
Reliability of the Preliminary OMERACT Juvenile Idiopathic Arthritis MRI Score (OMERACT JAMRIS-SIJ)

 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Bone Marrow Edema | Joint Space Inflammation | Capsulitis | Sclerosis | Erosion | Fat Lesion | Ankylosis | Backfill | |
|---|---|---|---|---|---|---|---|---|
| Right upper ilium | 8.09 | 8.09 | 8.09 | 8.41 | 8.41 | 8.41 | 8.41 | 8.41 |
| Right upper sacrum | 8.09 | 8.41 | ||||||
| Right lower ilium | 8.06 | 8.09 | 8.09 | 8.41 | 8.41 | 8.41 | 8.41 | 8.41 |
| Right lower sacrum | 8.09 | 8.41 | 8.41 | 8.41 | ||||
| Right depth | 8.09 | |||||||
| Right intensity | 8.09 | |||||||
| Left Upper Ilium | 8.09 | 8.09 | 8.09 | 8.41 | 8.41 | 8.41 | 8.41 | 8.41 |
| Left Upper Sacrum | 8.09 | 8.41 | 8.41 | 8.41 | ||||
| Left Lower Ilium | 8.09 | 8.09 | 8.09 | 8.41 | 8.41 | 8.41 | 8.41 | 8.41 |
| Left Lower Sacrum | 8.09 | 8.41 | 8.41 | 8.41 | ||||
| Left Depth | 8.09 | |||||||
| Left Intensity | 8.09 | |||||||
| R+L Upper Ilium | 8.09 (7–9, 8) | 8.09 (7–9, 8) | 8.09 (7–9, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) |
| R+L Upper Sacrum | 7.95 (7–9, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | ||||
| R+L Lower Ilium | 8.07 (7–9, 8) | 8.09 (7–9, 8) | 8.09 (7–9, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) |
| R+L Lower Sacrum | 8.09 (7–7, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | 8.41 (7–10, 8) | ||||
| R+L Depth | 8.09 (7–7, 8) | |||||||
| R+L Intensity | 8.09 (7–9, 8) |
Appendix C
| Bone Marrow Edema | Joint Space Inflammation | Capsulitis | Erosion | Fat Lesion | Ankylosis | Backfill | |
|---|---|---|---|---|---|---|---|
| Right upper ilium | 0.17 | 0.18 | 0.06 | 0.14 | 0.06 | 0.03 | 0.02 |
| Right upper sacrum | 0.15 | 0.05 | 0.05 | ||||
| Right lower ilium | 0.17 | 0.16 | 0.03 | 0.10 | 0.05 | 0.01 | 0.02 |
| Right lower sacrum | 0.13 | 0.04 | 0.03 | ||||
| Right depth | 0.23 | ||||||
| Right intensity | 0.11 | ||||||
| Left Upper Ilium | 0.20 | 0.18 | 0.05 | 0.18 | 0.06 | 0.00 | 0.02 |
| Left Upper Sacrum | 0.16 | 0.06 | 0.03 | ||||
| Left Lower Ilium | 0.29 | 0.16 | 0.04 | 0.17 | 0.03 | 0.00 | 0.01 |
| Left Lower Sacrum | 0.15 | 0.03 | 0.01 | ||||
| Left Depth | 0.30 | ||||||
| Left Intensity | 0.14 | ||||||
| R+L Upper Ilium | 0.19 | 0.18 | 0.05 | 0.16 | 0.06 | 0.01 | 0.02 |
| R+L Upper Sacrum | 0.16 | 0.05 | 0.04 | ||||
| R+L Lower Ilium | 0.23 | 0.16 | 0.03 | 0.13 | 0.04 | 0.00 | 0.03 |
| R+L Lower Sacrum | 0.14 | 0.04 | 0.02 | ||||
| R+L Depth | 0.26 | ||||||
| R+L Intensity | 0.12 |
References
- Weiss, P.F.; Maksymowych, W.P.; Lambert, R.G.; Jaremko, J.L.; Biko, D.M.; Paschke, J.; Brandon, T.G.; Xiao, R.; Chauvin, N.A. Feasibility and reliability of the Spondyloarthritis Research Consortium of Canada sacroiliac joint inflammation score in children. Arthritis Res. Ther. 2018, 20, 56. [Google Scholar] [CrossRef] [PubMed]
- Petty, R.E.; Southwood, T.R.; Manners, P.; Baum, J.; Glass, D.N.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.-M.; et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: Second revision, Edmonton, 2001. J. Rheumatol. 2004, 31, 390–392. [Google Scholar] [PubMed]
- Martini, A.; Ravelli, A.; Avcin, T.; Beresford, M.W.; Burgos-Vargas, R.; Cuttica, R.; Ilowite, N.T.; Khubchandani, R.; Laxer, R.M.; Lovell, D.J.; et al. Toward New Classification Criteria for Juvenile Idiopathic Arthritis: First Steps, Pediatric Rheumatology International Trials Organization International Consensus. J. Rheumatol. 2019, 46, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Consolaro, A.; Ruperto, N.; Bazso, A.; Pistorio, A.; Magni-Manzoni, S.; Filocamo, G.; Malattia, C.; Viola, S.; Martini, A.; Ravelli, A. Development and validation of a composite disease activity score for juvenile idiopathic arthritis. Arthritis Care Res. Off. J. Am. Coll. Rheumatol. 2009, 61, 658–666. [Google Scholar] [CrossRef]
- Consolaro, A.; Negro, G.; Gallo, M.C.; Bracciolini, G.; Ferrari, C.; Schiappapietra, B.; Pistorio, A.; Bovis, F.; Ruperto, N.; Martini, A.; et al. Defining criteria for disease activity states in nonsystemic juvenile idiopathic arthritis based on a three-variable juvenile arthritis disease activity score. Arthritis Care Res. 2014, 66, 1703–1709. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.S.; Malcarne, V.L.; Roesch, S.C.; Sadler, G.R. The Cultural Health Attributions Questionnaire (CHAQ): Reliability, validity, and refinement. Cult. Divers. Ethn. Minor. Psychol. 2014, 20, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Ringold, S.; Angeles-Han, S.T.; Beukelman, T.; Lovell, D.; Cuello, C.A.; Becker, M.L.; Colbert, R.A.; Feldman, B.M.; Ferguson, P.J.; Gewanter, H.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Treatment of Juvenile Idiopathic Arthritis: Therapeutic Approaches for Non-Systemic Polyarthritis, Sacroiliitis, and Enthesitis. Arthritis Care Res. 2019, 71, 717–734. [Google Scholar] [CrossRef]
- Vleeming, A.; Schuenke, M.D.; Masi, A.T.; Carreiro, J.E.; Willard, F.H. The sacroiliac joint: An overview of its anatomy, function and potential clinical implications. J. Anat. 2012, 221, 537–567. [Google Scholar] [CrossRef]
- Colebatch-Bourn, A.N.; Edwards, C.J.; Collado, P.; D’Agostino, M.-A.; Hemke, R.; Jousse-Joulin, S.; Maas, M.; Martini, A.; Naredo, E.; Østergaard, M.; et al. EULAR-PReS points to consider for the use of imaging in the diagnosis and management of juvenile idiopathic arthritis in clinical practice. Ann. Rheum. Dis. 2015, 74, 1946–1957. [Google Scholar] [CrossRef]
- Cellucci, T.; Guzman, J.; Petty, R.E.; Batthish, M.; Benseler, S.M.; Ellsworth, J.E.; Houghton, K.M.; Leblanc, C.M.A.; Huber, A.M.; Luca, N.; et al. Management of Juvenile Idiopathic Arthritis 2015: A position statement from the pediatric Committee of the Canadian Rheumatology Association. J. Rheumatol. 2016, 43, 1773–1776. [Google Scholar] [CrossRef]
- Restrepo, R.; Lee, E.Y.; Babyn, P.S. Juvenile idiopathic arthritis: Current practical imaging assessment with emphasis on magnetic resonance imaging. Radiol. Clin. N. Am. 2013, 51, 703–719. [Google Scholar] [CrossRef][Green Version]
- Herregods, N.; Dehoorne, J.; Joos, R.; Jaremko, J.L.; Baraliakos, X.; Leus, A.; Van den Bosch, F.; Verstraete, K.; Jans, L. Diagnostic value of MRI features of sacroiliitis in juvenile spondyloarthritis. Clin. Radiol. 2015, 70, 1428–1438. [Google Scholar] [CrossRef] [PubMed]
- Lambert, R.G.; Bakker, P.A.C.; van der Heijde, D.; Weber, U.; Rudwaleit, M.; Hermann, K.-G.A.; Sieper, J.; Baraliakos, X.; Bennett, A.; Braun, J.; et al. Defining active sacroiliitis on MRI for classification of axial spondyloarthritis: Update by the ASAS MRI working group. Ann. Rheum. Dis. 2016, 75, 1958–1963. [Google Scholar] [CrossRef]
- Maksymowych, W.P.; Weber, U. Diagnostic utility of MRI in early spondyloarthritis. Curr. Rheumatol. Rep. 2011, 13, 402–408. [Google Scholar] [CrossRef]
- Maksymowych, W.P.; Inman, R.D.; Salonen, D.; Dhillon, S.S.; Williams, M.; Stone, M.; Conner-spady, B.; Palsat, J.; Lambert, R.G.W. Spondyloarthritis research Consortium of Canada magnetic resonance imaging index for assessment of sacroiliac joint inflammation in ankylosing spondylitis. Arthritis Rheum. 2005, 53, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Maksymowych, W.P.; Wichuk, S.; Chiowchanwisawakit, P.; Lambert, R.G.; Pedersen, S.J. Development and preliminary validation of the spondyloarthritis research consortium of Canada magnetic resonance imaging sacroiliac joint structural score. J. Rheumtol. 2015, 42, 79–86. [Google Scholar] [CrossRef]
- Malattia, C.; Damasio, M.B.; Pistorio, A.; Ioseliani, M.; Vilca, I.; Valle, M.; Ruperto, N.; Viola, S.; Buoncompagni, A.; Magnano, G.M.; et al. Development and preliminary validation of a paediatric-targeted MRI scoring system for the assessment of disease activity and damage in juvenile idiopathic arthritis. Ann. Rheum. Dis. 2011, 70, 440–446. [Google Scholar] [CrossRef]
- Althoff, C.E.; Sieper, J.; Song, I.-H.; Haibel, H.; Weiß, A.; Diekhoff, T.; Rudwaleit, M.; Freundlich, B.; Hamm, B.; Hermann, K.-G.A. Active inflammation and structural change in early active axial spondyloarthritis as detected by whole-body MRI. Ann. Rheum. Dis. 2013, 72, 967–973. [Google Scholar] [CrossRef]
- Weiss, P.F.; Maksymowych, W.P.; Lambert, R.G.; Jaremko, J.L.; Biko, D.M.; Paschke, J.; Brandon, T.G.; Xiao, R.; Chauvin, N.A. Feasibility and Reliability of the Spondyloarthritis Research Consortium of Canada Sacroiliac Joint Structural Score in Children. J. Rheumatol. 2018, 45, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Panwar, J.; Tse, S.M.L.; Lim, L.; Tolend, M.A.; Radhakrishnan, S.; Salman, M.; Moineddin, R.; Doria, A.S.; Stimec, J. Spondyloarthritis Research Consortium of Canada Scoring System for Sacroiliitis in Juvenile Spondyloarthritis/Enthesitis-related Arthritis: A Reliability, Validity, and Responsiveness Study. J. Rheumatol. 2019, 46, 636–644. [Google Scholar] [CrossRef]
- Otobo, T.M.; Conaghan, P.G.; Maksymowych, W.P.; van der Heijde, D.; Weiss, P.; Sudol-Szopinska, I.; Herregods, N.; Jaremko, J.L.; Meyers, A.B.; Rumsey, D.; et al. Preliminary Definitions for Sacroiliac Joint Pathologies in the OMERACT Juvenile Idiopathic Arthritis MRI Score (OMERACT JAMRIS-SIJ). J. Rheumatol. 2019, 46, 1192–1197. [Google Scholar] [CrossRef]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Maksymowych, W.P.; Krabbe, S.; Biko, D.; Weiss, P.; Maksymowych, M.P.; Cheah, J.; Kröber, G.; Weber, U.; Danebod, K.; Bird, P.; et al. FRI0597 Validation of web-based calibration modules for imaging scoring systems based on principles of artificial intelligence: The sparcc mri sacroiliac joint inflammation score. Ann. Rheum. Dis. 2018, 77, 822. [Google Scholar] [CrossRef]
- Leblanc, C.M.A.; Lang, B.; Bencivenga, A.; Chetaille, A.-L.; Dancey, P.; Dent, P.; Miettunen, P.; Oen, K.; Rosenberg, A.; Roth, J.; et al. Access to Biologic Therapies in Canada for Children with Juvenile Idiopathic Arthritis. J. Rheumatol. 2012, 39, 1875–1879. [Google Scholar] [CrossRef] [PubMed]
- Clemente, E.J.I.; Tolend, M.; Junhasavasdikul, T.; Stimec, J.; Tzaribachev, N.; Koos, B.; Spiegel, L.; Moineddin, R.; Doria, A.S. Qualitative and semi-quantitative assessment of temporomandibular joint MRI protocols for juvenile idiopathic arthritis at 1.5 and 3.0 T. Eur. J. Radiol. 2018, 98, 90–99. [Google Scholar] [CrossRef]
- Chauvin, N.A.; Xiao, R.; Brandon, T.G.; Biko, D.M.; Francavilla, M.; Khrichenko, D.; Weiss, P.F. MRI of the Sacroiliac Joint in Healthy Children. Am. J. Roentgenol. 2019, 212, 1–7. [Google Scholar] [CrossRef]
- Herregods, N.; Jans, L.B.O.; Chen, M.; Paschke, J.; De Buyser, S.L.; Renson, T.; Dehoorne, J.; Joos, R.; Lambert, R.G.W.; Jaremko, J.L. Normal subchondral high T2 signal on MRI mimicking sacroiliitis in children: Frequency, age distribution, and relationship to skeletal maturity. Eur. Radiol. 2021, 31, 3498–3507. [Google Scholar] [CrossRef]
- Mehta, S.; Bastero-Caballero, R.F.; Sun, Y.; Zhu, R.; Murphy, D.K.; Hardas, B.; Koch, G. Performance of intraclass correlation coefficient (ICC) as a reliability index under various distributions in scale reliability studies. Stat. Med. 2018, 37, 2734–2752. [Google Scholar] [CrossRef]



| Features | Definitions | Scores |
|---|---|---|
| Inflammation MRI Components | Score range/slide | |
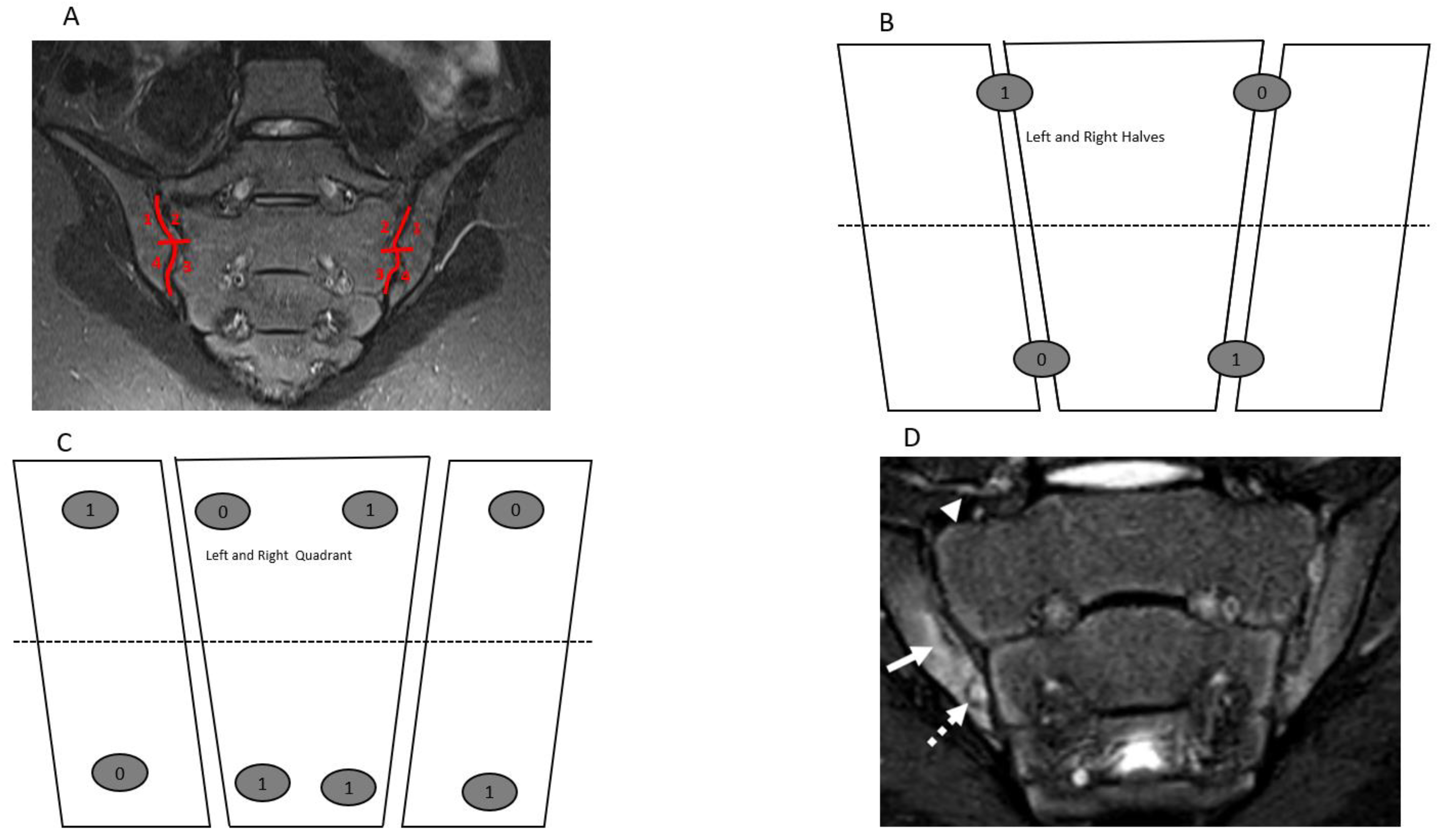
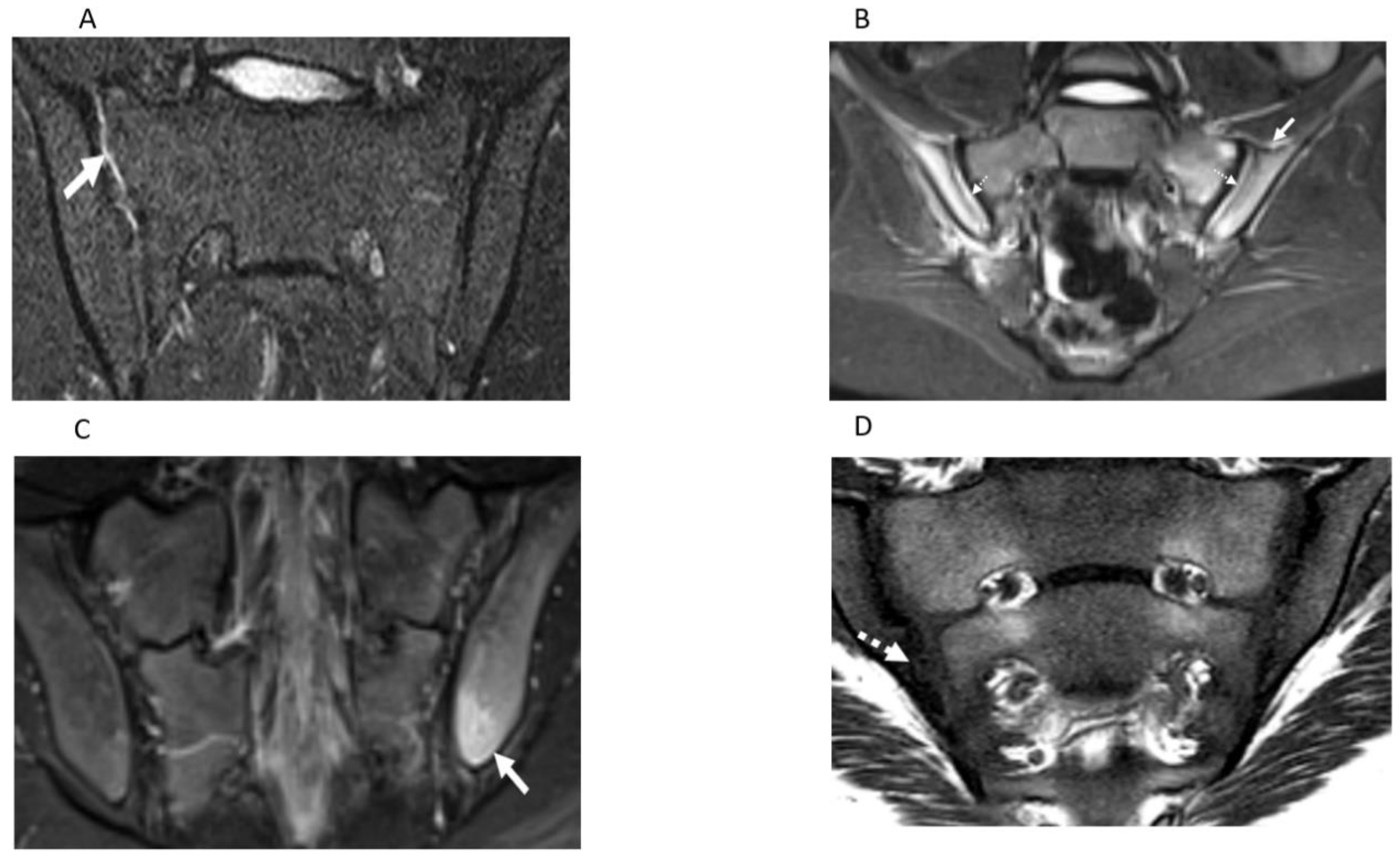
| BME | An ill-defined area of high bone marrow signal intensity † within the subchondral bone in the ilium or sacrum on fluid-sensitive images | Score 4 quadrant/SIJ 0/1, range 0–8 |
| BME Intensity | Hyperintensity of the marrow edema using the presacral veins as reference | Score each SIJ 0/1, 0–2 |
| BME Depth | Continues to increase the signal of depth ≥ 5 mm/ ≥ 1 cm from the articular surface | Score each SIJ 0/1, 0–2 |
| Capsulitis | High signal on fluid-sensitive and/or post-contrast enhancement involving the SIJ capsule | Score halves / SIJ 0/1, 0–4 |
| JSI | Increased signal on fluid-sensitive or contrast-enhanced T1-weighted images within the joint space of the cartilaginous portion of the SIJ | Score halves/ SIJ 0/1, 0–4 |
| Enthesitis | High signal in bone marrow and/or soft tissue on a fluid-sensitive sequences or a contrast-enhanced T1-weighted sequence at sites where ligaments and tendons attach to a bone | Score each case 0/1, 0–1 |
| Structural MRI Components | ||
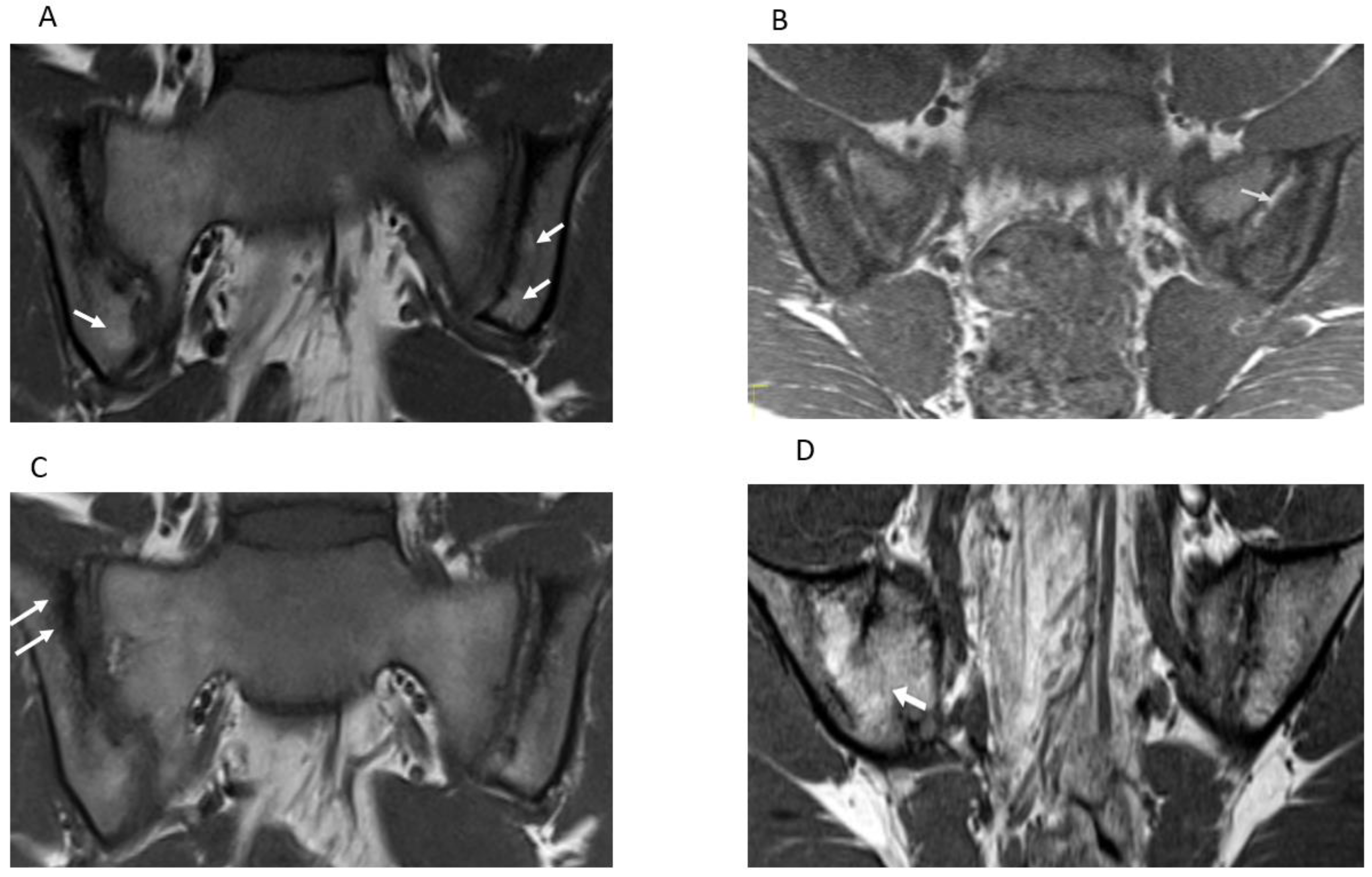
| Sclerosis | A substantially wider than normal area of low subarticular bone signal on T1-weighted and fluid-sensitive images (of ≥5 mm in adolescents) | Score 4 quadrants/SIJ 0/1, 0–8 |
| Erosion | Bony defect (or irregularity with associated bone marrow edema, sclerosis, or fatty lesion) at the osteochondral interface involving both contour and signal on both T1-weighted and fluid-sensitive images | Score 4 quadrants/SIJ 0/1, 0–8 |
| Fat Lesion | Increased homogenous signal intensity on T1-weighted non-FS image in subchondral bone with a distinct border | Score 4 quadrants /SIJ 0/1, 0–8 |
| Backfill | A bright signal on a T1-weighted sequence in a typical location for an erosion, with signal intensity greater than normal bone marrow, and meeting the following requirements. 1. It is associated with complete loss of the dark appearance of the subchondral cortex at its expected location. 2. It is clearly demarcated from adjacent bone marrow by an irregular band dark signal reflecting sclerosis at the border of the original erosion | Score halves/SIJ 0/1, 0–4 |
| Ankylosis | Presence of signal equivalent to regional bone marrow continuously bridging a portion of the joint space between the iliac and sacral bones | Score halves/0/1, 0–4 |
| Bone Marrow Edema | Joint Space Inflammation | Capsulitis | Enthesitis | Inflammation Domain | Sclerosis | Erosion | Fat Lesion | Ankylosis | Backfill | Damage Domain | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 17.36 | 5.48 | 1.42 | 0.21 | 24.26 | 1.89 | 6.33 | 2.49 | 0.31 | 0.68 | 11.70 |
| Median | 3 | 0 | 0 | 0 | 5 | 0 | 3 | 0 | 0 | 0 | 5 |
| SD | 24.94 | 8.30 | 3.74 | 0.41 | 34.26 | 3.74 | 9.03 | 6.31 | 1.75 | 3.14 | 15.54 |
| Kurtosis | 1.23 | 1.75 | 9.18 | 0.13 | 1.06 | 4.65 | 6.48 | 21.11 | 35.27 | 38.08 | 6.14 |
| Skewness | 1.48 | 1.52 | 3.00 | 1.46 | 1.44 | 2.27 | 2.19 | 3.98 | 5.92 | 5.93 | 2.15 |
| Range | 99 | 42 | 22 | 1 | 141 | 19 | 60 | 53 | 14 | 27 | 99 |
| Minimum | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Maximum | 99 | 42 | 22 | 1 | 141 | 19 | 60 | 53 | 14 | 27 | 99 |
| Confidence Level (95.0%) | 3.17 | 1.06 | 0.48 | 0.06 | 4.36 | 0.48 | 1.15 | 0.80 | 0.22 | 0.40 | 1.98 |
| ICC | 0.76 | 0.61 | 0.58 | 0.20 | 0.77 | 0.54 | 0.51 | 0.40 | 0.90 | 0.38 | 0.60 |
| Radiologist | Bone Marrow Edema | Joint Space Inflammation | Capsulitis | Enthesitis | Inflammation Domain | Rheumatologist | Bone Marrow Edema | Joint Space Inflammation | Capsulitis | Enthesitis | Inflammation Domain |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 19.87 | 5.84 | 1.64 | 0.21 | 27.35 | Mean | 9.85 | 4.38 | 0.75 | 0.08 | 14.98 |
| Median | 4 | 0 | 0 | 0 | 7 | Median | 1 | 0 | 0 | 0 | 1 |
| SD | 26.98 | 8.59 | 4.09 | 0.40 | 36.79 | SD | 15.28 | 7.30 | 2.27 | 0.28 | 23.03 |
| Kurtosis | 0.52 | 1.78 | 7.48 | 0.04 | 0.49 | Kurtosis | 1.16 | 0.76 | 9.74 | 7.83 | 0.84 |
| Skewness | 1.28 | 1.51 | 2.77 | 1.43 | 1.29 | Skewness | 1.54 | 1.478 | 3.23 | 3.09 | 1.48 |
| Range | 99 | 42 | 22 | 1 | 141 | Range | 56 | 24 | 11 | 1 | 80 |
| Confidence level (95.0%) | 3.97 | 1.26 | 0.60 | 0.06 | 5.41 | Confidence Level (95.0%) | 3.95 | 1.89 | 0.59 | 0.07 | 5.95 |
| IQR | 0–35 | 0–11 | 0–0 | 0–0 | 0–50 | IQR | 0–14 | 0–6 | 0–0 | 0–0 | 0–21 |
| ICC | 0.82 | 0.61 | 0.60 | 0.16 | 0.81 | ICC | 0.76 | 0.50 | 0.80 | 0.09 | 0.73 |
| Radiologist | Sclerosis | Erosion | Fatty Lesion | Ankylosis | Backfill | Damage Domain | Rheumatologist | Sclerosis | Erosion | Fatty Lesion | Ankylosis | Backfill | Damage Domain |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 1.93 | 6.66 | 3.19 | 0.28 | 0.72 | 12.77 | Mean | 1.75 | 5.37 | 0.38 | 0.40 | 0.57 | 8.47 |
| Median | 0 | 3 | 0 | 0 | 0 | 6 | Median | 0 | 2.5 | 0 | 0 | 0 | 4.5 |
| SD | 3.88 | 9.58 | 7.10 | 1.57 | 3.23 | 16.87 | SD | 3.30 | 7.09 | 1.53 | 2.20 | 2.87 | 10.04 |
| Kurtosis | 4.72 | 6.47 | 15.77 | 34.49 | 36.95 | 5.16 | Kurtosis | 3.55 | 0.20 | 22.47 | 30.85 | 45.25 | 1.58 |
| Skewness | 2.30 | 2.24 | 3.44 | 5.88 | 5.81 | 2.04 | Skewness | 2.05 | 1.22 | 4.66 | 5.57 | 6.49 | 1.34 |
| Range | 19 | 60 | 53 | 11 | 27 | 99 | Range | 14 | 24 | 9 | 14 | 21 | 44 |
| Confidence level (95.0%) | 0.57 | 1.41 | 1.04 | 0.23 | 0.48 | 2.48 | Confidence Level (95.0%) | 0.85 | 1.83 | 0.40 | 0.57 | 0.74 | 2.59 |
| IQR | 0–2 | 0–10 | 0–4 | 0–0 | 0–0 | 0–20 | IQR | 0–2 | 0–9 | 0–0 | 0–0 | 0–0 | 0–15 |
| ICC | 0.61 | 0.44 | 0.52 | 0.90 | 0.29 | 0.62 | ICC | 0.17 | 0.17 | 0.02 | 0.95 | 0.53 | 0.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otobo, T.M.; Herregods, N.; Jaremko, J.L.; Sudol-Szopinska, I.; Maksymowych, W.P.; Meyers, A.B.; Weiss, P.; Tse, S.; Paschke, J.; Moineddin, R.; et al. Reliability of the Preliminary OMERACT Juvenile Idiopathic Arthritis MRI Score (OMERACT JAMRIS-SIJ). J. Clin. Med. 2021, 10, 4564. https://doi.org/10.3390/jcm10194564
Otobo TM, Herregods N, Jaremko JL, Sudol-Szopinska I, Maksymowych WP, Meyers AB, Weiss P, Tse S, Paschke J, Moineddin R, et al. Reliability of the Preliminary OMERACT Juvenile Idiopathic Arthritis MRI Score (OMERACT JAMRIS-SIJ). Journal of Clinical Medicine. 2021; 10(19):4564. https://doi.org/10.3390/jcm10194564
Chicago/Turabian StyleOtobo, Tarimobo M., Nele Herregods, Jacob L. Jaremko, Iwona Sudol-Szopinska, Walter P. Maksymowych, Arthur B. Meyers, Pamela Weiss, Shirley Tse, Joel Paschke, Rahim Moineddin, and et al. 2021. "Reliability of the Preliminary OMERACT Juvenile Idiopathic Arthritis MRI Score (OMERACT JAMRIS-SIJ)" Journal of Clinical Medicine 10, no. 19: 4564. https://doi.org/10.3390/jcm10194564
APA StyleOtobo, T. M., Herregods, N., Jaremko, J. L., Sudol-Szopinska, I., Maksymowych, W. P., Meyers, A. B., Weiss, P., Tse, S., Paschke, J., Moineddin, R., Haroon, N., Tzaribachev, N., Appenzeller, S., Papakonstantinou, O., Kirkhus, E., van Rossum, M. A. J., Carrino, J., Conaghan, P. G., Tolend, M., ... Doria, A. S. (2021). Reliability of the Preliminary OMERACT Juvenile Idiopathic Arthritis MRI Score (OMERACT JAMRIS-SIJ). Journal of Clinical Medicine, 10(19), 4564. https://doi.org/10.3390/jcm10194564