
Comparison of Therapeutic Effects of Topical Calcineurin Inhibitor and Moisturizing Cream on Pruritic External Auditory Canal



Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics and Clinical Characteristics
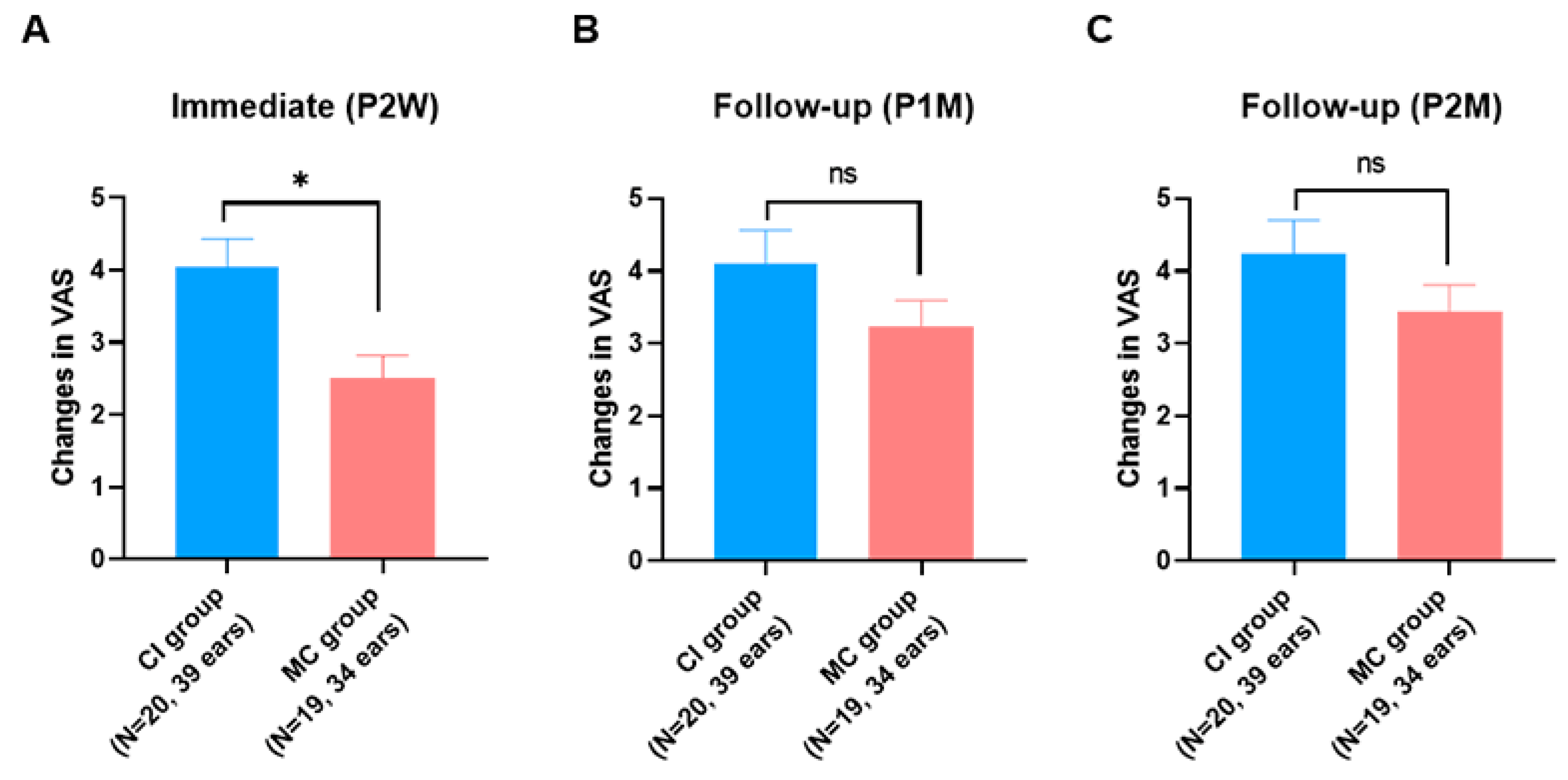
3.2. Subjective Outcomes
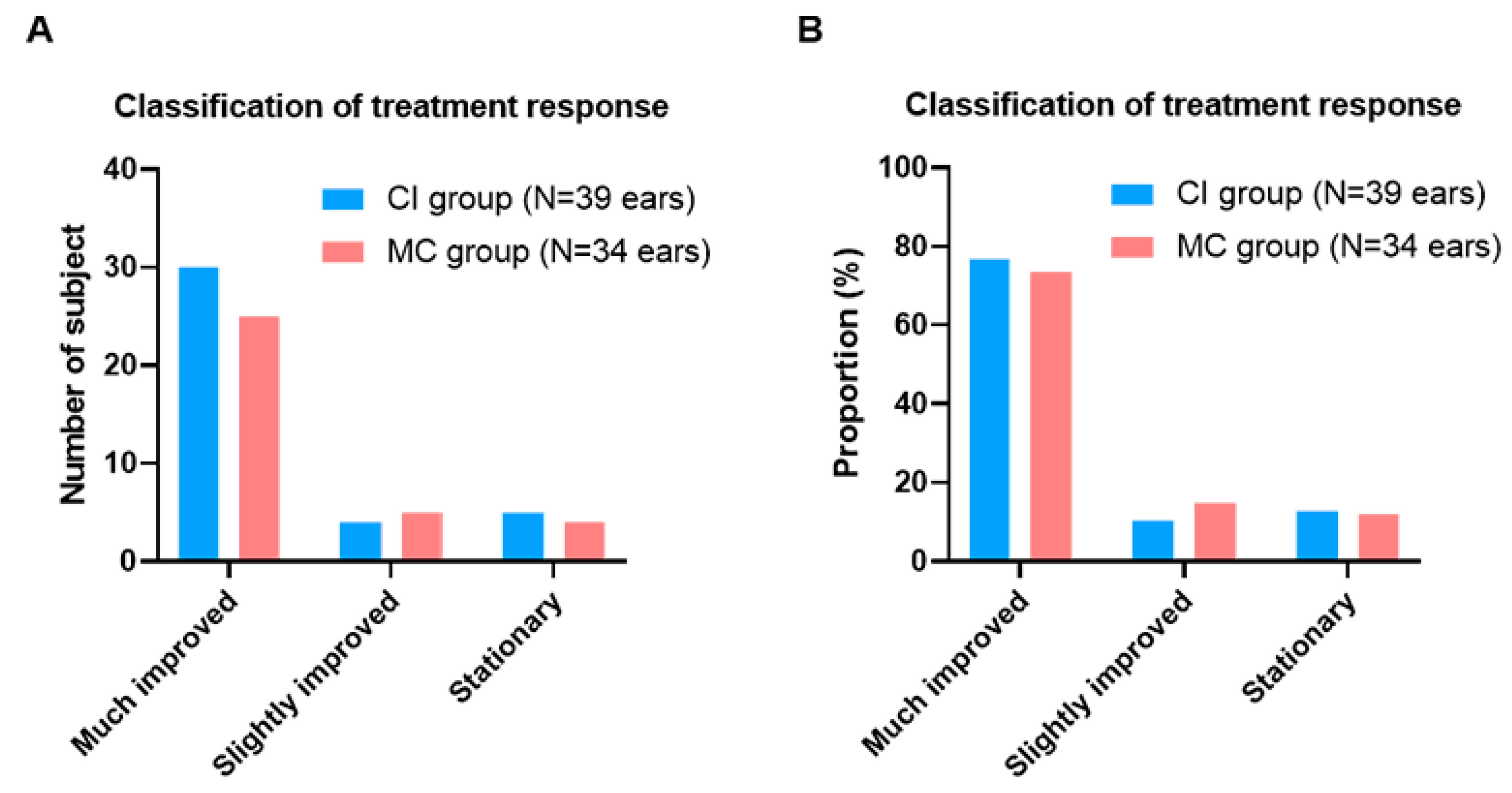
3.3. Objective Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- King, W. Allergic disorders in the otolaryngologic practice. Otolaryngol. Clin. N. Am. 1985, 18, 677–690. [Google Scholar] [CrossRef]
- Acar, B.; Simsek, G.G.; Oguztuzun, S.; Zaim, M.; Karasen, R.M. Isolated itching of external auditory canal: Clinicopathological study with immunohistochemical determination of antimicrobial peptides. J. Laryngol. Otol. 2011, 125, 227. [Google Scholar] [CrossRef]
- Kroon, D.F.; Strasnick, B. Diseases of the auricle, external auditory canal, and tympanic membrane. In Surgery of the Ear, 5th ed.; BC Decker: Hamilton, ON, Canada, 2003; pp. 345–367. [Google Scholar]
- Main, T.; Lim, D. The human external auditory canal secretory system—An ultrastructural study. Laryngoscope 1976, 86, 1164–1176. [Google Scholar] [CrossRef]
- Yoon, Y.J.; Yoon, J.; Lee, E.J.; Kim, J.S. Substance P and Calcitonin Gene-Related Peptide in the Glands of External Auditory Canal Skin. Clin. Exp. Otorhinolaryngol. 2017, 10, 321. [Google Scholar] [CrossRef]
- Mabry, R. Treatment of itching ears with fluocinolone acetonide. Eye Ear Nose Throat. Mon. 1974, 53, 333. [Google Scholar] [PubMed]
- Seftel, D.M. Itching In The Ear Canal Due To Hypocerumenosis—An Effective Method of Treatment. Calif. Med. 1963, 98, 151. [Google Scholar]
- Kolbe, L.; Kligman, A.M.; Schreiner, V.; Stoudemayer, T. Corticosteroid-induced atrophy and barrier impairment measured by non-invasive methods in human skin. Skin Res. Technol. 2001, 7, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Cevik, C.; Kaya, O.A.; Akbay, E.; Yula, E.; Yengil, E.; Gulmez, M.I.; Akoglu, E. Investigation of demodex species frequency in patients with a persistent itchy ear canal treated with a local steroid. J. Laryngol Otol. 2014, 128, 698–701. [Google Scholar] [CrossRef]
- Tuzuner, A.; Akdagli, S.; Sen, T.; Demirci, S.; Tarimci, N.; Caylan, R. An objective analysis of sebum, pH and moisture levels of the external ear canal skin. Am. J. Otolaryngol. 2015, 36, 424–428. [Google Scholar] [CrossRef]
- Karakuş, M.F.; Arda, H.N.; Ikincioğullari, A.; Gedikli, Y.; Coşkun, S.; Balaban, N.; Akdoğan, O. Microbiology of the external auditory canal in patients with asteatosis and itching. Kulak Burun Bogaz Ihtis. Dergisi KBB J. Ear Nose Throat 2003, 11, 33–38. [Google Scholar]
- Djalilia, H.R.; Memar, O. Topical pimecrolimus 1% for the treatment of pruritic external auditory canals. Laryngoscope 2006, 116, 1809–1812. [Google Scholar] [CrossRef] [PubMed]
- Marsland, A.M.; Griffiths, C. The macrolide immunosuppressants in dermatology: Mechanisms of action. Eur. J. Dermatol. EJD 2002, 12, 618–622. [Google Scholar]
- Acar, B.; Karadag, A.S.; Karabulut, H.; Babademez, M.A.; Zaim, M.; Karasen, R.M.; Djalilian, H.; Memar, O.; Acar, B.; Karabulut, H. Evaluation of contact sensitivity in patients with isolated itching of the external auditory canal. J. Otolaryngol. Head Neck Surg. 2011, 40, 187. [Google Scholar] [PubMed]
- Acar, B.; Karabulut, H.; Sahin, Y.; Babademez, M.; Karadag, A.; Karasen, R. New treatment strategy and assessment questionnaire for external auditory canal pruritis: Topical pimecrolimus therapy and Modified Itch Severity Scale. J. Laryngol. Otol. 2010, 124, 147. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Babakurban, S.T.; Topal, O.; Aydin, E.; Hizal, E.; Copur, S.; Ekici, M.D. Therapeutic effect of Castellani’s paint in patients with an itchy ear canal. J. Laryngol. Otol. 2016, 130, 934. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Triviño, F.J.; Ruiz-Villaverde, R. Successful treatment of erythematous-squamous disorders of the external auditory canal with tacrolimus and clotrimazole in otic oil: Our experience in 25 patients. Dermatol. Ther. 2020, 36, e14471. [Google Scholar] [CrossRef]
- Pilkington, S.M.; Bulfone-Paus, S.; Griffiths, C.E.; Watson, R.E. Inflammaging and the Skin. J. Investig. Dermatol. 2021, 141, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- Freund, A.; Orjalo, A.V.; Desprez, P.-Y.; Campisi, J. Inflammatory networks during cellular senescence: Causes and consequences. Trends Mol. Med. 2010, 16, 238–246. [Google Scholar] [CrossRef]
- Okazaki, M.; Yoshimura, K.; Uchida, G.; Harii, K. Correlation between age and the secretions of melanocyte-stimulating cytokines in cultured keratinocytes and fibroblasts. Br. J. Dermatol. 2005, 153, 23–29. [Google Scholar] [CrossRef]
- Bhushan, M.; Cumberbatch, M.; Dearman, R.; Andrew, S.; Kimber, I.; Griffiths, C. Tumour necrosis factor-α-induced migration of human Langerhans cells: The influence of ageing. Br. J. Dermatol. 2002, 146, 32–40. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, T.-G.; Kim, S.H.; Park, J.Y.; Lee, M.; Lee, J.W.; Lee, S.H.; Lee, M.-G. Epidermal barrier function is impaired in langerhans cell-depleted mice. J. Invest. Dermatol. 2019, 139, 1182–1185. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, G.; Di Bona, D.; Belluzzo, F.; Macchia, L. Immunological and non-immunological mechanisms of allergic diseases in the elderly: Biological and clinical characteristics. Immun. Ag. 2017, 14, 1–8. [Google Scholar] [CrossRef]
- Howell, A.N.; Ghamrawi, R.I.; Strowd, L.C.; Feldman, S.R. Pharmacological management of atopic dermatitis in the elderly. Exp. Op. Pharmacother. 2020, 21, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Pawliczak, R. Efficacy and safety of topical calcineurin inhibitors for the treatment of atopic dermatitis: Meta-analysis of randomized clinical trials. Adv. Dermatol. Allergol. Post. Dermatol. Alergol. 2019, 36, 752. [Google Scholar]
- Billich, A.; Aschauer, H.; Aszódi, A.; Stuetz, A. Percutaneous absorption of drugs used in atopic eczema: Pimecrolimus permeates less through skin than corticosteroids and tacrolimus. Int. J. Pharm. 2004, 269, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Kelly, K.E.; Mohs, D.C. The external auditory canal: Anatomy and physiology. Otolaryngol. Clin. North Am. 1996, 29, 725–739. [Google Scholar] [CrossRef]
- Kurban, R.S.; Bhawan, J. Histologic changes in skin associated with aging. J. Dermatol. Surg. Oncol. 1990, 16, 908–914. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Topical Calcineurine Inhibitor Group (n = 20, 39 Ears) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subject | Age | Sex | Laterality | Culture | Total Ig E | MAST | Underlying Disease | Previous Itchy Ear Treatment | Intial VAS (R) | Intial VAS (L) | P2W VAS (R) | P2W VAS (L) | P1M VAS (R) | P1M VAS (L) | P2M VAS (R) | P2M VAS (L) |
| 1 | 69 | M | B | NG | 40.8 | Negative | HTN | Steroid otic drop | 10 | 10 | 5 | 5 | 2 | 2 | 2 | 2 |
| 2 | 46 | M | B | NG | 961 | DF (class 2), Cladosporium (class 1) | Angina | Antihistamine (oral) | 7 | 4 | 1 | 1 | 0 | 0 | 0 | 0 |
| 3 | 65 | M | B | NG | 20.5 | DF (class1) | - | Steroid otic drop | 4 | 6 | 4 | 6 | 6 | 7 | 7 | 7 |
| 4 | 64 | F | B | NG | 17 | Negative | HTN | - | 10 | 10 | 3 | 3 | 1 | 1 | 2 | 1 |
| 5 | 81 | M | B | NG | <2 | Negative | Angina | Vinegar irrigation | 5 | 5 | 2 | 2 | 2 | 2 | 2 | 2 |
| 6 | 90 | M | L | NG | 7.63 | Negative | HTN, BPH | - | 0 | 7 | 0 | 6 | 0 | 6 | 0 | 6 |
| 7 | 80 | F | B | NG | 21.7 | Negative | Dementia | - | 8 | 10 | 2 | 1 | 2 | 1 | 2 | 1 |
| 8 | 85 | F | B | NG | 12.3 | Negative | - | Antibiotics Otic drop | 8 | 5 | 5 | 3 | 3 | 3 | 2 | 2 |
| 9 | 74 | M | B | NG | 236 | Negative | - | - | 6 | 6 | 2 | 1 | 1 | 1 | 0 | 0 |
| 10 | 49 | F | B | NG | 42.8 | DP (class 1) | - | - | 5 | 5 | 3 | 3 | 0 | 0 | 0 | 0 |
| 11 | 68 | M | B | NG | 84.9 | Negative | HTN, Arrythmia | Topical steroid oint | 10 | 10 | 1 | 1 | 3 | 3 | 2 | 2 |
| 12 | 52 | F | B | NG | 130 | Positive control > 100 | - | - | 6 | 2 | 2 | 0 | 6 | 1 | 6 | 1 |
| 13 | 61 | F | B | NG | 393 | DP/DF (class 2/3) | HTN | - | 5 | 8 | 3 | 6 | 2 | 2 | 2 | 2 |
| 14 | 57 | F | B | NG | 36 | Negative | HTN | Topical steroid oint | 10 | 10 | 3 | 3 | 4 | 4 | 7 | 7 |
| 15 | 64 | F | B | NG | <2 | Positive control > 100 | HTN, DM (on insulin) | - | 8 | 5 | 5 | 0 | 5 | 0 | 5 | 0 |
| 16 | 78 | M | B | NG | 1160 | DF (class 2) | HTN | - | 5 | 5 | 2 | 2 | 2 | 2 | 2 | 2 |
| 17 | 45 | F | B | NG | 22.3 | Negative | HTN | Antihistamine (oral) | 8 | 7 | 2 | 1 | 1 | 2 | 1 | 1 |
| 18 | 79 | F | B | NG | 31.8 | Japanese hop (class 1) | HTN | - | 6 | 6 | 2 | 2 | 3 | 3 | 3 | 3 |
| 19 | 78 | M | B | NG | 10 | Negative | BPH | Topical steroid oint | 10 | 10 | 8 | 8 | 10 | 10 | 10 | 10 |
| 20 | 71 | M | B | NG | 160.7 | Negative | HTN | Vinegar irrigation | 6 | 6 | 4 | 3 | 4 | 3 | 3 | 2 |
| Topical moisturizing cream group (n = 19, 34 ears) | ||||||||||||||||
| Subject | Age | Sex | Laterality | Culture | Total Ig E | MAST | Underlying disease | Previous itchy ear treatment | intial VAS (Rt.) | intial VAS (Lt.) | P2W VAS (Rt.) | P2W VAS (Lt.) | P1M VAS (Rt.) | P1M VAS (Lt.) | P2M VAS (Rt.) | P2M VAS (Lt.) |
| 1 | 54 | M | L | NG | 39.1 | Negative | HTN, DM (on insulin) | Antihistamine (oral) | NA | 9 | 0 | 3 | 0 | 4 | 0 | 4 |
| 2 | 63 | F | B | NG | 23.9 | Negative | Ovarian cancer | - | 5 | 7 | 2 | 5 | 1 | 2 | 1 | 2 |
| 3 | 82 | M | B | NG | <2 | Negative | HTN | Steroid otic drop | 9 | 1 | 9 | 1 | 9 | 1 | 9 | 1 |
| 4 | 58 | F | L | NG | 4.84 | Negative | - | - | 0 | 6 | 0 | 5 | 0 | 0 | 0 | 0 |
| 5 | 55 | F | B | NG | 10.8 | DF (class 1) | - | - | 5 | 5 | 3 | 3 | 2 | 2 | 1 | 1 |
| 6 | 69 | F | B | NG | 53.2 | Negative | - | Topical steroid oint | 3 | 3 | 1 | 1 | 0 | 0 | 0 | 0 |
| 7 | 31 | M | B | NG | 102 | cat (class 4) dog (class 2) | - | Antibiotics otic drop Antihistamine (oral) | 7 | 7 | 7 | 7 | 7 | 7 | 7 | 7 |
| 8 | 64 | F | B | NG | 115 | DP/DF (class 1/1) | - | Steroid otic drop | 10 | 10 | 4 | 4 | 6 | 6 | 6 | 6 |
| 9 | 63 | F | B | NG | 94.3 | Negative | - | - | 5 | 5 | 3 | 3 | 1 | 1 | 1 | 1 |
| 10 | 69 | M | B | NG | <2 | Negative | HTN | Vinegar irrigation | 2 | 4 | 1 | 3 | 1 | 1 | 1 | 1 |
| 11 | 55 | F | B | NG | 18.3 | Negative | HTN | - | 5 | 5 | 2 | 2 | 4 | 4 | 4 | 4 |
| 12 | 64 | F | R | NG | 9.97 | Negative | HTN | Topical steroid oint | 8 | 0 | 2 | 0 | 0 | 0 | 0 | 0 |
| 13 | 63 | F | B | NG | 85.1 | Negative | HTN | - | 4 | 8 | 3 | 5 | 3 | 4 | 2 | 2 |
| 14 | 59 | F | R | NG | 59.7 | Negative | - | Topical steroid oint | 8 | 0 | 5 | 0 | 6 | 0 | 6 | 0 |
| 15 | 70 | F | B | NG | 3.32 | Negative | - | 2 | 7 | 0 | 4 | 0 | 1 | 0 | 0 | |
| 16 | 75 | F | B | NG | 21.8 | Negative | - | Steroid otic drop | 6 | 6 | 4 | 4 | 3 | 3 | 2 | 2 |
| 17 | 57 | F | B | NG | 29 | Negative | - | - | 3 | 6 | 1 | 3 | 1 | 3 | 1 | 3 |
| 18 | 80 | M | B | NG | 83.9 | Negative | HTN, BPH, Angina | - | 4 | 8 | 3 | 7 | 1 | 1 | 1 | 2 |
| 19 | 69 | F | B | NG | 19.5 | DP/DF (class 1/1) | HTN | Vinegar irrigation Antihistamine (oral) | 7 | 9 | 1 | 3 | 1 | 3 | 1 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-Y.; Cho, S.; Kim, M.; Lee, D.-H.; Kim, Y.H. Comparison of Therapeutic Effects of Topical Calcineurin Inhibitor and Moisturizing Cream on Pruritic External Auditory Canal. J. Clin. Med. 2021, 10, 4313. https://doi.org/10.3390/jcm10194313
Lee S-Y, Cho S, Kim M, Lee D-H, Kim YH. Comparison of Therapeutic Effects of Topical Calcineurin Inhibitor and Moisturizing Cream on Pruritic External Auditory Canal. Journal of Clinical Medicine. 2021; 10(19):4313. https://doi.org/10.3390/jcm10194313
Chicago/Turabian StyleLee, Sang-Yeon, Soyun Cho, Minju Kim, Dong-Han Lee, and Young Ho Kim. 2021. "Comparison of Therapeutic Effects of Topical Calcineurin Inhibitor and Moisturizing Cream on Pruritic External Auditory Canal" Journal of Clinical Medicine 10, no. 19: 4313. https://doi.org/10.3390/jcm10194313
APA StyleLee, S.-Y., Cho, S., Kim, M., Lee, D.-H., & Kim, Y. H. (2021). Comparison of Therapeutic Effects of Topical Calcineurin Inhibitor and Moisturizing Cream on Pruritic External Auditory Canal. Journal of Clinical Medicine, 10(19), 4313. https://doi.org/10.3390/jcm10194313