
Prognostic Significance of the Extranodal Extension of Regional Lymph Nodes in Stage III-N2 Non-Small-Cell Lung Cancer after Curative Resection

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
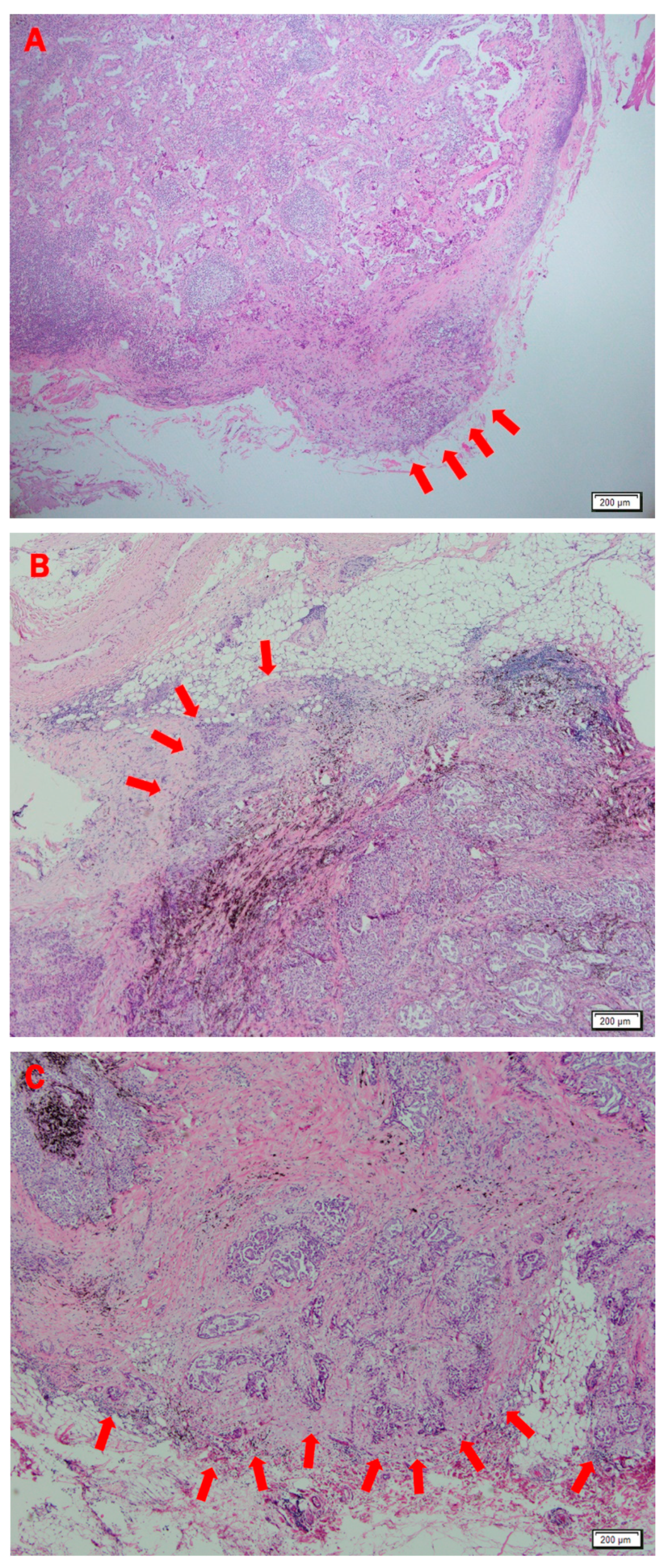
2.2. Histopathologic Review
2.3. Follow Up
2.4. Statistical Analysis
3. Results
3.1. Clinicopathologic Characteristics of Extranodal Extension
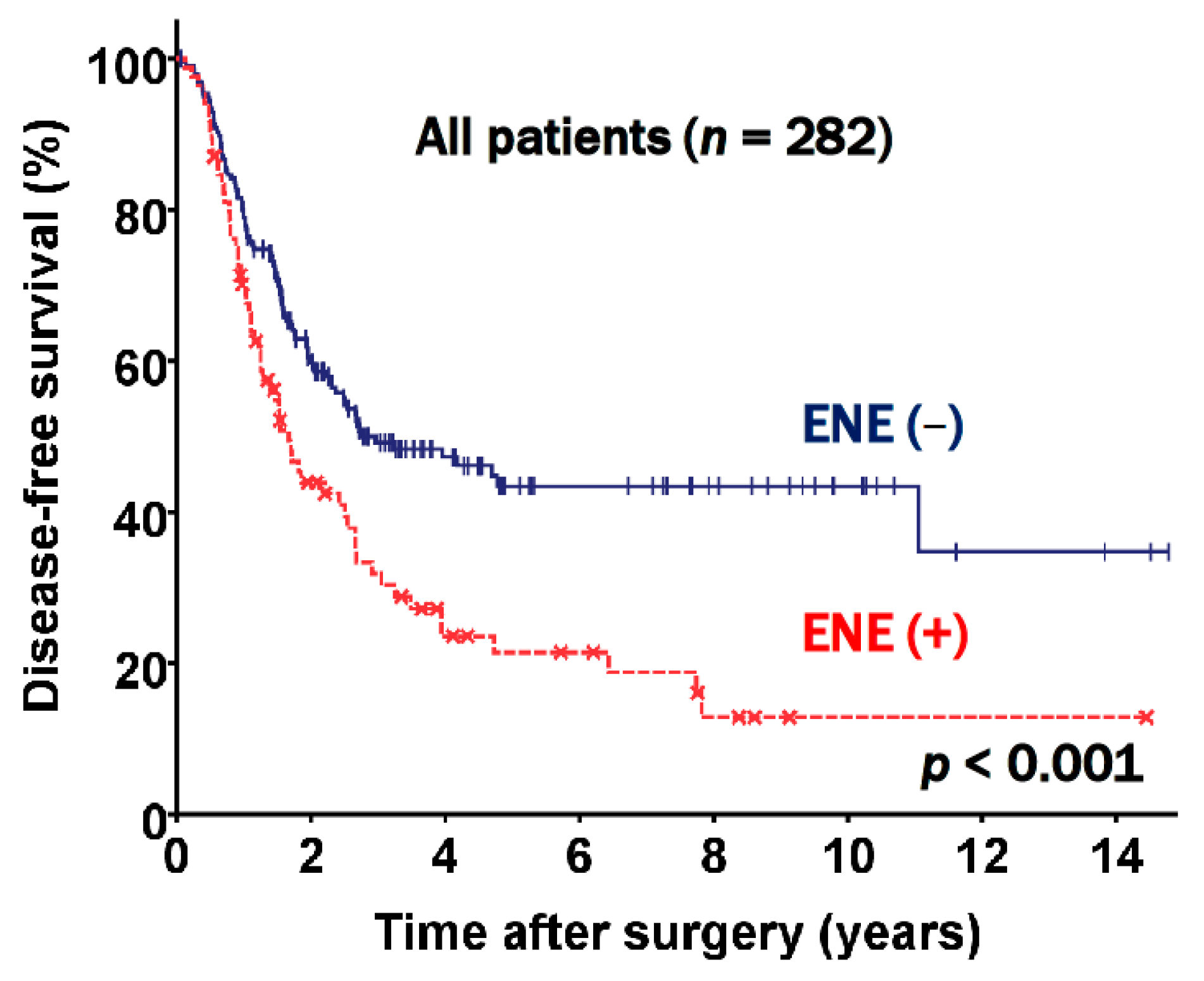
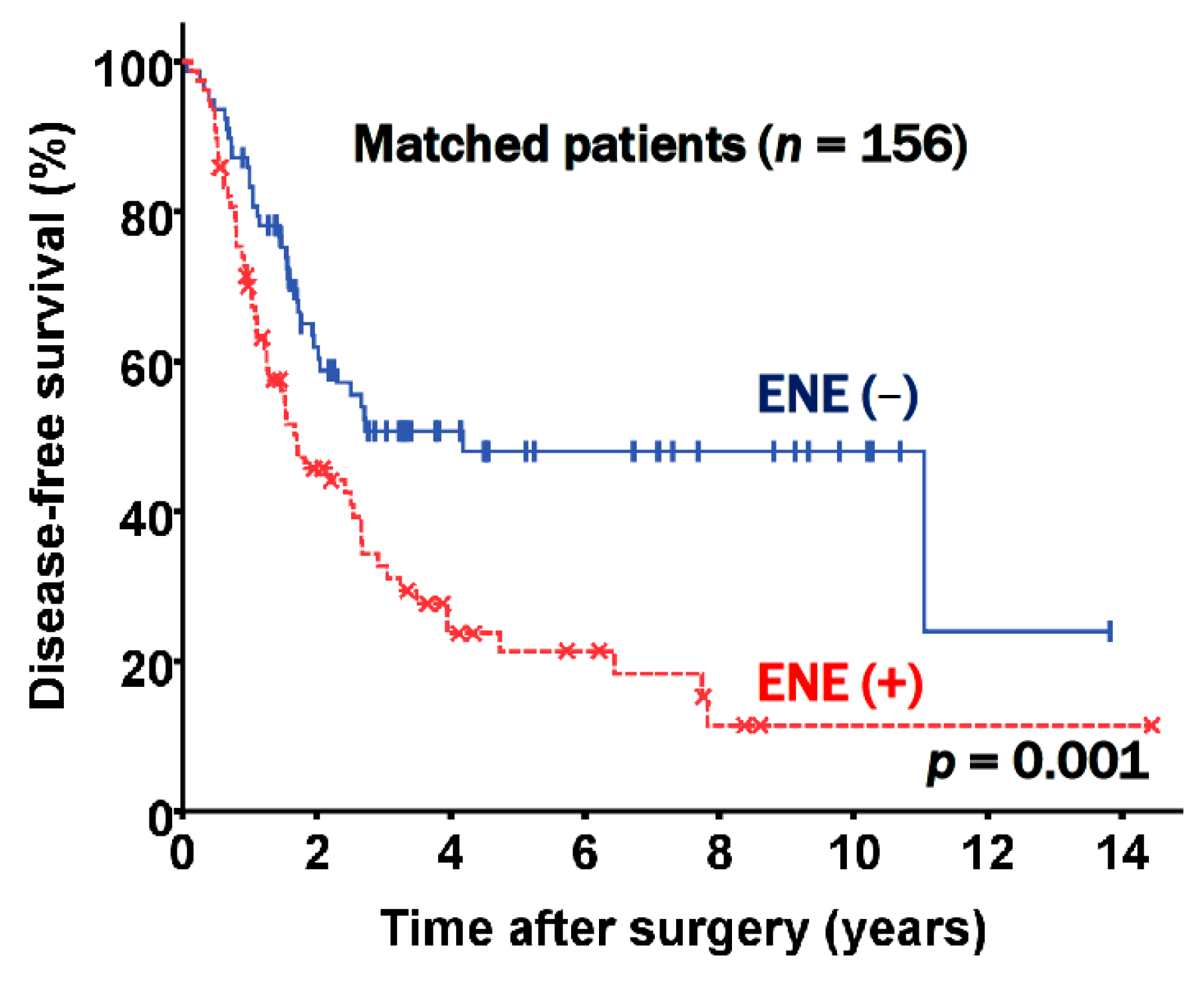
3.2. Prognostic Factors for Disease-Free Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Committee for Scientific Affairs; Sakata, R.; Fujii, Y.; Kuwano, H. Thoracic and cardiovascular surgery in Japan during 2009: Annual report by the Japanese Association for Thoracic Surgery. Gen. Thorac. Cardiovasc. Surg. 2011, 59, 636–637. [Google Scholar] [CrossRef] [PubMed]
- Ravdin, P.M.; Davis, G. Prognosis of patients with resected non-small cell lung cancer: Impact of clinical and pathologic variables. Lung Cancer 2006, 52, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Moretti, L.; Yu, D.S.; Chen, H.; Carbone, D.P.; Johnson, D.H.; Keedy, V.L.; Putnam, J.B.; Sandler, A.B.; Shyr, Y.; Lu, B. Prognostic Factors for Resected Non-Small Cell Lung Cancer with pN2 Status: Implications for Use of Postoperative Radiotherapy. Oncologist 2009, 14, 1106–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, A.A.; Berry, M.F.; Tzao, C.; Gandhi, M.; Worni, M.; Pietrobon, R.; D’Amico, T.A. Induction Chemoradiation Is Not Superior to Induction Chemotherapy Alone in Stage IIIA Lung Cancer. Ann. Thorac. Surg. 2012, 93, 1807–1812. [Google Scholar] [CrossRef]
- Yang, C.-F.J.; Gulack, B.C.; Gu, L.; Speicher, P.J.; Wang, X.; Harpole, D.H.; Onaitis, M.W.; D’Amico, T.A.; Berry, M.F.; Hartwig, M.G. Adding radiation to induction chemotherapy does not improve survival of patients with operable clinical N2 non–small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2015, 150, 1484–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luchini, C.; Fleischmann, A.; Boormans, J.L.; Fassan, M.; Nottegar, A.; Lucato, P.; Stubbs, B.; Solmi, M.; Porcaro, A.; Veronese, N.; et al. Extranodal extension of lymph node metastasis influences recurrence in prostate cancer: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 2374. [Google Scholar] [CrossRef] [PubMed]
- Nottegar, A.; Veronese, N.; Senthil, M.; Roumen, R.; Stubbs, B.; Choi, A.; Verheuvel, N.; Solmi, M.; Pea, A.; Capelli, P.; et al. Extra-nodal extension of sentinel lymph node metastasis is a marker of poor prognosis in breast cancer patients: A systematic review and an exploratory meta-analysis. Eur. J. Surg. Oncol. 2016, 42, 919–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altinyollar, H.; Berberoğlu, U.; Gülben, K.; Irkin, F. The correlation of extranodal invasion with other prognostic parameters in lymph node positive breast cancer. J. Surg. Oncol. 2007, 95, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Yajima, R.; Tatsuki, H.; Kuwano, H. Prediction of Extracapsular Invasion at Metastatic Sentinel Nodes and Non-sentinel Lymph Nodal Metastases by FDG-PET in Cases with Breast Cancer. Anticancer Res. 2016, 36, 1785–1789. [Google Scholar]
- Choi, A.H.; Blount, S.; Perez, M.N.; De Paz, C.E.C.; Rodriguez, S.A.; Surrusco, M.; Garberoglio, C.A.; Lum, S.S.; Senthil, M. Size of Extranodal Extension on Sentinel Lymph Node Dissection in the American College of Surgeons Oncology Group Z0011 Trial Era. JAMA Surg. 2015, 150, 1141–1148. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.-H.; Shen, W.T.; Gosnell, J.; Duh, Q.-Y. Prognostic significance of extranodal extension of regional lymph node metastasis in papillary thyroid cancer. Head Neck 2015, 37, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Song, C.M.; Ji, Y.B.; Pyo, J.Y.; Yi, K.J.; Song, Y.S.; Park, Y.W.; Tae, K. Significance of the Extracapsular Spread of Metastatic Lymph Nodes in Papillary Thyroid Carcinoma. Clin. Exp. Otorhinolaryngol. 2015, 8, 289–294. [Google Scholar] [CrossRef]
- Kelder, W.; Ebrahimi, A.; Forest, V.I.; Gao, K.; Murali, R.; Clark, J.R. Cutaneous head and neck squamous cell carcinoma with regional metastases: The prognostic importance of soft tissue metastases and extranodal spread. Ann. Surg. Oncol. 2012, 19, 274–279. [Google Scholar] [CrossRef] [Green Version]
- Taghavi, N.; Yazdi, I. Prognostic factors of survival rate in oral squamous cell carcinoma: Clinical, histologic, genetic and molecular concepts. Arch. Iran. Med. 2015, 18, 314–319. [Google Scholar] [PubMed]
- Märkl, B.; Rößle, J.; Arnholdt, H.M.; Schaller, T.; Krammer, I.; Cacchi, C.; Jähnig, H.; Schenkirsch, G.; Spatz, H.; Anthuber, M.; et al. The clinical significance of lymph node size in colon cancer. Mod. Pathol. 2012, 25, 1413–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veronese, N.; Nottegar, A.; Pea, A.; Solmi, M.; Stubbs, B.; Capelli, P.; Sergi, G.; Manzato, E.; Fassan, M.; Wood, L.D.; et al. Prognostic impact and implications of extracapsular lymph node involvement in colorectal cancer: A systematic review with meta-analysis. Ann. Oncol. 2016, 27, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Alakus, H.; Hölscher, A.H.; Grass, G.; Hartmann, E.; Schulte, C.; Drebber, U.; Baldus, S.E.; Bollschweiler, E.; Metzger, R.; Mönig, S.P. Extracapsular lymph node spread: A new prognostic factor in gastric cancer. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2010, 116, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Metindir, J.; Dilek, G.B. Evaluation of prognostic significance in extracapsular spread of pelvic lymph node metastasis in patients with cervical cancer. Eur. J. Gynaecol. Oncol. 2008, 29, 476–478. [Google Scholar]
- Luchini, C.; Nottegar, A.; Solmi, M.; Sergi, G.; Manzato, E.; Capelli, P.; Scarpa, A.; Veronese, N. Prognostic implications of extranodal extension in node-positive squamous cell carcinoma of the vulva: A systematic review and meta-analysis. Surg. Oncol. 2016, 25, 60–65. [Google Scholar] [CrossRef]
- Luchini, C.; Veronese, N.; Nottegar, A.; Cheng, M.; Kaneko, T.; Pilati, C.; Tabbò, F.; Stubbs, B.; Pea, A.; Bagante, F.; et al. Extranodal extension of nodal metastases is a poor prognostic moderator in non-small cell lung cancer: A meta-analysis. Virchows Arch. 2018, 472, 939–947. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Wu, C.-T.; Kuo, S.-W.; Tseng, Y.-T.; Chang, Y.-L. Significance of Extranodal Extension of Regional Lymph Nodes in Surgically Resected Non-small Cell Lung Cancer. Chest 2007, 131, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Detterbeck, F.C.; Chansky, K.; Groome, P.; Bolejack, V.; Crowley, J.; Shemanski, L.; Kennedy, C.; Krasnik, M.; Peake, M.; Rami-Porta, R.; et al. The IASLC Lung Cancer Staging Project: Methodology and Validation Used in the Development of Proposals for Revision of the Stage Classification of NSCLC in the Forthcoming (Eighth) Edition of the TNM Classification of Lung Cancer. J. Thorac. Oncol. 2016, 11, 1433–1446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Ann. Intern. Med. 2007, 147, W163–W194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabatabaei, S.V.; Nitche, C.; Michel, M.; Rasche, K.; Hekmat, K. Prognostic Impact of Extracapsular Lymph Node Invasion on Survival in Non-small-Cell Lung Cancer: A Systematic Review and Meta-analysis. Adv. Exp. Med. Biol. 2018, 1116, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Nomura, K.; Aokage, K.; Nakai, T.; Sakashita, S.; Miyoshi, T.; Tane, K.; Samejima, J.; Suzuki, K.; Tsuboi, M.; Ishii, G. Prognostic impact of extranodal extension in patients with pN1–N2 lung adenocarcinoma. J. Cancer Res. Clin. Oncol. 2021, 1–9. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ENE Positive (%) (n = 85) | ENE Negative (%) (n = 197) | p-Value | |
|---|---|---|---|
| Age (years) | 62.1 ± 10.3 | 64.5 ± 10.4 | 0.078 |
| Sex (male) | 58 (68.2) | 121 (61.4) | 0.275 |
| Histology | 0.780 | ||
| Adenocarcinoma | 59 (69.4) | 140 (71.1) | |
| Squamous cell carcinoma | 19 (22.3) | 42 (21.3) | |
| Other cell types | 7 (8.3) | 15 (7.6) | |
| FEV1 (%) | 99.0 ± 23.5 | 101.1 ± 19.2 | 0.455 |
| DLCO (%) | 99.9 ± 20.4 | 102 ± 21.3 | 0.421 |
| Never smoker | 31 (36.5) | 87 (44.2) | 0.230 |
| T stage | 0.034 | ||
| T1 | 12 (14.1) | 42 (21.3) | |
| T2 | 51 (60.0) | 125 (63.4) | |
| T3 | 12 (14.1) | 23 (11.7) | |
| T4 | 10 (11.8) | 7 (3.60) | |
| N stage | <0.001 | ||
| N2a1 | 10 (11.8) | 74 (37.6) | |
| N2a2 | 46 (54.1) | 84 (42.6) | |
| N2b | 29 (34.1) | 39 (19.8) | |
| Extent of operation | 0.002 | ||
| Lobectomy | 76 (89.4) | 193 (98.0) | |
| Pneumonectomy | 9 (10.6) | 4 (2.0) | |
| Adjuvant treatment | 75 (88.2) | 174 (88.3) | 0.983 |
| Visceral pleural invasion (+) | 51 (60.0) | 95 (48.2) | 0.069 |
| Vascular invasion (+) | 63 (74.1) | 129 (65.5) | 0.153 |
| Lymphatic invasion (+) | 49 (57.6) | 72 (36.5) | 0.001 |
| Perineural invasion (+) | 13 (15.3) | 17 (8.60) | 0.096 |
| Variables | Univariate Analysis | Multivariable Analysis | |
|---|---|---|---|
| p-Value | HR (95% CI) | p-Value | |
| Age | 0.007 | 1.031 (1.014–1.049) | <0.001 |
| Sex (male) | 0.275 | ||
| Never smoker | 0.559 | ||
| Preoperative FEV1 (%) | 0.380 | ||
| Preoperative DLCO (%) | 0.529 | ||
| Presence of ENE | <0.001 | 1.629 (1.161–2.284) | 0.005 |
| T stages (T1) | <0.001 | 0.012 | |
| T2 | 1.392 (0.799–2.424) | ||
| T3 | 2.526 (1.338–4.770) | ||
| T4 | 2.158 (0.974–4.784) | ||
| N stages (N2a1) | <0.001 | 0.005 | |
| N2a2 | 0.995 (0.660–1.501) | ||
| N2b | 1.784 (0.990–2.105) | ||
| Visceral pleural invasion (+) | 0.001 | ||
| Vascular invasion (+) | 0.306 | ||
| Lymphatic invasion (+) | 0.497 | ||
| Perineural invasion (+) | 0.280 | ||
| Histology (adenocarcinoma) | 0.695 | ||
| Operation type (pneumonectomy) | 0.622 | ||
| Adjuvant treatment (+) | 0.189 | ||
| ENE Positive (%) (n = 78) | ENE Negative (%) (n = 78) | p-Value | |
|---|---|---|---|
| Age (years) | 62.6 ± 10.3 | 61.7 ± 11.7 | 0.593 |
| Sex (male) | 53 (67.9) | 53 (67.9) | 1.000 |
| Histology (adenocarcinoma) | 54 (69.2) | 49 (61.5) | 0.564 |
| FEV1 (%) | 99.7 ± 24.1 | 99.0 ± 21.1 | 0.859 |
| DLCO (%) | 100.5 ± 20.5 | 98.9 ± 21.4 | 0.642 |
| Never smoker | 29 (37.2) | 28 (35.9) | 1.000 |
| T stage | 0.278 | ||
| T1 | 11 (14.1) | 12 (15.4) | |
| T2 | 48 (61.5) | 52 (66.7) | |
| T3 | 11 (14.1) | 12 (15.4) | |
| T4 | 8 (10.3) | 2 (2.6) | |
| N stage | 0.968 | ||
| N2a1 | 9 (11.5) | 10 (12.8) | |
| N2a2 | 42 (53.8) | 41 (52.6) | |
| N2b | 27 (34.6) | 27 (34.6) | |
| Extent of operation | 0.534 | ||
| Lobectomy | 71 (91.0) | 74 (94.9) | |
| Pneumonectomy | 7 (9.00) | 4 (5.10) | |
| Adjuvant treatment | 68 (87.2) | 72 (92.3) | 0.667 |
| Visceral pleural invasion (+) | 46 (59.0) | 41 (52.6) | 0.519 |
| Vascular invasion (+) | 56 (71.8) | 50 (64.1) | 0.391 |
| Lymphatic invasion (+) | 42 (53.8) | 38 (48.7) | 0.631 |
| Perineural invasion (+) | 9 (11.5) | 10 (12.8) | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, B.C.-H.; Jeon, J.H.; Chung, J.-H.; Kwon, H.J.; Lee, J.H.; Jung, W.; Hwang, Y.; Cho, S.; Kim, K.; Jheon, S. Prognostic Significance of the Extranodal Extension of Regional Lymph Nodes in Stage III-N2 Non-Small-Cell Lung Cancer after Curative Resection. J. Clin. Med. 2021, 10, 3324. https://doi.org/10.3390/jcm10153324
Shih BC-H, Jeon JH, Chung J-H, Kwon HJ, Lee JH, Jung W, Hwang Y, Cho S, Kim K, Jheon S. Prognostic Significance of the Extranodal Extension of Regional Lymph Nodes in Stage III-N2 Non-Small-Cell Lung Cancer after Curative Resection. Journal of Clinical Medicine. 2021; 10(15):3324. https://doi.org/10.3390/jcm10153324
Chicago/Turabian StyleShih, Beatrice Chia-Hui, Jae Hyun Jeon, Jin-Haeng Chung, Hyun Jung Kwon, Jeong Hoon Lee, Woohyun Jung, Yoohwa Hwang, Sukki Cho, Kwhanmien Kim, and Sanghoon Jheon. 2021. "Prognostic Significance of the Extranodal Extension of Regional Lymph Nodes in Stage III-N2 Non-Small-Cell Lung Cancer after Curative Resection" Journal of Clinical Medicine 10, no. 15: 3324. https://doi.org/10.3390/jcm10153324
APA StyleShih, B. C.-H., Jeon, J. H., Chung, J.-H., Kwon, H. J., Lee, J. H., Jung, W., Hwang, Y., Cho, S., Kim, K., & Jheon, S. (2021). Prognostic Significance of the Extranodal Extension of Regional Lymph Nodes in Stage III-N2 Non-Small-Cell Lung Cancer after Curative Resection. Journal of Clinical Medicine, 10(15), 3324. https://doi.org/10.3390/jcm10153324