkowicz, A., Szczepanik-Kułak, P., & Krasowska, D. (2021). Photodynamic Therapy in the Treatment of Vulvar Lichen Sclerosus: A Systematic Review of the Literature. Journal of Clinical Medicine, 10(23), 5491. https://doi.org/10.3390/jcm10235491