
Airway Care Interventions for Invasively Ventilated Critically Ill Adults—A Dutch National Survey

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Survey Development and Formatting
2.3. Survey Pilot Testing
2.4. Sample
2.5. Survey Administration
2.6. Analysis Plan
2.7. Ethical Considerations
3. Results
3.1. Participants and Responses
3.2. Airway Care Practices
3.3. Heated Humidification
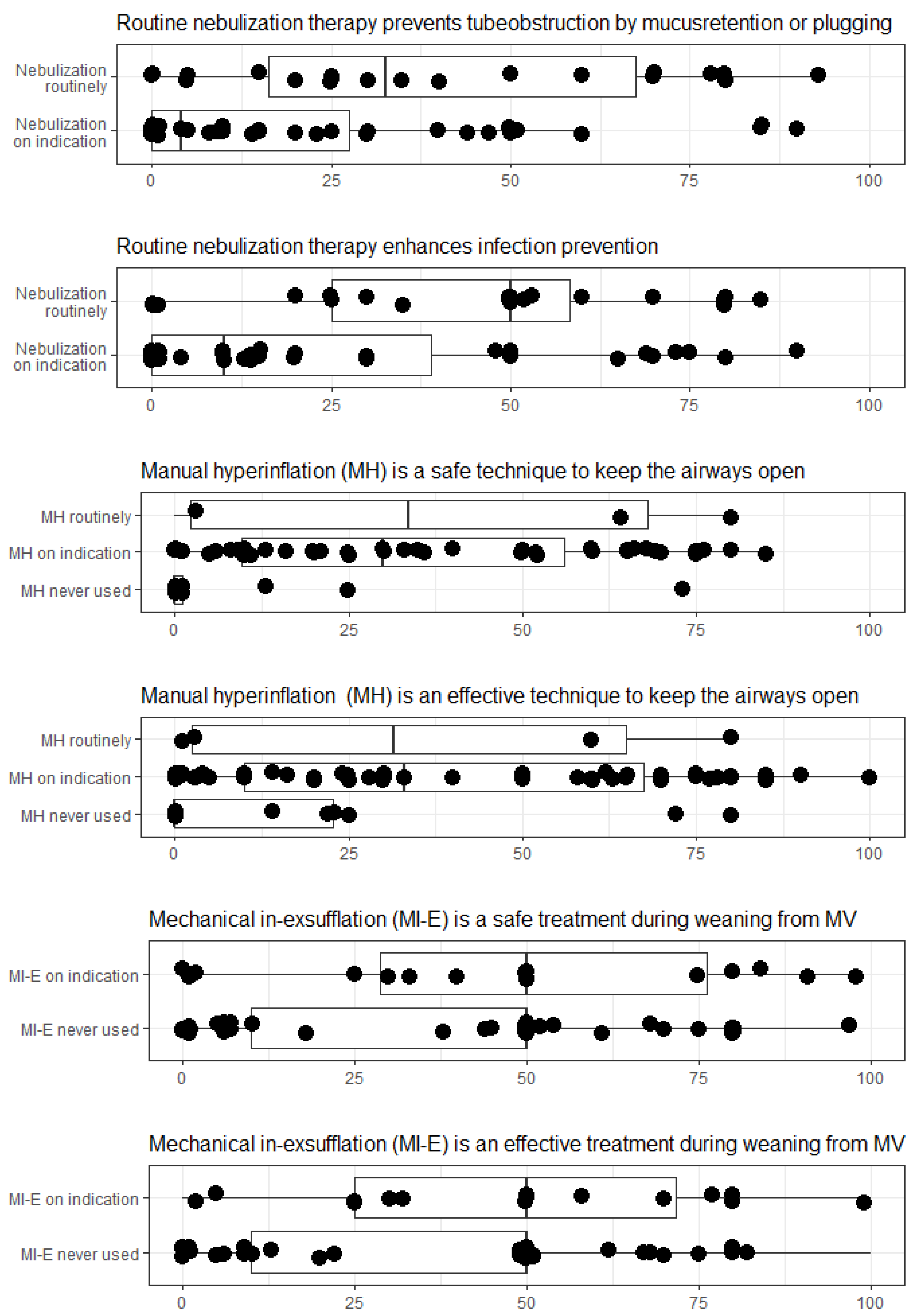
3.4. Nebulization Therapy
3.5. Manual Hyperinflation
3.6. Mechanical Insufflation-Exsufflation
3.7. Training and Education
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fahy, J.V.; Dickey, B.F. Airway Mucus Function and Dysfunction. N. Engl. J. Med. 2010, 363, 2233–2247. [Google Scholar] [CrossRef] [Green Version]
- Konrad, F.; Schreiber, T.; Brecht-Kraus, D.; Georgieff, M. Mucociliary Transport in ICU Patients. Chest 1994, 105, 237–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restrepo, R.D.; Walsh, B.K.; American Association for Respiratory Care. Humidification during invasive and noninvasive mechanical ventilation. Respir. Care 2012, 57, 782–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konrad, F.; Schoenberg, M.H.; Wiedmann, H.; Kilian, J.; Georgieff, M. The application of n-acetylcysteine as an antioxidant and mucolytic in mechanical ventilation in intensive care patients. A prospective, randomized, placebo-controlled, double-blind study. Der. Anaesthesist 1995, 44, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Ehrmann, S.; Roche-Campo, F.; Papa, G.F.S.; Isabey, D.; Brochard, L.; Apiou-Sbirlea, G.; For the REVA Research Network. Aerosol therapy during mechanical ventilation: An international survey. Intensiv. Care Med. 2013, 39, 1048–1056. [Google Scholar] [CrossRef]
- Grivans, C.; Lindgren, S.; Aneman, A.; Stenqvist, O.; Lundin, S. A Scandinavian survey of drug administration through inhalation, suctioning and recruitment maneuvers in mechanically ventilated patients. Acta Anaesthesiol. Scand. 2009, 53, 710–716. [Google Scholar] [CrossRef]
- Zhang, Z.; Xu, P.; Fang, Q.; Ma, P.; Lin, H.; Fink, J.B.; Liang, Z.; Chen, R.; Ge, H.; China Union of Respiratory Care (CURC). Practice pattern of aerosol therapy among patients undergoing mechanical ventilation in mainland China: A web-based survey involving 447 hospitals. PLoS ONE 2019, 14, e0221577. [Google Scholar] [CrossRef] [Green Version]
- Ntoumenopoulos, G.; Hammond, N.; Watts, N.R.; Thompson, K.; Hanlon, G.; Paratz, J.D.; Thomas, P. Secretion clearance strategies in Australian and New Zealand Intensive Care Units. Aust. Crit. Care 2018, 31, 191–196. [Google Scholar] [CrossRef]
- Paulus, F.; Binnekade, J.M.; Middelhoek, P.; Schuitz, M.J.; Vroom, M.B. Manual hyperinflation of intubated and mechanically ventilated patients in Dutch intensive care units—A survey into current practice and knowledge. Intensiv. Crit. Care Nurs. 2009, 25, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Paulus, F.; Binnekade, J.M.; Vroom, M.B.; Schultz, M.J. Benefits and risks of manual hyperinflation in intubated and mechanically ventilated intensive care unit patients: A systematic review. Crit. Care 2012, 16, R145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach, J.R. Mechanical insufflation-exsufflation: Comparison of peak expiratory flows with manually assisted and unassisted coughing techniques. Chest 1993, 104, 1553–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, L.; Adhikari, N.K.; Leasa, D.; A Fergusson, D.; McKim, D. Cough augmentation techniques for extubation and weaning critically ill patients from mechanical ventilation. Cochrane Database Syst. Rev. 2015, 1:CD011833. [Google Scholar] [CrossRef]
- Gillies, D.; A Todd, D.; Foster, J.P.; Batuwitage, B.T. Heat and moisture exchangers versus heated humidifiers for mechanically ventilated adults and children. Cochrane Database Syst. Rev. 2017, 2017, CD004711. [Google Scholar] [CrossRef] [PubMed]
- van Meenen, D.M.P.; van der Hoeven, S.M.; Binnekade, J.M. Effect of On-Demand vs Routine Nebulization of Acetylcysteine With Salbutamol on Ventilator-Free Days in Intensive Care Unit Patients Receiving Invasive Ventilation: A Randomized Clinical Trial. JAMA 2018, 319, 993–1001. [Google Scholar] [CrossRef] [Green Version]
- American Association for Respiratory Care. AARC Clinical Practice Guidelines. Endotracheal suctioning of mechanically ventilated patients with artificial airways. Respir Care 2010, 55, 758–764. [Google Scholar]
- Strickland, S.L.; Rubin, B.K.; Drescher, G.S.; Haas, C.F.; O’Malley, C.A.; Volsko, T.A.; Branson, R.D.; Hess, D.R. AARC Clinical Practice Guideline: Effectiveness of Nonpharmacologic Airway Clearance Therapies in Hospitalized Patients. Respir. Care 2013, 58, 2187–2193. [Google Scholar] [CrossRef] [Green Version]
- Rose, L.; Adhikari, N.K.; Poon., J.; Leasa, D.; McKim, D.A.; Group, C.A. Cough Augmentation Techniques in the Critically Ill: A Canadian National Survey. Respir Care 2016, 61, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- SurveyMonkey Audience hnsc. Momentive Inc. Location: San Mateo, California, USA. Available online: www.surveymonkey.com/mp/audience (accessed on 26 May 2021).
- Burns, K.E.; Duffett, M.; Kho, M.; Meade, M.O.; Adhikari, N.K.; Sinuff, T.; Cook, D.J.; for the ACCADEMY Group. A guide for the design and conduct of self-administered surveys of clinicians. Can. Med Assoc. J. 2008, 179, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engle, S.; Whalen, S.; Joshi, A.; Pollard, K.S. Unboxing cluster heatmaps. BMC Bioinform. 2017, 18, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- RC Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: https://www.R-project.org/ (accessed on 26 May 2021).
- Cook, D.; Ricard, J.-D.; Reeve, B.; Randall, J.; Wigg, M.; Brochard, L.; Dreyfuss, D. Ventilator circuit and secretion management strategies: A Franco-Canadian survey. Crit. Care Med. 2000, 28, 3547–3554. [Google Scholar] [CrossRef] [PubMed]
- Menegueti, M.G.; Auxiliadora-Martins, M.; Nunes, A.A. Cost-Effectiveness Analysis of Heat and Moisture Exchangers in Mechanically Ventilated Critically Ill Patients. Anesthesiol. Pain Med. 2016, 6, ee32602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargas, M.; Chiumello, D.; Sutherasan, Y.; Ball, L.; Esquinas, A.M.; Pelosi, P.; Servillo, G. Heat and moisture exchangers (HMEs) and heated humidifiers (HHs) in adult critically ill patients: A systematic review, meta-analysis and meta-regression of randomized controlled trials. Crit. Care 2017, 21, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucci, M.R.; Nakamura, M.A.; Carvalho, N.C.; Volpe, M.S. Manual Hyperinflation: Is It Effective? (editorial). Respir Care 2019, 64, 870–873. [Google Scholar] [CrossRef] [PubMed]
- Paulus, F.; Binnekade, J.M.; Middelhoek, P.; Vroom, M.B.; Schultz, M.J. Performance of manual hyperinflation: A skills lab study among trained intensive care unit nurses. Med Sci. Monit. 2009, 15, CR418–CR422. [Google Scholar] [PubMed]
- Swingwood, E.; Tume, L.; Cramp, F. A survey examining the use of mechanical insufflation-exsufflation on adult intensive care units across the UK. J. Intensiv. Care Soc. 2020, 21, 283–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Respondent | |
| ICU nurse | 31 (43) |
| Advanced ventilation nurse specialist * | 35 (49) |
| Intensivist | 6 (8) |
| Hospital type | |
| Academic | 6 (8) |
| Teaching † | 32 (44) |
| General | 34 (47) |
| ICU beds available for invasive ventilation | |
| 3–5 | 10 (14) |
| 6–10 | 16 (22) |
| 11–20 | 20 (28) |
| 21–30 | 21 (29) |
| >30 | 5 (7) |
| Characteristics | n (%) | ||
|---|---|---|---|
| Nebulization therapy | |||
| Practice of use | N = 72 | ||
| routine use | 31 (43) | ||
| as treatment on indication | 41 (57) | ||
| never used | 0 | ||
| Indications for use * | Bronchodilators | Mucolytics | |
| Bronchospasm | 39 (54) | 4 (6) | |
| Wheezing | 37 (51) | 2 (3) | |
| in use prior to admission | 29 (40) | 7 (10) | |
| decrease in tidal volume | 10 (14) | 2 (3) | |
| tenacious mucus | 10 (14) | 33 (46) | |
| purulent mucus | 10 (14) | 8 (11) | |
| increase in peak inspiratory pressure | 9 (13) | 1 (1) | |
| mucus retention | 9 (13) | 21 (29) | |
| Contra-indications * | |||
| known drug allergy | 54 (75) | ||
| Arrhythmias | 23 (32) | ||
| pulmonary edema | 5 (1) | ||
| >15 cm H2O PEEP | 4 (1) | ||
| Nebulizer type * | |||
| jet nebulizer | 40 (56) | ||
| metered dose inhalers | 38 (53) | ||
| vibrating mesh nebulizer | 22 (31) | ||
| ultrasonic nebulizer | 12 (17) | ||
| Manual Hyperinflation | |||
| Practice of use | N = 72 | ||
| routine use | 5 (7) | ||
| as treatment on indication | 53 (74) | ||
| never used | 16 (19) | ||
| Indications * | N = 58 | ||
| difficult oxygenation | 44 (76) | ||
| presumed mucous presence | 35 (60) | ||
| decrease in tidal volume | 28 (48) | ||
| rising inspiratory pressures | 24 (41) | ||
| Contraindications * | |||
| unstable hemodynamics | 35 (60) | ||
| active pneumothorax | 33 (57) | ||
| intracranial hypertension | 32 (55) | ||
| >15 cm H2O PEEP | 25 (43) | ||
| bronchospasm | 13 (22) | ||
| pulmonary oedema | 12 (20) | ||
| Materials used | |||
| Mapleson C© (waterset) circuit | 41 (71) | ||
| Laerdal AMBU© bag | 10 (17) | ||
| Jackson Rees-system© | 1 (2) | ||
| other † | 6 (10) | ||
| Mechanical Insufflation-Exsufflation | |||
| Practice of use | N = 72 | ||
| routine use | 0 | ||
| as treatment on indication | 16 (22) | ||
| never used | 56 (78) | ||
| Indications * | N = 16 | ||
| insufficient cough strength | 16 (100) | ||
| already using at home | 10 (63) | ||
| repeated atelectasis | 8 (50) | ||
| regular airway care ineffectivein removing mucus | 6 (38) | ||
| prevention of reintubation | 5 (31) | ||
| prevention of intubation | 4 (25) | ||
| difficult weaning | 3 (19) | ||
| as a weaning adjunctduring all weaning | 1 (6) | ||
| prevention of pneumonia | 1 (6) | ||
| Contraindications * | |||
| bullous emphysema | 10 (63) | ||
| severe COPD/asthma | 5 (31) | ||
| haemoptysis | 6 (38) | ||
| intracranial hypertension | 9 (56) | ||
| Device used | |||
| Cough assist (Respironics (Philips)© | 16 (100) | ||
| Other: IPV | 3 (19) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stilma, W.; van der Hoeven, S.M.; Scholte op Reimer, W.J.M.; Schultz, M.J.; Rose, L.; Paulus, F. Airway Care Interventions for Invasively Ventilated Critically Ill Adults—A Dutch National Survey. J. Clin. Med. 2021, 10, 3381. https://doi.org/10.3390/jcm10153381
Stilma W, van der Hoeven SM, Scholte op Reimer WJM, Schultz MJ, Rose L, Paulus F. Airway Care Interventions for Invasively Ventilated Critically Ill Adults—A Dutch National Survey. Journal of Clinical Medicine. 2021; 10(15):3381. https://doi.org/10.3390/jcm10153381
Chicago/Turabian StyleStilma, Willemke, Sophia M. van der Hoeven, Wilma J. M. Scholte op Reimer, Marcus J. Schultz, Louise Rose, and Frederique Paulus. 2021. "Airway Care Interventions for Invasively Ventilated Critically Ill Adults—A Dutch National Survey" Journal of Clinical Medicine 10, no. 15: 3381. https://doi.org/10.3390/jcm10153381
APA StyleStilma, W., van der Hoeven, S. M., Scholte op Reimer, W. J. M., Schultz, M. J., Rose, L., & Paulus, F. (2021). Airway Care Interventions for Invasively Ventilated Critically Ill Adults—A Dutch National Survey. Journal of Clinical Medicine, 10(15), 3381. https://doi.org/10.3390/jcm10153381