Serum C-Reactive Protein and Interleukin-6 Levels as Biomarkers for Disease Severity and Clinical Outcomes in Patients with Idiopathic Granulomatous Mastitis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Serum Assays
2.3. Treatments
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Characteristics According to Disease Severity
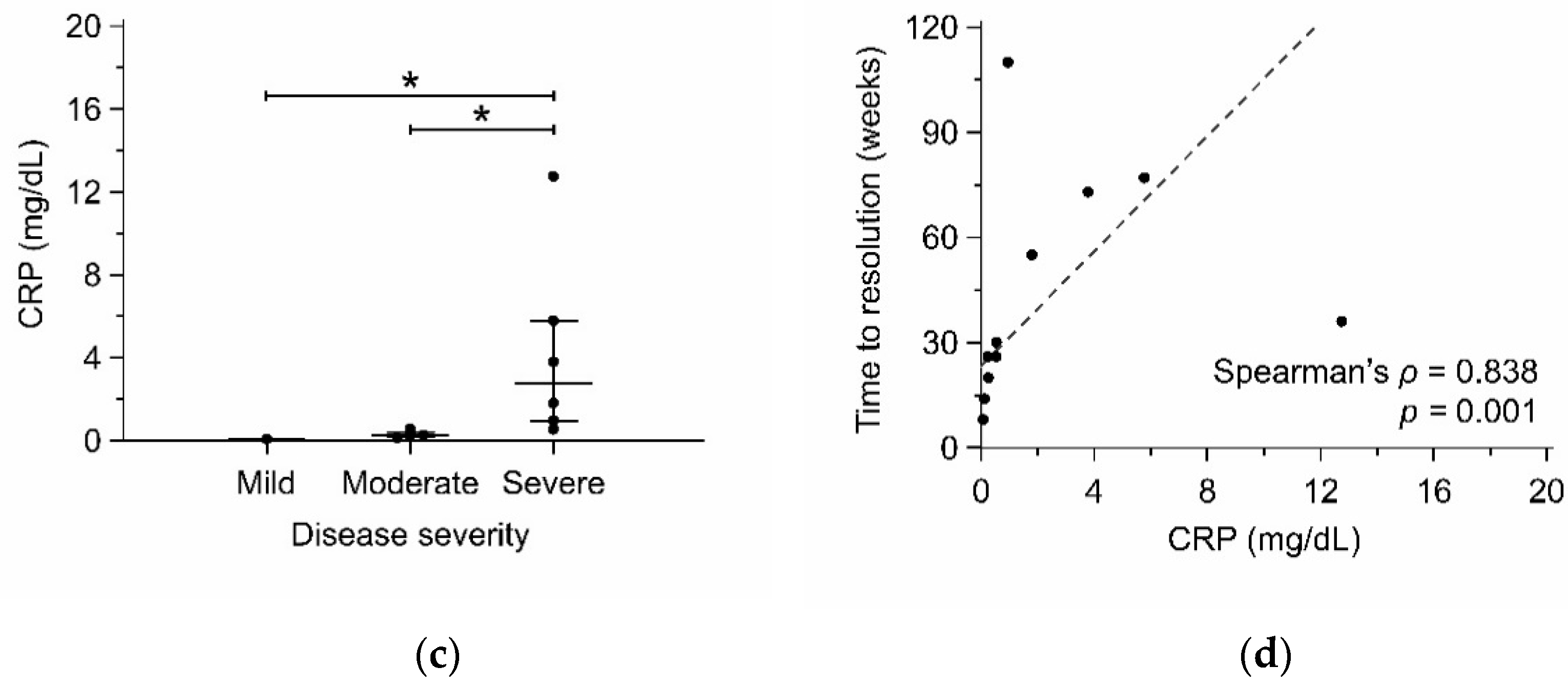
3.2. IL-6 and CRP as Biomarkers for Disease Severity
3.3. Factors Associated with Time to Resolution
3.4. Factors Associated with Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kessler, E.; Wolloch, Y. Granulomatous mastitis: A lesion clinically simulating carcinoma. Am. J. Clin. Pathol. 1972, 58, 642–646. [Google Scholar] [CrossRef] [PubMed]
- Tan, Q.T.; Tay, S.P.; Gudi, M.A.; Nadkarni, N.V.; Lim, S.H.; Chuwa, E.W.L. Granulomatous mastitis and factors associated with recurrence: An 11-year single-centre study of 113 patients in Singapore. World J. Surg. 2019, 43, 1737–1745. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Ramos, D.; Simon-Monterde, L.; Suelves-Piqueres, C.; Queralt-Martin, R.; Granel-Villach, L.; Laguna-Sastre, J.M.; Nicolau, M.J.; Escrig-Sos, J. Idiopathic granulomatous mastitis: A systematic review of 3060 patients. Breast J. 2019, 25, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Sheybani, F.; Naderi, H.R.; Gharib, M.; Sarvghad, M.; Mirfeizi, Z. Idiopathic granulomatous mastitis: Long-discussed but yet-to-be-known. Autoimmunity 2016, 49, 236–239. [Google Scholar] [CrossRef]
- Prasad, S.; Jaiprakash, P.; Dave, A.; Pai, D. Idiopathic granulomatous mastitis: An institutional experience. Turk. J. Surg. 2017, 33, 100–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altintoprak, F.; Kivilcim, T.; Ozkan, O.V. Aetiology of idiopathic granulomatous mastitis. World J. Clin. Cases 2014, 2, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Goulabchand, R.; Hafidi, A.; Van de Perre, P.; Millet, I.; Maria, A.T.J.; Morel, J.; Quellec, A.L.; Perrochia, H.; Guilpain, P. Mastitis in autoimmune diseases: Review of the literature, diagnostic pathway, and pathophysiological key players. J. Clin. Med. 2020, 9, 958. [Google Scholar] [CrossRef] [Green Version]
- Lacambra, M.; Thai, T.A.; Lam, C.C.; Yu, A.M.; Pham, H.T.; Tran, P.V.; Law, B.K.; Van Nguyen, T.; Pham, D.X.; Tse, G.M. Granulomatous mastitis: The histological differentials. J. Clin. Pathol. 2011, 64, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.T.; Lin, J.C.; Li, C.F.; Lee, Y.H. A successful case of etanercept used for idiopathic granulomatous mastitis. Breast J. 2019, 25, 343–345. [Google Scholar] [CrossRef]
- Neel, A.; Hello, M.; Cottereau, A.; Graveleau, J.; De Faucal, P.; Costedoat-Chalumeau, N.; Rondeau-Lutz, M.; Lavigne, C.; Chiche, L.; Hachulla, E.; et al. Long-term outcome in idiopathic granulomatous mastitis: A western multicentre study. QJM 2013, 106, 433–441. [Google Scholar] [CrossRef]
- Raj, N.; Macmillan, R.D.; Ellis, I.O.; Deighton, C.M. Rheumatologists and breasts: Immunosuppressive therapy for granulomatous mastitis. Rheumatology 2004, 43, 1055–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadena-Semanate, R.E.; Estrella-Tapia, L.F.; Contreras-Yametti, F.I.; Contreras-Yametti, J.E.; Salazar-Molina, R.D. Adalimumab in a patient with refractory idiopathic granulomatous mastitis: A case report. Breast J. 2021, 27, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Saydam, M.; Yilmaz, K.B.; Sahin, M.; Yanik, H.; Akinci, M.; Yilmaz, I.; Balas, S.; Azili, C.; Gulcelik, M.A. New findings on autoimmune etiology of idiopathic granulomatous mastitis: Serum IL-17, IL-22 and IL-23 levels of patients. J. Investig. Surg. 2020, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Koksal, H.; Vatansev, H.; Artac, H.; Kadoglou, N. The clinical value of interleukins-8, -10, and -17 in idiopathic granulomatous mastitis. Clin. Rheumatol. 2020, 39, 1671–1677. [Google Scholar] [CrossRef] [PubMed]
- Yigitbasi, M.R.; Guntas, G.; Atak, T.; Sonmez, C.; Yalman, H.; Uzun, H. The role of interleukin-33 as an inflammatory marker in differential diagnosis of idiopathic granulomatous mastitis and breast cancer. J. Investig. Surg. 2017, 30, 272–276. [Google Scholar] [CrossRef]
- Kaviani, A.; Vasigh, M.; Omranipour, R.; Mahmoudzadeh, H.; Elahi, A.; Farivar, L.; Zand, S. Idiopathic granulomatous mastitis: Looking for the most effective therapy with the least side effects according to the severity of the disease in 374 patients in Iran. Breast J. 2019, 25, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Chirappapha, P.; Thaweepworadej, P.; Supsamutchai, C.; Biadul, N.; Lertsithichai, P. Idiopathic granulomatous mastitis: A retrospective cohort study between 44 patients with different treatment modalities. Ann. Med. Surg. 2018, 36, 162–167. [Google Scholar] [CrossRef]
- Cetin, K.; Sikar, H.E.; Goret, N.E.; Rona, G.; Barisik, N.O.; Kucuk, H.F.; Gulluoglu, B.M. Comparison of topical, systemic, and combined therapy with steroids on idiopathic granulomatous mastitis: A prospective randomized study. World J. Surg. 2019, 43, 2865–2873. [Google Scholar] [CrossRef]
- Lei, X.; Chen, K.; Zhu, L.; Song, E.; Su, F.; Li, S. Treatments for idiopathic granulomatous mastitis: Systematic review and meta-analysis. Breastfeed. Med. 2017, 12, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Postolova, A.; Troxell, M.L.; Wapnir, I.L.; Genovese, M.C. Methotrexate in the treatment of idiopathic granulomatous mastitis. J. Rheumatol. 2020, 47, 924–927. [Google Scholar] [CrossRef] [PubMed]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection—A review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erhan, Y.; Veral, A.; Kara, E.; Ozdemir, N.; Kapkac, M.; Ozdedeli, E.; Yilmaz, R.; Koyuncu, A.; Erhan, Y.; Ozbal, O. A clinicopthologic study of a rare clinical entity mimicking breast carcinoma: Idiopathic granulomatous mastitis. Breast 2000, 9, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Ucaryilmaz, H.; Koksal, H.; Emsen, A.; Kadoglou, N.; Dixon, J.M.; Artac, H. The role of regulatory T and B cells in the etiopathogenesis of idiopathic granulomatous mastitis. Immunol. Investig. 2020, 1–11. [Google Scholar] [CrossRef]
- Garbers, C.; Heink, S.; Korn, T.; Rose-John, S. Interleukin-6: Designing specific therapeutics for a complex cytokine. Nat. Rev. Drug Discov. 2018, 17, 395–412. [Google Scholar] [CrossRef]
- Al-Khaffaf, B.; Knox, F.; Bundred, N.J. Idiopathic granulomatous mastitis: A 25-year experience. J. Am. Coll. Surg. 2008, 206, 269–273. [Google Scholar] [CrossRef]
- Davis, J.; Cocco, D.; Matz, S.; Hsu, C.H.; Brown, M.J.; Lee, J.; Bouton, M.E.; Caruso, D.M.; Komenaka, I.K. Re-evaluating if observation continues to be the best management of idiopathic granulomatous mastitis. Surgery 2019, 166, 1176–1180. [Google Scholar] [CrossRef]
- Cetinkaya, O.A.; Celik, S.U.; Terzioglu, S.G.; Eroglu, A. The predictive value of the neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in patients with recurrent idiopathic granulomatous mastitis. Eur. J. Breast Health 2020, 16, 61–65. [Google Scholar] [CrossRef]
- Kim, S.; Eliot, M.; Koestler, D.C.; Wu, W.C.; Kelsey, K.T. Association of neutrophil-to-lymphocyte ratio with mortality and cardiovascular disease in the Jackson Heart Study and modification by the Duffy antigen variant. JAMA Cardiol. 2018, 3, 455–462. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Seruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocana, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [Green Version]
- Azizi, A.; Prasath, V.; Canner, J.; Gharib, M.; Sadat Fattahi, A.; Naser Forghani, M.; Sajjadi, S.; Farhadi, E.; Vasigh, M.; Kaviani, A.; et al. Idiopathic granulomatous mastitis: Management and predictors of recurrence in 474 patients. Breast J. 2020, 26, 1358–1362. [Google Scholar] [CrossRef]
- Yilmaz, T.U.; Gurel, B.; Guler, S.A.; Baran, M.A.; Ersan, B.; Duman, S.; Utkan, Z. Scoring idiopathic granulomatous mastitis: An effective system for predicting recurrence? Eur. J. Breast Health. 2018, 14, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Kany, S.; Vollrath, J.T.; Relja, B. Cytokines in inflammatory disease. Int. J. Mol. Sci. 2019, 20, 6008. [Google Scholar] [CrossRef] [Green Version]
- Chatzileontiadou, D.S.M.; Sloane, H.; Nguyen, A.T.; Gras, S.; Grant, E.J. The many faces of CD4(+) T cells: Immunological and structural characteristics. Int. J. Mol. Sci. 2020, 22, 73. [Google Scholar] [CrossRef]
- Walzl, G.; Ronacher, K.; Hanekom, W.; Scriba, T.J.; Zumla, A. Immunological biomarkers of tuberculosis. Nat. Rev. Immunol. 2011, 11, 343–354. [Google Scholar] [CrossRef]
- Grunewald, J.; Grutters, J.C.; Arkema, E.V.; Saketkoo, L.A.; Moller, D.R.; Muller-Quernheim, J. Sarcoidosis. Nat. Rev. Dis. Primers 2019, 5, 45. [Google Scholar] [CrossRef]
- Xue, J.X.; Ye, B.; Liu, S.; Cao, S.H.; Bian, W.H.; Yao, C. Treatment efficacy of Chuang Ling Ye, a traditional chinese herbal medicine compound, on idiopathic granulomatous mastitis: A randomized controlled trial. Evid. Based. Complement. Alternat. Med. 2020, 2020, 6964801. [Google Scholar] [CrossRef]
- Choy, E.H.; De Benedetti, F.; Takeuchi, T.; Hashizume, M.; John, M.R.; Kishimoto, T. Translating IL-6 biology into effective treatments. Nat. Rev. Rheumatol. 2020, 16, 335–345. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, W.A.; Dasgupta, B.; Luqmani, R.; Unizony, S.H.; Blockmans, D.; Lai, Z.; Kurrasch, R.H.; Lazic, I.; Brown, K.; Rao, R. A multicentre, randomised, double-blind, placebo-controlled, parallel-group study to evaluate the efficacy and safety of sirukumab in the treatment of giant cell arteritis. Rheumatol. Ther. 2020, 7, 793–810. [Google Scholar] [CrossRef]
- Deshayes, S.; Ly, K.H.; Rieu, V.; Maigne, G.; Silva, N.M.; Manrique, A.; Monteil, J.; de Boysson, H.; Aouba, A. French Study Group for Large Vessel Vasculitis (GEFA). Steroid-sparing effect of anakinra in giant-cell arteritis: A case series with clinical, biological and iconographic long-term assessments. Rheumatology 2021. [Google Scholar] [CrossRef]
- Conway, R.; O’Neill, L.; O’Flynn, E.; Gallagher, P.; McCarthy, G.M.; Murphy, C.C.; Veale, D.J.; Fearon, U.; Molloy, E.S. Ustekinumab for the treatment of refractory giant cell arteritis. Ann. Rheum. Dis. 2016, 75, 1578–1579. [Google Scholar] [CrossRef]
- Conway, R.; O’Neill, L.; Gallagher, P.; McCarthy, G.M.; Murphy, C.C.; Veale, D.J.; Fearon, U.; Molloy, E.S. Ustekinumab for refractory giant cell arteritis: A prospective 52-week trial. Semin. Arthritis Rheum. 2018, 48, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Matza, M.A.; Fernandes, A.D.; Stone, J.H.; Unizony, S.H. Ustekinumab for the treatment of giant cell arteritis. Arthritis Care. Res. 2020. [Google Scholar] [CrossRef]
- Rotar, Z.; Tomsic, M.; Hocevar, A. Secukinumab for the maintenance of glucocorticoid-free remission in a patient with giant cell arteritis and psoriatic arthritis. Rheumatology 2018, 57, 934–936. [Google Scholar] [CrossRef] [Green Version]
- Freeman, C.M.; Xia, B.T.; Wilson, G.C.; Lewis, J.D.; Khan, S.; Lee, S.J.; Lower, E.E.; Edwards, M.J.; Shaughnessy, E.A. Idiopathic granulomatous mastitis: A diagnostic and therapeutic challenge. Am. J. Surg. 2017, 214, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Haddad, M.; Sheybani, F.; Arian, M.; Gharib, M. Methotrexate-based regimen as initial treatment of patients with idiopathic granulomatous mastitis. Breast J. 2020, 26, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Berben, L.; Floris, G.; Kenis, C.; Dalmasso, B.; Smeets, A.; Vos, H.; Neven, P.; Antoranz Martinez, A.; Laenen, A.; Wildiers, H.; et al. Age-related remodelling of the blood immunological portrait and the local tumor immune response in patients with luminal breast cancer. Clin. Transl. Immunol. 2020, 9, e1184. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 41) | Mild (n = 5) | Moderate (n = 15) | Severe (n = 21) | p-Value | Adjusted p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mild vs. Moderate | Mild vs. Severe | Moderate vs. Severe | ||||||||||
| Age, mean (SD), years | 35.9 | (5.8) | 34.8 | (4.6) | 35.1 | (4.8) | 36.8 | (6.8) | 0.635 | |||
| Body mass index, median (IQR), kg/m2 | 23.6 | (20.6−26.1) | 22.4 | (20.2−27.0) | 23.9 | (21.1−26.2) | 23.5 | (20.1−27.1) | 0.821 | |||
| Age of menarche, median (IQR), years | 12.0 | (12.0−13.0) | 12.0 | (11.0−14.0) | 13.0 | (12.0−13.0) | 12.0 | (12.0−13.0) | 0.786 | |||
| Pregnancy | 38 | (92.7) | 5 | (100) | 14 | (93.3) | 19 | (90.5) | >0.900 | |||
| Gestation, median (IQR) | 1.0 | (1.0−2.0) | 2.0 | (1.5−2.5) | 1.0 | (1.0−2.0) | 1.0 | (1.0−2.0) | 0.426 | |||
| Age of first pregnancy, mean (SD), years | 31.1 | (6.4) | 31.0 | (5.2) | 30.9 | (5.9) | 31.2 | (7.2) | >0.900 | |||
| Breastfeeding | 37 | (90.2) | 5 | (100) | 14 | (93.3) | 18 | (85.7) | 0.782 | |||
| Smoking | 2 | (4.9) | 1 | (20.0) | 0 | (0.0) | 1 | (4.8) | 0.360 | |||
| Diabetes mellitus | 1 | (2.4) | 1 | (20.0) | 0 | (0.0) | 0 | (0.0) | 0.122 | |||
| Lesion size, median (IQR), cm | 4.0 | (2.1−5.1) | 1.0 | (0.6−1.6) | 3.0 | (2.1−4.8) | 5.0 | (3.8−6.0) | <0.001 | 0.031 | <0.001 | 0.018 |
| Abscess formation | 20 | (48.8) | 0 | (0.0) | 8 | (53.3) | 12 | (57.1) | 0.087 | |||
| Multiple lesions | 29 | (70.7) | 0 | (0.0) | 15 | (100) | 14 | (66.7) | <0.001 | <0.001 | 0.036 | 0.082 |
| Skin ulcer or fistula | 21 | (51.2) | 0 | (0.0) | 6 | (40.0) | 15 | (71.4) | 0.008 | 0.780 | 0.021 | 0.269 |
| Symptom duration, median (IQR), weeks | 8.0 | (3.4−14.5) | 1.3 | (0.5−8.0) | 7.6 | (3.2−13.4) | 10.0 | (5.0−16.4) | 0.111 | |||
| Bilateral lesions | 9 | (22.0) | 0 | (0.0) | 2 | (13.3) | 7 | (33.3) | 0.221 | |||
| Extramammary manifestation | 11 | (26.8) | 2 | (40.0) | 2 | (13.3) | 7 | (33.3) | 0.330 | |||
| Corynebacterium infection | 10 | (24.4) | 0 | (0.0) | 3 | (20.0) | 7 | (33.3) | 0.305 | |||
| C-reactive protein, median (IQR), mg/dL | 0.56 | (0.14−2.89) | 0.08 | (0.05−0.23) | 0.26 | (0.13−0.83) | 1.80 | (0.75−5.14) | <0.001 | 0.571 | 0.002 | 0.007 |
| Methotrexate use | 16 | (39.0) | 1 | (20.0) | 4 | (26.7) | 11 | (52.4) | 0.251 | |||
| Surgery | 14 | (34.1) | 0 | (0.0) | 7 | (46.7) | 7 | (33.3) | 0.162 | |||
| Time to resolution, median (IQR), weeks | 26.3 | (12.4−56.0) | 8.0 | (4.4−15.1) | 20.3 | (13.3−32.6) | 54.7 | (26.1−77.0) | 0.002 | 0.328 | 0.004 | 0.061 |
| Recurrence | 9 | (22.0) | 0 | (0.0) | 1 | (6.7) | 8 | (38.1) | 0.051 | |||
| Cytokines | IGM (n = 11) | HC (n = 7) | p-Value | ||
|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | ||||
| TNF-α, pg/mL | 11.66 | (8.70−24.11) | 7.21 | (4.97−7.21) | <0.001 |
| IL-1β, pg/mL | 2.80 | (1.59−3.52) | 0.21 | (N.D.−1.42) | <0.001 |
| IL-2, pg/mL | 13.77 | (3.97−22.08) | 2.63 | (N.D.−6.97) | 0.023 |
| IL-4, pg/mL | N.D. | N.D. | N.A. | ||
| IL-6, pg/mL | 3.89 | (N.D.−6.09) | N.D. | 0.023 | |
| IL-10, pg/mL | 1.13 | (0.55−1.59) | 1.06 | (0.81−1.99) | 0.892 |
| IL-12p70, pg/mL | 6.39 | (6.24−6.98) | 6.10 | (5.95−6.10) | 0.016 |
| IL-17A, pg/mL | 1.13 | (0.41−1.98) | N.D. | 0.041 | |
| IL-22, pg/mL | N.D. | (N.D.−14.29) | N.D. | (N.D.−48.66) | 0.885 |
| IL-23, pg/mL | N.D. | N.D. | N.A. | ||
| GM-CSF, pg/mL | N.D. | (N.D.−3.52) | N.D. | 0.118 | |
| Characteristics (n = 41) | Simple Linear Regression | |||||
|---|---|---|---|---|---|---|
| Unstandardized B (SE) | 95% CI | p-Value | ||||
| Age, years | −0.009 | (0.029) | −0.069 | to | 0.050 | 0.756 |
| Body mass index, kg/m2 | 0.064 | (0.887) | −1.731 | to | 1.858 | >0.900 |
| Age of menarche, years | 0.501 | (1.542) | −2.618 | to | 3.621 | 0.747 |
| Pregnancy | −1.012 | (0.630) | −2.285 | to | 0.262 | 0.116 |
| Gestation | 0.037 | (0.332) | −0.636 | to | 0.710 | >0.900 |
| Age of first pregnancy, years | 0.026 | (0.028) | −0.030 | to | 0.082 | 0.345 |
| Breastfeeding | −1.188 | (0.538) | −2.276 | to | −0.100 | 0.033 |
| Smoking | −1.650 | (0.740) | −3.147 | to | −0.153 | 0.032 |
| Diabetes mellitus | −1.175 | (1.081) | −3.362 | to | 1.012 | 0.284 |
| Lesion size, cm | 0.435 | (0.287) | −0.146 | to | 1.015 | 0.138 |
| Abscess formation | 0.417 | (0.332) | −0.255 | to | 1.088 | 0.217 |
| Multiple lesions | 0.674 | (0.356) | −0.047 | to | 1.394 | 0.066 |
| Skin ulcer or fistula | 1.480 | (0.242) | 0.991 | to | 1.969 | <0.001 |
| Symptom duration, weeks | 0.083 | (0.129) | −0.179 | to | 0.345 | 0.525 |
| Bilateral lesions | 1.325 | (0.350) | 0.618 | to | 2.032 | <0.001 |
| Extramammary manifestation | 0.466 | (0.375) | −0.292 | to | 1.224 | 0.221 |
| Corynebacterium infection | 0.666 | (0.380) | −0.102 | to | 1.434 | 0.087 |
| C-reactive protein, mg/dL | 0.404 | (0.071) | 0.260 | to | 0.548 | <0.001 |
| Methotrexate use | 1.203 | (0.289) | 0.619 | to | 1.787 | <0.001 |
| Surgery | −0.131 | (0.356) | −0.852 | to | 0.590 | 0.715 |
| Recurrence | 0.784 | (0.389) | −0.003 | to | 1.572 | 0.051 |
| Characteristics (n = 41) | Multiple Linear Regression (Backward) | |||||
|---|---|---|---|---|---|---|
| Unstandardized B (SE) | 95% CI | p-Value | ||||
| Breastfeeding | −0.724 | (0.339) | −1.414 | to | −0.034 | 0.040 |
| Smoking | −1.001 | (0.489) | −1.898 | to | 0.091 | 0.074 |
| Bilateral lesions | 0.549 | (0.266) | 0.008 | to | 1.089 | 0.047 |
| C-reactive protein, mg/dL | 0.322 | (0.086) | 0.148 | to | 0.497 | <0.001 |
| Methotrexate use | 0.707 | (0.230) | 0.239 | to | 1.176 | 0.004 |
| Recurrence | −0.612 | (0.322) | −1.266 | to | 0.042 | 0.066 |
| Characteristics (n = 41) | Univariate Logistic Regression | ||||
|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p-Value | |||
| Age, years | 1.179 | 1.000 | to | 1.390 | 0.049 |
| Body mass index, kg/m2 | 0.969 | 0.827 | to | 1.135 | 0.697 |
| Age of menarche, years | 1.113 | 0.604 | to | 2.052 | 0.731 |
| Pregnancy | 0.533 | 0.043 | to | 6.655 | 0.625 |
| Gestation | 1.817 | 0.873 | to | 3.783 | 0.110 |
| Age of first pregnancy, years | 1.027 | 0.904 | to | 1.166 | 0.687 |
| Breastfeeding | 0.828 | 0.075 | to | 9.074 | 0.877 |
| Smoking | N.A. | ||||
| Diabetes mellitus | N.A. | ||||
| Lesion size, cm | 1.165 | 0.737 | to | 1.843 | 0.514 |
| Abscess formation | 2.571 | 0.545 | to | 12.139 | 0.233 |
| Multiple lesions | 1.591 | 0.279 | to | 9.066 | 0.601 |
| Skin ulcer or fistula | 11.692 | 1.302 | to | 105.028 | 0.028 |
| Symptom duration, weeks | 1.016 | 0.975 | to | 1.059 | 0.456 |
| Bilateral lesions | 4.320 | 0.851 | to | 21.929 | 0.078 |
| Extramammary manifestation | 2.857 | 0.601 | to | 13.586 | 0.187 |
| Corynebacterium infection | 0.857 | 0.147 | to | 4.999 | 0.864 |
| C-reactive protein, mg/dL | 1.874 | 1.139 | to | 3.084 | 0.013 |
| Methotrexate use | 4.400 | 0.911 | to | 21.248 | 0.065 |
| Surgery | 0.955 | 0.199 | to | 4.571 | >0.900 |
| Time to resolution, weeks | 1.015 | 0.993 | to | 1.038 | 0.171 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-M.; Lo, C.; Cheng, C.-F.; Lu, C.-H.; Hsieh, S.-C.; Li, K.-J. Serum C-Reactive Protein and Interleukin-6 Levels as Biomarkers for Disease Severity and Clinical Outcomes in Patients with Idiopathic Granulomatous Mastitis. J. Clin. Med. 2021, 10, 2077. https://doi.org/10.3390/jcm10102077
Huang Y-M, Lo C, Cheng C-F, Lu C-H, Hsieh S-C, Li K-J. Serum C-Reactive Protein and Interleukin-6 Levels as Biomarkers for Disease Severity and Clinical Outcomes in Patients with Idiopathic Granulomatous Mastitis. Journal of Clinical Medicine. 2021; 10(10):2077. https://doi.org/10.3390/jcm10102077
Chicago/Turabian StyleHuang, Yi-Min, Chiao Lo, Chiao-Feng Cheng, Cheng-Hsun Lu, Song-Chou Hsieh, and Ko-Jen Li. 2021. "Serum C-Reactive Protein and Interleukin-6 Levels as Biomarkers for Disease Severity and Clinical Outcomes in Patients with Idiopathic Granulomatous Mastitis" Journal of Clinical Medicine 10, no. 10: 2077. https://doi.org/10.3390/jcm10102077