
Clinical Outcomes following Large Vessel Coronary Artery Perforation Treated with Covered Stent Implantation: Comparison between Polytetrafluoroethylene- and Polyurethane-Covered Stents (CRACK-II Registry)


 , ,
, ,  , , , , , , add
Show full author list
, , , , , , add
Show full author list
Abstract
1. Introduction
2. Methods
2.1. Evaluated Covered Stents and Structural Insight
2.2. Procedure
2.3. Angiography Analysis
2.4. Patient Follow-Up and Study Endpoints
2.5. Statistical Analysis
3. Results
3.1. Baseline Clinical Characteristics
3.2. Angiographic and Culprit Lesion Characteristics
3.3. Procedural Indices
3.4. Coronary Artery Perforation and Periprocedural Complications
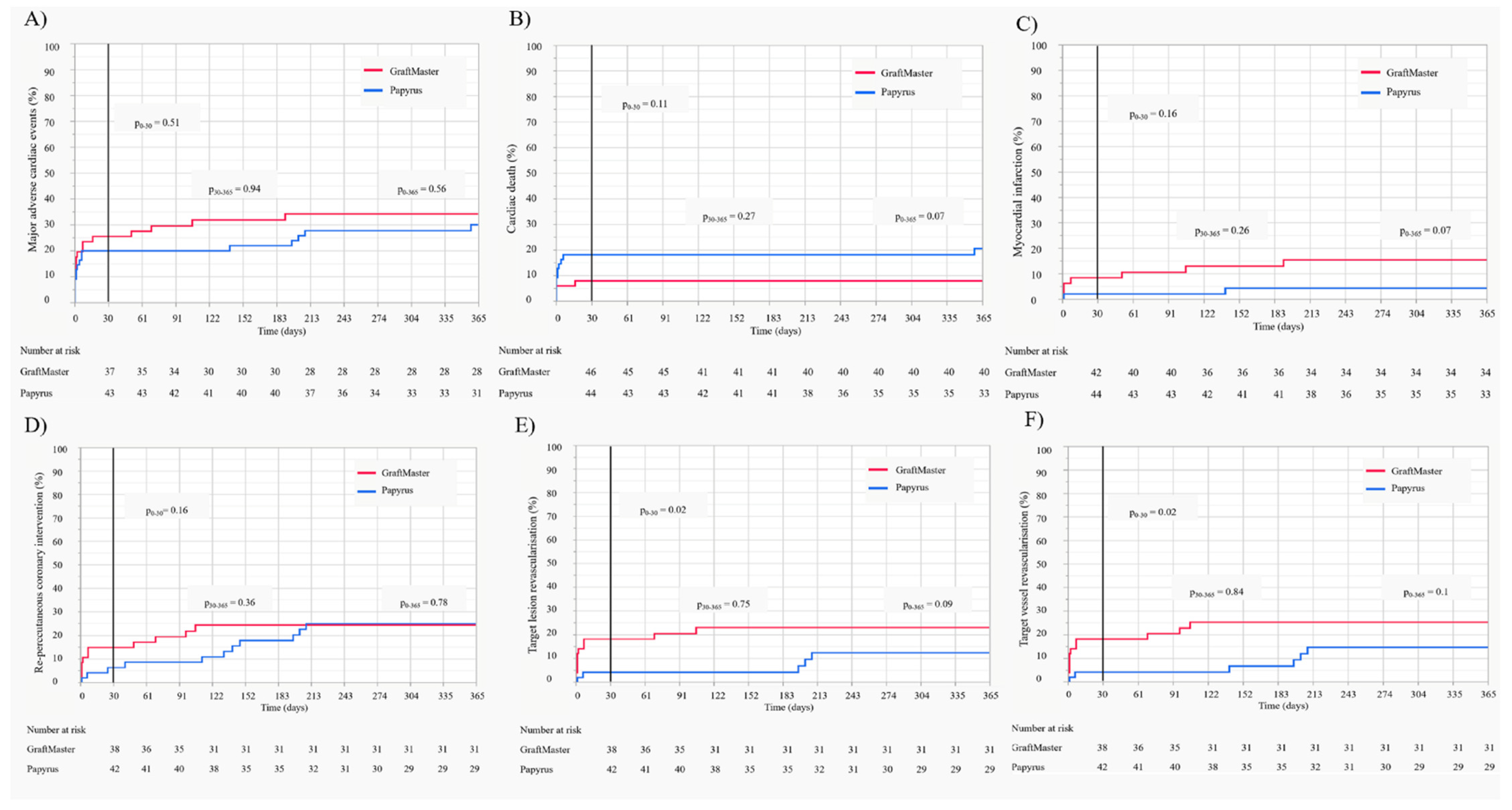
3.5. Clinical Endpoints and Follow-Up
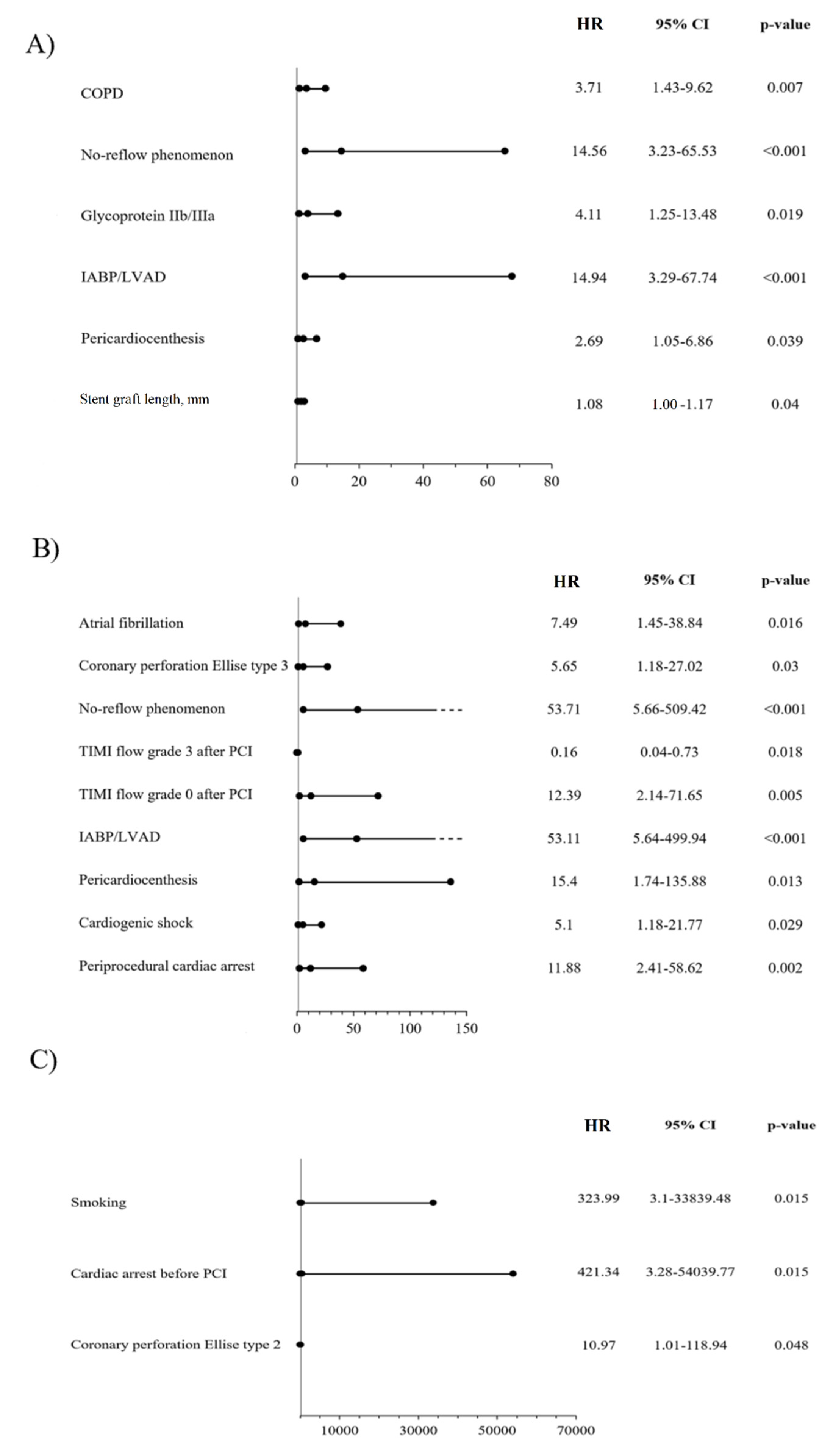
3.6. Predictors of Clinical Outcomes
4. Discussion
Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shimony, A.; Joseph, L.; Mottillo, S.; Eisenberg, M.J. Coronary artery perforation during percutaneous coronary intervention: A systematic review and meta-analysis. Can. J. Cardiol. 2011, 27, 843–850. [Google Scholar] [CrossRef]
- Januszek, R.; Bryniarski, L.; Siudak, Z.; Malinowski, K.P.; Bryniarski, K.L.; Surdacki, A.; Dziewierz, A.; Mika, P.; Wańha, W.; Wojakowski, W.; et al. Five-year report from the Polish national registry on percutaneous coronary interventions with a focus on coronary artery perforations within chronic total occlusions. Postepy Kardiol. Interwencyjnej 2020, 16, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Tajti, P.; Burke, M.N.; Karmpaliotis, D.; Alaswad, K.; Werner, G.S.; Azzalini, L.; Carlino, M.; Patel, M.; Mashayekhi, K.; Egred, M.; et al. Update in the Percutaneous Management of Coronary Chronic Total Occlusions. JACC Cardiovasc. Interv. 2018, 11, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Danek, B.A.; Karatasakis, A.; Tajti, P.; Sandoval, Y.; Karmpaliotis, D.; Alaswad, K.; Jaffer, F.; Yeh, R.W.; Kandzari, D.E.; Lembo, N.J.; et al. Incidence, Treatment, and Outcomes of Coronary Perforation during Chronic Total Occlusion Percutaneous Coronary Intervention. Am. J. Cardiol. 2017, 120, 1285–1292. [Google Scholar] [CrossRef] [PubMed]
- Ellis, S.G.; Ajluni, S.; Arnold, A.Z.; Popma, J.J.; Bittl, J.A.; Eigler, N.L.; Cowley, M.J.; Raymond, R.E.; Safian, R.D.; Whitlow, P.L. Increased coronary perforation in the new device era. Incidence, classification, management, and outcome. Circulation 1994, 90, 2725–2730. [Google Scholar] [CrossRef] [PubMed]
- Lemmert, M.E.; van Bommel, R.J.; Diletti, R.; Wilschut, J.M.; de Jaegere, P.P.; Zijlstra, F.; Daemen, J.; Van Mieghem, N.M. Clinical Characteristics and Management of Coronary Artery Perforations: A Single-Center 11-Year Experience and Practical Overview. J. Am. Heart Assoc. 2017, 6, e007049. [Google Scholar] [CrossRef] [PubMed]
- Kilic, I.D.; Fabris, E.; Serdoz, R.; Caiazzo, G.; Foin, N.; Abou-Sherif, S.; Di Mario, C. Coronary covered stents. EuroIntervention 2016, 12, 1288–1295. [Google Scholar] [CrossRef] [PubMed]
- Takano, M.; Yamamoto, M.; Inami, S.; Xie, Y.; Murakami, D.; Okamatsu, K.; Ohba, T.; Seino, Y.; Mizuno, K. Delayed endothelialization after polytetrafluoroethylene-covered stent implantation for coronary aneurysm. Circ. J. 2009, 73, 190–193. [Google Scholar] [CrossRef]
- Harnek, J.; James, S.K.; Lagerqvist, B. Very long-term outcome of coronary covered stents: A report from the SCAAR registry. EuroIntervention 2019, 14, 1660–1667. [Google Scholar] [CrossRef]
- Schächinger, V.; Hamm, C.W.; Münzel, T.; Haude, M.; Baldus, S.; Grube, E.; Bonzel, T.; Konorza, T.; Köster, R.; Arnold, R.; et al. A randomized trial of polytetrafluoroethylene-membrane-covered stents compared with conventional stents in aortocoronary saphenous vein grafts. J. Am. Coll. Cardiol. 2003, 42, 1360–1369. [Google Scholar] [CrossRef]
- Wańha, W.; Januszek, R.; Kołodziejczak, M.; Gilis-Malinowska, N.; Figatowski, T.; Milewski, M.; Pawlik, A.; Staszczak, B.; Wybraniec, M.; Tomasiewicz, B.; et al. Procedural and 1-year outcomes following large vessel coronary artery perforation treated by covered stents implantation: Multicentre CRACK registry. PLoS ONE 2021, 16, e0249698. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.J.; Faxon, D.P.; Gunnar, R.M.; Kennedy, J.W.; King, S.B., 3rd; Loop, F.D.; Peterson, K.L.; Reeves, T.J.; Williams, D.O.; Winters, W.L., Jr.; et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation 1988, 78, 486–502. [Google Scholar] [PubMed]
- Cutlip, D.E.; Windecker, S.; Mehran, R.; Boam, A.; Cohen, D.J.; van Es, G.A.; Steg, P.G.; Morel, M.A.; Mauri, L.; Vranckx, P.; et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007, 115, 2344–2351. [Google Scholar] [CrossRef]
- Gercken, U.; Lansky, A.J.; Buellesfeld, L.; Desai, K.; Badereldin, M.; Mueller, R.; Selbach, G.; Leon, M.B.; Grube, E. Results of the Jostent coronary stent graft implantation in various clinical settings: Procedural and follow-up results. Catheter. Cardiovasc. Interv. 2002, 56, 353–360. [Google Scholar] [CrossRef]
- Kimura, T.; Itoh, T.; Sugawara, S.; Fusazaki, T.; Nakamura, M.; Morino, Y. Serial endovascular assessment of polytetrafluoroethylene-covered stent: Capabilities and limitations of intravascular imaging modalities affected by a temporal factor. J. Cardiol. Cases 2014, 11, 91–95. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lukito, G.; Vandergoten, P.; Jaspers, L.; Dendale, P.; Benit, E. Six months clinical, angiographic, and IVUS follow-up after PTFE graft stent implantation in native coronary arteries. Acta Cardiol. 2000, 55, 255–260. [Google Scholar] [CrossRef]
- Araki, M.; Hikita, H.; Sudo, Y.; Hishikari, K.; Takahashi, A. Restenosis of a Polytetrafluoroethylene-Covered Stent Visualized by Coronary Angioscopy and Optical Coherence Tomography: A Case Report. Int. J. Angiol. 2020, 29, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Papafaklis, M.I.; Sianos, G.; Cost, B.; Vaina, S.; Manginas, A.; Dardas, P.S.; Tsikaderis, D.; van Mieghem, C.A.; Michalis, L.K.; Serruys, P.W. Clinical and angiographic follow-up after overlapping implantation of polytetrafluoroethylene covered stents with drug eluting stents. EuroIntervention 2006, 2, 218–223. [Google Scholar] [PubMed]
- Stone, G.W.; Goldberg, S.; O’Shaughnessy, C.; Midei, M.; Siegel, R.M.; Cristea, E.; Dangas, G.; Lansky, A.J.; Mehran, R. 5-year follow-up of polytetrafluoroethylene-covered stents compared with bare-metal stents in aortocoronary saphenous vein grafts the randomized BARRICADE (barrier approach to restenosis: Restrict intima to curtail adverse events) trial. JACC Cardiovasc. Interv. 2011, 4, 300–309. [Google Scholar] [CrossRef]
- Tcheng, J.E.; Lim, I.H.; Srinivasan, S.; Jozic, J.; Gibson, C.M.; O’Shea, J.C.; Puma, J.A.; Simon, D.I. Stent parameters predict major adverse clinical events and the response to platelet glycoprotein IIb/IIIa blockade: Findings of the ESPRIT trial. Circ. Cardiovasc. Interv. 2009, 2, 43–51. [Google Scholar] [CrossRef] [PubMed][Green Version]
- PK Papyrus Covered Coronary Stent System. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfhde/hde.cfm?id=H170004 (accessed on 18 November 2021).
- GRAFT MASTER RX CORONARY STENT GRAFT SYSTM. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfhde/hde.cfm?id=396156 (accessed on 18 November 2021).




{kind=link}
{kind=link}
{kind=link}
| Selected Indices | Total n = 106 | GraftMaster n = 51 | Papyrus n = 55 | p-Value |
|---|---|---|---|---|
| Age, years | 69.05 ± 9.6 | 68.7 ± 9.5 | 69.3 ± 9.8 | 0.74 |
| Gender, males | 57 (53.8) | 26 (51) | 31 (56.4) | 0.57 |
| BMI, kg/m2 | 26.1 ± 5.4 | 26.6 ± 5.8 | 25.7 ± 5 | 0.8 |
| Chronic kidney failure | 27 (25.5) | 13 (25.5) | 14 (25.4) | 0.99 |
| Diabetes mellitus | 32 (30.2) | 16 (31.4) | 16 (29.1) | 0.79 |
| Arterial hypertension | 81 (76.4) | 39 (76.5) | 42 (76.4) | 0.98 |
| Hyperlipidaemia | 71 (67) | 35 (68.6) | 36 (65.5) | 0.72 |
| COPD | 15 (14.3) | 10 (20) | 5 (9) | 0.11 |
| Atrial fibrillation | 22 (20.7) | 6 (11.8) | 16 (29.1) | 0.03 |
| Smoking | 35 (33) | 14 (27.5) | 21 (38.2) | 0.24 |
| Prior myocardial infarction | 36 (34) | 22 (43.1) | 14 (25.5) | 0.05 |
| Prior PCI | 38 (35.9) | 22 (43.1) | 16 (29.1) | 0.13 |
| Prior CABG | 13 (12.3) | 6 (11.8) | 7 (12.7) | 0.88 |
| Neoplasm | 7 (6.6) | 5 (9.8) | 2 (3.6) | 0.25 |
| Clinical presentation | ||||
| Chronic coronary syndrome | 41 (38.7) | 24 (47.1) | 17 (30.9) | 0.09 |
| Unstable angina | 18 (17) | 8 (15.7) | 10 (18.2) | 0.73 |
| NSTEMI | 24 (22.6) | 6 (11.8) | 18 (32.7) | 0.01 |
| STEMI | 23 (21.7) | 13 (25.5) | 10 (18.2) | 0.36 |
| LVEF | 48.8 ± 12.4 | 48.9 ± 11.4 | 48.8 ± 13.4 | 0.89 |
| Selected Indices | Total n = 106 | GraftMaster n = 51 | Papyrus n = 55 | p-Value |
|---|---|---|---|---|
| Radial vascular access | 70 (66) | 31 (60.8) | 39 (70.9) | 0.27 |
| Coronary angiography | ||||
| Single-vessel disease | 44 (41.5) | 20 (39.2) | 24 (43.6) | 0.64 |
| Two-vessel disease | 41 (38.7) | 21 (41.2) | 20 (36.4) | 0.61 |
| Three-vessel disease | 19 (17.9) | 9 (17.6) | 10 (18.2) | 0.94 |
| Location of culprit lesion | ||||
| Left main coronary artery | 5 (4.7) | 1 (2) | 4 (7.3) | 0.36 |
| LAD | 54 (50.9) | 30 (58.8) | 24 (43.6) | 0.12 |
| Circumflex coronary artery | 18 (17) | 7 (13.7) | 11 (20) | 0.39 |
| Right coronary artery | 26 (24.5) | 8 (15.7) | 18 (32.7) | 0.04 |
| SvG | 9 (8.5) | 6 (11.8) | 3 (5.5) | 0.31 |
| Type of stenosis | ||||
| De novo lesion | 97 (91.5) | 44 (86.3) | 53 (96.4) | 0.08 |
| Thrombosis | 1 (0.9) | 1 (2) | 0 (0) | 0.48 |
| In-stent restenosis | 9 (8.5) | 7 (13.7) | 2 (3.6) | 0.08 |
| ACC/AHA lesion type | ||||
| - A | 3 (2.8) | 1 (2) | 2 (3.6) | 1 |
| - B | 36 (34.0) | 18 (35.3) | 18 (32.7) | 0.78 |
| - B/C | 28 (26.4) | 12 (23.5) | 16 (29.1) | 0.52 |
| - C | 39 (36.8) | 20 (39.2) | 19 (34.6) | 0.62 |
| Severe calcification | 29 (27.4) | 10 (19.6) | 19 (34.6) | 0.08 |
| Degree of stenosis | 88.2 ± 11.4 | 88.5 ± 10.7 | 87.9 ± 12 | 0.91 |
| Tortuosity | 12 (11.3) | 4 (7.8) | 8 (14.6) | 0.28 |
| Length of stenosis | 27.3 ± 14.1 | 23.4 ± 9.1 | 30.1 ± 16.5 | 0.1 |
| Length of stenosis ≥20 mm | 55 (71.4) | 22 (66.7) | 33 (75) | 0.42 |
| Bifurcation | 14 (13.2) | 6 (11.8) | 8 (14.6) | 0.67 |
| Chronic total occlusion | 6 (5.7) | 3 (5.9) | 3 (5.5) | 1 |
| Type of PCI | ||||
| Drug-eluting stent | 73 (70.2) | 28 (57.1) | 45 (81.8) | 0.006 |
| Bare-metal stent | 10 (9.6) | 7 (14.3) | 3 (5.5) | 0.18 |
| Plain-old balloon angioplasty | 16 (15.4) | 13 (26.5) | 3 (5.5) | 0.003 |
| Bioresorbable scaffold | 5 (4.8) | 1 (2) | 4 (7.3) | 0.37 |
| Rotablation | 8 (7.6) | 3 (5.9) | 5 (9.1) | 0.72 |
| Intravascular ultrasound | 4 (3.9) | 0 (0) | 4 (7.3) | 0.12 |
| Number of non-CS | ||||
| 0 | 20 (19.1) | 13 (25.5) | 7 (13) | 0.11 |
| 1 | 48 (45.7) | 22 (43.1) | 26 (48.2) | |
| 2 | 33 (31.4) | 15 (29.4) | 18 (33.3) | |
| 3 | 3 (2.9) | 1 (2) | 2 (3.7) | |
| 4 | 1 (1) | 0 (0) | 1 (1.9) | |
| Non-CS length, mm | 26.7 ± 8.6 | 25 ± 8.2 | 28.02 ± 8.7 | 0.17 |
| Non-CS diameter, mm | 3.45 ± 0.8 | 3.37 ± 0.6 | 3.5 ± 0.9 | 0.58 |
| Non-CS deployment max. pressure, atm. | 14.8 ± 2.9 | 13.7 ± 2.6 | 15.5 ± 2.9 | 0.01 |
| Balloon predilatation | 89 (84.8) | 41 (80.4) | 48 (88.9) | 0.23 |
| Balloon predilatation max. pressure, atm | 15.3 ± 4.6 | 13.6 ± 3.4 | 17.1 ± 5.1 | 0.003 |
| Balloon postdilatation | 36 (34.3) | 21 (41.2) | 15 (27.8) | 0.15 |
| Number of stent grafts | ||||
| 1 | 92 (86.8) | 45 (88.2) | 47 (85.5) | 0.23 |
| 2 | 12 (11.3) | 6 (11) | 6 (10.9) | |
| 3 | 2 (1.9) | 0 (0) | 2 (3.6) | |
| Stent graft length, mm | 18.9 ± 4.5 | 18.3 ± 4.6 | 19.4 ± 4.3 | 0.004 |
| Stent graft diameter, mm | 3.3 ± 0.5 | 3.2 ± 0.4 | 3.3 ± 0.54 | 0.87 |
| Pressure, atm | 15.4 ± 4.2 | 14.5 ± 3.1 | 16.1 ± 4.7 | 0.09 |
| Inflation time, s | 21.5 ± 25.9 | 20.5 ± 14.5 | 21.9 ± 29.4 | 0.84 |
| Selected Indices | Total n = 106 | GraftMaster n = 51 | Papyrus n = 55 | p-Value |
|---|---|---|---|---|
| Ellis type | ||||
| 1 | 33 (31.1) | 16 (31.4) | 17 (30.9) | 0.96 |
| 2 | 26 (24.5) | 10 (19.6) | 16 (29.1) | 0.26 |
| 3 | 47 (44.3) | 25 (49) | 22 (40) | 0.35 |
| Dissection | 27 (25.5) | 10 (19.6) | 17 (30.9) | 0.18 |
| No-reflow | 8 (7.6) | 4 (7.8) | 4 (7.3) | 1 |
| TIMI 3 after PCI | 89 (84) | 45 (88.2) | 44 (80) | 0.25 |
| TIMI 0 after PCI | 5 (4.7) | 2 (3.9) | 3 (5.4) | 1 |
| Glycoprotein IIb/IIIa inhibitor | 9 (8.6) | 4 (8) | 5 (9.1) | 1 |
| IABP/LVAD | 5 (4.8) | 2 (3.9) | 3 (5.7) | 1 |
| Protamine sulphate administration | 18 (17) | 1 (2) | 17 (30.9) | <0.001 |
| Prolonged balloon dilatation | 37 (34.9) | 16 (31.4) | 21 (38.2) | 0.46 |
| Transcatheter fat embolization | 1 (0.9) | 0 (0) | 1 (1.8) | 1 |
| Non-CS implantation to seal rupture | 98 (92.5) | 48 (94.1) | 50 (90.9) | 0.72 |
| Tamponade–echo | 44 (41.5) | 27 (52.9) | 17 (30.9) | 0.02 |
| Pericardiocentesis | 43 (40.6) | 25 (49) | 18 (32.7) | 0.09 |
| Emergency cardiac surgery | 12 (11.3) | 8 (15.7) | 4 (7.3) | 0.17 |
| Cardiogenic shock | 28 (26.4) | 14 (27.5) | 14 (25.5) | 0.81 |
| Periprocedural death | 8 (7.6) | 3 (5.9) | 5 (9.1) | 0.72 |
| Urgency blood transfusion | 19 (17.9) | 9 (17.7) | 10 (18.2) | 0.94 |
| Periprocedural cardiac arrest | 18 (17) | 9 (17.7) | 9 (16.4) | 0.86 |
| Length of DAPT (months) | ||||
| - 0 | 2 (2.3) | 1 (2.1) | 1 (2.4) | 0.006 |
| - 1 | 4 (4.5) | 1 (2.1) | 3 (7.1) | |
| - 6 | 9 (10.1) | 0 (0) | 9 (21.4) | |
| - 12 | 74 (83.2) | 45 (95.7) | 29 (69.1) |
| Selected Indices | Total n = 106 | 30 Days | 365 Days | ||||
|---|---|---|---|---|---|---|---|
| GraftMaster n = 51 | Papyrus n = 55 | p-Value | GraftMaster n = 51 | Papyrus n = 55 | p-Value | ||
| Re-PCI | 22 (20.7) | 7 (13.70 | 3 (5.4) | 0.19 | 11 (21.6) | 11 (20) | 0.84 |
| TVR | 18 (17) | 9 (17.6) | 2 (3.6) | 0.02 | 12 (23.5) | 6 (10.9) | 0.08 |
| TLR | 16 (15.1) | 9 (17.6) | 2 (3.6) | 0.02 | 11 (21.6) | 5 (9.1) | 0.07 |
| Cardiac death | 15 (14.1) | 4 (7.8) | 10 (18.2) | 0.11 | 4 (7.8) | 11 (20) | 0.07 |
| Myocardial infarction | 9 (8.5) | 4 (7.8) | 1 (1.8) | 0.19 | 7 (13.7) | 2 (3.6) | 0.08 |
| MACE | 33 (31.1) | 13 (25.5) | 11 (20) | 0.5 | 17 (33.3) | 16 (29.1) | 0.63 |
| Stent Thrombosis | |||||||
| Acute | 4 (3.8) | 3 (5.9) | 1 (1.8) | 0.34 | - | - | - |
| Subacute | 1 (0.9) | 1 (2) | 0 (0) | 0.48 | - | - | - |
| Late | 1 (0.9) | - | - | - | 1 (2) | 0 (0) | 0.48 |
| Overall | 6 (5.7) | - | - | - | 5 (9.8) | 1 (1.8) | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartuś, J.; Januszek, R.; Hudziak, D.; Kołodziejczak, M.; Kuźma, Ł.; Tajstra, M.; Figatowski, T.; Pawłowski, T.; Gruz-Kwapisz, M.; Smolarek-Nicpoń, M.; et al. Clinical Outcomes following Large Vessel Coronary Artery Perforation Treated with Covered Stent Implantation: Comparison between Polytetrafluoroethylene- and Polyurethane-Covered Stents (CRACK-II Registry). J. Clin. Med. 2021, 10, 5441. https://doi.org/10.3390/jcm10225441
Bartuś J, Januszek R, Hudziak D, Kołodziejczak M, Kuźma Ł, Tajstra M, Figatowski T, Pawłowski T, Gruz-Kwapisz M, Smolarek-Nicpoń M, et al. Clinical Outcomes following Large Vessel Coronary Artery Perforation Treated with Covered Stent Implantation: Comparison between Polytetrafluoroethylene- and Polyurethane-Covered Stents (CRACK-II Registry). Journal of Clinical Medicine. 2021; 10(22):5441. https://doi.org/10.3390/jcm10225441
Chicago/Turabian StyleBartuś, Jerzy, Rafał Januszek, Damian Hudziak, Michalina Kołodziejczak, Łukasz Kuźma, Mateusz Tajstra, Tomasz Figatowski, Tomasz Pawłowski, Monika Gruz-Kwapisz, Malwina Smolarek-Nicpoń, and et al. 2021. "Clinical Outcomes following Large Vessel Coronary Artery Perforation Treated with Covered Stent Implantation: Comparison between Polytetrafluoroethylene- and Polyurethane-Covered Stents (CRACK-II Registry)" Journal of Clinical Medicine 10, no. 22: 5441. https://doi.org/10.3390/jcm10225441
APA StyleBartuś, J., Januszek, R., Hudziak, D., Kołodziejczak, M., Kuźma, Ł., Tajstra, M., Figatowski, T., Pawłowski, T., Gruz-Kwapisz, M., Smolarek-Nicpoń, M., Skoczyńska, A., Tomasiewicz, B., Włodarczak, A., Kulczycki, J., Plens, K., Jaguszewski, M., Dobrzycki, S., Ochała, A., Gąsior, M., ... Wańha, W. (2021). Clinical Outcomes following Large Vessel Coronary Artery Perforation Treated with Covered Stent Implantation: Comparison between Polytetrafluoroethylene- and Polyurethane-Covered Stents (CRACK-II Registry). Journal of Clinical Medicine, 10(22), 5441. https://doi.org/10.3390/jcm10225441