
SARS-CoV-2 and the Brain: What Do We Know about the Causality of ‘Cognitive COVID?

 , , ,
, , , 
{kind=link}
Abstract
:1. Introduction
2. History of Cognitive Impairment in Previous Major Coronavirus Outbreaks and Other Classical Infectious Diseases
3. Brief Review of Manifestation of Acute and Long-Term Cognitive Deficits
4. Causality
4.1. Neurotropism and the ACE2 Receptor
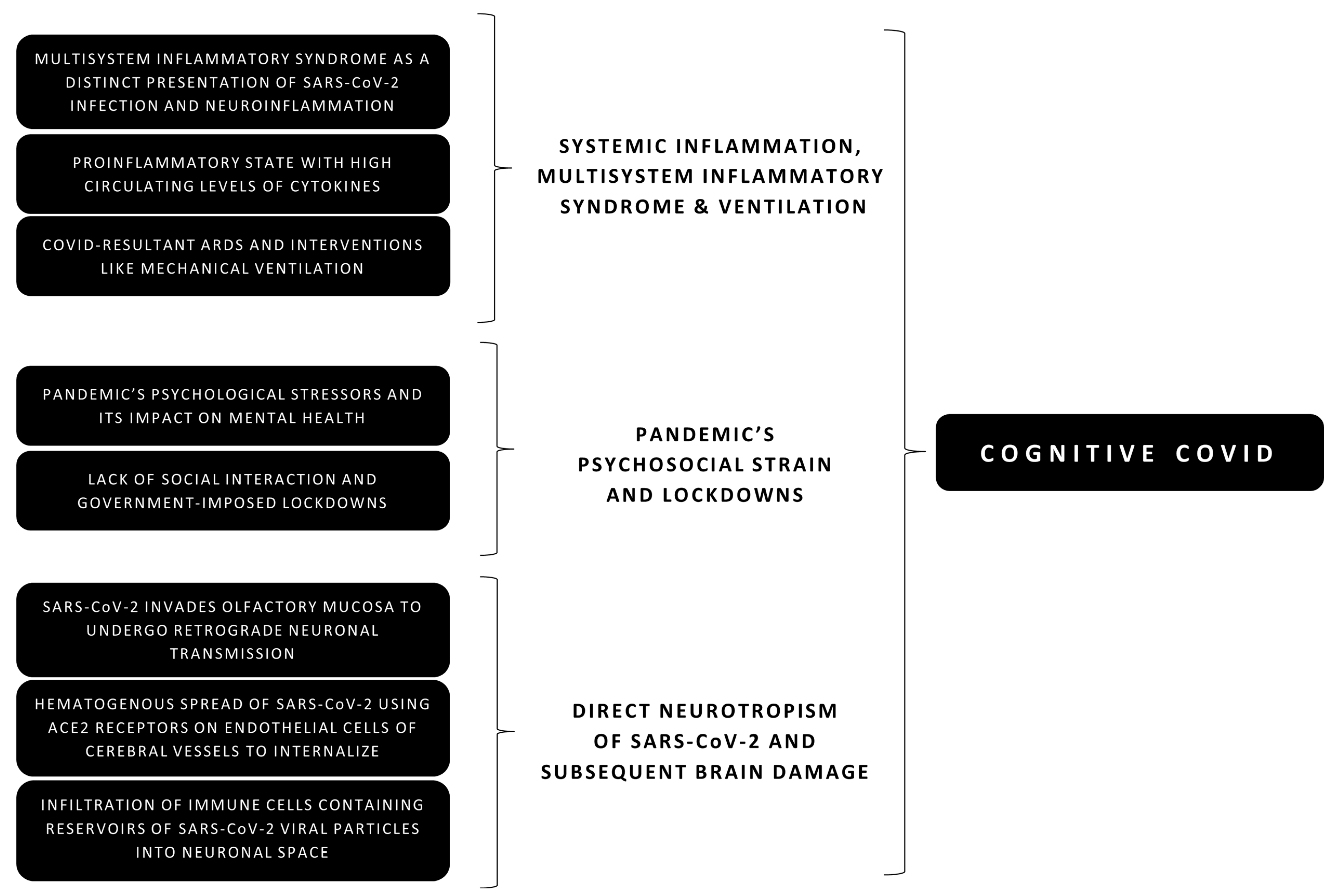
- Olfactory invasion: There is emerging evidence of SARS-CoV-2 affecting the olfactory and gustatory sensations, producing well-known symptoms of ‘loss of taste and smell’ in infected individuals [44,45,46]. With time, evidence has surfaced supporting the pathobiology of olfactory and gustatory dysfunction because of a direct invasion of the mucosal epithelium and olfactory bulb [47]. The invasion can potentially be attributed to their expression of the ACE2 surface receptor and Transmembrane Protease Serine 2 (TMPRSS2), cleaving the spike protein of SARS-CoV-2 and facilitating the fusion of SARS-CoV-2 with cellular membranes [48,49]. Furthermore, having a genome that is 79% similar to that of SARS-CoV, the spike glycoprotein of SARS-CoV-2 also binds to Angiotensin-Converting Enzyme 2 (ACE2) receptor on multiple organs, including the brain, acting as the viral functional receptor [50,51]. However, SARS-CoV-2 binds to ACE2 receptors with a considerably greater affinity than SARS-CoV [52]. Animal studies focusing on SARS-CoV have shown trans-neuronal spread from the olfactory bulb to certain ‘connected’ regions of the brain, providing key ‘circumstantial evidence’ in the potential neurotropic properties of SARS-CoV-2, as well [43,53]. The entorhinal cortex and the hippocampus are such ‘connected’ regions. They are involved in episodic memory and other domains, illustrating how damage directed at these areas may cause lasting cognitive dysfunction [54].
- Hematogenous spread: Some authors [8] claim hematogenous spread via the cerebral vasculature plays a more critical role in direct brain entry and damage-causing cognitive deficits in COVID-19. Evidence of SARS-CoV-2’s presence in blood samples of some confirmed COVID-19 patients exists. As many as 41% [55] of the samples showed viremia [43], showcasing the ability of the virus to easily reach the brain once the blood-brain barrier (BBB) is damaged. The distribution of SARS-CoV-2’s functional (ACE2) receptor is widespread in endothelial cells and pericytes throughout the body [56]. Analysis of available genomic databases confirms noteworthy expression of the receptor in neuronal and glial tissues of the CNS [56]. Consequently, the nervous tissue is potentially vulnerable if the virus comes in direct contact and interacts with the ACE2 receptors. In addition, SARS-CoV-2’s potential neurotropic properties may allow it to assume latency inside neuronal tissue of patients even after recovery from COVID-19, putting them at greater risk of long-term or delayed cognitive deficits and neurological symptoms [6]. Notably, it is still unclear how abundantly ACE2 receptors are expressed in the cerebral vasculature. However, other docking receptors, importantly basigin (BSG) and neuropilin (NRP1), have been identified as facilitators of the viral entry or internalization—making the brain vulnerable to viral inflammation even with an intact BBB [7] In addition, SARS-CoV-2 and the accompanying inflammatory cytokines, including Interleukins (IL) and Tumor Necrosis Factor (TNF), may damage the BBB [57]. Moreover, evidence shows that SARS-CoV-2 affects vasculature integrity by direct viral infection, leading to endothelium damage and increased vascular permeability in peripheral vessels [58]; extrapolated from the cerebral endothelial cells, this could explain the disruption of the BBB. Therefore, immune-mediated action or direct inflammation may be responsible for endothelial dysfunction in the BBB, enabled by the recruitment of host immune cells. Additional factors that may aid in the hematogenous spread of SARS-CoV-2 to the brain include a pre-existing or underlying neurological pathology and entry via circumventricular organs such as the median eminence of the hypothalamus [7].
- Infiltration of infected cells: A 2005 study aimed at SARS-CoV found a sizeable proportion of immune cells (29.7% of monocytes and 51.5% of lymphocytes) in 6 out of 22 patients to contain viral particles [59], signaling their potential as a reservoir for the virus. If immune cells were to infiltrate the neuronal space by crossing the BBB, this would allow the viral particles in them to cause direct brain damage by binding to ACE2 receptors on neuronal and glial cells [7]. However, whether these findings can be accurately extrapolated to SARS-CoV-2 remains yet to be ascertained. In addition, autopsies and studies conducted on samples obtained from infected individuals have been inconclusive about direct immune cell infiltration during COVID-19 [60].
4.2. Non-Specific Systemic Inflammation, Multisystem Inflammatory Syndrome (MIS), and ARDS
- Widespread systemic inflammation: A significant increase in inflammatory cytokines plays a role in SARS symptoms, with inflammation persisting even after the viral clearance, and a similar ramped up an innate immune response in the form of ‘cytokine storm’ is behind COVID-19 as well [16,34,61]. Highly circulating amounts of Interleukins and other mediators (including IL-6, IL-1β, and TNF, and others) resulting in a pro-inflammatory status are commonly found in COVID-19 patients [62,63]. This amplified immune response may cause increased vascular permeability and vasculopathy arising from disseminated intravascular coagulation (DIC). Subsequently, the BBB is compromised, allowing cytokines to activate a microglial inflammatory response [64]. This mechanism may potentially lead to delirium and seizures due to an immune-mediated encephalopathy [6]. There is a substantial risk of Cerebral Vascular Disease in infected individuals potentially due to this exact pathophysiology, with studies showing increased incidences of hypoxic-ischemic conditions [8]. A study in April 2020 investigated the histopathological changes during autopsy, and all 18 patients’ brain specimens depicted hypoxic changes [60]. It also drew attention to how cerebral white matter is at high risk for damage due to ischemia, manifesting as loss of vital cognitive functions during and after COVID-19 [8]. Several studies investigating Alzheimer’s Disease (AD) patients found a notable inflammation in patients showing cognitive deficits compared to the control group, indicating the link between the development of cognitive impairment and increased inflammatory molecules [65]. In addition, previous studies have highlighted the long-term detrimental effects of severe inflammation on the cognitive ability of a person, especially those already with or at high risk of developing a neurodegenerative disease [66,67,68]. A study investigated links between serum inflammatory markers and C-reactive protein (CRP) in COVID-19 patients with cognitive functions and found loss of some domains, such as sustained attention, to be significantly correlated to CRP levels in the blood [34]. In addition, previous longitudinal studies have confirmed a significant association between CRP levels and cognitive decline [69], affirming how underlying inflammation (using CRP as a marker) likely affects an individual’s cognitive functioning in the long run. Some studies have claimed the role of NLRP3 inflammasome activity in exacerbating systemic inflammation and its outcomes [16]. In addition, some proteins of SARS-CoV have shown to induce NLRP4 inflammasome activity, making it likely that SARS-CoV-2 also utilizes similar pathways to cause extensive inflammation [70]. This pathway has further been suggested to explain cognitive deficits due to high IL-1β activity in the setting of hypercapnia caused by mechanical ventilation [71].
- Multisystem Inflammatory Syndrome (MIS): Demographically, COVID-19 has been shown to cause more severe disease in adults, but increasing reports of COVID-associated Multisystem Inflammatory Syndrome (MIS) have surfaced [72,73,74]. While more prevalent in children, as MIS in children (MIS-C), it can potentially occur in adults as well (MIS-A). A meta-analysis comparing MIS-C’s clinical course to COVID-19 revealed how it can potentially lead to multi-organ failure [75]. MIS-C was also shown to have a relatively higher incidence of neurological manifestations compared to acute COVID-19 [75]. As a distinct manifestation of a SARS-CoV-2 infection even in adults [76], with a high risk of neurological symptoms, MIS warrants discussion as a potential causal factor in the development of Cognitive COVID. MIS-C is considered to cause a hyperinflammatory shock and resembles Kawasaki Disease (KD) [77] or Toxic Shock Syndrome (TSS) [78]. Several cases with serologic evidence of a SARS-CoV-2 infection reported symptoms of MIS-C such as shock, cardiac symptoms, gastrointestinal complains, and elevated markers of inflammation, particularly after it was recognized by the Centers for Disease Control and Prevention (CDC) in May 2020 [78]. The pathophysiology of MIS-C during and after a SARS-CoV-2 infection is largely unknown [78]. Generally, MIS-C is believed to cause a dysregulated immune response possibly by viral mimicry of the host and development of autoantibodies. This leads to widespread systemic inflammation that potentially has a damaging impact on multiple systems, including the neurological system [79,80,81]. Interestingly, some cases depicted a milder, ‘overlapping’ syndrome with acute COVID-19, while other cases reported MIS-C symptoms weeks after an acute infection. However, children with an active COVID-19 infection confirmed via a positive RT-PCR test form only one-third of the total MIS-C cases, with a majority showing evidence of a past infection confirmed via serological tests [80]. Jiang et al. uses epidemiological data from different countries to suggest that MIS-C is more likely caused by an acquired, albeit dysfunctional, immune response to SARS-CoV-2 instead of direct viral involvement [80]. The above discussion on widespread systemic inflammation in severe COVID-19 in adults is of value here when discussing MIS-C or MIS-A. The pathophysiology of MIS-C is also believed to involve a cytokine storm with elevated inflammatory mediators [80,82] which may ultimately lead to neurocognitive manifestations, as elucidated previously in this text.
- Acute respiratory distress syndrome (ARDS), mechanical ventilation, and associated cognitive decline: Although the exact ratio of COVID-19 patients developing severe disease and requiring hospitalization or intensive care unit (ICU) admission varies extensively, there is undoubtedly a noticeable proportion that progresses to life-threatening conditions [83]. Preliminary studies from China investigating data of more than 70 thousand patients suggested that around 19% of patients with COVID-19 develop severe or critical disease, most likely necessitating hospitalization [84]. A survey of 17 studies examining statistics of hospitalized COVID-19 patients from different regions found that one-third of all hospitalized and three-quarters of all ICU-admitted patients develop ARDS [83]. Cognitive impairment following ARDS of variable etiology is widely reported and reviewed [85]. Although severe inflammation, hemodynamic instability, and hypoxia have been indicted, the exact mechanism causing it is unknown. However, a review of studies has shown that cognitive impairment post-ARDS has a high incidence and ranges from 70–100% at hospital discharge, to 46–80% at one year after discharge, to 20% at five years after discharge [85]. In addition, an observational study in France described several ICU-admitted COVID-19 patients with complaints of ARDS developing encephalopathy manifesting as confusion and agitation [31]. According to Tzotzos et al., of the COVID-19 ICU-admitted patients who develop ARDS, more than 80% must receive mechanical ventilation [83]. Mechanical ventilation, regardless of ARDS, is associated with cognitive decline and reduced quality of life in the long run [86]. Since mechanical ventilation inextricably leads to the administration of sedatives, it is essential to note delirium and other cognitive consequences that may accompany, both in the short and long term [87]. The likelihood of a systemic inflammation playing a significant role in the development of cognitive loss compared to direct viral damage is underscored by the sparse evidence of the virus being found in the CSF [16]. Furthermore, instead of being two entirely independent processes, the neurotropism of SARS-CoV-2 and the widespread parallel inflammation may also operate in conjunction [7] and collectively lead to direct and indirect neuronal damage with cognitive deficits. Lastly, it is crucial to not trivialize non-specific but potentially key elements in developing cognitive sequelae, namely COVID-19 complications such as ARDS and subsequent mechanical ventilation [11].
4.3. The Psychosocial Strain of the Pandemic and Associated Lockdowns
- Psychological stressors: While countries battle their second or third waves, confinement due to lockdowns and the fear of one or one’s loved ones contracting COVID-19 are just some of the reasons that continue to cause an unprecedented psychological burden on people across the world [12,88]. With psychological conditions such as anxiety and depression now being recorded globally, cognitive consequences can be reasonably expected as a unique symptomatic presentation [89]. A systematic review remarked that some studies had shown the prevalence of post-traumatic stress disorder (PTSD) ranging from 7% to as high as 53.8% during the pandemic [90]. Moreover, this psychological disorder has been correlated with diminishing cognitive function, especially in the elderly [91], showing how ‘Cognitive COVID’ is possibly related to an individual’s psychological state.
- Social isolation and government-mandated lockdowns: An article published in late 2020 had reviewed the available evidence and stipulated that social distancing/isolation and lack of human interaction may have a detrimental effect on a person’s cognition [92]. Echoing these findings, a study conducted in Italy during May 2020 investigated the effects of psychological stressors as a result of isolation in the form of national lockdown as a mitigation technique on the global cognitive function of the public [93]. Findings suggested cognitive function such as barring memory deteriorated during lockdowns. Furthermore, with a greater prevalence of anxiety, depression, and other mental health changes, a significant deleterious impact on cognitive function(s) was noted in those who had lesser social interactions [93].
5. COVID-19 Vaccination, Autoimmunity, and Cognitive Impairment
6. Discussion
7. Conclusions, Limitations and Way Forward
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Nabavi, N. Long covid: How to define it and how to manage it. BMJ 2020, 370, m3489. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: What do we know about “long covid”? BMJ 2020, 370, m2815. [Google Scholar] [CrossRef]
- Jaywant, A.; Vanderlind, W.M.; Alexopoulos, G.S.; Fridman, C.B.; Perlis, R.H.; Gunning, F.M. Frequency and profile of objective cognitive deficits in hospitalized patients recovering from COVID-19. Neuropsychopharmacology 2021, 15, 1–6. [Google Scholar] [CrossRef]
- Barbosa-Silva, M.C.; Lima, M.N.; Battaglini, D.; Robba, C.; Pelosi, P.; Rocco, P.R.M.; Maron-Gutierrez, T. Infectious disease-associated encephalopathies. Crit. Care 2021, 25, 236. [Google Scholar] [CrossRef]
- Kumar, S.; Veldhuis, A.; Malhotra, T. Neuropsychiatric and cognitive sequelae of COVID-19. Front. Psychol. 2021, 12, 577529. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C.; Anrather, J.; Kamel, H. Effects of COVID-19 on the nervous system. Cell 2020, 183, 16–27.e1. [Google Scholar] [CrossRef]
- Miners, S.; Kehoe, P.G.; Love, S. Cognitive impact of COVID-19: Looking beyond the short term. Alzheimers Res. Ther. 2020, 12, 170. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A. Long-term neurological threats of COVID-19: A call to update the thinking about the outcomes of the coronavirus pandemic. Front. Neurol. 2020, 11, 308. [Google Scholar] [CrossRef]
- Uversky, V.N.; Elrashdy, F.; Aljadawi, A.; Ali, S.M.; Khan, R.H.; Redwan, E.M. Severe acute respiratory syndrome coronavirus 2 infection reaches the human nervous system: How? J. Neurosci. Res. 2020, 99, 750–777. [Google Scholar] [CrossRef] [PubMed]
- Rabinovitz, B.; Jaywant, A.; Fridman, C.B. Neuropsychological functioning in severe acute respiratory disorders caused by the coronavirus: Implications for the current COVID-19 pandemic. Clin. Neuropsychol. 2020, 34, 1453–1479. [Google Scholar] [CrossRef]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Ksiazek, T.G.; Erdman, D.; Goldsmith, C.S.; Zaki, S.R.; Peret, T.; Emery, S.; Tong, S.; Urbani, C.; Comer, J.A.; Lim, W.; et al. A novel coronavirus associated with severe acute respiratory syndrome. N. Engl. J. Med. 2003, 348, 1953–1966. [Google Scholar] [CrossRef]
- Al-Osail, A.M.; Al-Wazzah, M.J. The history and epidemiology of Middle East respiratory syndrome corona virus. Multidiscip. Respir. Med. 2017, 12, 20. [Google Scholar] [CrossRef] [Green Version]
- Ellul, M.A.; Benjamin, L.; Singh, B.; Lant, S.; Michael, B.D.; Easton, A.; Kneen, R.; Defres, S.; Sejvar, J.; Solomon, T. Neurological associations of COVID-19. Lancet Neurol. 2020, 19, 767–783. [Google Scholar] [CrossRef]
- Heneka, M.T.; Golenbock, D.; Latz, E.; Morgan, D.; Brown, R. Immediate and long-term consequences of COVID-19 infections for the development of neurological disease. Alzheimers Res. Ther. 2020, 12, 69. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Harthi, A.; Hussein, J.; Bouchama, A.; Johani, S.; Hajeer, A.H.; Saeed, B.T.; Wahbi, A.; Saedy, A.; Aldabbagh, T.; et al. Severe neurologic syndrome associated with Middle East respiratory syndrome corona virus (MERS-CoV). Infection 2015, 43, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Saad, M.; Omrani, A.; Baig, K.; Bahloul, A.; Elzein, F.; Matin, M.A.; Selim, M.A.; Al Mutairi, M.; Al Nakhli, D.; Al Aidaroos, A.Y.; et al. Clinical aspects and outcomes of 70 patients with Middle East respiratory syndrome coronavirus infection: A single-center experience in Saudi Arabia. Int. J. Infect. Dis. 2014, 29, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Kanmogne, G.D.; Fonsah, J.Y.; Umlauf, A.; Moul, J.; Doh, R.F.; Kengne, A.M.; Tang, B.; Tagny, C.T.; Nchindap, E.; Kenmogne, L.; et al. Attention/Working memory, learning and memory in adult cameroonians: Normative data, effects of HIV infection and viral genotype. J. Int. Neuropsychol. Soc. 2020, 26, 607–623. [Google Scholar] [CrossRef] [PubMed]
- Raper, J.; Kovacs-Balint, Z.; Mavigner, M.; Gumber, S.; Burke, M.W.; Habib, J.; Mattingly, C.; Fair, D.; Earl, E.; Feczko, E.; et al. Long-term alterations in brain and behavior after postnatal Zika virus infection in infant macaques. Nat. Commun. 2020, 11, 2534. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.J. Neurologic Complications of Influenza. Semin. Pediatr. Neurol. 2012, 19, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-W.; Teng, C.-K.; Tsai, Y.-S.; Wang, J.-N.; Tu, Y.-F.; Shen, C.-F.; Liu, C.-C. Influenza-associated neurological complications during 2014–2017 in Taiwan. Brain Dev. 2018, 40, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Martin, J.; Ahearn, M.A.; Osborne, C.; Moss, A.; Dempsey, A.; Dominguez, S.R.; Weinberg, A.; Messacar, K.B. Neurologic manifestations of influenza A(H3N2) infection in children during the 2016–2017 season. J. Pediatr. Infect. Dis. Soc. 2018, 9, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Ismail, H.I.M.; Teh, C.M.; Lee, Y.L. Neurologic manifestations and complications of pandemic influenza A H1N1 in Malaysian children: What have we learnt from the ordeal? Brain Dev. 2015, 37, 120–129. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.V.; McGuire, P.; Fusar-Poli, P.; Zandi, M.; Lewis, G.; David, A. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Filatov, A.; Sharma, P.; Hindi, F.; Espinosa, P.S. Neurological complications of coronavirus disease (COVID-19): Encephalopathy. Cureus 2020, 12, e7352. [Google Scholar] [CrossRef] [Green Version]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683. [Google Scholar] [CrossRef] [Green Version]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.S.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M.; et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: A UK-wide surveillance study. Lancet Psychiatry 2020, 7, 875–882. [Google Scholar] [CrossRef]
- Moriguchi, T.; Harii, N.; Goto, J.; Harada, D.; Sugawara, H.; Takamino, J.; Ueno, M.; Sakata, H.; Kondo, K.; Myose, N.; et al. A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int. J. Infect. Dis. 2020, 94, 55–58. [Google Scholar] [CrossRef]
- Ardila, A.; Lahiri, D. Executive dysfunction in COVID-19 patients. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1377–1378. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef]
- Amalakanti, S.; Arepalli, K.V.R.; Jillella, J.P. Cognitive assessment in asymptomatic COVID-19 subjects. Virusdisease 2021, 32, 146–149. [Google Scholar] [CrossRef]
- Wang, F.; Kream, R.M.; Stefano, G.B. Long-term respiratory and neurological sequelae of COVID-19. Med. Sci. Monit. 2020, 26, e928996. [Google Scholar] [CrossRef]
- Zhou, H.; Lu, S.; Chen, J.; Wei, N.; Wang, D.; Lyu, H.; Shi, C.; Hu, S. The landscape of cognitive function in recovered COVID-19 patients. J. Psychiatr. Res. 2020, 129, 98–102. [Google Scholar] [CrossRef]
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.-Y.; Huang, C.-C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral micro-structural changes in COVID-19 patients–An MRI-based 3-month follow-up study. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef]
- Woo, M.S.; Malsy, J.; Pöttgen, J.; Zai, S.S.; Ufer, F.; Hadjilaou, A.; Schmiedel, S.; Addo, M.M.; Gerloff, C.; Heesen, C.; et al. Frequent neurocognitive deficits after recovery from mild COVID-19. Brain Commun. 2020, 2, fcaa205. [Google Scholar] [CrossRef]
- Kwong, K.C.N.K.; Mehta, P.R.; Shukla, G.; Mehta, A.R. COVID-19, SARS and MERS: A neurological perspective. J. Clin. Neurosci. 2020, 77, 13–16. [Google Scholar] [CrossRef]
- Valiuddin, H.M.; Kalajdzic, A.; Rosati, J.; Boehm, K.; Hill, D. Update on neurological manifestations of SARS-CoV-2. West. J. Emerg. Med. 2020, 21, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.; Frontera, J.; Placantonakis, D.G.; Lighter, J.; Galetta, S.; Balcer, L.; Melmed, K. Cerebrospinal fluid in COVID-19: A systematic review of the literature. J. Neurol. Sci. 2021, 421, 117316. [Google Scholar] [CrossRef] [PubMed]
- Bohmwald, K.; Gálvez, N.M.S.; Ríos, M.; Kalergis, A.M. Neurologic alterations due to respiratory virus infections. Front. Cell. Neurosci. 2018, 12, 386. [Google Scholar] [CrossRef]
- Desforges, M.; Le Coupanec, A.; Dubeau, P.; Bourgouin, A.; Lajoie, L.; Dube, M.; Talbot, P.J. Human coronaviruses and other respiratory viruses: Underestimated opportunistic pathogens of the central nervous system? Viruses 2019, 12, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Zhou, Z.; Kang, H.; Li, S.; Zhao, X. Understanding the neurotropic characteristics of SARS-CoV-2: From neurological manifestations of COVID-19 to potential neurotropic mechanisms. J. Neurol. 2020, 267, 2179–2184. [Google Scholar] [CrossRef] [PubMed]
- Hornuss, D.; Lange, B.; Schröter, N.; Rieg, S.; Kern, W.; Wagner, D. Anosmia in COVID-19 patients. Clin. Microbiol. Infect. 2020, 26, 1426–1427. [Google Scholar] [CrossRef]
- Dawson, P.; Rabold, E.M.; Laws, R.L.; Conners, E.E.; Gharpure, R.; Yin, S.; Buono, S.A.; Dasu, T.; Bhattacharyya, S.; Westergaard, R.P.; et al. Loss of taste and smell as distinguishing symptoms of coronavirus disease 2019. Clin. Infect. Dis. 2020, 72, 682–685. [Google Scholar] [CrossRef]
- Mullol, J.; Alobid, I.; Mariño-Sánchez, F.; Izquierdo-Domínguez, A.; Marin, C.; Klimek, L.; Wang, D.-Y.; Liu, Z. The loss of smell and taste in the COVID-19 outbreak: A tale of many countries. Curr. Allergy Asthma Rep. 2020, 20, 61. [Google Scholar] [CrossRef]
- Mehraeen, E.; Behnezhad, F.; Salehi, M.A.; Noori, T.; Harandi, H.; SeyedAlinaghi, S. Olfactory and gustatory dysfunctions due to the coronavirus disease (COVID-19): A review of current evidence. Eur. Arch. Oto-Rhino-Laryngol. 2020, 278, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Brann, D.H.; Tsukahara, T.; Weinreb, C.; Lipovsek, M.; Berge, K.V.D.; Gong, B.; Chance, R.; Macaulay, I.C.; Chou, H.-J.; Fletcher, R.B.; et al. Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Sci. Adv. 2020, 6, eabc5801. [Google Scholar] [CrossRef]
- Dong, M.; Zhang, J.; Ma, X.; Tan, J.; Chen, L.; Liu, S.; Xin, Y.; Zhuang, L. ACE2, TMPRSS2 distribution and extrapulmonary organ injury in patients with COVID-19. Biomed. Pharmacother. 2020, 131, 110678. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. Addendum: A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nat. Cell Biol. 2020, 588, E6. [Google Scholar] [CrossRef]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.-L.; Abiona, O.; Graham, B.S.; McLellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef] [Green Version]
- Netland, J.; Meyerholz, D.K.; Moore, S.; Cassell, M.; Perlman, S. Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J. Virol. 2008, 82, 7264–7275. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, K.; Chan, D. The emergence of cognitive COVID. World Psychiatr. 2021, 20, 52–53. [Google Scholar] [CrossRef]
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Xie, G.; Lin, S.; Wang, R.; Yang, X.; et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: Retrospective cohort study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef] [Green Version]
- Baig, A.M.; Khaleeq, A.; Ali, U.; Syeda, H. Evidence of the COVID-19 virus targeting the CNS: Tissue distribution, host–virus interaction, and proposed neurotropic mechanisms. ACS Chem. Neurosci. 2020, 11, 995–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teuwen, L.-A.; Geldhof, V.; Pasut, A.; Carmeliet, P. COVID-19: The vasculature unleashed. Nat. Rev. Immunol. 2020, 20, 389–391. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Gu, J.; Gong, E.; Zhang, B.; Zheng, J.; Gao, Z.; Zhong, Y.; Zou, W.; Zhan, J.; Wang, S.; Xie, Z.; et al. Multiple organ infection and the pathogenesis of SARS. J. Exp. Med. 2005, 202, 415–424. [Google Scholar] [CrossRef]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F.; Sabeti, P. Neuropathological features of Covid-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2020, 93, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jiang, M.; Chen, X.; Montaner, L.J. Cytokine storm and leukocyte changes in mild versus severe SARS-CoV-2 infection: Review of 3939 COVID-19 patients in China and emerging pathogenesis and therapy concepts. J. Leukoc. Biol. 2020, 108, 17–41. [Google Scholar] [CrossRef]
- Anderberg, S.B.; Luther, T.; Berglund, M.; Larsson, R.; Rubertsson, S.; Lipcsey, M.; Larsson, A.; Frithiof, R.; Hultström, M. Increased levels of plasma cytokines and correlations to organ failure and 30-day mortality in critically ill Covid-19 patients. Cytokine 2021, 138, 155389. [Google Scholar] [CrossRef]
- Boldrini, M.; Canoll, P.D.; Klein, R.S. How COVID-19 affects the brain. JAMA Psychiatry 2021, 78, 682–683. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.-N.; Niu, L.-D.; Wang, Y.-J.; Cao, X.-P.; Liu, Q.; Tan, L.; Zhang, C.; Yu, J.-T. Inflammatory markers in Alzheimer’s disease and mild cognitive impairment: A meta-analysis and systematic review of 170 studies. J. Neurol. Neurosurg. Psychiatry 2019, 90, 590–598. [Google Scholar] [CrossRef]
- Iwashyna, T.J.; Ely, E.W.; Smith, D.M.; Langa, K. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA 2010, 304, 1787–1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widmann, C.N.; Heneka, M.T. Long-term cerebral consequences of sepsis. Lancet Neurol. 2014, 13, 630–636. [Google Scholar] [CrossRef]
- Chakrabarty, T.; Torres, I.J.; Bond, D.J.; Yatham, L.N. Inflammatory cytokines and cognitive functioning in early-stage bipolar I disorder. J. Affect. Disord. 2019, 245, 679–685. [Google Scholar] [CrossRef]
- Zheng, F.; Xie, W. High-sensitivity C-reactive protein and cognitive decline: The english longitudinal study of ageing. Psychol. Med. 2017, 48, 1381–1389. [Google Scholar] [CrossRef]
- Siu, K.; Yuen, K.; Castano-Rodriguez, C.; Ye, Z.; Yeung, M.; Fung, S.; Yuan, S.; Chan, C.P.; Yuen, K.-Y.; Enjuanes, L.; et al. Severe acute respiratory syndrome Coronavirus ORF3a protein activates the NLRP3 inflammasome by promoting TRAF3-dependent ubiquitination of ASC. FASEB J. 2019, 33, 8865–8877. [Google Scholar] [CrossRef]
- Ding, H.-G.; Deng, Y.-Y.; Yang, R.-Q.; Wang, Q.-S.; Jiang, W.-Q.; Han, Y.-L.; Huang, L.-Q.; Wen, M.-Y.; Zhong, W.-H.; Li, X.-S.; et al. Hypercapnia induces IL-1β overproduction via activation of NLRP3 inflammasome: Implication in cognitive impairment in hypoxemic adult rats. J. Neuroinflamm. 2018, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leon, M.P.D.; Redzepi, A.; McGrath, E.; Abdel-Haq, N.; Shawaqfeh, A.; Sethuraman, U.; Tilford, B.; Chopra, T.; Arora, H.; Ang, J.; et al. COVID-19–Associated pediatric multisystem inflammatory syndrome. J. Pediatr. Infect. Dis. Soc. 2020, 9, 407–408. [Google Scholar] [CrossRef]
- Cheung, E.W.; Zachariah, P.; Gorelik, M.; Boneparth, A.; Kernie, S.; Orange, J.S.; Milner, J.D. Multisystem inflammatory syndrome related to COVID-19 in previously healthy children and adolescents in New York City. JAMA 2020, 324, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Sadiq, M.; Aziz, O.A.; Kazmi, U.; Hyder, N.; Sarwar, M.; Sultana, N.; Bari, A.; Rashid, J. Multisystem inflammatory syndrome associated with COVID-19 in children in Pakistan. Lancet Child. Adolesc. Health 2020, 4, e36–e37. [Google Scholar] [CrossRef]
- Yasuhara, J.; Watanabe, K.; Takagi, H.; Sumitomo, N.; Kuno, T. COVID-19 and multisystem inflammatory syndrome in children: A systematic review and meta-analysis. Pediatr. Pulmonol. 2021, 56, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.B.; Schwartz, N.G.; Patel, P.; Abbo, L.; Beauchamps, L.; Balan, S.; Lee, E.H.; Paneth-Pollak, R.; Geevarughese, A.; Lash, M.K.; et al. Case series of multisystem inflammatory syndrome in adults associated with SARS-CoV-2 infection—United Kingdom and United States, March–August 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1450–1456. [Google Scholar] [CrossRef]
- Ebina-Shibuya, R.; Namkoong, H.; Shibuya, Y.; Horita, N. Multisystem inflammatory syndrome in children (MIS-C) with COVID-19: Insights from simultaneous familial Kawasaki disease cases. Int. J. Infect. Dis. 2020, 97, 371–373. [Google Scholar] [CrossRef]
- Godfred-Cato, S.; Bryant, B.; Leung, J.; Oster, M.E.; Conklin, L.; Abrams, J.; Roguski, K.; Wallace, B.; Prezzato, E.; Koumans, E.H.; et al. COVID-19–Associated multisystem inflammatory syndrome in children—United States, March–July 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1074–1080. [Google Scholar] [CrossRef]
- Diorio, C.; Henrickson, S.E.; Vella, L.A.; McNerney, K.O.; Chase, J.M.; Burudpakdee, C.; Lee, J.H.; Jasen, C.; Balamuth, F.; Barrett, D.M.; et al. Multisystem inflammatory syndrome in children and COVID-19 are distinct presentations of SARS–CoV-2. J. Clin. Investig. 2020, 130, 5967–5975. [Google Scholar] [CrossRef]
- Jiang, L.; Tang, K.; Levin, M.; Irfan, O.; Morris, S.K.; Wilson, K.; Klein, J.D.; A Bhutta, Z. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect. Dis. 2020, 20, e276–e288. [Google Scholar] [CrossRef]
- Maltezou, H.; Pavli, A.; Tsakris, A. Post-COVID syndrome: An insight on its pathogenesis. Vaccines 2021, 9, 497. [Google Scholar] [CrossRef]
- Rowley, A.H.; Shulman, S.T.; Arditi, M. Immune pathogenesis of COVID-19–related multisystem inflammatory syndrome in children. J. Clin. Investig. 2020, 130, 5619–5621. [Google Scholar] [CrossRef]
- Tzotzos, S.J.; Fischer, B.; Fischer, H.; Zeitlinger, M. Incidence of ARDS and outcomes in hospitalized patients with COVID-19: A global literature survey. Crit. Care 2020, 24, 516. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the Coronavirus disease 2019 (COVID-19) outbreak in China. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef]
- Sasannejad, C.; Ely, E.W.; Lahiri, S. Long-term cognitive impairment after acute respiratory distress syndrome: A review of clinical impact and pathophysiological mechanisms. Crit. Care 2019, 23, 352. [Google Scholar] [CrossRef] [Green Version]
- Jackson, J.C.; Hart, R.P.; Gordon, S.M.; Shintani, A.; Truman, B.; May, L.; Ely, E.W. Six-month neuropsychological outcome of medical intensive care unit patients. Crit. Care Med. 2003, 31, 1226–1234. [Google Scholar] [CrossRef]
- Girard, T.D.; Thompson, J.L.; Pandharipande, P.; Brummel, N.E.; Jackson, J.C.; Patel, M.B.; Hughes, C.G.; Chandrasekhar, R.; Pun, B.T.; Boehm, L.M.; et al. Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: A prospective cohort study. Lancet Respir. Med. 2018, 6, 213–222. [Google Scholar] [CrossRef]
- Ammar, A.; Mueller, P.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Brach, M.; Schmicker, M.; Bentlage, E.; et al. Psychological consequences of COVID-19 home confinement: The ECLB-COVID19 multicenter study. PLoS ONE 2020, 15, e0240204. [Google Scholar] [CrossRef]
- Ritchie, K.; Chan, D.; Watermeyer, T. The cognitive consequences of the COVID-19 epidemic: Collateral damage? Brain Commun. 2020, 2, fcaa069. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Qureshi, S.U.; Long, M.E.; Bradshaw, M.R.; Pyne, J.M.; Magruder, K.M.; Kimbrell, T.; Hudson, T.J.; Jawaid, A.; E Schulz, P.; E Kunik, M. Does PTSD impair cognition beyond the effect of trauma? J. Neuropsychiatry Clin. Neurosci. 2011, 23. [Google Scholar] [CrossRef] [PubMed]
- Bzdok, D.; Dunbar, R.I. The neurobiology of social distance. Trends Cogn. Sci. 2020, 24, 717–733. [Google Scholar] [CrossRef]
- Fiorenzato, E.; Zabberoni, S.; Costa, A.; Cona, G. Cognitive and mental health changes and their vulnerability factors related to COVID-19 lockdown in Italy. PLoS ONE 2021, 16, e0246204. [Google Scholar] [CrossRef]
- Drugs and Lactation Database(LactMed); National Library of Medicine(US): Bethesda, MD, USA, 2006; COVID-19 Vaccines. Available online: https://www.ncbi.nlm.nih.gov/books/NBK565969/ (accessed on 19 July 2021).
- Liu, B.D.; Ugolini, C.; Jha, P. Two Cases of Post-Moderna COVID-19 Vaccine Encephalopathy Associated With Nonconvulsive Status Epilepticus. Cureus 2021, 13, e16172. [Google Scholar] [CrossRef]
- Zavala-Jonguitud, L.F.; Pérez-García, C.C. Delirium triggered by COVID -19 vaccine in an elderly patient. Geriatr. Gerontol. Int. 2021, 21, 540. [Google Scholar] [CrossRef] [PubMed]
- Uwaydah, A.K.; Hassan, N.M.M.; Abu Ghoush, M.S.; Shahin, K.M.M. Adult multisystem inflammatory syndrome in a patient who recovered from COVID-19 postvaccination. BMJ Case Rep. 2021, 14, e242060. [Google Scholar] [CrossRef]
- Lyons-Weiler, J. Pathogenic priming likely contributes to serious and critical illness and mortality in COVID-19 via autoimmunity. J. Transl. Autoimmun. 2020, 3, 100051. [Google Scholar] [CrossRef]
- Terrando, N.; Pavlov, V.A. Editorial: Neuro-immune interactions in inflammation and autoimmunity. Front. Immunol. 2018, 9, 772. [Google Scholar] [CrossRef]
- Lal, H.; Forster, M.J. Autoimmunity and age-associated cognitive decline. Neurobiol. Aging 1988, 9, 733–742. [Google Scholar] [CrossRef]
- Mantovani, E.; Zucchella, C.; Bottiroli, S.; Federico, A.; Giugno, R.; Sandrini, G.; Chiamulera, C.; Tamburin, S. Telemedicine and virtual reality for cognitive rehabilitation: A roadmap for the COVID-19 pandemic. Front. Neurol. 2020, 11, 926. [Google Scholar] [CrossRef]
- O’Brien, M.; McNicholas, F. The use of telepsychiatry during COVID-19 and beyond. Ir. J. Psychol. Med. 2020, 37, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Fedak, K.M.; Bernal, A.; Capshaw, Z.A.; Gross, S. Applying the Bradford Hill criteria in the 21st century: How data integration has changed causal inference in molecular epidemiology. Emerg. Themes Epidemiol. 2015, 12, 14. [Google Scholar] [CrossRef] [Green Version]
- Callaway, E. Delta coronavirus variant: Scientists brace for impact. Nat. Cell Biol. 2021, 595, 17–18. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali Awan, H.; Najmuddin Diwan, M.; Aamir, A.; Ali, M.; Di Giannantonio, M.; Ullah, I.; Shoib, S.; De Berardis, D. SARS-CoV-2 and the Brain: What Do We Know about the Causality of ‘Cognitive COVID? J. Clin. Med. 2021, 10, 3441. https://doi.org/10.3390/jcm10153441
Ali Awan H, Najmuddin Diwan M, Aamir A, Ali M, Di Giannantonio M, Ullah I, Shoib S, De Berardis D. SARS-CoV-2 and the Brain: What Do We Know about the Causality of ‘Cognitive COVID? Journal of Clinical Medicine. 2021; 10(15):3441. https://doi.org/10.3390/jcm10153441
Chicago/Turabian StyleAli Awan, Hashir, Mufaddal Najmuddin Diwan, Alifiya Aamir, Muneeza Ali, Massimo Di Giannantonio, Irfan Ullah, Sheikh Shoib, and Domenico De Berardis. 2021. "SARS-CoV-2 and the Brain: What Do We Know about the Causality of ‘Cognitive COVID?" Journal of Clinical Medicine 10, no. 15: 3441. https://doi.org/10.3390/jcm10153441
APA StyleAli Awan, H., Najmuddin Diwan, M., Aamir, A., Ali, M., Di Giannantonio, M., Ullah, I., Shoib, S., & De Berardis, D. (2021). SARS-CoV-2 and the Brain: What Do We Know about the Causality of ‘Cognitive COVID? Journal of Clinical Medicine, 10(15), 3441. https://doi.org/10.3390/jcm10153441