
Computed Tomography and Spirometry Can Predict Unresectability in Malignant Pleural Mesothelioma

 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
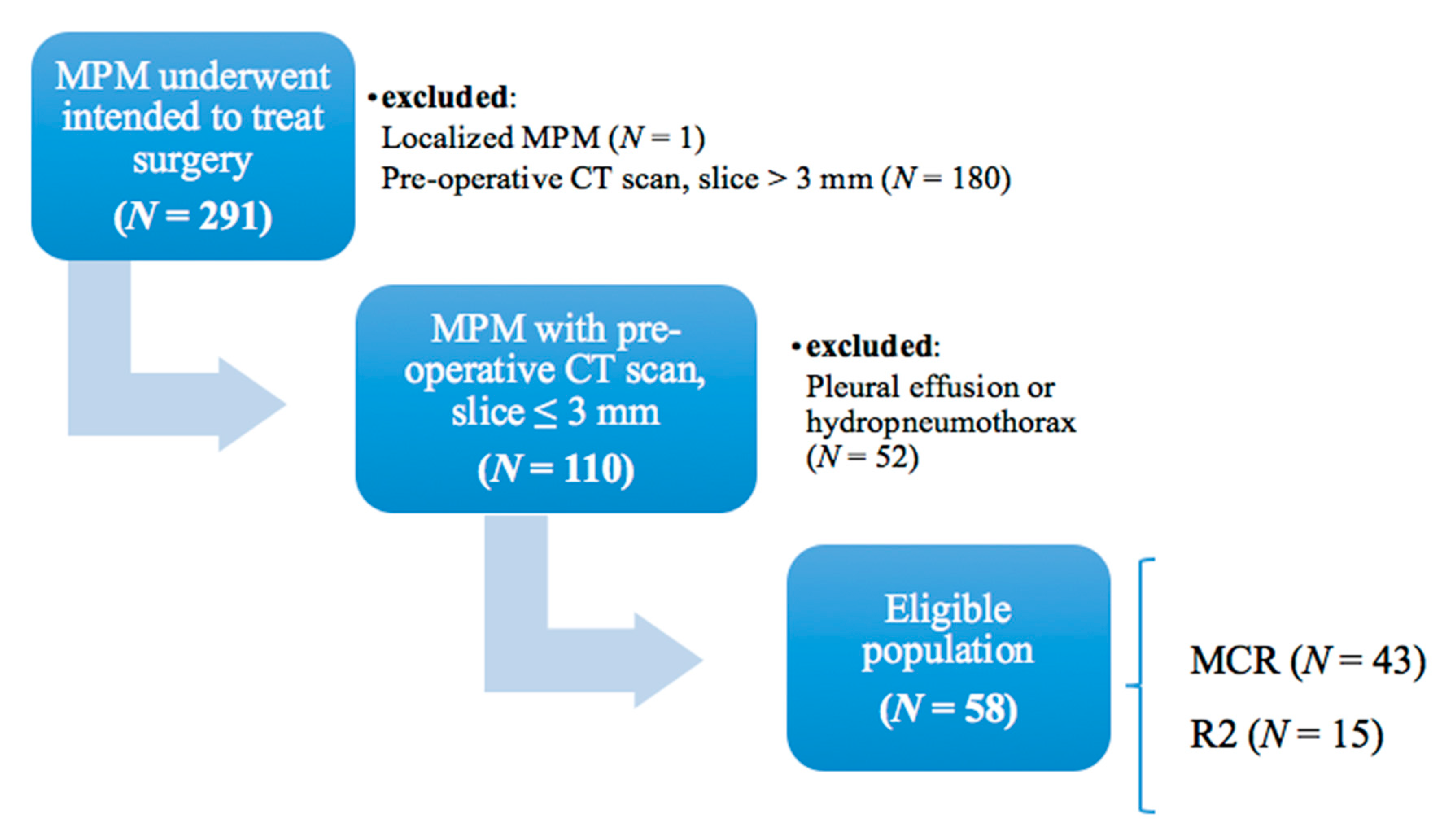
2.1. Patient Selection
2.2. Preoperative Evaluation and Surgical Approach
2.3. Radiological Evaluation
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Preoperative Predictors of Unresectability in MPM
4. Discussion
4.1. MCR Is the Central Principle of Surgery for MPM
4.2. The Role of CT and Spirometry
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Comprehensive Cancer Network. 2021. Malignant Pleural Mesothelioma (Version 1.2021). Available online: https://www.nccn.org/professionals/physician_gls/pdf/mpm_blocks.pdf (accessed on 4 December 2020).
- Rusch, V.; Baldini, E.H.; Bueno, R.; De Perrot, M.; Flores, R.; Hasegawa, S.; Klepetko, W.; Krug, L.; Lang-Lazdunski, L.; Pass, H.; et al. The role of surgical cytoreduction in the treatment of malignant pleural mesothelioma: Meeting summary of the International Mesothelioma Interest Group Congress, 11–14 September 2012, Boston, MA, USA. J. Thorac. Cardiovasc. Surg. 2013, 145, 909–910. [Google Scholar] [CrossRef] [PubMed]
- Burt, M.B.; Lee, H.S.; Raghuram, A.C.; Strange, C.; Mason, J.; Strange, T.; Delago, J.; Sugarbaker, D.J. Preoperative prediction of unresectability in malignant pleural mesothelioma. J. Thorac. Cardiovasc. Surg. 2020, 159, 2512–2520. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V. Standardization of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Wanger, J.; Clausen, J.L.; Coates, A.; Pedersen, O.F.; Brysasco, V.; Burgos, F.; Casaburi, R.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; et al. Standardization of the measurement of lung volumes. Eur. Respir. J. 2005, 26, 511–522. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, N.; Crapo, R.O.; Viegi, G.; Johnson, D.C.; van der Grinten, C.P.M.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Enright, P.; et al. Standardization of the single-breath determination of carbon monoxide uptake in the lung. Eur. Respir. J. 2005, 26, 720–735. [Google Scholar] [CrossRef]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.E.A.; Wanger, J. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef]
- Bezenji, L.; Van Schil, P.E.; Carp, L. The eight TNM classification for malignant pleural mesothelioma. Transl. Lung Cancer Res. 2018, 7, 543–549. [Google Scholar] [CrossRef]
- Sensakovic, W.F.; Armato, S.G., III; Straus, C.; Roberts, R.Y.; Caligiuri, P.; Starkey, A.; Kindler, H.L. Computerized segmentation and measurement of malignant pleural mesothelioma. Med. Phys. 2011, 38, 238–244. [Google Scholar] [CrossRef]
- Armato, S.G., III; Nowak, A.K. Revised modified RECIST criteria for the assessment of response in malignant pleural mesothelioma (version 1.1). J. Thorac. Oncol. 2018, 13, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Marulli, G.; Breda, C.; Fontana, P.; Ratto, G.B.; Leoncini, G.; Alloisio, M.; Rea, F. Pleurectomy-decortication in malignant pleural mesothelioma: Are different surgical techniques associated with different outcomes? Results from a multicentre study. Eur. J. Cardiothorac. Surg. 2017, 52, 63–69. [Google Scholar] [CrossRef]
- Sugarbaker, D.J. Macroscopic complete resection: The goal of primary surgery in multimodality therapy for pleural mesothelioma. J. Thorac. Oncol. 2006, 1, 175–176. [Google Scholar] [CrossRef]
- Treasure, T. What is the best approach for surgery of malignant pleural mesothelioma? It is to put our efforts into obtaining trustworthy evidence for practice. J. Thorac. Cardiovasc. Surg. 2016, 151, 307–309. [Google Scholar] [CrossRef]
- Sugarbaker, D.J.; Flores, R.M.; Jaklitsch, M.T.; Richards, W.G.; Strauss, G.M.; Corson, J.M.; Mentzer, S.J. Resection margins, extrapleural nodal status and cell type determine post-operative long term survival in trimodality therapy of malignant pleural mesothelioma: Results in 183 patients. J. Thorac. Cardiovasc. Surg. 1999, 171, 54–63. [Google Scholar] [CrossRef]
- Rusch, V.W.; Giroux, D.; Kennedy, C. Initial analysis of the international association for the study of lung cancer mesothelioma database. J. Thorac. Oncol. 2012, 7, 1631–1639. [Google Scholar] [CrossRef]
- Lang-Lazdunski, L.; Bille, A.; Papa, S.; Ruffini, E.; Cangir, A.K.; Rice, D.; Van Meerbeeck, J.P. Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine, prophylactic radiotherapy and systemic chemotherapy in patients with malignant pleural mesothelioma: A 10-year experience. J. Thorac. Cardiovasc. Surg. 2015, 149, 558–566. [Google Scholar] [CrossRef]
- Giles, A.E.; Kidane, B. Commentary: Know your enemy–understanding futility in the battle against malignant pleural mesothelioma. J. Thorac. Cardiovasc. Surg. 2020, 159, 2523–2524. [Google Scholar] [CrossRef] [PubMed]
- Armato, S.G., III; Sensakovic, W.F. Automated lung segmentation for thoracic CT: Impact on computer-aided diagnosis. Acad. Radiol. 2004, 11, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Labby, E.Z.; ArmaTo, S.G., III; Dignam, J.J.; Straus, C.; Kindler, H.L.; Nowak, A.K. Lung volume measurements as surrogate marker for patient response in malingant pleural mesothelioa. J. Thorac. Oncol. 2013, 8, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, M.; Takeuchi, J.; Teruhisa, T.; Kuroda, A.; Nakamura, A.; Nakamichi, T.; Hasegawa, S. Pleural thickness after neoadjuvant chemotherapy is a prognostic factor in malignant pleural mesothelioma. J. Thorac. Cardiovasc. Surg. 2019, 157, 404–413. [Google Scholar] [CrossRef] [PubMed]
- De Perrot, M. Commentary: Is thoracic cage volume a new parameter for clinical staging in mesothelioma? J. Thorac. Cardiovasc. Surg. 2020, 159, 2520–2521. [Google Scholar] [CrossRef] [PubMed]
- Marulli, G.; Rea, F.; Nicotra, S.; Favaretto, A.G.; Perissinotto, E.; Chizzolini, M.; Braccioni, F. Effect of induction chemotherapy on lung function and exercise capacity in patients affected by malignant pleural mesothelioma. Eur. J. Cardioth. Surg. 2010, 37, 1464–1469. [Google Scholar] [CrossRef] [PubMed]
- Marulli, G.; Di Chiara, F.; Braccioni, F.; Perissinotto, E.; Pasello, G.; Favaretto, A.G.; Rea, F. Changes in pulmonary function tests predict radiological response to chemotherapy in malignant pleural mesothelioma. Eur. J. Cardiothorac. Surg. 2013, 44, 104–110. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nowak, A.K.; Chansky, K.; Rice, D.C.; Pass, H.I.; Kindler, H.L.; Shemanski, L.; Yoshimura, M. The IASLC Mesothelioma Staging Project: Proposals for revisions of the T descriptors in the forthcoming eighth editions of the TNM classification for mesothelioma. J. Thorac. Oncol. 2016, 11, 2089–2099. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | MCR, N = 43 | R2, N = 15 | p-Value |
|---|---|---|---|
| Age (years), median (IQR) | 64 (56–68) | 63 (59–69) | 0.6 |
| Sex, n (%) | 0.01 | ||
| Male | 25 (58) | 14 (93) | |
| Female | 18 (42) | 1 (7) | |
| Side, n (%) | 0.4 | ||
| Right | 22 (51) | 10 (67) | |
| Left | 21 (49) | 5 (33) | |
| iCT regimen, n (%) | Platinum + pemetrexed, 42 (97.7) gemcitabine, 1 (2.3) | Platinum + pemetrexed, 13 (87) Platinum + gemcitabine, 2 (13) | 0.2 |
| iCT cycles, median (IQR) | 4 (4–5.25) | 4 (4–4) | 0.5 |
| CV (%), median (IQR) | 92.5 (78–106.8) | 73 (65–77) | <0.001 |
| FVC (%), median (IQR) | 92 (78–105.3) | 73 (60–75) | <0.001 |
| FEV1 (%), median (IQR) | 89 (77–102) | 77 (67–87) | 0.007 |
| TLC (%), median (IQR) | 89 (79–97) | 75 (71–80) | 0.003 |
| DLCO (%), median (IQR) | 76 (63–87) | 66 (51–77) | 0.04 |
| Scintigraphy scan, n (%) | 0.3 | ||
| No | 10 (23) | 6 (40) | |
| Ventilation/Perfusion | 30 (70) | 9 (60) | |
| Perfusion only | 3 (7) | 0 (0) | |
| Ipsilateral lung perfusion (%), median (IQR) | 37.76 (32.57–45.88) | 34.05 (19.62–38.86) | 0.08 |
| Ipsilateral lung ventilation (%), median (IQR) | 33.31 (25–44.88) | 28.4 (9.92–35.34) | 0.07 |
| Post-induction PET/CT, n (%) | 0.2 | ||
| No | 11 (26) | 3 (20) | |
| Negative/reduced | 16 (37) | 3 (20) | |
| Stable/augmented | 16 (37) | 9 (60) | |
| Preoperative SUV max, median (IQR) | 7.58 (2.53–11.23) | 7.95 (5.99–11.52) | 0.3 |
| Talc pleurodesis, n (%) | 0.1 | ||
| No | 12 (28) | 8 (53) | |
| Yes | 31 (72) | 7 (47) | |
| Histology, n (%) | >0.99 | ||
| Epithelial | 37 (86) | 13 (87) | |
| Non-epithelial | 6 (14) | 2 (13) | |
| cTNM8, n (%) | >0.99 | ||
| I | 34 (79) | 12 (80) | |
| II | 9 (21) | 3 (20) | |
| pTNM8, n (%) | <0.001 | ||
| Complete remission-I–II | 29 (67) | 0 (0) | |
| III–IV | 14 (33) | 15 (100%) | |
| Ipsilateral pathological lung volume (cm3), median (IQR) | 1944 (1528–2352) | 1545 (1322–1782) | 0.03 |
| Difference in contralateral and ipsilateral lung volume (cm3), median (IQR) | 677.2 (217.4–1252) | 1371 (667.4–2164) | 0.02 |
| Difference in contralateral and ipsilateral lung volume (%), median (IQR) | 25.28 (7.4–41.73) | 47.01 (28.39–59.01) | 0.01 |
| Max pleural thickness at upper level (mm), median (IQR) | 10 (5–20) | 23 (9–32) | 0.002 |
| Max pleural thickness at medium level (mm), median (IQR) | 12 (5–21) | 22 (13–35) | 0.007 |
| Max pleural thickness at inferior level (mm), median (IQR) | 13 (5–21) | 28 (17–43) | 0.005 |
| Disease burden (mm), median (IQR) | 57 (36–99) | 133 (70–181) | 0.001 |
| Patient | Sex | Side | Cause of R2 | TLC (%) | Disease Burden (mm) | Ipsilateral Lung Volume (cm3) | Difference Contralateral-Ipsilateral Lung Volume (%) |
|---|---|---|---|---|---|---|---|
| 1 | M | Right | DCWI | 88 | 241 | 1337.17 | 49.25 |
| 2 | M | Left | DCWI | 71 | 201 | 989.9 | 76.68 |
| 3 | M | Right | DCWI | 75 | 99 | 1512.07 | 59.01 |
| 4 | M | Right | DCWI | 73 | 58 | 2130.43 | 1.88 |
| 5 | M | Right | DCWI | 77 | 35 | 1584.56 | 52.92 |
| 6 | M | Left | Aortic adventitia infiltration | 86 | 183 | 2009.94 | 33.98 |
| 7 | M | Left | DCWI | 93 | 133 | 1683.51 | 28.39 |
| 8 | M | Right | DCWI | 72 | 181 | 991.43 | 75.10 |
| 9 | M | Right | DCWI | 74 | 70 | 1776.78 | 46.35 |
| 10 | M | Right | Diaphragmatic pillar infiltration | 71 | 134 | 2964.71 | −28.35 |
| 11 | M | Right | DCWI | 80 | 140 | 1545.46 | 47.01 |
| 12 | M | Left | DCWI | 56 | 162 | 711.33 | 75.26 |
| 13 | M | Right | DCWI | 75 | 89 | 1471.99 | 34.46 |
| 14 | M | Left | DCWI | 60 | 123 | 1321.67 | 55.41 |
| 15 | F | Right | DCWI | 77 | 34 | 1782.33 | 0.74 |
| Univariable | Multivariable | ||
|---|---|---|---|
| p-Value | OR (95%CI) | p-Value | |
| TLC (%) | 0.005 | 0.920 (0.853–0.992) | 0.03 |
| Ipsilateral pathological lung volume (cm3) | 0.04 | 1.000 (0.998–1.002) | 0.9 |
| Difference in contralateral and ipsilateral lung volume (%) | 0.03 | 0.995 (0.955–1.037) | 0.8 |
| Disease burden (mm) | 0.002 | 1.020 (1.003–1.038) | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, A.; Dell’Amore, A.; Giraudo, C.; Modugno, A.; Bernardinello, N.; Terzi, S.; Zambello, G.; Pasello, G.; Zuin, A.; Rea, F. Computed Tomography and Spirometry Can Predict Unresectability in Malignant Pleural Mesothelioma. J. Clin. Med. 2021, 10, 4407. https://doi.org/10.3390/jcm10194407
Bellini A, Dell’Amore A, Giraudo C, Modugno A, Bernardinello N, Terzi S, Zambello G, Pasello G, Zuin A, Rea F. Computed Tomography and Spirometry Can Predict Unresectability in Malignant Pleural Mesothelioma. Journal of Clinical Medicine. 2021; 10(19):4407. https://doi.org/10.3390/jcm10194407
Chicago/Turabian StyleBellini, Alice, Andrea Dell’Amore, Chiara Giraudo, Antonella Modugno, Nicol Bernardinello, Stefano Terzi, Giovanni Zambello, Giulia Pasello, Andrea Zuin, and Federico Rea. 2021. "Computed Tomography and Spirometry Can Predict Unresectability in Malignant Pleural Mesothelioma" Journal of Clinical Medicine 10, no. 19: 4407. https://doi.org/10.3390/jcm10194407
APA StyleBellini, A., Dell’Amore, A., Giraudo, C., Modugno, A., Bernardinello, N., Terzi, S., Zambello, G., Pasello, G., Zuin, A., & Rea, F. (2021). Computed Tomography and Spirometry Can Predict Unresectability in Malignant Pleural Mesothelioma. Journal of Clinical Medicine, 10(19), 4407. https://doi.org/10.3390/jcm10194407