
The Impact of Infectious Complications after Esophagectomy for Esophageal Cancer on Cancer Prognosis and Treatment Strategy


Abstract
:1. Introduction
2. The Effect of Postoperative Complications after Esophagectomy for Cancer on Survival
2.1. Pulmonary Complications
2.2. Anastomotic Leakage
2.3. Overall Complications
3. Clinical Significance of Proinflammatory Cytokines
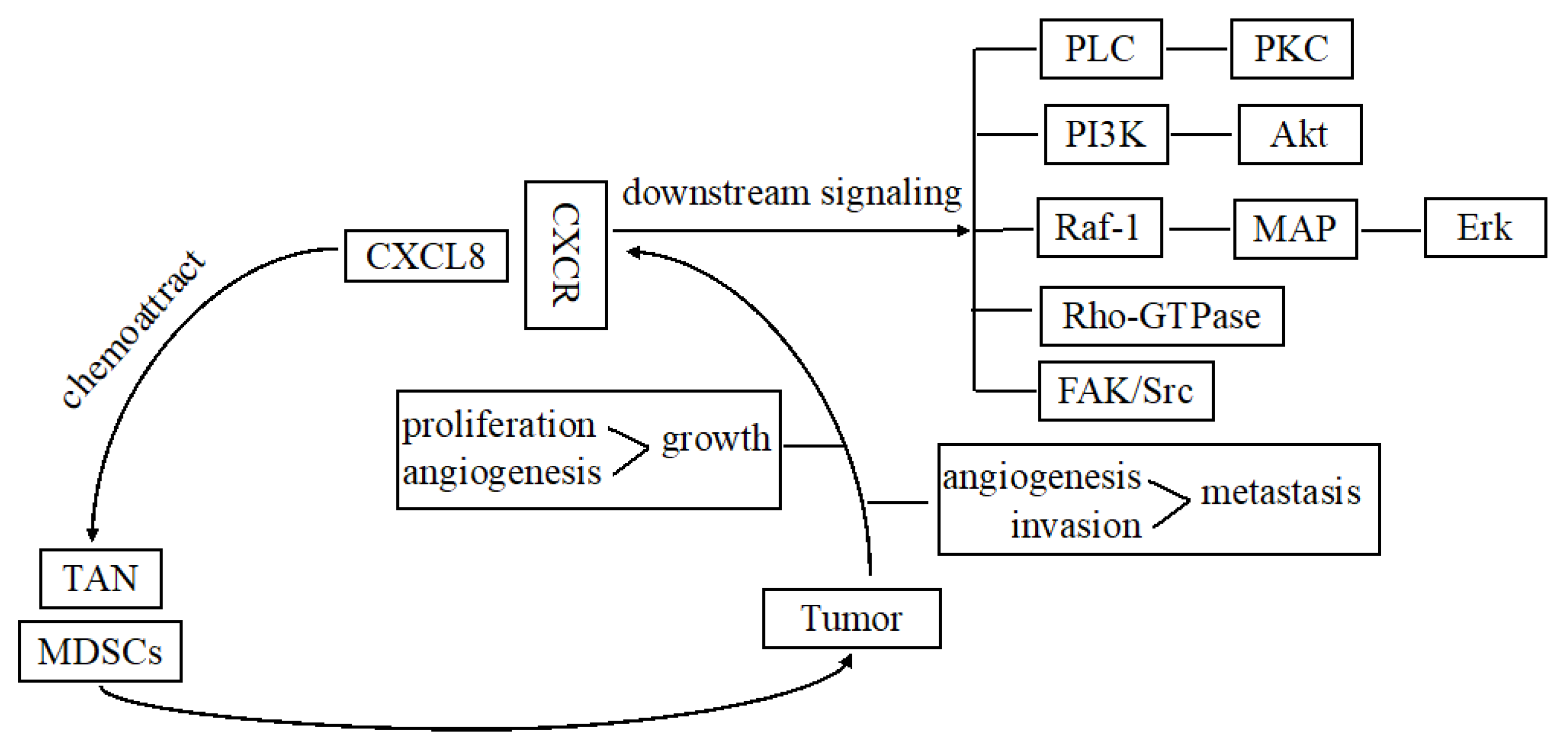
4. The Major Signaling Pathways of CXCL8 in Esophageal Cancers
5. Multidisciplinary Team Management for Prevention of Postoperative Complications after Esophagectomy
6. Introduction of Minimally Invasive Esophagectomy
7. Definitive Chemoradiotherapy
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries 2021. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Ando, N.; Ozawa, S.; Kitagawa, Y.; Shinozawa, Y.; Kitajima, M. Improvement in the results of surgical treatment of advanced squamous esophageal carcinoma during 15 consecutive years. Ann. Surg. 2000, 232, 225–232. [Google Scholar] [CrossRef]
- Cooper, J.S.; Guo, M.D.; Herskovic, A.; Macdonald, J.S.; Martenson, J.A., Jr.; Al-Sarraf, M.; Byhardt, R.; Russell, A.H.; Beitler, J.J.; Spencer, S.; et al. Chemoradiotherapy of locally advanced esophageal cancer: Long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA 1999, 281, 1623–7162. [Google Scholar] [CrossRef] [PubMed]
- Booka, E.; Takeuchi, H.; Nishi, T.; Matsuda, S.; Kaburagi, T.; Fukuda, K.; Nakamura, R.; Takahashi, T.; Wada, N.; Kawakubo, H.; et al. The Impact of Postoperative Complications on Survivals After Esophagectomy for Esophageal Cancer. Medicine 2015, 94, e1369. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Miyata, H.; Gotoh, M.; Kitagawa, Y.; Baba, H.; Kimura, W.; Tomita, N.; Nakagoe, T.; Shimada, M.; Sugihara, K.; et al. A Risk Model for Esophagectomy Using Data of 5354 Patients Included in a Japanese Nationwide Web-Based Database. Ann. Surg. 2014, 260, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, M.; Tanizawa, Y.; Bando, E.; Kawamura, T.; Terashima, M. Poor survival rate in patients with postoperative intra-abdominal infectious complications following curative gastrectomy for gastric cancer. Ann. Surg. Oncol. 2013, 20, 1575–1583. [Google Scholar] [CrossRef]
- McSorley, S.T.; Horgan, P.G.; McMillan, D.C. The impact of the type and severity of postoperative complications on long-term outcomes following surgery for colorectal cancer: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2016, 97, 168–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kataoka, K.; Takeuchi, H.; Mizusawa, J.; Igaki, H.; Ozawa, S.; Abe, T.; Nakamura, K.; Kato, K.; Ando, N.; Kitagawa, Y. Prognostic impact of postoperative morbidity after esophagectomy for esophageal cancer: Exploratory analysis of JCOG9907. Ann. Surg. 2017, 265, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.W.; Swisher, S.G.; Hofstetter, W.; Correa, A.M.; Mehran, R.J.; Rice, D.C.; Vaporciyan, A.A.; Walsh, G.L.; Roth, J.A. Intrathoracic leaks following esophagectomy are no longer associated with increased mortality. Ann. Surg. 2005, 242, 392–399. [Google Scholar] [CrossRef]
- Booka, E.; Takeuchi, H.; Suda, K.; Fukuda, K.; Nakamura, R.; Wada, N.; Kawakubo, H.; Kitagawa, Y. Meta-analysis of the impact of postoperative complications on survival after oesophagectomy for cancer. BJS Open 2018, 2, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, H.; Miyata, H.; Ozawa, S.; Udagawa, H.; Osugi, H.; Matsubara, H.; Konno, H.; Seto, Y.; Kitagawa, Y. Comparison of short-term outcomes between open and minimally invasive esophagectomy for esophageal cancer using a nationwide database in Japan. Ann. Surg. Oncol. 2017, 24, 1821–1827. [Google Scholar] [CrossRef] [PubMed]
- Ancona, E.; Cagol, M.; Epifani, M.; Cavallin, F.; Zaninotto, G.; Castoro, C.; Alfieri, R.; Ruol, A. Surgical Complications Do Not Affect Longterm Survival after Esophagectomy for Carcinoma of the Thoracic Esophagus and Cardia. J. Am. Coll. Surg. 2006, 203, 661–669. [Google Scholar] [CrossRef]
- Baba, Y.; Yoshida, N.; Shigaki, H.; Iwatsuki, M.; Miyamoto, Y.; Sakamoto, Y.; Watanabe, M.; Baba, H. Prognostic impact of postoperative complications in 502 patients with surgically resected esophageal squamous cell carcinoma: A retrospective single-institution study. Ann. Surg. 2016, 264, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Saeki, H.; Tsutsumi, S.; Tajiri, H.; Yukaya, T.; Tsutsumi, R.; Nishimura, S.; Nakaji, Y.; Kudou, K.; Akiyama, S.; Kasagi, Y.; et al. Prognostic Significance of Postoperative Complications After Curative Resection for Patients with Esophageal Squamous Cell Carcinoma. Ann. Surg. 2017, 265, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Markar, S.; Gronnier, C.; Duhamel, A.; Mabrut, J.-Y.; Bail, J.-P.; Carrere, N.; Lefevre, J.H.; Brigand, C.; Vaillant, J.-C.; Adham, M.; et al. The Impact of Severe Anastomotic Leak on Long-term Survival and Cancer Recurrence After Surgical Resection for Esophageal Malignancy. Ann. Surg. 2015, 262, 972–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferri, L.E.; Law, S.; Wong, K.H.; Kwok, K.F.; Wong, J. The influence of technical complications on postoperative outcome and survival after esophagectomy. Ann. Surg. Oncol. 2006, 13, 557–564. [Google Scholar] [CrossRef]
- Liu, Q.; Li, A.; Tian, Y.; Wu, J.D.; Liu, Y.; Li, T.; Chen, Y.; Han, X.; Wu, K. The CXCL8-CXCR1/2 pathways in cancer. Cytokine Growth Factor Rev. 2016, 31, 61–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuccari, D.A.P.D.C.; Leonel, C.; Castro, R.; Gelaleti, G.B.; Jardim, B.V.; Moscheta, M.G.; Regiani, V.R.; Ferreira, L.C.; Lopes, J.R.; Neto, D.D.S.; et al. An immunohistochemical study of interleukin-8 (IL-8) in breast cancer. Acta Histochem. 2012, 114, 571–576. [Google Scholar] [CrossRef]
- Araki, S.; Omori, Y.; Lyn, D.; Singh, R.K.; Meinbach, D.M.; Sandman, Y.; Lokeshwar, V.B.; Lokeshwar, B.L. Interleukin-8 Is a Molecular Determinant of Androgen Independence and Progression in Prostate Cancer. Cancer Res. 2007, 67, 6854–6862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masuya, D.; Huang, C.; Liu, D.; Kameyama, K.; Hayashi, E.; Yamauchi, A.; Kobayashi, S.; Haba, R.; Yokomise, H. The intratumoral expression of vascular endothelial growth factor and interleukin-8 associated with angiogenesis in nonsmall cell lung carcinoma patients. Cancer 2001, 92, 2628–2638. [Google Scholar] [CrossRef]
- Brew, R.; Erikson, J.S.; West, D.C.; Kinsella, A.R.; Slavin, J.; Christmas, S.E. Interleukin-8 as an autocrine growth factor for human colon carcinoma cells in vitro. Cytokine 2000, 12, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Varney, M.; Singh, R.K. Host CXCR2-dependent regulation of melanoma growth, angiogenesis, and experimental lung metastasis. Cancer Res. 2009, 69, 411–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamura, A.; Takeuchi, H.; Matsuda, S.; Ogura, M.; Miyasho, T.; Nakamura, R.; Takahashi, T.; Wada, N.; Kawakubo, H.; Saikawa, Y.; et al. Factors Affecting Cytokine Change After Esophagectomy for Esophageal Cancer. Ann. Surg. Oncol. 2015, 22, 3130–3135. [Google Scholar] [CrossRef] [PubMed]
- Ogura, M.; Takeuchi, H.; Kawakubo, H.; Nishi, T.; Fukuda, K.; Nakamura, R.; Takahashi, T.; Wada, N.; Saikawa, Y.; Omori, T.; et al. Clinical significance of CXCL-8/CXCR-2 network in esophageal squamous cell carcinoma. Surgery 2013, 154, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Takeuchi, H.; Matsuda, S.; Nishi, T.; Fukuda, K.; Nakamura, R.; Takahashi, T.; Wada, N.; Kawakubo, H.; Kitagawa, Y. IL-8/CXCR2 signalling promotes cell proliferation in oesophageal squamous cell carcinoma and correlates with poor prognosis. Anticancer. Res. 2021, 41, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Cadigan, K.M.; Nusse, R. Wnt signaling: A common theme in animal development. Genes Dev. 1997, 11, 3286–3305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, Y.; Wang, Q.-G.; Wang, J.-X.; Zhu, S.-T.; Jiao, Y.; Li, P.; Zhang, S.-T. Epigenetic Inactivation of the SFRP1 Gene in Esophageal Squamous Cell Carcinoma. Dig. Dis. Sci. 2011, 56, 3195–3203. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.; de Young, N.J.; Pavey, S.J.; Hayward, N.K.; Nancarrow, D.J.; Whiteman, D.C.; Smithers, B.M.; Ruszkiewicz, A.R.; Clouston, A.D.; Gotley, D.C.; et al. Similarity of aberrant DNA methylation in Barrett’s esophagus and esophageal adenocarcinoma. Mol. Cancer 2008, 7, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawata, S.; Hiramatsu, Y.; Shirai, Y.; Watanabe, K.; Nagafusa, T.; Matsumoto, T.; Kikuchi, H.; Kamiya, K.; Takeuchi, H. Multidisciplinary team management for prevention of pneumonia and long-term weight loss after esophagectomy: A single-center retrospective study. Esophagus 2020, 17, 270–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valkenet, K.; Trappenburg, J.C.A.; Ruurda, J.P.; Guinan, E.; Reynolds, J.V.; Nafteux, P.; Fontaine, M.; Rodrigo, H.E.; van der Peet, D.L.; Hania, S.W.; et al. Multicentre randomized clinical trial of inspiratory muscle training versus usual care before surgery for oesophageal cancer. Br. J. Surg. 2018, 105, 502–511. [Google Scholar] [CrossRef]
- Cuschieri, A.; Shimi, S.; Banting, S. Endoscopic oesophagectomy through a right thoracoscopic approach. J. R. Coll. Surg. Edinb. 1992, 37, 7–11. [Google Scholar] [PubMed]
- Marubashi, S.; Takahashi, A.; Kakeji, Y.; Hasegawa, H.; Ueno, H.; Eguchi, S.; Endo, I.; Goi, T.; Saiura, A.; Sasaki, A.; et al. Surgical outcomes in gastroenterological surgery in Japan: Report of the National Clinical. Database: 2011–2019. Ann. Gastroenterol. Surg. 2021, 5. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; Kuppusamy, M.K.; Alderson, D.; Cecconello, I.; Chang, A.; Darling, G.; Davies, A.; D’Journo, X.B.; Gisbertz, S.S.; Griffin, S.M.; et al. Benchmarking Complications Associated with Esophagectomy. Ann. Surg. 2019, 269, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booka, E.; Takeuchi, H.; Kikuchi, H.; Hiramatsu, Y.; Kamiya, K.; Kawakubo, H.; Kitagawa, Y. Recent advances in thoracoscopic esophagectomy for esophageal cancer. Asian J. Endosc. Surg. 2018, 12, 19–29. [Google Scholar] [CrossRef]
- Kingma, B.F.; de Maat, M.F.G.; van der Horst, S.; van der Sluis, P.C.; Ruurda, J.P.; van Hillegersberg, R. Robot-assisted minimally invasive esophagectomy (RAMIE) improves perioperative outcomes: A review. J. Thorac. Dis. 2019, 11, S735–S742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booka, E.; Kikuchi, H.; Haneda, R.; Soneda, W.; Kawata, S.; Murakami, T.; Matsumoto, T.; Hiramatsu, Y.; Takeuchi, H. Short-term Outcomes of Robot-assisted Minimally Invasive Esophagectomy Compared with Thoracoscopic or Transthoracic Esophagectomy. Anticancer. Res. 2021, 41, 4455–4462. [Google Scholar] [CrossRef]
- Mariette, C.; Markar, S.R.; Dabakuyo-Yonli, T.S.; Meunier, B.; Pezet, D.; Collet, D.; D’Journo, X.B.; Brigand, C.; Perniceni, T.; Carrère, N.; et al. Hybrid minimally invasive esophagectomy for esophageal cancer. N. Engl. J. Med. 2019, 380, 152–162. [Google Scholar] [CrossRef]
- Booka, E.; Tsubosa, Y.; Haneda, R.; Ishii, K. Ability of laparoscopic gastric mobilization to prevent pulmonary complications after open thoracotomy or thoracoscopic esophagectomy for esophageal cancer: A systematic review and meta-analysis. World J. Surg. 2020, 44, 980–989. [Google Scholar] [CrossRef]
- Kitagawa, Y.; Uno, T.; Oyama, T.; Kato, K.; Kato, H.; Kawakubo, H.; Kawamura, O.; Kusano, M.; Kuwano, H.; Takeuchi, H.; et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: Part 1. Esophagus 2019, 16, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Kitagawa, Y.; Uno, T.; Oyama, T.; Kato, K.; Kato, H.; Kawakubo, H.; Kawamura, O.; Kusano, M.; Kuwano, H.; Takeuchi, H.; et al. Esophageal cancer practice guidelines 2017 edited by the Japan esophageal society: Part 2. Esophagus 2019, 16, 25–43. [Google Scholar] [CrossRef]
- Haneda, R.; Booka, E.; Ishii, K.; Kikuchi, H.; Hiramatsu, Y.; Kamiya, K.; Ogawa, H.; Yasui, H.; Takeuchi, H.; Tsubosa, Y. Evaluation of Definitive Chemoradiotherapy Versus Radical Esophagectomy in Clinical T1bN0M0 Esophageal Squamous Cell Carcinoma. World J. Surg. 2021, 45, 1835–1844. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Dental Screening and Professional Cleaning |
|---|
| Cessation of smoking and drinking |
| Measurement of physical fitness |
| Respiratory exercise using a device |
| Nutritional screening and support |
| Sufficient pain control |
| Early ambulation |
| Early enteral nutrition via jejunostomy tube |
| Swallowing evaluation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Booka, E.; Kikuchi, H.; Hiramatsu, Y.; Takeuchi, H. The Impact of Infectious Complications after Esophagectomy for Esophageal Cancer on Cancer Prognosis and Treatment Strategy. J. Clin. Med. 2021, 10, 4614. https://doi.org/10.3390/jcm10194614
Booka E, Kikuchi H, Hiramatsu Y, Takeuchi H. The Impact of Infectious Complications after Esophagectomy for Esophageal Cancer on Cancer Prognosis and Treatment Strategy. Journal of Clinical Medicine. 2021; 10(19):4614. https://doi.org/10.3390/jcm10194614
Chicago/Turabian StyleBooka, Eisuke, Hirotoshi Kikuchi, Yoshihiro Hiramatsu, and Hiroya Takeuchi. 2021. "The Impact of Infectious Complications after Esophagectomy for Esophageal Cancer on Cancer Prognosis and Treatment Strategy" Journal of Clinical Medicine 10, no. 19: 4614. https://doi.org/10.3390/jcm10194614
APA StyleBooka, E., Kikuchi, H., Hiramatsu, Y., & Takeuchi, H. (2021). The Impact of Infectious Complications after Esophagectomy for Esophageal Cancer on Cancer Prognosis and Treatment Strategy. Journal of Clinical Medicine, 10(19), 4614. https://doi.org/10.3390/jcm10194614