
Combined Cardiac Risk Factors Predict COVID-19 Related Mortality and the Need for Mechanical Ventilation in Coptic Clergy


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Patients
2.2. Cardiovascular Risk Factor Assessment
2.3. Clinical Events
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Indices for Clergy with COVID-19
3.2. Demographic and Clinical Data of Clergy with and without AH
3.3. Geographical Impact on Clinical Events
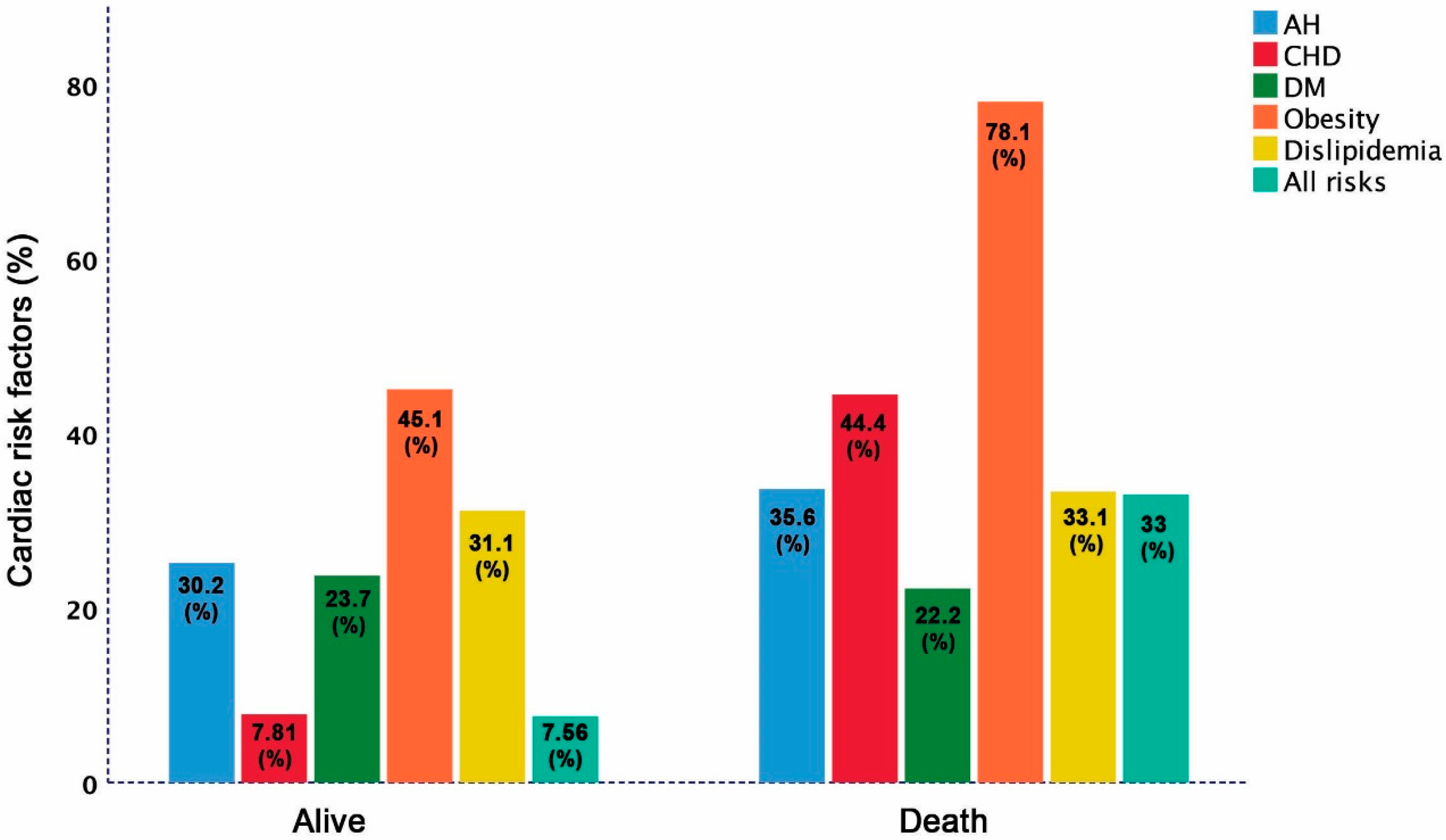
3.4. Distribution of Cardiac Risk Factors among Clergy with and without Adverse Clinical Events
3.5. Predictors of COVID-19-Related Adverse Clinical Events
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Weiss, P.; Murdoch, D.R. Clinical course and mortality risk of severe COVID-19. Lancet 2020, 395, 1014–1015. [Google Scholar] [CrossRef]
- Pillaye, J. Covid-19 and ethnic minorities: The Public Health England report distracts from proactive and timely intervention. BMJ 2020, 370, m3054. [Google Scholar] [CrossRef] [PubMed]
- Keys, C.; Nanayakkara, G.; Onyejekwe, C.; Sah, R.K.; Wright, T. Health Inequalities and Ethnic Vulnerabilities During COVID-19 in the UK: A Reflection on the PHE Reports. Fem. Leg. Stud. 2021, 14, 1–12. [Google Scholar]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; COVID-19 Systematic Urgent Review Group Effort (SURGE) Study Authors. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- WHO. Infection Prevention and Control during Health Care When Novel Coronavirus (nCoV) Infection Is Suspected. Interim Guidance. 2020. Available online: https://apps.who.int/iris/rest/bitstreams/1266296/retrieve (accessed on 1 March 2020).
- Li, Y.D.; Chi, W.Y.; Su, J.H.; Ferrall, L.; Hung, C.F.; Wu, T.C. Coronavirus vaccine development: From SARS and MERS to COVID-19. J. Biomed. Sci. 2020, 27, 104. [Google Scholar] [CrossRef]
- Izda, V.; Jeffries, M.A.; Sawalha, A.H. COVID-19: A review of therapeutic strategies and vaccine candidates. Clin. Immunol. 2021, 222, 108634. [Google Scholar] [CrossRef] [PubMed]
- Henein, M.Y.; Bytyçi, I.; Nicoll, R.; Shenouda, R.; Ayad, S.; Vanchari, F.; Cameli, M. Obesity strongly predicts COVID-19-related major clinical adverse events in Coptic Clergy. 2021; submitted. [Google Scholar]
- D’Agostino, R.B., Sr.; Pencina, M.J.; Massaro, J.M.; Coady, S. Cardiovascular Disease Risk Assessment: Insights from Framingham. Glob. Heart 2013, 8, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Kannel, W.B. Framingham study insights into hypertensive risk of cardiovascular disease. Hypertens Res. 1995, 18, 181–196. [Google Scholar] [CrossRef] [Green Version]
- Wood, D.A.; Kotseva, K.; Connolly, S.; Jennings, C.; Mead, A.; Jones, J.; Holden, A.; de Bacquer, D.; Collier, T.; de Backer, G.; et al. Nurse-coordinated multidisciplinary, family-based cardiovascular disease prevention programme (EUROACTION) for patients with coronary heart disease and asymptomatic individuals at high risk of cardiovascular disease: A paired, cluster-randomised controlled trial. Lancet 2008, 371, 1999–2012. [Google Scholar]
- Kones, R. Primary prevention of coronary heart disease: Integration of new data, evolving views, revised goals, and role of rosuvastatin in management. A comprehensive survey. Drug Des. Dev. Ther. 2011, 5, 325–380. [Google Scholar] [CrossRef] [Green Version]
- Madjid, M.; Solomon, S.; Vardeny, O. ACC Clinical Bulletin: Cardiac Implications of Novel Wuhan Coronavirus (2019-nCoV). Available online: https://www.acc.org/latest-in-cardiology/articles/2020/02/13/12/42/acc-clinical-bulletin-focuses-on-cardiac-implications-of-coronavirus-2019-ncov (accessed on 13 February 2020).
- Rozanski, A.; Bavishi, C.; Kubzansky, L.D.; Cohen, R. Association of Optimism with Cardiovascular Events and All-Cause Mortality: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e1912200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, T.W.; Andercheck, B.; Tom, J.C.; Martinez, B.C.; Stroope, S. Occupational conditions, self-care, and obesity among clergy in the United States. Soc. Sci. Res. 2015, 49, 249–263. [Google Scholar] [CrossRef]
- Proeschold-Bell, R.J.; LeGrand, S.H. High rates of obesity and chronic disease among United Methodist clergy. Obesity 2010, 18, 1867–1870. [Google Scholar] [CrossRef]
- Lucas, C.; Team, Y.I.; Wong, P.; Klein, J.; Castro, T.B.R.; Silva, J.; Sundaram, M.; Ellingson, M.K.; Mao, T.; Oh, J.E.; et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature 2020, 584, 463–469. [Google Scholar] [CrossRef]
- Bae, S.; Kim, S.R.; Kim, M.; Shim, W.J.; Park, S.-M. Impact of cardiovascular disease and risk factors on fatal outcomes in patients with COVID-19 according to age: A systematic review and meta-analysis. Heart 2021, 107, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Chiappetta, S.; Sharma, A.M.; Bottino, V.; Stier, C. COVID-19 and the role of chronic inflammation in patients with obesity. Int. J. Obes. 2020, 44, 1790–1792. [Google Scholar] [CrossRef]
- Mohammad, S.; Aziz, R.; Al Mahri, S.; Malik, S.S.; Haji, E.; Khan, A.H.; Khatlani, T.S.; Bouchama, A. Obesity and COVID-19: What makes obese host so vulnerable? Immun. Ageing 2021, 18, 1. [Google Scholar] [CrossRef]
- Trump, S.; Lukassen, S.; Anker, M.S.; Chua, R.L.; Liebig, J.; Thürmann, L.; Corman, V.M.; Binder, M.; Loske, J.; Klasa, C.; et al. Hypertension delays viral clearance and exacerbates airway hyperinflammation in patients with COVID-19. Nat. Biotechnol. 2020. [Google Scholar] [CrossRef]
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Clergy | Clergy AH- | Clergy AH+ | p |
|---|---|---|---|---|
| (n = 213) | (n = 136) | (n = 77) | Value | |
| Demographic and Clinical Data | ||||
| Age (years) | 49.6 ± 12 | 46.3 ± 11 | 56.1± 11 | <0.001 |
| BMI (m/kg2) | 31.9 ± 6.2 | 31.5 ± 6.3 | 33.1 ± 5.9 | 0.09 |
| SBP (mmHg) | 127 ± 13 | 121 ± 8.5 | 135 ± 14 | <0.001 |
| DBP (mmHg) | 83 ± 9.1 | 81 ± 6.6 | 87 ± 11 | <0.001 |
| Underweight (n, %) | 0 (0) | 0 (0) | 0 (0) | 0.91 |
| Normal weight (n, %) | 17 (7.9) | 12 (9.3) | 5 (6.3) | 0.12 |
| Overweight (n, %) | 74 (34.7) | 54 (39.7) | 20 (15.5) | 0.02 |
| Obese (n, %) | 122 (57.3) | 70 (51.7) | 52 (68.2) | 0.04 |
| DM (n, %) | 59 (27.7) | 26 (19.1) | 33 (43.2) | 0.001 |
| Dyslipidemia | 68 (31.9) | 22 (16.4) | 46 (60.6) | 0.001 |
| CHD (n, %) | 20 (9.4) | 10 (7.4) | 10 (13.6) | 0.04 |
| Family history of CHD (n, %) | 22 (10.3) | 10 (7.4) | 12 (15.6) | 0.01 |
| Family history of stroke (n, %) | 16 (7.5) | 6 (4.76) | 10 (10.3) | 0.04 |
| Variable | Clergy | Clergy AH- | Clergy AH+ | p |
|---|---|---|---|---|
| (n = 213) | (n = 136) | (n = 77) | Value | |
| Outcome data | ||||
| Home treatment (n, %) | 171 (80.2) | 110 (81.6) | 61 (78.7) | 0.55 |
| Hospital treatment (n, %) | 36 (16.9) | 21 (15.4) | 15 (19.7) | 0.23 |
| Intensive care (n, %) | 17 (7.9) | 11 (8.3) | 6 (8.3) | 0.81 |
| Prevalence (%) | 13.6 | 10.2 | 20.1 | 0.001 |
| Mechanical ventilator (n, %) | 15 (7.1) | 8 (5.9) | 7 (9.1) | 0.09 |
| Death (n, %) | 10 (4.69) | 5 (3.68) | 5 (6.49) | 0.058 |
| Variable | EU +USA | Northern Egypt | Southern Egypt | p |
|---|---|---|---|---|
| (n = 31) | (n = 136) | (n = 46) | Value | |
| Death (n, %) | 0 (0) | 7 (5.22) | 3 (6.51) a,b | 0.001 |
| Clergy AH- | 0 (0%) | 4 (4.71) | 2 (6.21) a,b | 0.01 |
| Clergy AH+ | 0 (0%) | 3 (5.88) | 1 (7.10) a,b | 0.02 |
| Variable | Univariate Predictors | p | Multivariate Predictors | p |
|---|---|---|---|---|
| OR (95% CI) | Value | OR (95% CI) | Value | |
| Mortality | ||||
| Diabetes | 0.845 (0.045 to 2.896) | 0.02 | 1.003 (0.202 to 3.804) | 0.09 |
| Obesity | 2.301 (1.002 to 4.094) | 0.03 | 3.403 (1.902 to 4.694) | 0.04 |
| AH | 0.918 (0.103 to 2.191) | 0.04 | 1.403 (0.802 to 4.001) | 0.23 |
| Dyslipidemia | 1.031 (0.007 to 4.019) | 0.11 | 2.003 (1.002 to 4.309) | 0.33 |
| CHD | 1.219 (1.098 to 3.004) | 0.001 | 1.607 (0.982 to 3.051) | 0.02 |
| Family history for CHD | 0.605 (0.025 to 4.106) | 0.21 | ||
| Family history for stroke | 0.729 (0.171 to 2.649) | 0.42 | ||
| Diabetes | 0.845 (0.045 to 2.896) | 0.02 | 0.146 (0.013 to 1.189) | 0.08 |
| Obesity | 2.301 (1.002 to 4.094) | 0.03 | 3.174 (0.254 to 9.679) | 0.31 |
| AH | 0.918 (0.103 to 2.191) | 0.04 | 0.587 (0.003 to 5.191) | 0.63 |
| Dyslipidemia | 1.031 (0.007 to 4.019) | 0.11 | 0.707 (0.101 to 4.201) | 0.63 |
| CHD | 1.219 (1.098 to 3.004) | 0.001 | 0.936 (1.082 to 8.517) | 0.86 |
| Model * | 2.400 (0.509 to 1.400) | 0.001 | 3.991 (1.919 to 6.844) | 0.002 |
| Mechanical ventilation | ||||
| Diabetes | 0.641 (0.077 to 3.377) | 0.51 | 0.641 (0.077 to 3.377) | 0.63 |
| Obesity | 3.872 (1.771 to 10.72) | 0.01 | 3.872 (1.771 to 10.72) | 0.01 |
| AH | 2.347 (1.197 to 4.501) | 0.03 | 2.347 (1.197 to 4.501) | 0.23 |
| Dyslipidemia | 1.056 (0.310 to 3.594) | 0.87 | 1.056 (0.310 to 3.594) | 0.77 |
| CHD | 5.321 (1.410 to 9.908) | 0.01 | 5.321 (1.410 to 9.908) | 0.01 |
| Diabetes | 0.641 (0.077 to 3.377) | 0.51 | 0.209 (0.027 to 1.616) | 0.13 |
| Obesity | 3.872 (1.771 to 10.72) | 0.01 | 1.358 (0.273 to 6.748) | 0.27 |
| AH | 2.347 (1.197 to 4.501) | 0.03 | 0.067 (0.007 to 1.145) | 0.06 |
| Dyslipidemia | 1.056 (0.310 to 3.594) | 0.87 | 0.098 (0.010 to 7.104) | 0.81 |
| CHD | 5.321 (1.410 to 9.908) | 0.01 | 3.235 (0.451 to 23.19) | 0.24 |
| Model ** | 1.807 (0.750 to 2.991) | <0.001 | 1.501 (0.809 to 6.108) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henein, M.Y.; Bytyçi, I.; Nicoll, R.; Shenouda, R.; Ayad, S.; Cameli, M.; Vancheri, F. Combined Cardiac Risk Factors Predict COVID-19 Related Mortality and the Need for Mechanical Ventilation in Coptic Clergy. J. Clin. Med. 2021, 10, 2066. https://doi.org/10.3390/jcm10102066
Henein MY, Bytyçi I, Nicoll R, Shenouda R, Ayad S, Cameli M, Vancheri F. Combined Cardiac Risk Factors Predict COVID-19 Related Mortality and the Need for Mechanical Ventilation in Coptic Clergy. Journal of Clinical Medicine. 2021; 10(10):2066. https://doi.org/10.3390/jcm10102066
Chicago/Turabian StyleHenein, Michael Y., Ibadete Bytyçi, Rachel Nicoll, Rafik Shenouda, Sherif Ayad, Matteo Cameli, and Federico Vancheri. 2021. "Combined Cardiac Risk Factors Predict COVID-19 Related Mortality and the Need for Mechanical Ventilation in Coptic Clergy" Journal of Clinical Medicine 10, no. 10: 2066. https://doi.org/10.3390/jcm10102066
APA StyleHenein, M. Y., Bytyçi, I., Nicoll, R., Shenouda, R., Ayad, S., Cameli, M., & Vancheri, F. (2021). Combined Cardiac Risk Factors Predict COVID-19 Related Mortality and the Need for Mechanical Ventilation in Coptic Clergy. Journal of Clinical Medicine, 10(10), 2066. https://doi.org/10.3390/jcm10102066