
Association between Oral Health Status and Relative Handgrip Strength in 11,337 Korean

Abstract
:1. Introduction
2. Materials and Methods
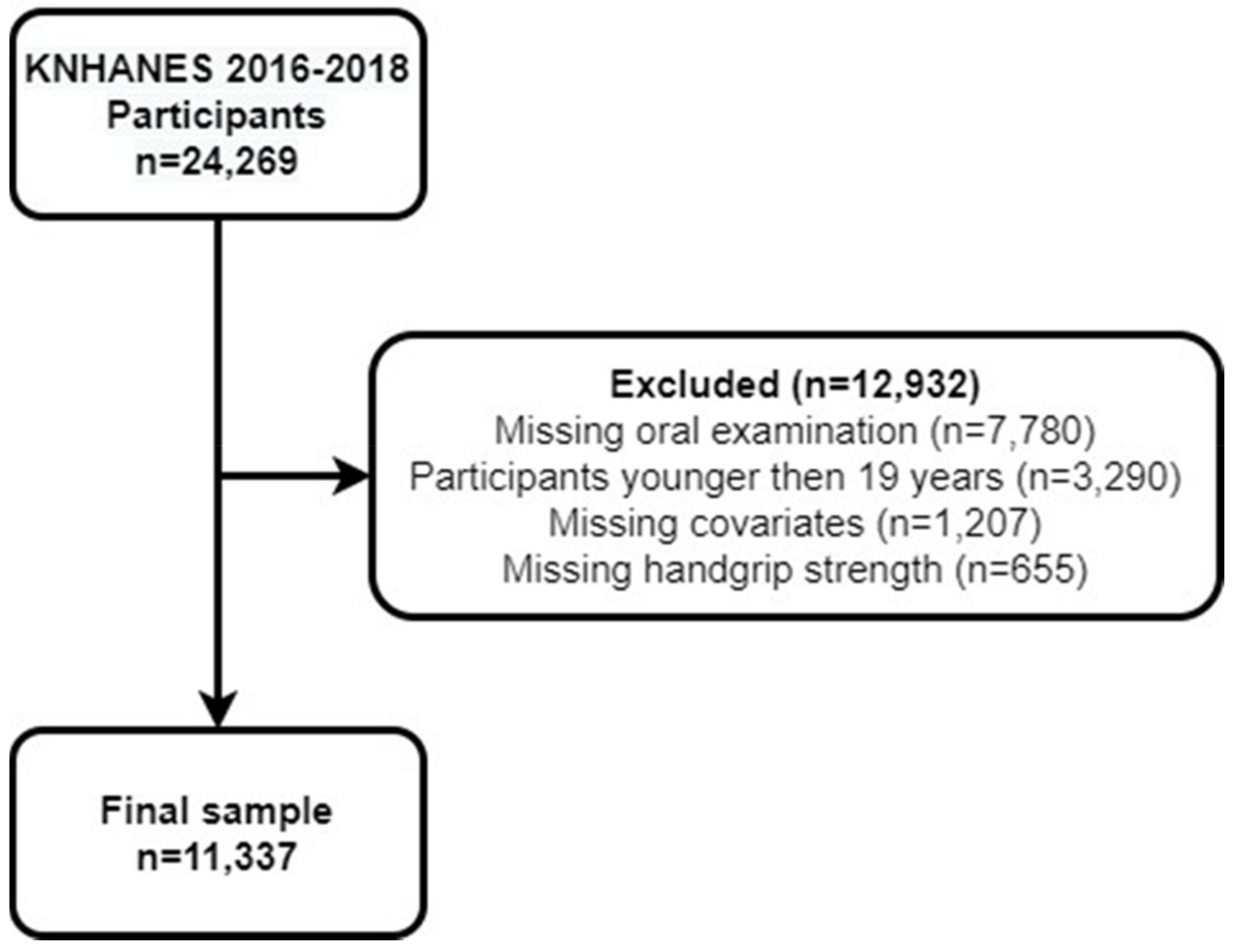
2.1. Study Population
2.2. Handgrip Strength
2.3. Oral Examination
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. General Characteristics of the Participants
3.2. Association between PT and Relative Handgrip Strength as a Continuous Variable
3.3. Association between Oral Health Status and Low Relative Handgrip Strength among the Subjects with Handgrip Strength Below the Lower Quartile (Lower 25%)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rizzoli, R.; Reginster, J.-Y.; Arnal, J.-F.; Bautmans, I.; Beaudart, C.; Bischoff-Ferrari, H.; Biver, E.; Boonen, S.; Brandi, M.-L.; Chines, A. Quality of life in sarcopenia and frailty. Calcif. Tissue Int. 2013, 93, 101–120. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alley, D.E.; Shardell, M.D.; Peters, K.W.; McLean, R.R.; Dam, T.-T.L.; Kenny, A.M.; Fragala, M.S.; Harris, T.B.; Kiel, D.P.; Guralnik, J.M. Grip strength cutpoints for the identification of clinically relevant weakness. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Choquette, S.; Bouchard, D.; Doyon, C.; Sénéchal, M.; Brochu, M.; Dionne, I.J. Relative strength as a determinant of mobility in elders 67–84 years of age. a nuage study: Nutrition as a determinant of successful aging. J. Nutr. Health Aging 2010, 14, 190–195. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Lawman, H.G.; Troiano, R.P.; Perna, F.M.; Wang, C.-Y.; Fryar, C.D.; Ogden, C.L. Associations of relative handgrip strength and cardiovascular disease biomarkers in US adults, 2011–2012. Am. J. Prev. Med. 2016, 50, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Yi, D.; Khang, A.R.; Lee, H.W.; Son, S.M.; Kang, Y.H. Relative handgrip strength as a marker of metabolic syndrome: The Korea National Health and Nutrition Examination Survey (KNHANES) VI (2014–2015). Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 227. [Google Scholar] [CrossRef] [Green Version]
- Manda, C.M.; Hokimoto, T.; Okura, T.; Isoda, H.; Shimano, H.; Wagatsuma, Y. Handgrip strength predicts new prediabetes cases among adults: A prospective cohort study. Prev. Med. Rep. 2020, 17, 101056. [Google Scholar] [CrossRef]
- Bramantoro, T.; Hariyani, N.; Setyowati, D.; Purwanto, B.; Zulfiana, A.A.; Irmalia, W.R. The impact of oral health on physical fitness: A systematic review. Heliyon 2020, 6, e03774. [Google Scholar] [CrossRef]
- Li, P.; He, L.; Sha, Y.q.; Luan, Q.x. Relationship of metabolic syndrome to chronic periodontitis. J. Periodontol. 2009, 80, 541–549. [Google Scholar] [CrossRef]
- Falcao, A.; Bullón, P. A review of the influence of periodontal treatment in systemic diseases. Periodontology 2000 2019, 79, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.C.; Yang, Y.H.; Ho, P.S.; Lee, I.C. Chewing ability, nutritional status and quality of life. J. Oral Rehabil. 2014, 41, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Elias, A.; Sheiham, A. The relationship between satisfaction with mouth and number and position of teeth. J. Oral Rehabil. 1998, 25, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Yamaga, T.; Yoshihara, A.; Ando, Y.; Yoshitake, Y.; Kimura, Y.; Shimada, M.; Nishimuta, M.; Miyazaki, H. Relationship between dental occlusion and physical fitness in an elderly population. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2002, 57, M616–M620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamdem, B.; Seematter-Bagnoud, L.; Botrugno, F.; Santos-Eggimann, B. Relationship between oral health and Fried’s frailty criteria in community-dwelling older persons. BMC Geriatr. 2017, 17, 174. [Google Scholar] [CrossRef] [Green Version]
- Hämäläinen, P.; Rantanen, T.; Keskinen, M.; Meurman, J.H. Oral health status and change in handgrip strength over a 5-year period in 80-year-old people. Gerodontology 2004, 21, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Lamster, I.B.; Asadourian, L.; Del Carmen, T.; Friedman, P.K. The aging mouth: Differentiating normal aging from disease. Periodontology 2000 2016, 72, 96–107. [Google Scholar] [CrossRef]
- Shin, H.S. Handgrip strength and the number of teeth among Korean population. J. Periodontol. 2019, 90, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Eremenko, M.; Pink, C.; Biffar, R.; Schmidt, C.O.; Ittermann, T.; Kocher, T.; Meisel, P. Cross-sectional association between physical strength, obesity, periodontitis and number of teeth in a general population. J. Clin. Periodontol. 2016, 43, 401–407. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency. Guidelines for the 7th National Health and Nutrition Examination Survey (2016–2018). Available online: https://knhanes.kdca.go.kr/knhanes/sub04/sub04_02_02.do?classType=4 (accessed on 23 September 2021).
- Li, D.; Guo, G.; Xia, L.; Yang, X.; Zhang, B.; Liu, F.; Ma, J.; Hu, Z.; Li, Y.; Li, W. Relative handgrip strength is inversely associated with metabolic profile and metabolic disease in the general population in China. Front. Physiol. 2018, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Woo, G.-J.; Lee, H.-R.; Kim, Y.; Kim, H.-J.; Park, D.-Y.; Kim, J.-B.; Oh, K.-W.; Choi, Y.-H. Data resource profile: Oral examination of the Korea National Health and Nutrition Examination Survey. J. Korean Acad. Oral Health 2018, 42, 101–108. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Oral Health Surveys: Basic Methods; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- McLean, R.R.; Shardell, M.D.; Alley, D.E.; Cawthon, P.M.; Fragala, M.S.; Harris, T.B.; Kenny, A.M.; Peters, K.W.; Ferrucci, L.; Guralnik, J.M. Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: The foundation for the National Institutes of Health (FNIH) sarcopenia project. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 576–583. [Google Scholar] [CrossRef]
- Rantanen, T.; Guralnik, J.M.; Foley, D.; Masaki, K.; Leveille, S.; Curb, J.D.; White, L. Midlife hand grip strength as a predictor of old age disability. JAMA 1999, 281, 558–560. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Gu, Y.; Zhang, Q.; Liu, L.; Wu, H.; Meng, G.; Bao, X.; Zhang, S.; Sun, S.; Wang, X. Association between tooth loss and handgrip strength in a general adult population. PLoS ONE 2020, 15, e0236010. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.; Tsakos, G.; Barbato, P.R.; Silva, D.A.; Peres, K.G. Tooth loss is associated with increased blood pressure in adults–a multidisciplinary population-based study. J. Clin. Periodontol. 2012, 39, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Pang, Z.; Zhang, D.; Jiang, W.; Wang, S.; Li, S.; Kruse, T.A.; Christensen, K.; Tan, Q. A cross-sectional analysis of age and sex patterns in grip strength, tooth loss, near vision and hearing levels in Chinese aged 50–74 years. Arch. Gerontol. Geriatr. 2012, 54, e213–e220. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.; Lee, Y. Association between oral health status and handgrip strength in older Korean adults. Eur. Geriatr. Med. 2020, 11, 459–464. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Tohara, H.; Hara, K.; Nakane, A.; Kajisa, E.; Yoshimi, K.; Minakuchi, S. Relationship of aging, skeletal muscle mass, and tooth loss with masseter muscle thickness. BMC Geriatr. 2018, 18, 67. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, Y.; Kamiyama, A.; Harikae, N.; Suzuki, M. Relationships among masticatory ability, handgrip strength, and dietary habits in subjects ranging in age from children to elderlies. J. Jpn. Soc. Mastication Sci. Health Promot. 2005, 15, 2–10. [Google Scholar]
- Park, S.; Chae, M.; Park, H.; Park, K. Higher Branched-Chain Amino Acid Intake Is Associated with Handgrip Strength among Korean Older Adults. Nutrients 2021, 13, 1522. [Google Scholar] [CrossRef]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-α with muscle mass and muscle strength in elderly men and women: The Health ABC Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Variables | Total (n = 11,337) | High Relative Handgrip Strength (n = 8846) | Low Relative Handgrip Strength (n = 2491) | p-Value |
|---|---|---|---|---|
| General characteristics | ||||
| Age | 49.81 ± 0.31 | 47.05 ± 0.28 | 59.67 ± 0.52 | <0.0001 a |
| 19–39 | 3399 (29.98) | 3008 (34.00) | 391 (15.70) | <0.0001 |
| 40–64 | 5426 (47.86) | 4570 (51.66) | 856 (34.36) | |
| ≥65 | 2512 (22.16) | 1268 (14.33) | 1244 (49.94) | |
| Educational level | ||||
| Primary | 2036 (17.96) | 1046 (11.82) | 990 (39.74) | <0.0001 |
| Middle | 1083 (9.55) | 778 (8.79) | 305 (12.24) | |
| High | 3742 (33.01) | 3121 (35.28) | 621 (24.93) | |
| College + | 4476 (39.48) | 3901 (44.10) | 575 (23.08) | |
| Household income | ||||
| Lowest quartile | 1964 (17.32) | 1125 (12.72) | 839 (33.68) | <0.0001 |
| Lower middle quartile | 2740 (24.17) | 2084 (23.56) | 656 (26.33) | |
| Upper middle quartile | 3241 (28.59) | 2690 (30.41) | 551 (22.12) | |
| Highest quartile | 3392 (29.92) | 2947 (33.31) | 445 (17.86) | |
| General health behaviors | ||||
| Smoking | ||||
| Nonsmoker | 6912 (60.97) | 5266 (59.53) | 1646 (66.08) | <0.0001 |
| Former smoker | 2395 (21.13) | 1853 (20.95) | 542 (21.76) | |
| Current smoker | 2030 (17.91) | 1727 (19.52) | 303 (12.16) | |
| Alcohol consumption | ||||
| Nondrinker | 2979 (26.28) | 1946 (22.00) | 1033 (41.47) | <0.0001 |
| Once per month | 3233 (28.52) | 2572 (29.08) | 661 (26.54) | |
| ≥Twice per month | 5125 (45.21) | 4328 (48.93) | 797 (32.00) | |
| Exercise | ||||
| No | 6377 (56.25) | 4720 (53.36) | 1657 (66.52) | <0.0001 |
| Yes | 4960 (43.75) | 4126 (46.64) | 834 (33.48) | |
| BMI (kg/m2) | ||||
| <18.5 | 426 (3.76) | 399 (4.51) | 27 (1.08) | <0.0001 |
| 18.5 to <25 | 6989 (61.65) | 5974 (67.53) | 1015 (40.75) | |
| ≥25 | 3922 (34.59) | 2473 (27.96) | 1449 (58.17) | |
| Comorbidity | ||||
| 0 | 7431 (65.55) | 6421 (72.59) | 1010 (40.55) | <0.0001 |
| 1 | 2402 (21.19) | 1686 (19.06) | 716 (28.74) | |
| ≥2 | 1504 (13.27) | 739 (8.35) | 765 (30.71) | |
| Oral health behaviors | ||||
| Frequency of brushing teeth per day | ||||
| ≤1 | 1086 (9.58) | 672 (7.60) | 414 (16.62) | <0.0001 |
| 2 | 4365 (38.50) | 3321 (37.54) | 1044 (41.91) | |
| ≥3 | 5886 (51.92) | 4853 (54.86) | 1033 (41.47) | |
| Use of oral hygiene products | ||||
| 0 | 5156 (45.48) | 3697 (41.79) | 1459 (58.57) | <0.0001 |
| 1 | 3975 (35.06) | 3250 (36.74) | 725 (29.10) | |
| ≥2 | 2206 (19.46) | 1899 (21.47) | 307 (12.32) | |
| Chewing problem | ||||
| Comfortable | 8940 (78.86) | 7267 (82.15) | 1673 (67.16) | <0.0001 |
| Uncomfortable | 2397 (21.14) | 1579 (17.85) | 818 (32.84) | |
| Speaking problem | ||||
| Comfortable | 10,533 (92.91) | 8405 (95.01) | 2128 (85.43) | <0.0001 |
| Uncomfortable | 804 (7.09) | 441 (4.99) | 363 (14.57) | |
| Dental visits during the past year | ||||
| No | 7165 (63.20) | 5395 (60.99) | 1770 (71.06) | <0.0001 |
| Yes | 4172 (36.80) | 3451 (39.01) | 721 (28.94) | |
| Self-perceived oral health status | ||||
| Good | 7033 (62.04) | 5704 (64.48) | 1329 (53.35) | <0.0001 |
| Poor | 4304 (37.96) | 3142 (35.52) | 1162 (46.65) | |
| Oral health status | ||||
| PT | 24.84 ± 0.08 | 25.51 ± 0.07 | 22.41 ± 0.19 | <0.0001 a |
| 0–9 | 437 (3.85) | 212 (2.40) | 225 (9.03) | <0.0001 |
| 10–19 | 940 (8.29) | 525 (5.93) | 415 (16.66) | |
| 20–28 | 9960 (87.85) | 8109 (91.67) | 1851 (74.31) | |
| Periodontitis | ||||
| No | 7849 (69.23) | 6338 (71.65) | 1511 (60.66) | <0.0001 |
| Yes | 3488 (30.77) | 2508 (28.35) | 980 (39.34) | |
| Relative handgrip strength (kgBMI) | 1.29 ± 0.01 | 1.40 ± 0.00 | 0.88 ± 0.01 | <0.0001 a |
| Independent Variables | Crude | Adjusted | ||
|---|---|---|---|---|
| β | p-Value | β | p-Value | |
| PT (continuous) | 0.014 | <0.0001 | 0.003 | <0.0001 |
| PT (categorical) | ||||
| 0~9 | −0.183 | <0.0001 | −0.040 | 0.0056 |
| 10~19 | −0.179 | <0.0001 | −0.038 | 0.0006 |
| 20~28 | Ref. | |||
| Independent Variables | Crude | Adjusted |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| Periodontitis | ||
| Yes | 1.69 (1.51–1.89) | 1.02 (0.89–1.16) |
| No | 1 | 1 |
| PT (continuous) | 0.91 (0.90–0.92) | 0.97 (0.96–0.99) |
| PT (categorical) | ||
| 0~9 | 4.33 (3.45–5.44) | 1.29 (1.00–1.67) |
| 10~19 | 3.41 (2.83–4.10) | 1.34 (1.10–1.62) |
| 20 ~ 28 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-E.; Kim, N.-Y.; Choi, C.-H.; Chung, K.-H. Association between Oral Health Status and Relative Handgrip Strength in 11,337 Korean. J. Clin. Med. 2021, 10, 5425. https://doi.org/10.3390/jcm10225425
Kim J-E, Kim N-Y, Choi C-H, Chung K-H. Association between Oral Health Status and Relative Handgrip Strength in 11,337 Korean. Journal of Clinical Medicine. 2021; 10(22):5425. https://doi.org/10.3390/jcm10225425
Chicago/Turabian StyleKim, Ji-Eun, Na-Yeong Kim, Choong-Ho Choi, and Ki-Ho Chung. 2021. "Association between Oral Health Status and Relative Handgrip Strength in 11,337 Korean" Journal of Clinical Medicine 10, no. 22: 5425. https://doi.org/10.3390/jcm10225425
APA StyleKim, J.-E., Kim, N.-Y., Choi, C.-H., & Chung, K.-H. (2021). Association between Oral Health Status and Relative Handgrip Strength in 11,337 Korean. Journal of Clinical Medicine, 10(22), 5425. https://doi.org/10.3390/jcm10225425