
The Use of Chitotriosidase as a Marker of Active Sarcoidosis and in the Diagnosis of Fever of Unknown Origin (FUO)


 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population and Study Protocol
2.2. Diagnosis and Measurements
2.3. Patient Stratification
2.3.1. Active Sarcoidosis Patients
2.3.2. FUO Patients
2.3.3. Inactive/Remitted Sarcoidosis Patients
2.3.4. Laboratory Measurements
2.3.5. Statistical Analysis
2.3.6. Sample Size
3. Results
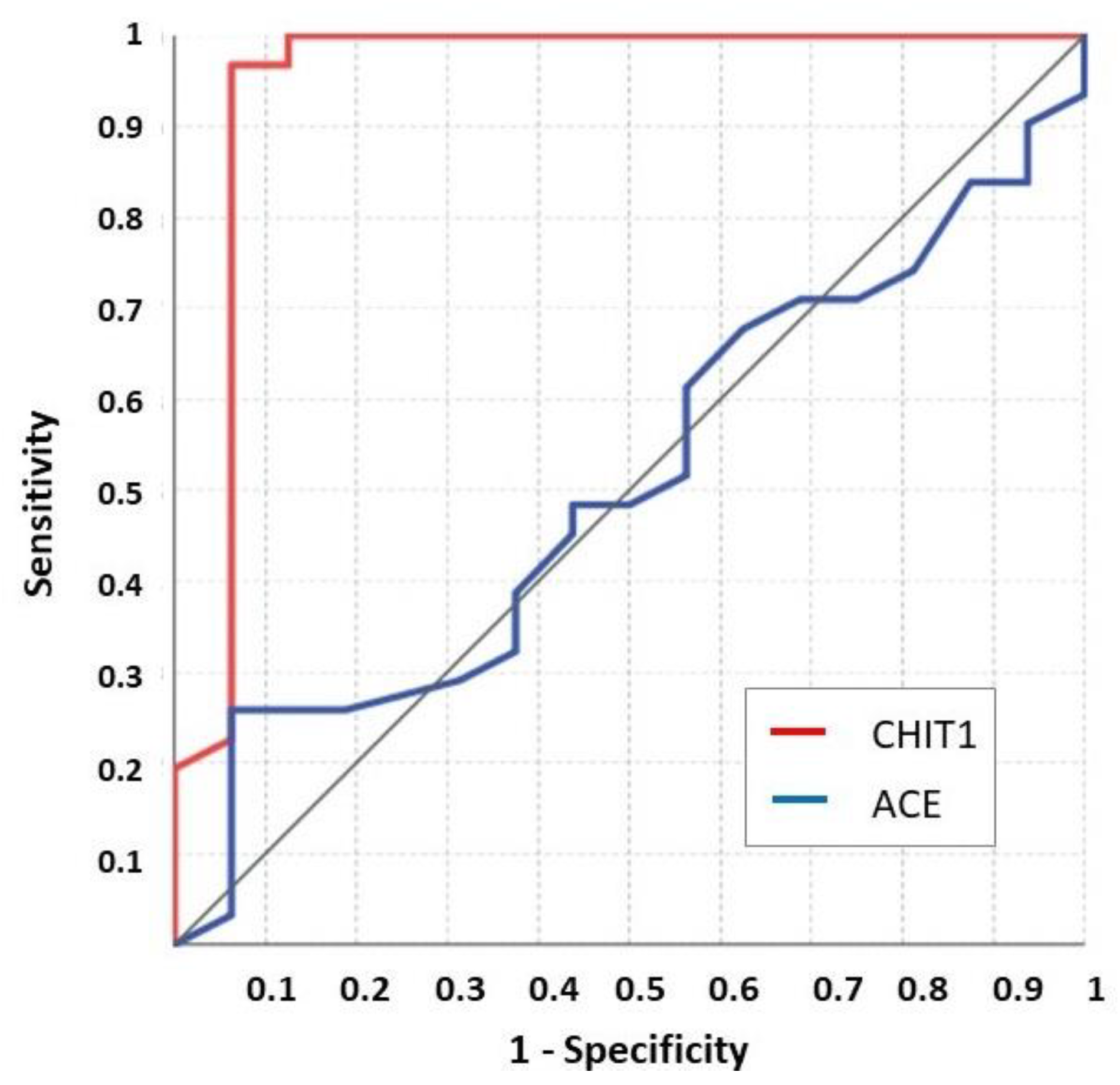
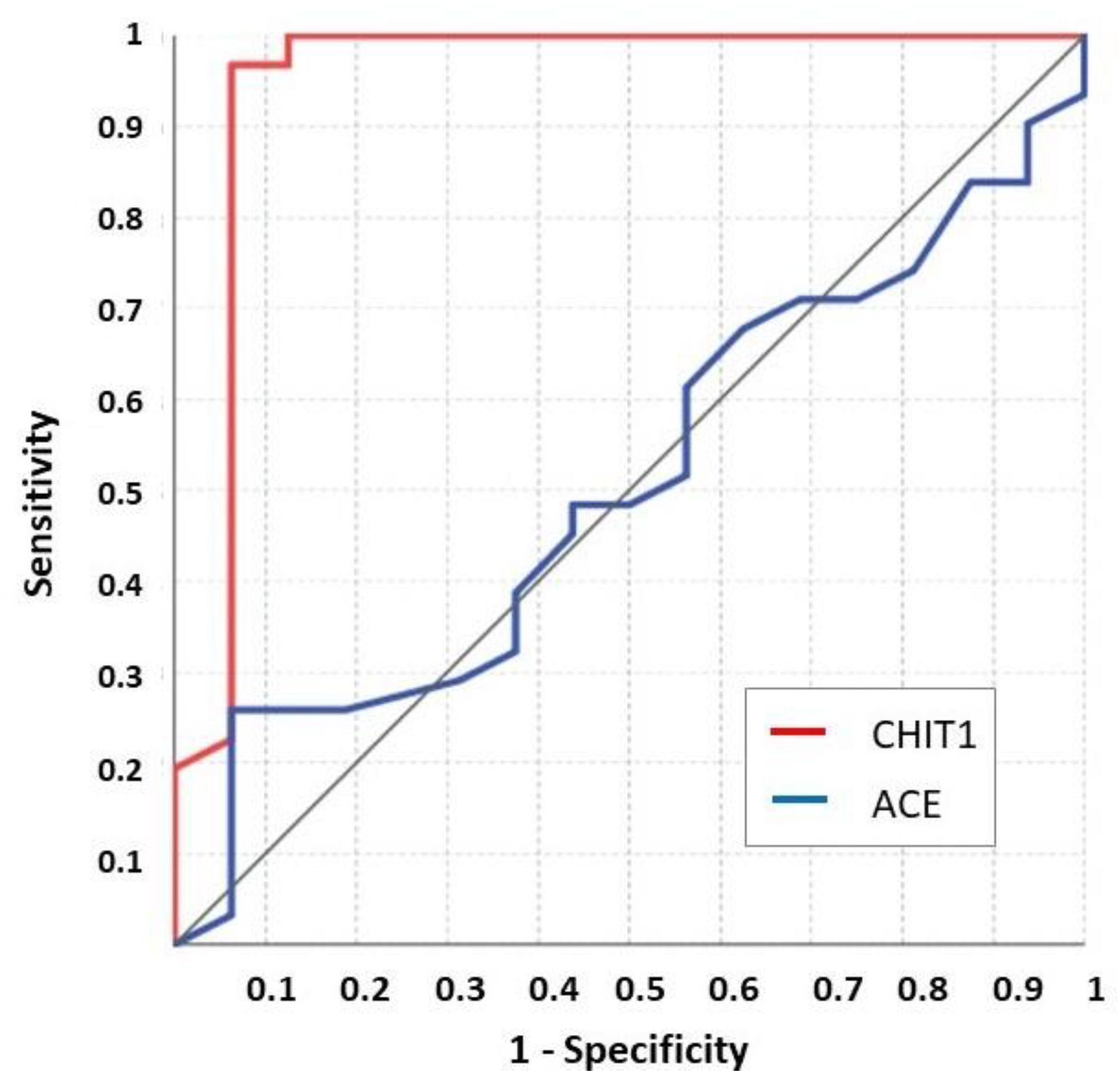
3.1. Active Sarcoidosis versus FUO Patients
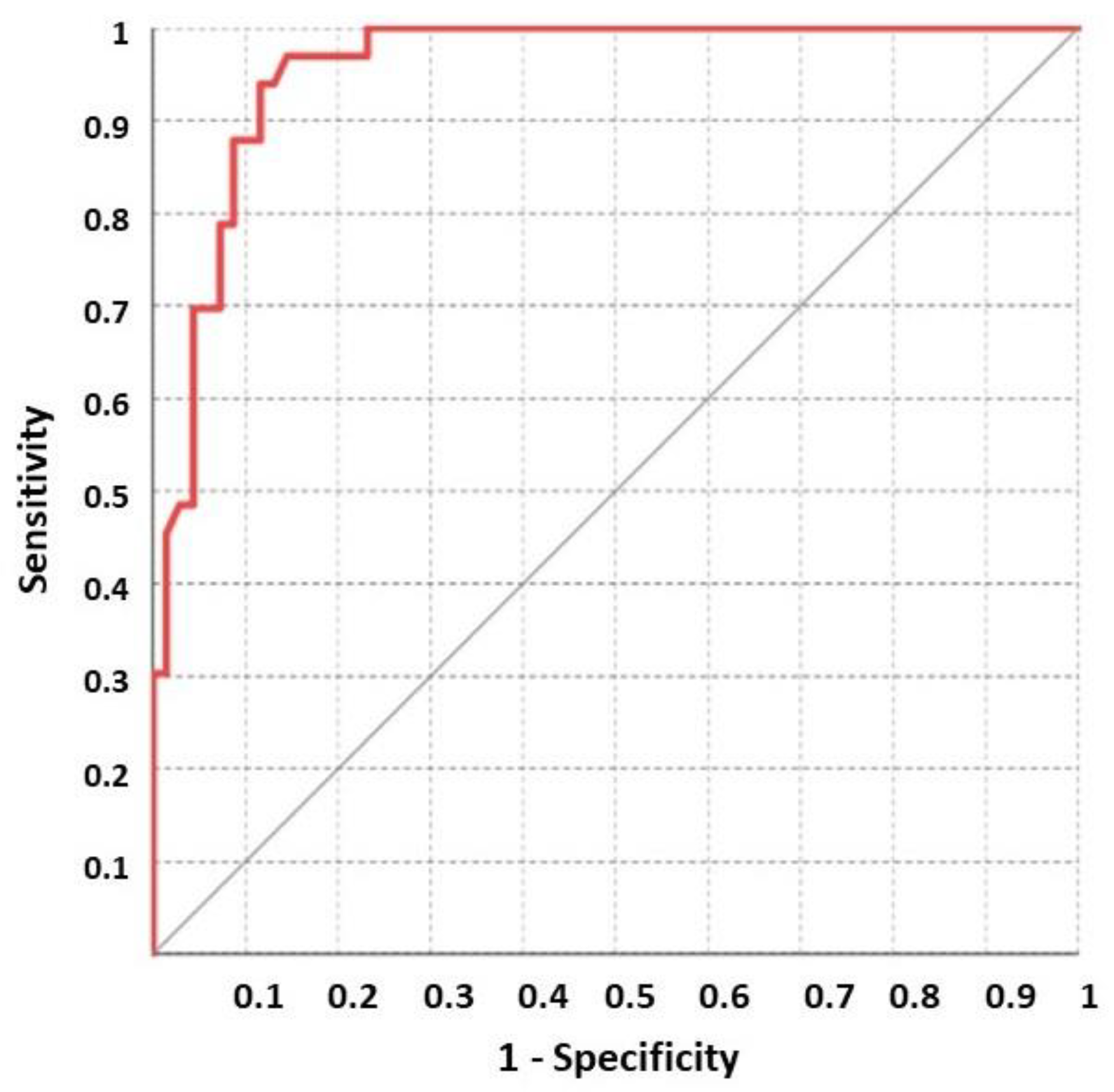
3.2. Active versus Inactive Sarcoidosis Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE | angiotensin-converting enzyme |
| ACEIs | angiotensin-converting enzyme inhibitors |
| AUROC | area under the receiver operating characteristics |
| CHIT1 | chitotriosidase or chitinase-1 |
| FUO | fever of unknown origin |
| N.D. | not determined. |
| n.v. | normal value |
References
- Petersdorf, R.G.; Beeson, P.B. Fever of unexplained origin: Report on 100 cases. Medicine 1961, 40, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Durack, D.T.; Street, A.C. Fever of unknown origin--reexamined and redefined. Curr. Clin. Top. Infect. Dis. 1991, 11, 1651090. [Google Scholar]
- Telenti, A.; Hermans, P.E. Idiopathic Granulomatosis Manifesting as Fever of Unknown Origin. Mayo Clin. Proc. 1989, 64, 44–50. [Google Scholar] [CrossRef]
- Grunewald, J.; Grutters, J.C.; Arkema, E.V.; Saketkoo, L.A.; Moller, D.R.; Müller-Quernheim, J. Sarcoidosis. Nat. Rev. Dis. Prim. 2019, 5, 45. [Google Scholar] [CrossRef]
- Lee, G.M.; Pope, K.; Meek, L.; Chung, J.H.; Hobbs, S.B.; Walker, C.M. Sarcoidosis: A Diagnosis of Exclusion. Am. J. Roentgenol. 2020, 214, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Eurelings, L.E.M.; Miedema, J.R.; Dalm, V.A.S.H.; Van Daele, P.L.A.; Van Hagen, P.M.; Van Laar, J.A.M.; Dik, W.A. Sensitivity and specificity of serum soluble interleukin-2 receptor for diagnosing sarcoidosis in a population of patients suspected of sarcoidosis. PLoS ONE 2019, 14, e0223897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groen-Hakan, F.; Eurelings, L.; Berge, J.C.T.; Van Laar, J.; Ramakers, C.R.B.; Dik, W.A.; Rothova, A. Diagnostic Value of Serum-Soluble Interleukin 2 Receptor Levels vs Angiotensin-Converting Enzyme in Patients With Sarcoidosis-Associated Uveitis. JAMA Ophthalmol. 2017, 135, 1352–1358. [Google Scholar] [CrossRef]
- Bargagli, E.; Bennett, D.; Maggiorelli, C.; Di Sipio, P.; Margollicci, M.; Bianchi, N.; Rottoli, P. Human Chitotriosidase: A Sensitive Biomarker of Sarcoidosis. J. Clin. Immunol. 2013, 33, 264–270. [Google Scholar] [CrossRef]
- Popević, S.; Šumarac, Z.; Jovanović, D.; Babić, D.; Stjepanović, M.; Jovičić, S.; Šobić-Šaranović, D.; Filipović, S.; Gvozdenović, B.; Omčikus, M.; et al. Verifying Sarcoidosis Activity: Chitotriosidase Versus ACE in Sarcoidosis—A Case-Control Study. J. Med. Biochem. 2016, 35, 390–400. [Google Scholar] [CrossRef]
- Lopes, M.C.; Amadeu, T.P.; Ribeiro-Alves, M.; Da Costa, C.H.; Rodrigues, L.S.; Bessa, E.J.C.; Bruno, L.P.; Lopes, A.; Rufino, R. Identification of Active Sarcoidosis Using Chitotriosidase and Angiotensin-Converting Enzyme. Lung 2019, 197, 295–302. [Google Scholar] [CrossRef]
- Bennett, D.; Cameli, P.; Lanzarone, N.; Carobene, L.; Bianchi, N.; Fui, A.; Rizzi, L.; Bergantini, L.; Cillis, G.; D’Alessandro, M.; et al. Correction to: Chitotriosidase: A biomarker of activity and severity in patients with sarcoidosis. Respir. Res. 2020, 21, 34. [Google Scholar] [CrossRef] [PubMed]
- Elias, J.A.; Homer, R.; Hamid, Q.; Lee, C.G. Chitinases and chitinase-like proteins in TH2 inflammation and asthma. J. Allergy Clin. Immunol. 2005, 116, 497–500. [Google Scholar] [CrossRef]
- Park, S.K.; Cho, H.W.; Heo, K.W.; Hur, D.Y.; Lee, H.-K. Role of Acidic Mammalian Chitinase and Chitotriosidase in Nasal Polyps. Otolaryngol. Head Neck Surg. 2009, 141, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Bergantini, L.; Bianchi, F.; Cameli, P.; Mazzei, M.A.; Fui, A.; Sestini, P.; Rottoli, P.; Bargagli, E. Prognostic Biomarkers of Sarcoidosis: A Comparative Study of Serum Chitotriosidase, ACE, Lysozyme, and KL-6. Dis. Markers 2019, 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef] [PubMed]
- Manna, R.; Cauda, R.; Feriozzi, S.; Gambaro, G.; Gasbarrini, A.; Lacombe, D.; Livneh, A.; Martini, A.; Ozdogan, H.; International Panel for RAre recurrent FUO-IPRAFUO; et al. Recommendations for the inclusion of Fabry disease as a rare febrile condition in existing algorithms for fever of unknown origin. Intern. Emerg. Med. 2017, 12, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; He, W.; Boer, A.M.; Wevers, R.A.; De Bruijn, A.M.; Groener, J.E.M.; Hollak, C.E.M.; Aerts, J.M.F.G.; Galjaard, H.; Van Diggelen, O.P. Elevated plasma chitotriosidase activity in various lysosomal storage disorders. J. Inherit. Metab. Dis. 1995, 18, 717–722. [Google Scholar] [CrossRef] [Green Version]
- Kocak, N.D.; Gungor, S.; Akturk, U.A.; Yalcinsoy, M.; Kavas, M.; Oztas, S.; Akkaya, M.E.; Aksoy, E.; Agca, M.C.; Duman, D.; et al. Analysis of Age Distribution and Disease Presentation of 1269 Patients with Sarcoidosis. Eurasian J. Med. 2017, 49, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Costabel, U. Sarcoidosis: Clinical update. Eur. Respir. J Suppl. 2001, 32, 56s–68s. [Google Scholar]
- Hollak, C.E.; Van Weely, S.; Van Oers, M.H.; Aerts, J. Marked elevation of plasma chitotriosidase activity. A novel hallmark of Gaucher disease. J. Clin. Investig. 1994, 93, 1288–1292. [Google Scholar] [CrossRef] [Green Version]
- Malaguarnera, L. Chitotriosidase: The yin and yang. Cell. Mol. Life Sci. 2006, 63, 3018–3029. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Sharma, L.; Cruz, C.S.D. Chitotriosidase: A marker and modulator of lung disease. Eur. Respir. Rev. 2020, 29, 190143. [Google Scholar] [CrossRef] [PubMed]
- Elmonem, M.A.; Amin, H.S.; El-Essawy, R.A.; Mehaney, D.A.; Nabil, M.; Kamel, L.N.; Farid, I.M. Association of chitotriosidase enzyme activity and genotype with the risk of nephropathy in type 2 diabetes. Clin. Biochem. 2016, 49, 444–448. [Google Scholar] [CrossRef]
- Kanneganti, M.; Kamba, A.; Mizoguchi, E. Role of Chitotriosidase (Chitinase 1) Under Normal and Disease Conditions. J. Epithel. Biol. Pharmacol. 2012, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Renkema, H.; Boot, R.; Muijsers, A.O.; Donker-Koopman, W.E.; Aerts, J. Purification and Characterization of Human Chitotriosidase, a Novel Member of the Chitinase Family of Proteins. J. Biol. Chem. 1995, 270, 2198–2202. [Google Scholar] [CrossRef] [Green Version]
- Renkema, G.H.; Boot, R.G.; Au, F.L.; Donker-Koopman, W.E.; Strijland, A.; Muijsers, A.O.; Hrebicek, M.; Aerts, J.M.F.G. Chitotriosidase, a chitinase, and the 39-kDa human cartilage glycoprotein, a chitin-binding lectin, are homologues of family 18 glycosyl hydrolases secreted by human macrophages. JBIC J. Biol. Inorg. Chem. 1998, 251, 504–509. [Google Scholar] [CrossRef]
- Boot, R.; Renkema, H.; Verhoek, M.; Strijland, A.; Bliek, J.; de Meulemeester, T.M.A.M.O.; Mannens, M.M.A.M.; Aerts, J. The Human Chitotriosidase Gene. J. Biol. Chem. 1998, 273, 25680–25685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grace, M.E.; Balwani, M.; Nazarenko, I.; Prakash-Cheng, A.; Desnick, R.J. Type 1 Gaucher disease: Null and hypomorphic novel chitotriosidase mutations-implications for diagnosis and therapeutic monitoring. Hum. Mutat. 2007, 28, 866–873. [Google Scholar] [CrossRef]
- Cunha, B.A.; Lortholary, O.; Cunha, C. Fever of Unknown Origin: A Clinical Approach. Am. J. Med. 2015, 128, 1138.e1–1138.e15. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, S.; Steinbrech, D.S.; Landas, S.K.; Hunninghake, G.W. Amounts of Angiotensin-converting Enzyme mRNA Reflect the Burden of Granulomas in Granulomatous Lung Disease. Am. Rev. Respir. Dis. 1993, 148, 483–486. [Google Scholar] [CrossRef]
- D’Alessandro, M.; Bergantini, L.; Perrone, A.; Cameli, P.; Cameli, M.; Prasse, A.; Plataroti, D.; Sestini, P.; Bargagli, E. Serial investigation of Angiotensin-Converting Enzyme in sarcoidosis patients treated with Angiotensin-Converting Enzyme Inhibitor. Eur. J. Intern. Med. 2020, 78, 58–62. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Patient | Age (Years) | Sex | ACE (n.v. < 64 UI/L) | CHIT1 (n.v.: 4–80 nmol/mL/h) | Site of Biopsy | ExtraP. | Pulmonary Stage |
|---|---|---|---|---|---|---|---|
| 1 * | 63 | F | 309 | 218.15 | Mediastinal adenopathy | No-EP | IV |
| 2 | 84 | F | N.D. | 247.36 | Mediastinal adenopathy | No-EP | IV |
| 3 | 63 | F | 20 | 147.62 | Mediastinal adenopathy | No-EP | I |
| 4 * | 63 | F | 15 | 109.20 | Adenopathic, splenic | Splenic | I |
| 5 | 54 | F | 42 | 234.00 | Lymph node/mediastinal adenopathy | No-EP | II |
| 6 | 58 | M | 6 | 218.,56 | Liver, supraclavicular adenopathy | No-EP | III |
| 7 | 75 | F | 16 | 254.45 | Liver | Liver, bone | II |
| 8 | 61 | F | 66 | 249.44 | Submandibular adenopathy | Liver, spleen, and abdominal lymph nodes | I |
| 9 | 30 | M | 32 | 102.13 | Liver | Liver and spleen | No-P |
| 10 | 83 | F | N.D. | 213.14 | Mediastinal adenopathy | Supraclavicular adenopathies | I |
| 11 | 76 | F | 51 | 244.02 | Mediastinal adenopathy | No-EP | II |
| 12 * | 65 | F | 20 | 110.48 | Skin | Skin | I |
| 13 * | 56 | F | 34 | 150.96 | Mediastinal adenopathy | No-EP | II |
| 14 * | 74 | F | 62 | 246.00 | Mediastinal adenopathy | Skin | II |
| 15 * | 63 | F | 147 | 251.95 | Skin and mediastinal adenopathy | No-EP | I |
| 16 | 53 | F | 29 | 121.33 | Mediastinal adenopathy | No-EP | II |
| 17 | 59 | F | 31 | 210.22 | Mediastinal adenopathy | No-EP | II |
| 18 * | 76 | F | 52 | 335.68 | Groin adenopathy | No-EP | I |
| 19 | 68 | M | 3 | 207.29 | Periorbital | Orbital | I |
| 20 | 76 | F | 30 | 207.29 | Periorbital | Orbital | I |
| 21 | 64 | F | 76 | 251.95 | Abdominal adenopathy | No-EP | No-P |
| 22 | 57 | F | 26 | 268.60 | Mediastinal adenopathy | Supraclavicular adenopathies | II |
| 23 | 59 | F | 99 | 164.73 | Mediastinal adenopathy | No-EP | III |
| 24 | 48 | F | 47 | 224.40 | Mediastinal adenopathy | No-EP | I |
| 25 * | 45 | M | 28 | 145.11 | Mediastinal adenopathy | No-EP | I |
| 26 | 80 | F | 46 | 209.38 | Mediastinal adenopathy | No-EP | III |
| 27 | 61 | M | 20 | 79.18 | Mediastinal adenopathy | Abdominal | No-P |
| 28 | 50 | F | 10 | 224.40 | Mediastinal adenopathy | Systemic adenopathies | I |
| 29* | 49 | F | 46 | 180.59 | Laterocervical adenopathy | Systemic adenopathies | I |
| 30 | 79 | F | 93 | 210.20 | Axillary adenopathy | Systemic adenopathies | II |
| 31 * | 64 | F | 29 | 221.07 | Mediastinal adenopathy | No-EP | I |
| 32 * | 63 | F | 72 | 226.07 | Laterocervical adenopathy | Systemic adenopathies | I |
| 33 | 59 | F | 79 | 202.29 | Mediastinal adenopathy | No-EP | II |
| Patient | Sex | Age (Years) | Diagnosis | CHIT1 at Diagnosis (n.v.: 4–80 nmol/mL/h) |
|---|---|---|---|---|
| 34 | F | 26 | Fucosidosis | 2.31 |
| 35 | M | 75 | Lung cancer (adenocarcinoma) | 19.36 |
| 36 | F | 22 | Recurrent fevers | 25.76 |
| 37 | F | 45 | Autoinflammatory disease | 1.20 |
| 38 | F | 40 | Dystermia | 57.06 |
| 39 | M | 60 | Recurrent fever with splenomegaly and erythema nodosum | 67.08 |
| 40 | M | 67 | Aortic stenosis | 57.06 |
| 41 | F | 22 | PFAPA | 82.09 |
| 42 | F | 37 | Suspected vasculitis | 47.88 |
| 43 | M | 27 | Granulomatosis with polyangitis disease | 102.13 |
| 44 | M | 17 | Still’s disease | 33.70 |
| 45 | M | 44 | Fabry disease | 4.77 |
| 46 | F | 48 | Behçet disease | 31.60 |
| 47 | F | 63 | Undifferentiated connectivitis in family idiopathic lymphedema | 192.27 |
| 48 | F | 63 | Recurrent peritonitis evolved into mesothelioma | 19.08 |
| 49 | F | 37 | Periodic fevers | 27.01 |
| 50 | F | 45 | Crohn’s disease | 87.94 |
| 51 | M | 57 | Fabry disease | 58.73 |
| 52 | F | 50 | Autoinflammatory disease | 231.50 |
| 53 | M | 33 | Suspected hereditary angioedema | 4.65 |
| 54 | F | 21 | Autoinflammatory disease | 65.82 |
| 55 | F | 23 | Hypertrophic heart disease | 37.86 |
| 56 | M | 62 | Hypertrophic heart disease | 5.12 |
| 57 | M | 61 | Renal insufficiency | 4.08 |
| 58 | M | 36 | Mitochondriopathy | 13.71 |
| 59 | M | 48 | Still’s disease with erythema nodosum | 90.86 |
| 60 | M | 52 | Fabry disease | 62.07 |
| 61 | F | 24 | Autoinflammatory disease | 16.16 |
| 62 | M | 73 | Large vessel vasculitis | 112.56 |
| 63 | M | 79 | BPCO | 6.16 |
| 64 | F | 52 | Fabry disease | 34.94 |
| 65 | F | 37 | FMF with erythema nodosum | 1.20 |
| 66 | F | 34 | Fever in immunodeficiency | 47.46 |
| 67 | F | 51 | Suspected Gaucher disease | 218.15 |
| 68 | M | 59 | Variable common immunodeficiency | 187.68 |
| 69 | F | 38 | Subclinical hyperthyroidism | 115.07 |
| 70 | M | 43 | Recurring fevers (Castleman disease) | 37.03 |
| 71 | M | 38 | Autoinflammatory disease | 90.45 |
| 72 | M | 48 | Lymphoma with sickle cell disease | 104.22 |
| 73 | F | 72 | Fibromyalgia | 24.93 |
| 74 | M | 75 | Bile ducts neoplasia | 15.33 |
| 75 | M | 74 | Fabry disease | 8.33 |
| 76 | M | 59 | Periodic fever NALP 12 | 15.16 |
| 77 | M | 72 | Fabry disease | 3.16 |
| 78 | M | 23 | Autoinflammatory disease | 10.32 |
| 79 | F | 24 | Undifferentiated connectivitis | 52.05 |
| 80 | F | 14 | Fibromyalgia | 10.74 |
| 81 | M | 39 | Still’s disease | 56.23 |
| 82 | M | 40 | Still’s disease | 9.84 |
| 83 | M | 57 | FMF with lung granulomatous reaction triggered by taking INF alpha | 213.97 |
| 84 | F | 70 | Suspected Fabry disease | 41.62 |
| 85 | F | 32 | Fikuchi–Fujmoto disease | 3.60 |
| 86 | M | 64 | Lymphoproliferating disease with hypogammaglobulinemia | 149.29 |
| 87 | F | 62 | Hypogammaglobulinemia | 89.62 |
| 88 | F | 80 | Periodic autoinflammatory fevers | 34.94 |
| 89 | M | 82 | FUO with hyperthyroidism | 30.35 |
| 90 | M | 45 | Hypertrophic heart disease | 13.60 |
| 91 | M | 54 | Fabry disease | 5.43 |
| 92 | F | 17 | Connectivitis with MEFV mutation | 46.63 |
| 93 | M | 27 | Fabry disease | 4.57 |
| 94 | F | 67 | Scleroderma | 38.70 |
| 95 | F | 72 | COP | 1.55 |
| 96 | M | 17 | Dystermia | 54.14 |
| 97 | F | 30 | FMF | 0.30 |
| 98 | F | 21 | Autoinflammatory disease | 82.08 |
| 99 | M | 41 | Fabry disease | 10.10 |
| 100 | M | 29 | Infection in patient under cortisone therapy | 7.46 |
| 101 | M | 47 | Leucocytoclastic vasculitis of medium-caliber vessels | 39.53 |
| 102 | M | 70 | Fabry disease | 30.35 |
| Patient | Age (Years) | Sex | ACE (n.v. < 64 UI/L) | CHIT1 (n.v.: 4–80 nmol/mL/h) | Site of Biopsy | ExtraP. | Pulmonary Stage | Treatment |
|---|---|---|---|---|---|---|---|---|
| 1 * | 63 | F | 309 | 60.61 | Mediastinal adenopathy | No-EP | IV | P |
| 103 | 52 | F | 64 | 39.53 | Skin (erythema nodosum) | Skin | I | Ib, Hy |
| 4 * | 64 | F | 19 | 43.30 | Adenopathic, splenic | Splenic | I | N.T. |
| 12 * | 65 | F | 20 | 31.19 | Skin | Skin | I | P + Chl |
| 13 * | 56 | F | 34 | 82.01 | Mediastinal adenopathy | No-EP | I | P |
| 104 | 66 | F | 10 | 30.77 | Mediastinal adenopathy | No-EP | I | N.T. |
| 14 * | 74 | F | 62 | 244.40 | Mediastinal adenopathy | Skin | II | P |
| 15 * | 67 | F | 40 | 3.53 | Skin and mediastinal adenopathy | No-EP | I | MP |
| 105 | 71 | F | N.D. | 6.76 | Abdominal adenopathy | No-EP | III | P |
| 18 * | 76 | F | N.D. | 23.00 | Groin adenopathy | No-EP | I | D |
| 106 | 66 | M | 65 | 43.14 | Mediastinal adenopathy | Liver | I | N.T. |
| 107 | 80 | F | 26 | 8.40 | Mediastinal adenopathy | No-EP | I | N.T. |
| 108 | 25 | F | 52 | 27.00 | Laterocervical adenopathy | Laterocervical adenopathy | I | N.T. |
| 109 | 67 | M | 62 | 27.40 | Mediastinal adenopathy | Systemic adenopathies | I | N.T. |
| 25 * | 45 | M | 28 | 65.40 | Mediastinal adenopathy | No-EP | I | P |
| 29 * | 49 | F | 46 | <2 | Laterocervical adenopathy | Systemic adenopathies | I | F/V |
| 110 | 74 | M | 27 | 30.40 | Lung | No-EP | I | N.T. |
| 31 * | 64 | F | 29 | 54.47 | Mediastinal adenopathy | No-EP | I | N.T. |
| 32 * | 65 | F | N.D. | 6.93 | Laterocervical adenopathy | Systemic adenopathies | I | N.T. |
| All Patients (n = 102) | Active Sarcoidosis (n = 33) | Other FUO (n = 69) | p-Value | |
|---|---|---|---|---|
| Age (years) | 58.0 (40–67) | 63.0 (56.5–74.5) | 45.0 (31.0–62.5) | <0.01 § |
| Sex (Male) | 42 (41.2) | 5 (15.2) | 37 (53.6) | <0.01 ç |
| ACE (UI/L) | / | 34.0 (26.0–62.0) | / | / |
| CHIT1 (nmol/mL/h) | 54.4 (17.6–172.6) | 213.1 (157–244.2) | 34.9 (9.9– 66.5) | <0.01 § |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Francesco, A.M.; Verrecchia, E.; Sicignano, L.L.; Massaro, M.G.; Antuzzi, D.; Covino, M.; Pasciuto, G.; Richeldi, L.; Manna, R. The Use of Chitotriosidase as a Marker of Active Sarcoidosis and in the Diagnosis of Fever of Unknown Origin (FUO). J. Clin. Med. 2021, 10, 5283. https://doi.org/10.3390/jcm10225283
Di Francesco AM, Verrecchia E, Sicignano LL, Massaro MG, Antuzzi D, Covino M, Pasciuto G, Richeldi L, Manna R. The Use of Chitotriosidase as a Marker of Active Sarcoidosis and in the Diagnosis of Fever of Unknown Origin (FUO). Journal of Clinical Medicine. 2021; 10(22):5283. https://doi.org/10.3390/jcm10225283
Chicago/Turabian StyleDi Francesco, Angela Maria, Elena Verrecchia, Ludovico Luca Sicignano, Maria Grazia Massaro, Daniela Antuzzi, Marcello Covino, Giuliana Pasciuto, Luca Richeldi, and Raffaele Manna. 2021. "The Use of Chitotriosidase as a Marker of Active Sarcoidosis and in the Diagnosis of Fever of Unknown Origin (FUO)" Journal of Clinical Medicine 10, no. 22: 5283. https://doi.org/10.3390/jcm10225283
APA StyleDi Francesco, A. M., Verrecchia, E., Sicignano, L. L., Massaro, M. G., Antuzzi, D., Covino, M., Pasciuto, G., Richeldi, L., & Manna, R. (2021). The Use of Chitotriosidase as a Marker of Active Sarcoidosis and in the Diagnosis of Fever of Unknown Origin (FUO). Journal of Clinical Medicine, 10(22), 5283. https://doi.org/10.3390/jcm10225283