
Effect of Vibrotherapy on Body Fatness, Blood Parameters and Fibrinogen Concentration in Elderly Men

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
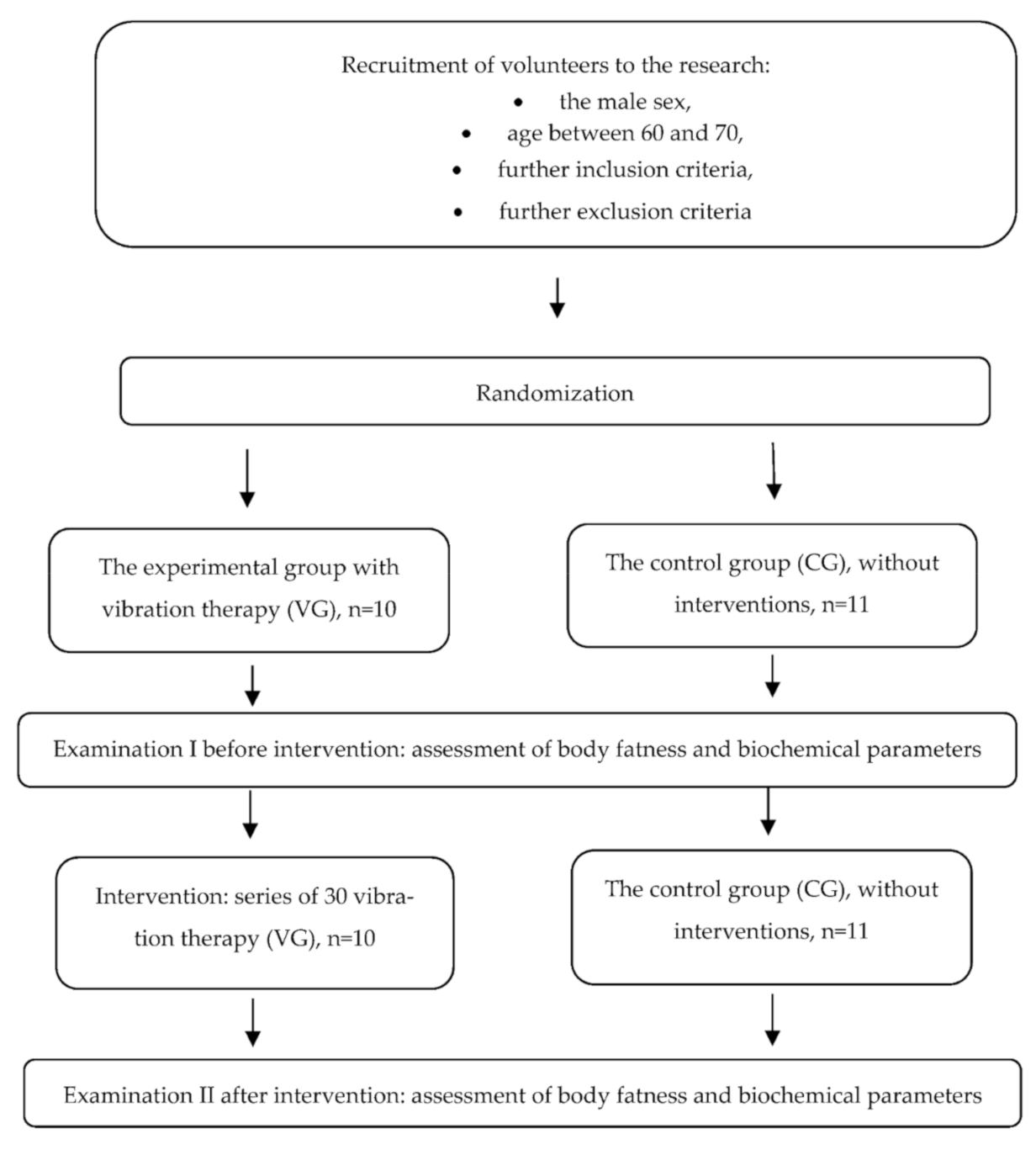
2. Materials and Methods
2.1. Materials
2.2. Methods
2.3. Description of the Intervention
2.4. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Rittweger, J. Vibration as an exercise modality: How it may work, and what its potential might be. Eur. J. Appl. Physiol. 2010, 108, 877–904. [Google Scholar] [CrossRef] [PubMed]
- Zaidell, L.N.; Mileva, K.N.; Sumners, D.P.; Bowtell, J.L. Experimental evidence of the tonic vibration reflex during whole-body vibration of the loaded and unloaded leg. PLoS ONE 2013, 8, e85247. [Google Scholar] [CrossRef] [PubMed]
- Kerschan-Schindl, K.; Grampp, S.; Henk, C.; Resch, H.; Preisinger, E.; Fialka-Moser, V.; Imhof, H. Whole-body vibration exercise leads to alterations in muscle blood volume. Clin. Physiol. 2001, 21, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Goswami, N. Falls and fall-prevention in older persons: Geriatrics meets spaceflight! Front. Physiol. 2017, 8, 603. [Google Scholar] [CrossRef] [PubMed]
- Goswami, N.; Blaber, A.; Hinghofer-Szalkay, H.; Montani, J.-P. Orthostatic intolerance in older persons: Etiology and countermeasures. Front Physiol. 2017, 8, 803. [Google Scholar] [CrossRef] [PubMed]
- Waha, J.E.; Goswami, N.; Schlagenhauf, A.; Leschnik, B.; Koestenberger, M.; Reibnegger, G.; Roller, R.E.; Hinghofer-Szalkay, H.; Cvirn, G. Effects of exercise and nutrition on the coagulation system during bedrest immobilization. Medicine 2015, 94, e1555. [Google Scholar] [CrossRef]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef]
- Ajmani, R.S.; Rifkind, J.M. Hemorheological changes during human aging. Gerontology 1998, 44, 111–120. [Google Scholar] [CrossRef]
- Koenig, W.; Ernst, E.; Matrai, A. Blood rheology associated with cardiovascular risk factors and chronic cardiovascular diseases: Results of an epidemiologic cross-sectional study. Angiology 1988, 39, 986–995. [Google Scholar] [CrossRef]
- Lee, A.J.; Lowe, G.D.O.; Woodward, M.; Tunstall-Pedoe, H. Fibrinogen in relation to personal history of prevalent hypertension, diabetes, stroke, intermittent claudication, coronary heart disease, and family history: The Scottish Heart Health Study. Br. Heart J. 1993, 69, 338–342. [Google Scholar] [CrossRef][Green Version]
- Behar, S. Lowering fibrinogen levels: Clinical update. Blood Coagul. Fibrinolysis 1999, 10, S41–S43. [Google Scholar]
- Sutera, S.P.; Gardner, R.A.; Boylan, C.W.; Carroll, G.L.; Chang, K.C.; Marvel, J.S.; Kilo, C.; Gonen, B.; Williamson, J.R. Age-related changes in deformability of human erythrocytes. Blood 1985, 65, 275–282. [Google Scholar] [CrossRef]
- Toth, A.; Papp, J.; Rabai, M.; Kenyeres, P.; Marton, Z.; Kesmarky, G.; Juricskay, I.; Meiselman, H.J.; Toth, K. The role of hemorheological factors in cardiovascular medicine. Clin. Hemorheol. Microcirc. 2014, 56, 197–204. [Google Scholar] [CrossRef]
- Baskurt, O.K.; Meiselman, H.J. Erythrocyte aggregation: Basic aspects and clinical importance. Clin. Hemorheol. Microcirc. 2013, 53, 23–37. [Google Scholar] [CrossRef]
- Connes, P.; Pichon, A.; Hardy-Dessources, M.D.; Waltz, X.; Lamarre, Y.; Simmonds, M.J.; Tripette, J. Blood viscosity and hemodynamics during exercise. Clin. Hemorheol. Microcirc. 2012, 51, 101–109. [Google Scholar] [CrossRef]
- Burkhardt, R.; Kettner, G.; Böhm, W.; Schmidmeier, M.; Schlag, R.; Frisch, B.; Mallmann, B.; Eisenmenger, W.; Gilg, T. Changes in trabecular bone, hematopoiesis and bone marrow vessels in aplastic anemia, primary osteoporosis, and old age: A comparative histomorphometric study. Bone 1987, 8, 157–164. [Google Scholar] [CrossRef]
- Brennan, D.S.; Singh, K.A. Dietary, self-reported oral health and socio-demographic Predictors of general health status among older adults. J. Nutr. Health Aging 2012, 16, 437–441. [Google Scholar] [CrossRef]
- Neel, D.R.; McClave, S.; Martindale, R. Hypoalbuminaemia in the perioperative period: Clinical significance and management options. Best Pract. Res. Clin. Anaesthesiol. 2011, 25, 395–400. [Google Scholar] [CrossRef]
- Prajapati, K.D.; Sharma, S.S.; Roy, N. Current perspectives on potential role of albumin in neuroprotection. Rev. Neurosci. 2011, 22, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Hardeman, M.R.; Dobbe, J.G.G.; Ince, C. The Laser-assisted Optical Rotational Cell Analyzer (LORCA) as red blood cell aggregometer. Clin. Hemorheol. Microcirc. 2001, 25, 1–11. [Google Scholar] [PubMed]
- Vitberg. Available online: https://www.vitberg.com/ (accessed on 4 May 2021).
- Piotrowska, A.M.; Bigosińska, M.; Potok, H.; Cisoń-Apanasewicz, U.; Czerwińska-Ledwig, O.; Tota, Ł.; Zuziak, R.; Pałka, T.; Pilch, W. Impact of oscillatory-cycloid vibration interventions on body composition, waist and hip circumference, and blood lipid profile in women aged over 65 years with hypercholesterolaemia. Menopause Rev. 2018, 17, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Vissers, D.; Verrijken, A.; Mertens, I.; Van Gils, C.; Van De Sompel, A.; Truijen, S.; Van Gaal, L. Effect of long-term whole body vibration training on visceral adipose tissue: A preliminary report. Obes. Facts 2010, 3, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Sañudo, B.; Alfonso-Rosa, R.; Del Pozo-Cruz, B.; Del Pozo-Cruz, J.; Galiano, D.; Figueroa, A. Whole body vibration training improves leg blood flow and adiposity in patients with type 2 diabetes mellitus. Eur. J. Appl. Physiol. 2013, 113, 2245–2252. [Google Scholar] [CrossRef]
- Wilms, B.; Frick, J.; Ernst, B.; Mueller, R.; Wirth, B.; Schultes, B. Whole body vibration added to endurance training in obese women—A pilot study. Int. J. Sports Med. 2012, 33, 740–743. [Google Scholar] [CrossRef] [PubMed]
- Rubin, C.T.; Capilla, E.; Luu, Y.K.; Busa, B.; Crawford, H.; Nolan, D.J.; Mittal, V.; Rosen, C.J.; Pessin, J.E.; Judex, S. Adipogenesis is inhibited by brief, daily exposure to high-frequency, extremely low-magnitude mechanical signals. Proc. Natl. Acad. Sci. USA 2007, 104, 17879–17884. [Google Scholar] [CrossRef]
- Solá, E.; Vayá, A.; Simó, M.; Hernández-Mijares, A.; Morillas, C.; España, F.; Estellés, A.; Corella, D. Fibrinogen, plasma viscosity and blood viscosity in obesity. Relationship with insulin resistance. Clin. Hemorheol. Microcirc. 2007, 37, 309–318. [Google Scholar]
- Marton, Z.; Kesmarky, G.; Vekasi, J.; Cser, A.; Russai, R.; Horvath, B.; Toth, K. Red blood cell aggregation measurements in whole blood and in fibrinogen solutions by different methods. Clin. Hemorheol. Microcirc. 2001, 24, 75–83. [Google Scholar]
- Simmonds, M.J.; Meiselman, H.J.; Baskurt, O.K. Blood rheology and aging. J. Geriatr. Cardiol. 2013, 10, 291–301. [Google Scholar]
- Tripolino, C.; Irace, C.; Carallo, C.; Scavelli, F.B.; Gnasso, A. Body fat and blood rheology: Evaluation of the association between different adiposity indices and blood viscosity. Clin. Hemorheol. Microcirc. 2017, 65, 241–248. [Google Scholar] [CrossRef]
- Christy, R.M.; Baskurt, O.K.; Gass, G.C.; Gray, A.B.; Marshall-Gradisnik, S.M. Erythrocyte aggregation and neutrophil function in an aging population. Gerontology 2010, 56, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Avellone, G.; Di Garbo, V.; Panno, A.V.; Cordova, R.; Alletto, G.; Raneli, G.; De Simone, R.; Strano, A.; Bompiani, G.D. Haemorheological components in the pre-geriatric and geriatric age range in a randomly selected Western Sicily population sample (Casteldaccia study). Clin. Hemorheol. Microcirc. 1993, 13, 83–92. [Google Scholar] [CrossRef]
- El-Sayed, M.S.; Jones, P.G.W.; Sale, C. Exercise induces a change in plasma fibrinogen concentration: Fact or fiction? Thromb. Res. 1999, 96, 467–472. [Google Scholar] [CrossRef]
- Womack, C.J.; Nagelkirk, P.R.; Coughlin, A.M. Exercise-induced changes in coagulation and fibrinolysis in healthy populations and patients with cardiovascular disease. Sport. Med. 2003, 33, 795–807. [Google Scholar] [CrossRef]
- Wosomu, D.; Allardyce, W.; Ballantyne, D.; Tansey, P. Influence of power and aerobic exercise training on haemostatic factors after coronary artery surgery. Heart 1992, 68, 181–186. [Google Scholar] [CrossRef]
- Stratton, J.R.; Chandler, W.L.; Schwartz, R.S.; Cerqueira, M.D.; Levy, W.C.; Kahn, S.E.; Larson, V.G.; Cain, K.C.; Beard, J.C.; Abrass, I.B. Effects of physical conditioning on fibrinolytic variables and fibrinogen in young and old healthy adults. Circulation 1991, 83, 1692–1697. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, N.; Yasu, T.; Tsuboi, K.; Sugawara, Y.; Kubo, N.; Umemoto, T.; Arao, K.; Kawakami, M.; Momomura, S.I. Effects of submaximal exercise on blood rheology and sympathetic nerve activity. Circ. J. 2010, 74, 730–734. [Google Scholar] [CrossRef] [PubMed]
- Brun, J.F.; Varlet-Marie, E.; Connes, P.; Aloulou, I. Hemorheological alterations related to training and overtraining. Biorheology 2010, 47, 95–115. [Google Scholar] [CrossRef]
- Games, K.E.; Sefton, J.E.M.; Wilson, A.E. Whole-body vibration and blood flow and muscle oxygenation: A meta-analysis. J. Athl. Train. 2015, 50, 542–549. [Google Scholar] [CrossRef]
- Fowler, B.D.; Palombo, K.T.; Feland, J.B.; Blotter, J.D. Effects of whole-body vibration on flexibility and stiffness: A literature review. Int. J. Exerc. Sci. 2019, 12, 735–747. [Google Scholar]
- Rittweger, J.; Beller, G.; Felsenberg, D. Acute physiological effects of exhaustive whole-body vibration exercise in man. Clin. Physiol. 2000, 20, 134–142. [Google Scholar] [CrossRef]
- Ghazalian, F. Effects of whole body vibration training on inflammatory markers in young healthy males. Ann. Mil. Health Sci. Res. 2019, 17. [Google Scholar] [CrossRef]
- Sackner, M.A.; Gummels, E.; Adams, J.A. Nitric oxide is released into circulation with whole-body, periodic acceleration. Chest 2005, 127. [Google Scholar] [CrossRef]
- Hagan, R.D.; Diaz, F.J.; McMurray, R.G.; Horvath, S.M. Plasma volume changes related to posture and exercise. Med. Sci. Sports Exerc. 1980, 19, 202–206. [Google Scholar] [CrossRef]
- Szygula, Z. Erythrocytic system under the influence of physical exercise and training. Sport. Med. 1990, 10, 181–197. [Google Scholar] [CrossRef] [PubMed]
- Ernst, E.; Daburger, L.; Saradeth, T. The kinetics of blood rheology during and after prolonged standardized exercise. Clin. Hemorheol. Microcirc. 1991, 11, 429–439. [Google Scholar] [CrossRef]
- Ando, H.; Nieminen, K.; Toppila, E.; Starck, J.; Ishitake, T. Effect of impulse vibration on red blood cells in vitro. Scand. J. Work. Environ. Health 2005, 31, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Bi, C.; Chaump, M.; Kaufman, H.W.; Kroll, M.H. Associations of aerobic and strength exercise with clinical laboratory test values. PLoS ONE 2017, 12, e0180840. [Google Scholar] [CrossRef]
- Röcker, L.; Kirsch, K.A.; Stoboy, H. Plasma volume, albumin and globulin concentrations and their intravascular masses—A comparative study in endurance athletes and sedentary subjects. Eur. J. Appl. Physiol. Occup. Physiol. 1976, 36, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Goswami, N.; Taucher, A.A.; Brix, B.; Roessler, A.; Koestenberger, M.; Reibnegger, G.; Cvirn, G. Coagulation changes during central hypovolemia across seasons. J. Clin. Med. 2020, 9, 3461. [Google Scholar] [CrossRef]
- Sachse, C.; Trozic, I.; Brix, B.; Roessler, A.; Goswami, N. Sex differences in cardiovascular responses to orthostatic challenge in healthy older persons: A pilot study. Physiol. Int. 2019, 106, 236–249. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total | CG | VG | p |
|---|---|---|---|---|
| X ± SD | X ± SD | X ± SD | ||
| Age | 65.3 ± 2.7 | 65.0 ± 2.4 | 65.6 ± 3.0 | 0.619 |
| BM (kg) | 85.6 ± 8.2 | 84.2 ± 6.7 | 87.2 ± 9.6 | 0.412 |
| BMI (kg/m2) | 27.8 ± 3.4 | 26.5 ± 2.7 | 29.3 ± 3.3 | 0.053 |
| FFM (kg) | 53.2 ± 4.2 | 53.8 ± 4.1 | 52.5 ± 4.5 | 0.499 |
| BF (kg) | 29.7 ± 8.9 | 27.5 ± 8.2 | 32.1 ± 9.4 | 0.251 |
| BF (%) | 34.2 ± 7.6 | 32.3 ± 7.9 | 36.2 ± 7.0 | 0.235 |
| TBW (%) | 50.8 ± 4.6 | 51.5 ± 4.2 | 50.0 ± 5.2 | 0.490 |
| Variables | CG | VG | p Int | p Time | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | ∆ | p | Pre | Post | ∆ | p | |||
| X ± SD | X ± SD | X ± SD | X ± SD | X ± SD | X ± SD | |||||
| BM (kg) | 84.2 ± 6.7 | 83.1 ± 6.0 | −1.1 ± 2.8 | 0.225 | 87.2 ± 9.6 | 84.5 ± 9.9 | −2.7 ± 2.0 | 0.002 * | 0.150 | 0.002 * |
| BMI (kg/m2) | 26.5 ± 2.7 | 26.2 ± 2.4 | −0.4 ± 0.9 | 0.218 | 29.3 ± 3.3 | 28.4 ± 3.4 | −0.9 ± 0.7 | 0.002 * | 0.136 | 0.002 * |
| FFM (kg) | 53.8 ± 4.1 | 53.6 ± 3.6 | −0.2 ± 1.3 | 0.660 | 52.5 ± 4.5 | 51.9 ± 3.8 | −0.6 ± 1.6 | 0.245 | 0.486 | 0.218 |
| BF (kg) | 27.5 ± 8.2 | 26.6 ± 7.7 | −0.9 ± 2.1 | 0.181 | 32.1 ± 9.4 | 29.6 ± 10.4 | −2.5 ± 2.5 | 0.013 * | 0.131 | 0.003 * |
| BF (%) | 32.3 ± 7.9 | 31.7 ± 7.5 | −0.6 ± 1.5 | 0.222 | 36.2 ± 7.0 | 34.2 ± 8.6 | −2.0 ± 2.7 | 0.041 * | 0.149 | 0.012 * |
| TBW (%) | 51.5 ± 4.2 | 51.9 ± 4.1 | 0.4 ± 1.1 | 0.288 | 50.0 ± 5.2 | 50.4 ± 4.6 | 0.4 ± 1.2 | 0.380 | 0.922 | 0.152 |
| Variables | CG | VG | p Int | p Time | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | ∆ | Pre | Post | ∆ | |||||
| X ± SD | X ± SD | X ± SD | p | X ± SD | X ± SD | X ± SD | p | |||
| Hb (g/dL) | 14.9 ± 0.7 | 14.7 ± 0.8 | −0.2 ± 0.7 | 0.515 | 15.3 ± 0.6 | 14.9 ± 0.4 | −0.4 ± 0.5 | 0.047 * | 0.438 | 0.078 |
| Hct (%) | 43.7 ± 2.6 | 43.7 ± 2.4 | −0.0 ± 2.1 | 0.978 | 44.4 ± 1.7 | 43.7 ± 1.0 | −0.7 ± 1.4 | 0.180 | 0.439 | 0.414 |
| RBC (T/L) | 4.8 ± 0.4 | 4.7 ± 0.3 | −0.2 ± 0.3 | 0.121 | 5.0 ± 0.3 | 5.0 ± 0.2 | −0.1 ± 0.1 | 0.035 * | 0.517 | 0.021 * |
| WBC (109/L) | 5.6 ± 1.2 | 5.9 ± 1.1 | 0.4 ± 1.2 | 0.332 | 6.0 ± 0.7 | 6.0 ± 0.5 | 0.0 ± 0.5 | 0.902 | 0.413 | 0.601 |
| PLT (109/L) | 220.1 ± 63.2 | 216.1 ± 32.4 | −4.0 ± 50.9 | 0.563 | 225.6 ± 50.5 | 219.8 ± 57.2 | −5.8 ± 20.6 | 0.203 | 0.918 | 0.808 |
| MPV (fl) | 12.1 ± 0.7 | 12.6 ± 0.2 | −0.0 ± 0.6 | 0.424 | 12.0 ± 1.0 | 12.1 ± 1.1 | 0.1 ± 0.7 | 0.779 | 0.783 | 0.883 |
| PDW (%) | 15.8 ± 0.2 | 15.9 ± 0.0 | 0.1 ± 0.2 | 0.240 | 15.8 ± 0.2 | 15.9 ± 0.2 | 0.1 ± 0.2 | 0.191 | 0.930 | 0.077 |
| PCT (%) | 0.3 ± 0.1 | 0.3 ± 3.4 | −0.0 ± 0.1 | 0.657 | 0.3 ± 0.1 | 0.3 ± 0.1 | −0.0 ± 0.0 | 0.418 | 0.893 | 0.695 |
| MCV (fl) | 91.2 ± 3.2 | 91.5 ± 1.2 | 0.3 ± 1.0 | 0.351 | 88.4 ± 2.2 | 88.0 ± 2.0 | −0.3 ± 0.5 | 0.060 | 0.080 | 0.578 |
| MCH (pg) | 30.9 ± 1.1 | 30.9 ± 0.8 | 0.0 ± 0.7 | 0.862 | 30.3 ± 1.0 | 29.9 ± 1.1 | −0.4 ± 0.4 | 0.013 * | 0.099 | 0.167 |
| MCHC (g/dL) | 33.9 ± 0.8 | 33.8 ± 10.5 | −0.1 ± 0.6 | 0.523 | 34.3 ± 0.6 | 34.0 ± 0.8 | −0.3 ± 0.6 | 0.151 | 0.550 | 0.136 |
| RDW-CV (%) | 13.8 ± 0.5 | 17.1 ± 2.0 | 3.4 ± 10.5 | 0.110 | 13.6 ± 0.5 | 13.8 ± 0.4 | 0.2 ± 0.3 | 0.101 | 0.349 | 0.676 |
| RDW-SD (fl) | 46.4 ± 2.4 | 46.5 ± 0.2 | 0.1 ± 1.5 | 0.827 | 44.2 ± 1.7 | 44.5 ± 1.4 | 0.4 ± 1.1 | 0.346 | 0.660 | 0.439 |
| Variables | CG | VG | p Int | p Time | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | ∆ | Pre | Post | ∆ | |||||
| X ± SD | X ± SD | X ± SD | p | X ± SD | X ± SD | X ± SD | p | |||
| AMP (au) | 21.0 ± 3.3 | 21.7 ± 2.7 | 0.7 ± 2.8 | 0.466 | 23.5 ± 2.0 | 23.6 ± 1.8 | 0.1 ± 2.8 | 0.921 | 0.656 | 0.556 |
| T½ (s) | 2.1 ± 0.7 | 1.8 ± 0.4 | −0.3 ± 0.7 | 0.184 | 2.0 ± 0.5 | 1.8 ± 0.4 | −0.1 ± 0.6 | 0.487 | 0.573 | 0.141 |
| AI (%) | 65.7 ± 8.1 | 67.4 ± 7.5 | 1.8 ± 7.1 | 0.328 | 63.6 ± 5.2 | 61.9 ± 4.5 | −1.7 ± 5.1 | 0.323 | 0.222 | 0.520 |
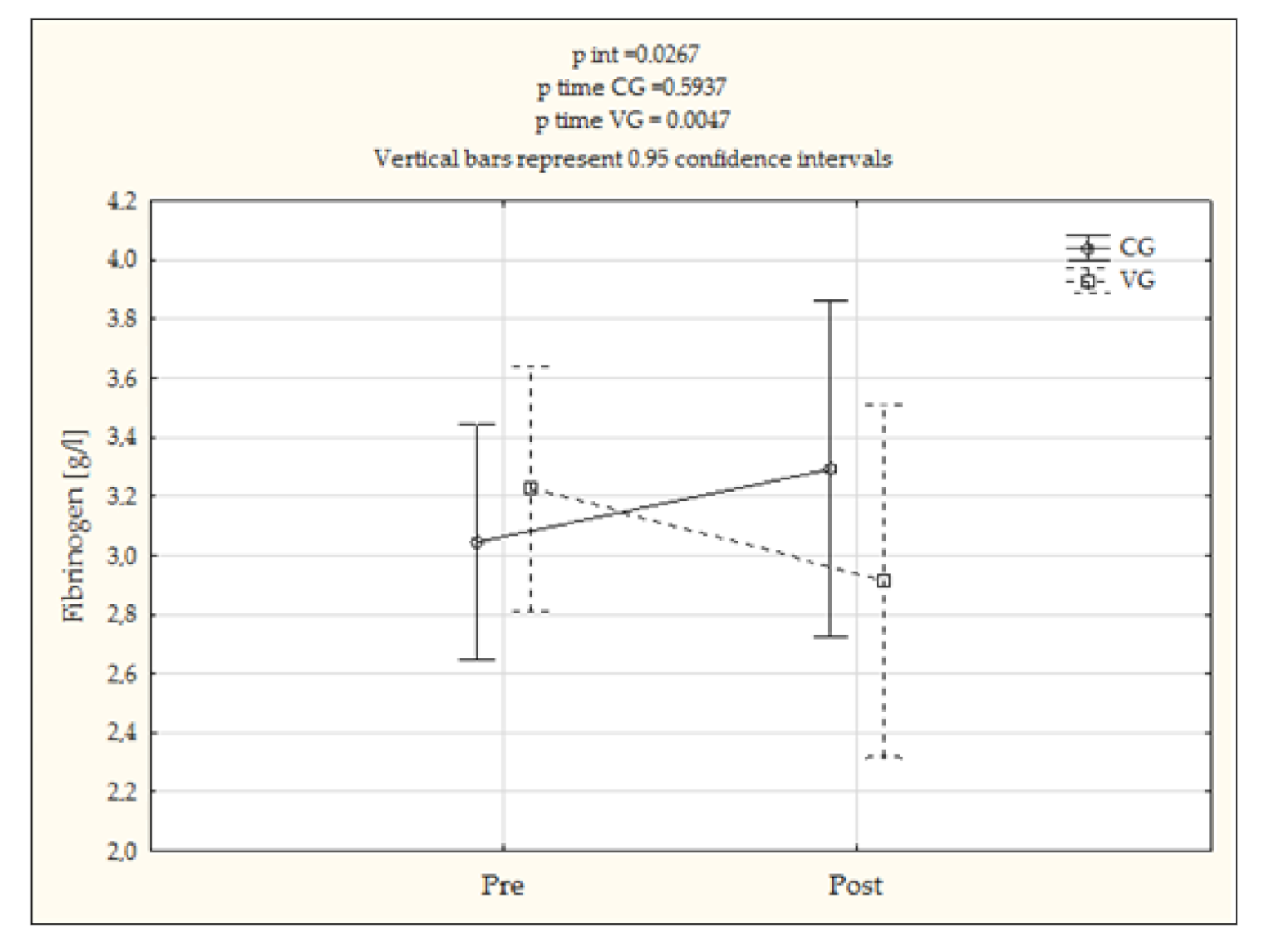
| Fib (g/L) | 3.1 ± 0.6 | 3.3 ± 1.1 | 0.3 ± 0.7 | 0.594 | 3.2 ± 0.7 | 2.9 ± 0.5 | −0.3 ± 0.3 | 0.005 * | 0.027 * | 0.192 |
| Variables | CG | VG | p Int | p Time | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | ∆ | Pre | Post | ∆ | |||||
| X ± SD | X ± SD | X ± SD | p | X ± SD | X ± SD | X ± SD | p | |||
| Total proteins (g/L) | 74.7 ± 4.5 | 72.1 ± 2.7 | −2.7 ± 5.2 | 0.182 | 73.5 ± 3.8 | 72.5 ± 3.7 | −1.0 ± 1.9 | 0.143 | 0.347 | 0.085 |
| Albumins (g/L) | 58.3 ± 4.5 | 58.4 ± 4.4 | 0.1 ± 4.1 | 0.972 | 58.7 ± 3.3 | 57.2 ± 9.5 | −1.4 ± 4.5 | 0.169 | 0.658 | 0.313 |
| α-1-globulins (g/L) | 3.1 ± 3.2 | 2.5 ± 0.8 | −0.7 ± 3.3 | 0.721 | 2.2 ± 0.3 | 2.1 ± 0.3 | −0.1 ± 0.3 | 0.069 | 0.626 | 0.514 |
| α-2-globulins (g/L) | 10.8 ± 1.4 | 11.2 ± 22.2 | 0.4 ± 1.8 | 0.542 | 10.3 ± 0.9 | 9.8 ± 1.3 | −0.5 ± 1.0 | 0.140 | 0.237 | 0.414 |
| β-1-globulins (g/L) | 9.0 ± 1.1 | 9.0 ± 0.5 | 0.0 ± 0.9 | 1.000 | 9.4 ± 0.8 | 9.5 ± 1.0 | 0.1 ± 0.7 | 0.686 | 0.784 | 0.807 |
| β-2-globulins (g/L) | 7.4 ± 1.4 | 7.1 ± 1.4 | −0.3 ± 0.9 | 0.610 | 6.9 ± 1.6 | 6.6 ± 1.4 | −0.3 ± 0.7 | 0.198 | 0.855 | 0.185 |
| γ-globulins (g/L) | 12.4 ± 2.3 | 10.7 ± 2.7 | −1.7 ± 3.2 | 0.091 | 12.4 ± 2.1 | 12.3 ± 1.7 | −0,1 ± 1.2 | 0.851 | 0.146 | 0.092 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kabata-Piżuch, A.; Suder, A.; Jagielski, P.; Kubasiak, K.; Handzlik, P.; Teległów, A.; Marchewka, A. Effect of Vibrotherapy on Body Fatness, Blood Parameters and Fibrinogen Concentration in Elderly Men. J. Clin. Med. 2021, 10, 3259. https://doi.org/10.3390/jcm10153259
Kabata-Piżuch A, Suder A, Jagielski P, Kubasiak K, Handzlik P, Teległów A, Marchewka A. Effect of Vibrotherapy on Body Fatness, Blood Parameters and Fibrinogen Concentration in Elderly Men. Journal of Clinical Medicine. 2021; 10(15):3259. https://doi.org/10.3390/jcm10153259
Chicago/Turabian StyleKabata-Piżuch, Anna, Agnieszka Suder, Paweł Jagielski, Katarzyna Kubasiak, Paulina Handzlik, Aneta Teległów, and Anna Marchewka. 2021. "Effect of Vibrotherapy on Body Fatness, Blood Parameters and Fibrinogen Concentration in Elderly Men" Journal of Clinical Medicine 10, no. 15: 3259. https://doi.org/10.3390/jcm10153259
APA StyleKabata-Piżuch, A., Suder, A., Jagielski, P., Kubasiak, K., Handzlik, P., Teległów, A., & Marchewka, A. (2021). Effect of Vibrotherapy on Body Fatness, Blood Parameters and Fibrinogen Concentration in Elderly Men. Journal of Clinical Medicine, 10(15), 3259. https://doi.org/10.3390/jcm10153259