
Role of Non-Invasive Respiratory Supports in COVID-19 Acute Respiratory Failure Patients with Do Not Intubate Orders

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Method
2.1. Procedure
2.2. Main Reasons for Non-Intubation
2.3. Data Collection
2.4. Target Trial Framework
2.5. Inverse Probability of Treatment Weighting
2.6. Statistical Analysis
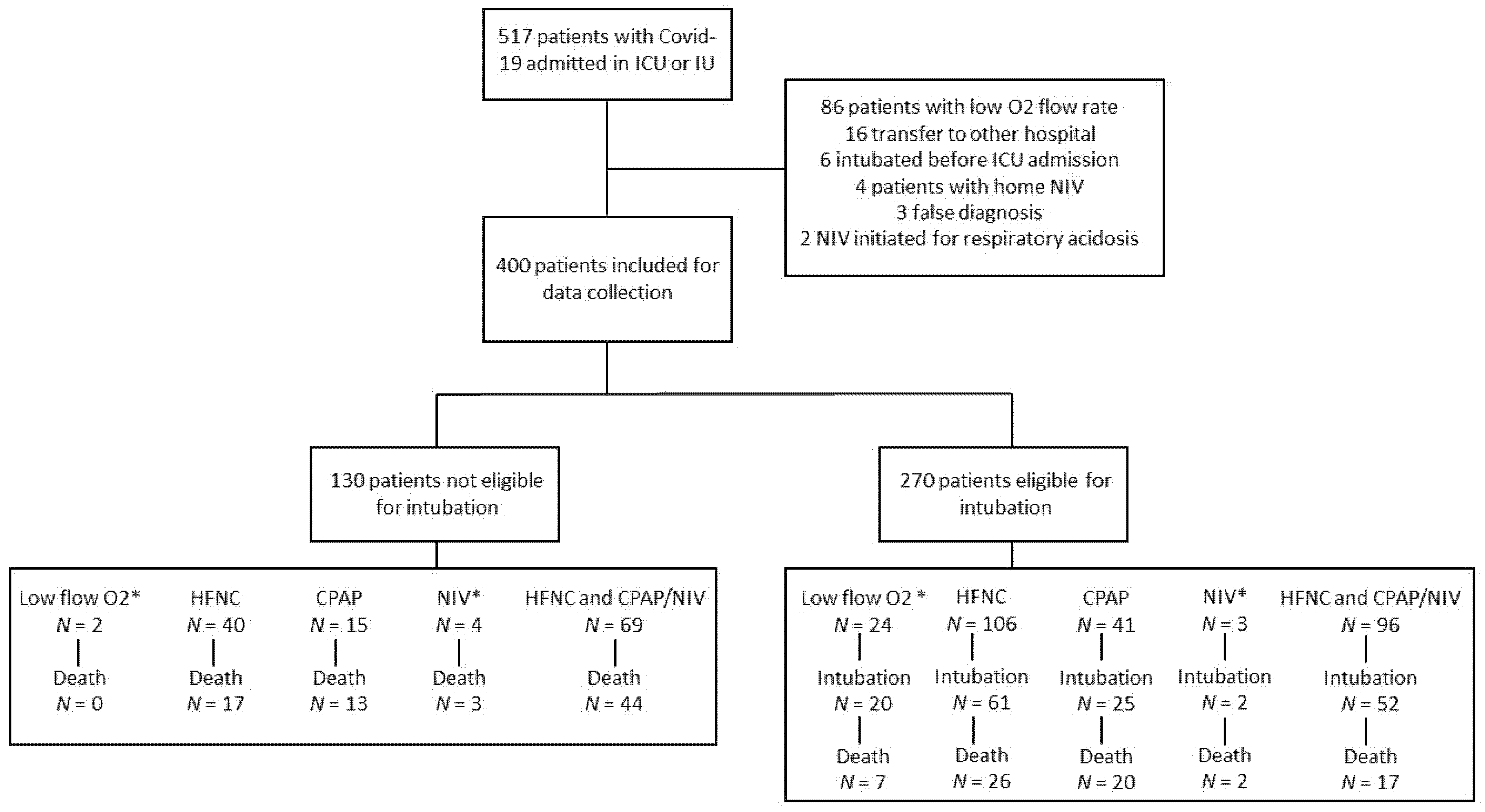
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574. [Google Scholar] [CrossRef] [Green Version]
- COVID-ICU Group on Behalf of the REVA Network and the COVID-ICU Investigators. Clinical Characteristics and Day-90 Outcomes of 4244 Critically Ill Adults with COVID-19: A Prospective Cohort Study. Intensive Care Med. 2021, 47, 60–73. [Google Scholar] [CrossRef] [PubMed]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, Clinical Course, and Outcomes of Critically Ill Adults with COVID-19 in New York City: A Prospective Cohort Study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Alhazzani, W.; Evans, L.; Alshamsi, F.; Møller, M.H.; Ostermann, M.; Prescott, H.C.; Arabi, Y.M.; Loeb, M.; Ng Gong, M.; Fan, E.; et al. Surviving Sepsis Campaign Guidelines on the Management of Adults With Coronavirus Disease 2019 (COVID-19) in the ICU: First Update. Crit. Care Med. 2021, 49, e219–e234. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Consortium; Van Aerde, N.; Van den Berghe, G.; Wilmer, A.; Gosselink, R.; Hermans, G. Intensive Care Unit Acquired Muscle Weakness in COVID-19 Patients. Intensive Care Med. 2020, 46, 2083–2085. [Google Scholar] [CrossRef] [PubMed]
- Medrinal, C.; Prieur, G.; Bonnevie, T.; Gravier, F.-E.; Mayard, D.; Desmalles, E.; Smondack, P.; Lamia, B.; Combret, Y.; Fossat, G. Muscle Weakness, Functional Capacities and Recovery for COVID-19 ICU Survivors. BMC Anesthesiol. 2021, 21, 64. [Google Scholar] [CrossRef] [PubMed]
- Lim, Z.J.; Subramaniam, A.; Ponnapa Reddy, M.; Blecher, G.; Kadam, U.; Afroz, A.; Billah, B.; Ashwin, S.; Kubicki, M.; Bilotta, F.; et al. Case Fatality Rates for Patients with COVID-19 Requiring Invasive Mechanical Ventilation. A Meta-Analysis. Am. J. Respir. Crit. Care Med. 2021, 203, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Creteur, J. Ethical Aspects of the COVID-19 Crisis: How to Deal with an Overwhelming Shortage of Acute Beds. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 248–252. [Google Scholar] [CrossRef]
- Truog, R.D.; Mitchell, C.; Daley, G.Q. The Toughest Triage—Allocating Ventilators in a Pandemic. N. Engl. J. Med. 2020, 382, 1973–1975. [Google Scholar] [CrossRef]
- Demoule, A.; Vieillard Baron, A.; Darmon, M.; Beurton, A.; Géri, G.; Voiriot, G.; Dupont, T.; Zafrani, L.; Girodias, L.; Labbé, V.; et al. High-Flow Nasal Cannula in Critically III Patients with Severe COVID-19. Am. J. Respir. Crit. Care Med. 2020, 202, 1039–1042. [Google Scholar] [CrossRef]
- Oranger, M.; Gonzalez-Bermejo, J.; Dacosta-Noble, P.; Llontop, C.; Guerder, A.; Trosini-Desert, V.; Faure, M.; Raux, M.; Decavele, M.; Demoule, A.; et al. Continuous Positive Airway Pressure to Avoid Intubation in SARS-CoV-2 Pneumonia: A Two-Period Retrospective Case-Control Study. Eur. Respir. J. 2020, 56, 2001692. [Google Scholar] [CrossRef]
- Nightingale, R.; Nwosu, N.; Kutubudin, F.; Fletcher, T.; Lewis, J.; Frost, F.; Haigh, K.; Robinson, R.; Kumar, A.; Jones, G.; et al. Is Continuous Positive Airway Pressure (CPAP) a New Standard of Care for Type 1 Respiratory Failure in COVID-19 Patients? A Retrospective Observational Study of a Dedicated COVID-19 CPAP Service. BMJ Open Respir. Res. 2020, 7, e000639. [Google Scholar] [CrossRef]
- Coppadoro, A.; Benini, A.; Fruscio, R.; Verga, L.; Mazzola, P.; Bellelli, G.; Carbone, M.; Mulinacci, G.; Soria, A.; Noè, B.; et al. Helmet CPAP to Treat Hypoxic Pneumonia Outside the ICU: An Observational Study during the COVID-19 Outbreak. Crit. Care 2021, 25, 80. [Google Scholar] [CrossRef]
- Franco, C.; Facciolongo, N.; Tonelli, R.; Dongilli, R.; Vianello, A.; Pisani, L.; Scala, R.; Malerba, M.; Carlucci, A.; Negri, E.A.; et al. Feasibility and Clinical Impact of Out-of-ICU Noninvasive Respiratory Support in Patients with COVID-19-Related Pneumonia. Eur. Respir. J. 2020, 56, 2002130. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Grasselli, G.; Cecconi, M.; Antolini, L.; Borelli, M.; De Giacomi, F.; Bosio, G.; Latronico, N.; Filippini, M.; Gemma, M.; et al. Noninvasive Ventilatory Support of COVID-19 Patients Outside the Intensive Care Units (WARd-COVID). Ann. Am. Thorac. Soc. 2021, 18, 1020–1026. [Google Scholar] [CrossRef]
- Radovanovic, D.; Rizzi, M.; Pini, S.; Saad, M.; Chiumello, D.A.; Santus, P. Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal. J. Clin. Med. 2020, 9, 1191. [Google Scholar] [CrossRef]
- Pfeifer, M.; Ewig, S.; Voshaar, T.; Randerath, W.J.; Bauer, T.; Geiseler, J.; Dellweg, D.; Westhoff, M.; Windisch, W.; Schönhofer, B.; et al. Position Paper for the State-of-the-Art Application of Respiratory Support in Patients with COVID-19. Respiration 2020, 99, 521–542. [Google Scholar] [CrossRef]
- Aliberti, S.; Radovanovic, D.; Billi, F.; Sotgiu, G.; Costanzo, M.; Pilocane, T.; Saderi, L.; Gramegna, A.; Rovellini, A.; Perotto, L.; et al. Helmet CPAP Treatment in Patients with COVID-19 Pneumonia: A Multicentre Cohort Study. Eur. Respir. J. 2020, 56, 2001935. [Google Scholar] [CrossRef]
- Alviset, S.; Riller, Q.; Aboab, J.; Dilworth, K.; Billy, P.-A.; Lombardi, Y.; Azzi, M.; Ferreira Vargas, L.; Laine, L.; Lermuzeaux, M.; et al. Continuous Positive Airway Pressure (CPAP) Face-Mask Ventilation Is an Easy and Cheap Option to Manage a Massive Influx of Patients Presenting Acute Respiratory Failure during the SARS-CoV-2 Outbreak: A Retrospective Cohort Study. PLoS ONE 2020, 15, e0240645. [Google Scholar] [CrossRef] [PubMed]
- On Behalf of the UCL Critical Care COVID-19 Research Group; Arina, P.; Baso, B.; Moro, V.; Patel, H.; Ambler, G. Discriminating between CPAP Success and Failure in COVID-19 Patients with Severe Respiratory Failure. Intensive Care Med. 2021, 47, 237–239. [Google Scholar] [CrossRef]
- Vaschetto, R.; Barone-Adesi, F.; Racca, F.; Pissaia, C.; Maestrone, C.; Colombo, D.; Olivieri, C.; De Vita, N.; Santangelo, E.; Scotti, L.; et al. Outcomes of COVID-19 Patients Treated with Continuous Positive Airway Pressure Outside the Intensive Care Unit. ERJ Open Res. 2021, 7, 00541–02020. [Google Scholar] [CrossRef] [PubMed]
- Serafim, R.; Gomes, J.A.; Salluh, J.; Póvoa, P. A Comparison of the Quick-SOFA and Systemic Inflammatory Response Syndrome Criteria for the Diagnosis of Sepsis and Prediction of Mortality. Chest 2018, 153, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yao, N.; Qiu, Y.; He, C. Predictive Performance of SOFA and QSOFA for In-Hospital Mortality in Severe Novel Coronavirus Disease. Am. J. Emerg. Med. 2020, 38, 2074–2080. [Google Scholar] [CrossRef] [PubMed]
- Cole, S.R.; Hernán, M.A. Constructing Inverse Probability Weights for Marginal Structural Models. Am. J. Epidemiol. 2008, 168, 656–664. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; Wiley Series in Probability and Statistics; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 1987; pp. i–xxix. ISBN 978-0-470-31669-6. [Google Scholar]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345. [Google Scholar] [CrossRef]
- Schweickert, W.D.; Pohlman, M.C.; Pohlman, A.S.; Nigos, C.; Pawlik, A.J.; Esbrook, C.L.; Spears, L.; Miller, M.; Franczyk, M.; Deprizio, D.; et al. Early Physical and Occupational Therapy in Mechanically Ventilated, Critically Ill Patients: A Randomised Controlled Trial. Lancet (Lond. Engl.) 2009, 373, 1874–1882. [Google Scholar] [CrossRef]
- Hopkins, R.O.; Suchyta, M.R.; Farrer, T.J.; Needham, D. Improving Post–Intensive Care Unit Neuropsychiatric Outcomes: Understanding Cognitive Effects of Physical Activity. Am. J. Respir. Crit. Care Med. 2012, 186, 1220–1228. [Google Scholar] [CrossRef]
- Grieco, D.L.; Menga, L.S.; Raggi, V.; Bongiovanni, F.; Anzellotti, G.M.; Tanzarella, E.S.; Bocci, M.G.; Mercurio, G.; Dell’Anna, A.M.; Eleuteri, D.; et al. Physiological Comparison of High-Flow Nasal Cannula and Helmet Noninvasive Ventilation in Acute Hypoxemic Respiratory Failure. Am. J. Respir. Crit. Care Med. 2020, 201, 303–312. [Google Scholar] [CrossRef]
- Carteaux, G.; Millán-Guilarte, T.; De Prost, N.; Razazi, K.; Abid, S.; Thille, A.W.; Schortgen, F.; Brochard, L.; Brun-Buisson, C.; Mekontso Dessap, A. Failure of Noninvasive Ventilation for De Novo Acute Hypoxemic Respiratory Failure: Role of Tidal Volume. Crit. Care Med. 2016, 44, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Esteban, A.; Frutos-Vivar, F.; Muriel, A.; Ferguson, N.D.; Peñuelas, O.; Abraira, V.; Raymondos, K.; Rios, F.; Nin, N.; Apezteguía, C.; et al. Evolution of Mortality over Time in Patients Receiving Mechanical Ventilation. Am. J. Respir. Crit. Care Med. 2013, 188, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Thille, A.W.; Muller, G.; Gacouin, A.; Coudroy, R.; Decavèle, M.; Sonneville, R.; Beloncle, F.; Girault, C.; Dangers, L.; Lautrette, A.; et al. Effect of Postextubation High-Flow Nasal Oxygen With Noninvasive Ventilation vs High-Flow Nasal Oxygen Alone on Reintubation Among Patients at High Risk of Extubation Failure: A Randomized Clinical Trial. JAMA 2019, 322, 1465–1475. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Population | Do Not Intubate Order (n = 130) | Intubation Eligible (n = 270) | p Value |
|---|---|---|---|---|
| Male, n (%) | 284 (71) | 87 (67) | 197 (73) | 0.21 |
| Age, years | 70 (61.2–78) | 79.5 (72–84) | 66 (58–73) | <0.0001 |
| Body Mass Index, kg/m2 | 28.4 (24.8–32) | 27.1 (23.2–31.1) | 29 (25.2–32.4) | 0.003 |
| Delay between PCR diagnostic and admission, days | 0 (0–5) | 1 (0–5) | 0 (0–5) | 0.51 |
| Comorbidities | ||||
| Chronic respiratory disease, n (%) | 81 (20) | 32 (24) | 49 (18) | 0.13 |
| Chronic heart disease, n (%) | 110 (27) | 58 (45) | 52 (19) | <0.0001 |
| Hypertension, n (%) | 228 (57) | 83 (64) | 145 (54) | 0.055 |
| Diabetes, n (%) | 175 (44) | 55 (42) | 120 (45) | 0.68 |
| Obesity, n (%) | 149 (37) | 40 (31) | 109 (40) | 0.06 |
| Cancer, n (%) | 41 (10) | 27 (21) | 14 (5) | <0.0001 |
| Neurological pathology, n (%) | 29 (7) | 19 (15) | 10 (3) | <0.0001 |
| Cognitive disorders, n (%) | 37 (9) | 18 (14) | 19 (7) | 0.03 |
| At admission | ||||
| Quick SOFA total score | 1 (1–2) | 1 (1–2) | 1 (1–2) | 0.09 |
| Respiratory rate > 22 c/min, n (%) | 332 (83) | 107 (83) | 225 (83) | 0.79 |
| Glasgow score < 15, n (%) | 80 (20) | 40 (31) | 40 (15) | 0.0002 |
| Systolic BP < 100 mmHg, n (%) | 71 (18) | 21 (16) | 50 (18) | 0.56 |
| PaO2/FiO2, (mmHg) | 140 (95–225) | 138 (101–205) | 143 (92–234) | 0.6 |
| C-reactive protein, (mg/L) | 113 (62.8–170) | 115 (76–140) | 111.5 (53.7–180.3) | 0.75 |
| D-dimer, (µg/L) | 1193 (731–2267) | 1387 (953–2923) | 1098 (700–2000) | 0.019 |
| Fibrinogen, (g/L) | 6.7 (5.8–7.5) | 6.4 (5.2–7.4) | 6.8 (5.9–7.6) | 0.11 |
| Respiratory Support | ||||
| HFNC, n (%) | 311 (78) | 109 (84) | 202 (75) | 0.04 |
| Delay between HFNC and Admission, days | 1 (0–4) | 2 (0–4) | 1 (0–4) | 0.37 |
| HFNC duration, days | 4 (2–7) | 6 (4–9) | 3 (2–5) | <0.0001 |
| CPAP, n (%) | 192 (48) | 74 (57) | 118 (44) | 0.013 |
| Delay between CPAP and Admission, days | 2 (0–4) | 3 (1–5) | 1 (0–4) | 0.01 |
| CPAP duration, days | 4 (2–8) | 6 (3–9) | 3 (2–7) | 0.001 |
| Bi-level NIV, n (%) | 51 (13) | 20 (15) | 31 (12) | 0.27 |
| Delay between Bi-level NIV and Admission, days | 2.5 (0–7) | 8 (0–14) | 2 (0–5) | 0.025 |
| Bi-level NIVduration, days | 3 (2–5) | 3.5 (2–6) | 2 (1–3 | 0.1 |
| IMV, n (%) | 161 (60) | - | 161 (60) | - |
| Delay between IMV and Admission, days | 3 (2–6.5) | - | 3 (2–6.5) | - |
| IMV duration, days | 13 (8–24) | - | 13 (8–24) | - |
| Medication | ||||
| Remdesivir, n (%) | 41 (10) | 18 (14) | 23 (9) | 0.09 |
| Plaquenil, n (%) | 1 (0.2) | 0 (0) | 1 (0.3) | 0.48 |
| Tozicilumab, n (%) | 26 (6) | 9 (7) | 17 (6) | 0.81 |
| Corticosteroids, n (%) | 374 (93) | 120 (92) | 254 (94) | 0.5 |
| Antibiotherapy, n (%) | 290 (72) | 87 (67) | 203 (75) | 0.08 |
| Meropenem, n (%) | 56 (14) | 9 (7) | 47 (18) | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medrinal, C.; Gillet, A.; Boujibar, F.; Dugernier, J.; Zwahlen, M.; Lamia, B.; Girault, C.; Creteur, J.; Fellrath, J.-M.; Haesler, L.; et al. Role of Non-Invasive Respiratory Supports in COVID-19 Acute Respiratory Failure Patients with Do Not Intubate Orders. J. Clin. Med. 2021, 10, 2783. https://doi.org/10.3390/jcm10132783
Medrinal C, Gillet A, Boujibar F, Dugernier J, Zwahlen M, Lamia B, Girault C, Creteur J, Fellrath J-M, Haesler L, et al. Role of Non-Invasive Respiratory Supports in COVID-19 Acute Respiratory Failure Patients with Do Not Intubate Orders. Journal of Clinical Medicine. 2021; 10(13):2783. https://doi.org/10.3390/jcm10132783
Chicago/Turabian StyleMedrinal, Clément, Alexis Gillet, Fairuz Boujibar, Jonathan Dugernier, Marcel Zwahlen, Bouchra Lamia, Christophe Girault, Jacques Creteur, Jean-Marc Fellrath, Laurence Haesler, and et al. 2021. "Role of Non-Invasive Respiratory Supports in COVID-19 Acute Respiratory Failure Patients with Do Not Intubate Orders" Journal of Clinical Medicine 10, no. 13: 2783. https://doi.org/10.3390/jcm10132783
APA StyleMedrinal, C., Gillet, A., Boujibar, F., Dugernier, J., Zwahlen, M., Lamia, B., Girault, C., Creteur, J., Fellrath, J.-M., Haesler, L., Lagache, L., Goubert, L., Artaud Macari, E., Taton, O., Gouin, P., Leduc, D., Van Hove, O., Norrenberg, M., Prieur, G., ... Contal, O. (2021). Role of Non-Invasive Respiratory Supports in COVID-19 Acute Respiratory Failure Patients with Do Not Intubate Orders. Journal of Clinical Medicine, 10(13), 2783. https://doi.org/10.3390/jcm10132783