Health-Related Quality of Life Trajectories across 10 Years after Moderate to Severe Traumatic Brain Injury in Norway

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analysis
3. Results
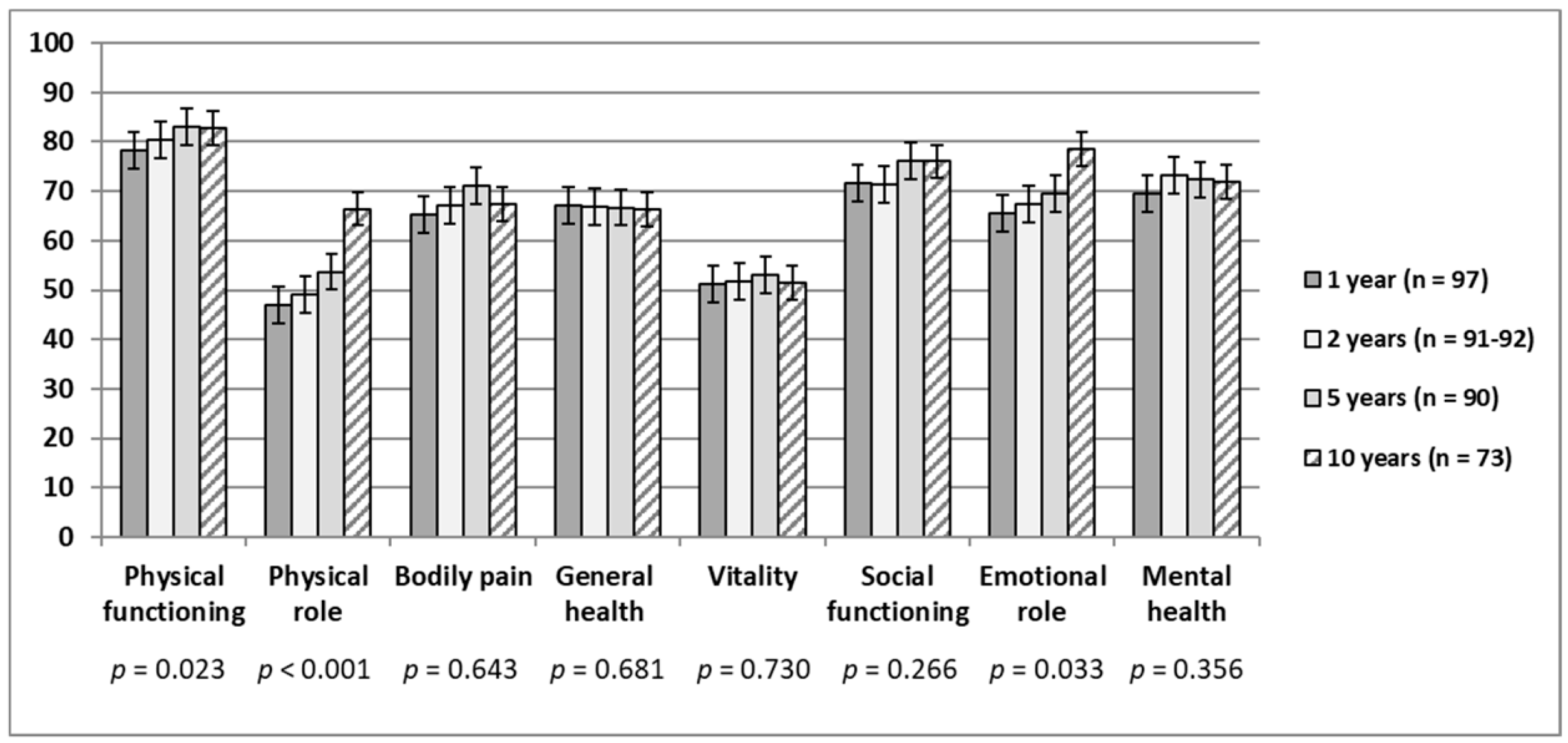
3.1. SF-36 Subscale and Component Summary Score Changes over Time
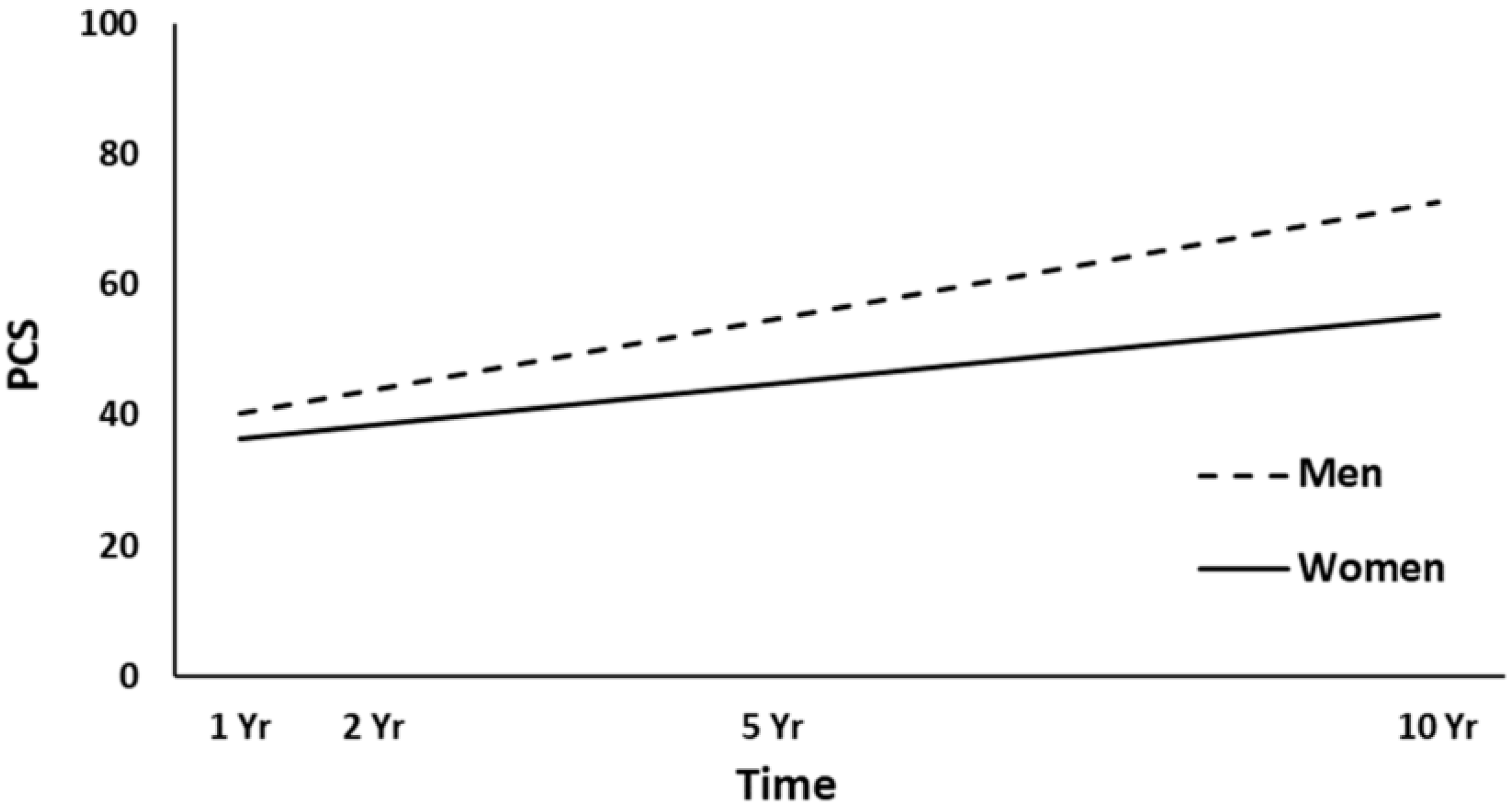
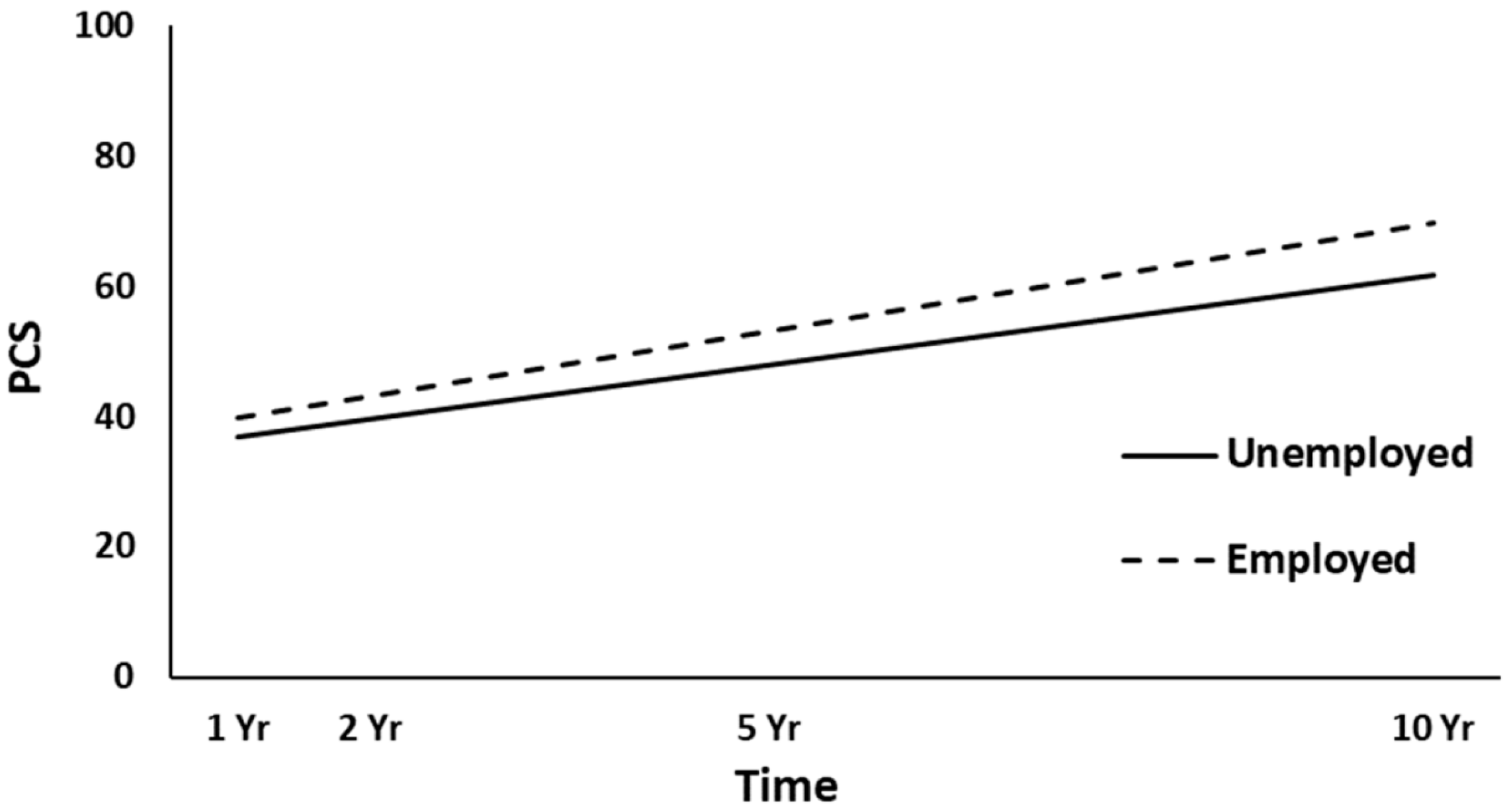
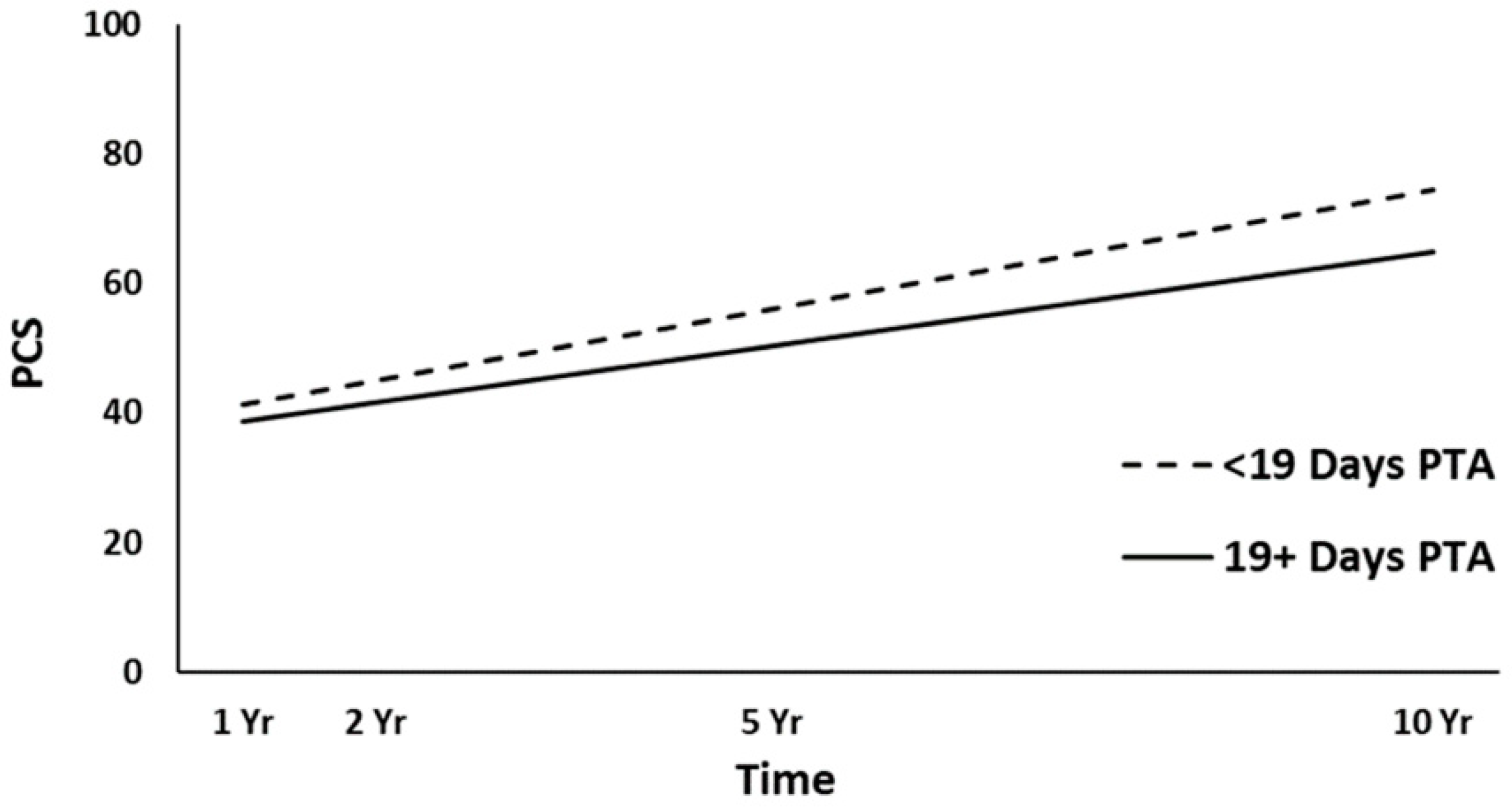
3.2. Physical Health (PCS) Trajectories
3.2.1. Unconditional and Unconditional Growth Models
3.2.2. Full Models
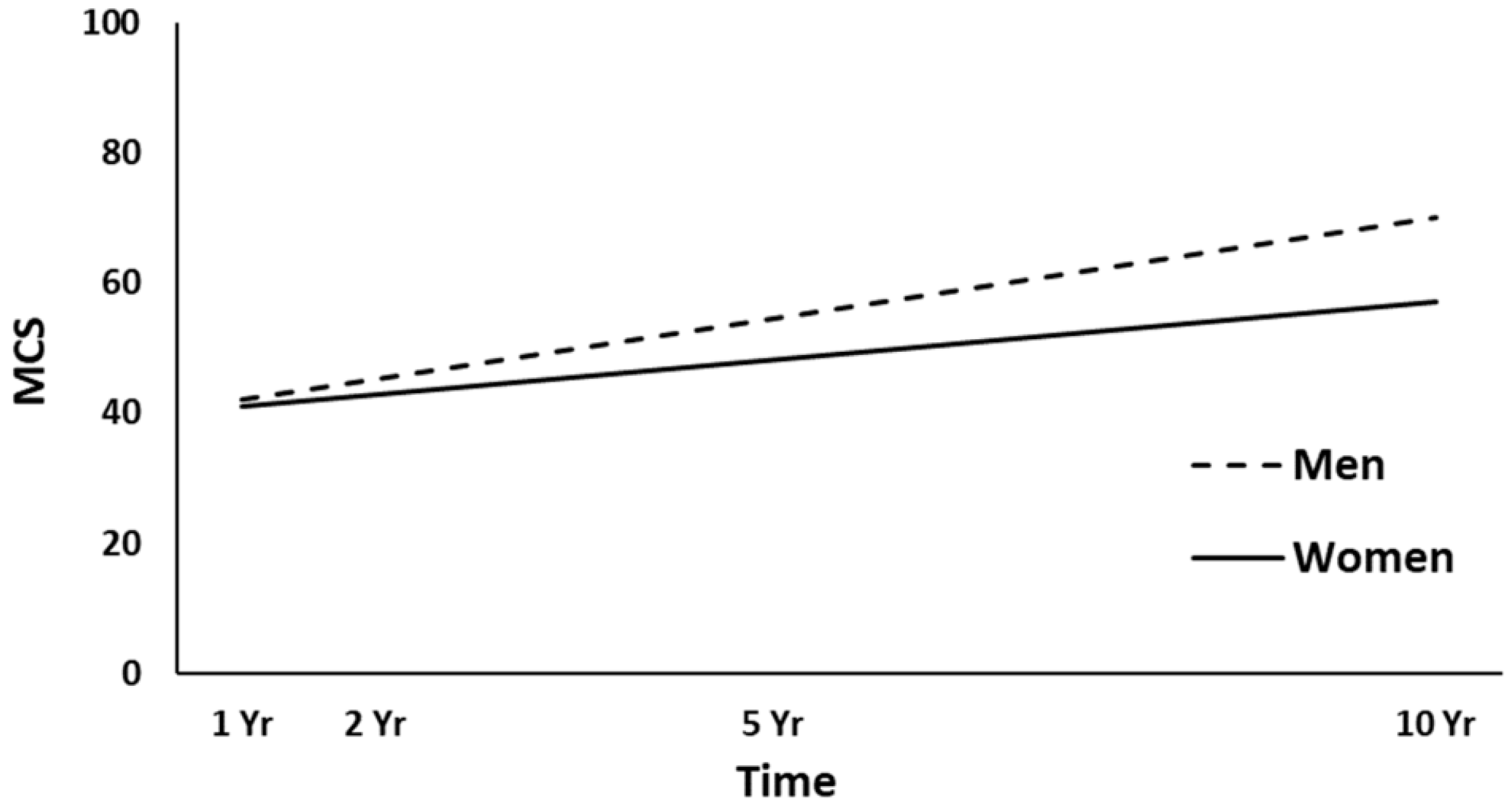
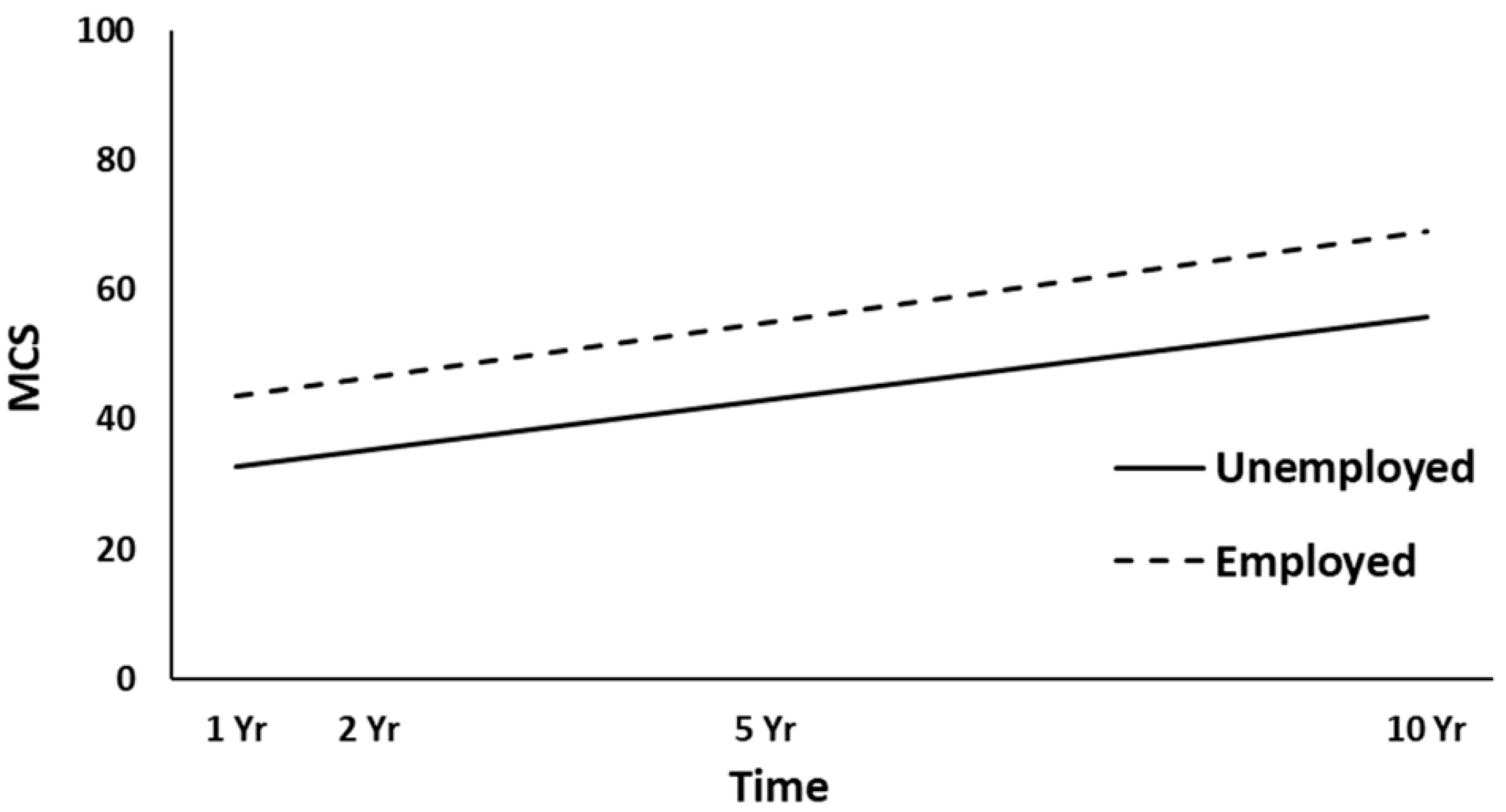
3.3. Mental Health (MCS) Trajectories
3.3.1. Unconditional and Unconditional Growth Models
3.3.2. Full Models
4. Discussion
4.1. Changes in SF-36 Subscales and Component Summary Scores
4.2. Predictors of Physical and Mental Health Trajectories
4.3. Limitations, Strengths, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilson, L.; Stewart, W.; Dams-O’Connor, K.; Diaz-Arrastia, R.; Horton, L.; Menon, D.K.; Polinder, S. The chronic and evolving neurological consequences of traumatic brain injury. Lancet Neurol. 2017, 16, 813–825. [Google Scholar] [CrossRef]
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Büki, A.; Chesnut, R.M.; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef]
- Arango-Lasprilla, J.C.; Krch, D.; Drew, A.; De Los Reyes Aragon, C.J.; Stevens, L.F. Health-related quality of life of individuals with traumatic brain injury in Barranquilla, Colombia. Brain Inj. 2012, 26, 825–833. [Google Scholar] [CrossRef]
- Polinder, S.; Haagsma, J.A.; van Klaveren, D.; Steyerberg, E.W.; van Beeck, E.F. Health-related quality of life after TBI: A systematic review of study design, instruments, measurement properties, and outcome. Popul. Health Metr. 2015, 13, 4. [Google Scholar] [CrossRef] [PubMed]
- von Steinbüchel, N.; Meeuwsen, M.; Zeldovich, M.; Vester, J.C.; Maas, A.; Koskinen, S.; Covic, A. Differences in Health-Related Quality of Life after Traumatic Brain Injury between Varying Patient Groups: Sensitivity of a Disease-Specific (QOLIBRI) and a Generic (SF-36) Instrument. J. Neurotrauma 2020, 37, 1242–1254. [Google Scholar] [CrossRef] [PubMed]
- Nichol, A.D.; Higgins, A.M.; Gabbe, B.J.; Murray, L.J.; Cooper, D.J.; Cameron, P.A. Measuring functional and quality of life outcomes following major head injury: Common scales and checklists. Injury 2011, 42, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Findler, M.; Cantor, J.; Haddad, L.; Gordon, W.; Ashman, T. The reliability and validity of the SF-36 health survey questionnaire for use with individuals with traumatic brain injury. Brain Inj. 2001, 15, 715–723. [Google Scholar] [CrossRef]
- Guilfoyle, M.R.; Seeley, H.M.; Corteen, E.; Harkin, C.; Richards, H.; Menon, D.K.; Hutchinson, P.J. Assessing quality of life after traumatic brain injury: Examination of the short form 36 health survey. J. Neurotrauma 2010, 27, 2173–2181. [Google Scholar] [CrossRef]
- Andelic, N.; Hammergren, N.; Bautz-Holter, E.; Sveen, U.; Brunborg, C.; Roe, C. Functional outcome and health-related quality of life 10 years after moderate-to-severe traumatic brain injury. Acta Neurol. Scand. 2009, 120, 16–23. [Google Scholar] [CrossRef]
- Colantonio, A.; Dawson, D.R.; McLellan, B.A. Head injury in young adults: Long-term outcome. Arch. Phys. Med. Rehabil. 1998, 79, 550–558. [Google Scholar] [CrossRef]
- Emanuelson, I.; Andersson, H.E.; Bjorklund, R.; Stalhammar, D. Quality of life and post-concussion symptoms in adults after mild traumatic brain injury: A population-based study in western Sweden. Acta Neurol. Scand. 2003, 108, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Nestvold, K.; Stavem, K. Determinants of health-related quality of life 22 years after hospitalization for traumatic brain injury. Brain Inj. 2009, 23, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Gorgoraptis, N.; Zaw-Linn, J.; Feeney, C.; Tenorio-Jimenez, C.; Niemi, M.; Malik, A.; Ham, T.; Goldstone, A.P.; Sharp, D.J. Cognitive impairment and health-related quality of life following traumatic brain injury. NeuroRehabilitation 2019, 44, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Jacobsson, L.J.; Westerberg, M.; Lexell, J. Health-related quality-of-life and life satisfaction 6–15 years after traumatic brain injuries in northern Sweden. Brain Inj. 2010, 24, 1075–1086. [Google Scholar] [CrossRef]
- Andelic, N.; Howe, E.I.; Hellstrøm, T.; Sanchez, M.F.; Lu, J.; Løvstad, M.; Røe, C. Disability and quality of life 20 years after traumatic brain injury. Brain Behav. 2018, 8, e01018. [Google Scholar] [CrossRef]
- Grauwmeijer, E.; Heijenbrok-Kal, M.H.; Peppel, L.D.; Hartjes, C.J.; Haitsma, I.K.; de Koning, I.; Ribbers, G.M. Cognition, Health-Related Quality of Life, and Depression Ten Years after Moderate to Severe Traumatic Brain Injury: A Prospective Cohort Study. J. Neurotrauma 2018, 35, 1543–1551. [Google Scholar] [CrossRef]
- Grauwmeijer, E.; Heijenbrok-Kal, M.H.; Ribbers, G.M. Health-related quality of life 3 years after moderate to severe traumatic brain injury: A prospective cohort study. Arch. Phys. Med. Rehabil. 2014, 95, 1268–1276. [Google Scholar] [CrossRef]
- Diaz, A.P.; Schwarzbold, M.L.; Thais, M.E.; Hohl, A.; Bertotti, M.M.; Schmoeller, R.; Nunes, J.C.; Prediger, R.; Linhares, M.N.; Guarnieri, R.; et al. Psychiatric disorders and health-related quality of life after severe traumatic brain injury: A prospective study. J. Neurotrauma 2012, 29, 1029–1037. [Google Scholar] [CrossRef]
- Forslund, M.V.; Roe, C.; Sigurdardottir, S.; Andelic, N. Predicting health-related quality of life 2 years after moderate-to-severe traumatic brain injury. Acta Neurol. Scand. 2013, 128, 220–227. [Google Scholar] [CrossRef]
- Steadman-Pare, D.; Colantonio, A.; Ratcliff, G.; Chase, S.; Vernich, L. Factors associated with perceived quality of life many years after traumatic brain injury. J. Head Trauma Rehabil. 2001, 16, 330–342. [Google Scholar] [CrossRef] [PubMed]
- Haagsma, J.A.; Scholten, A.C.; Andriessen, T.M.; Vos, P.E.; Van Beeck, E.F.; Polinder, S. Impact of depression and post-traumatic stress disorder on functional outcome and health-related quality of life of patients with mild traumatic brain injury. J. Neurotrauma 2015, 32, 853–862. [Google Scholar] [CrossRef]
- Ulfarsson, T.; Lundgren-Nilsson, A.; Blomstrand, C.; Nilsson, M. A history of unemployment or sick leave influences long-term functioning and health-related quality-of-life after severe traumatic brain injury. Brain Inj. 2014, 28, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Tsyben, A.; Guilfoyle, M.; Timofeev, I.; Anwar, F.; Allanson, J.; Outtrim, J.; Menon, D.; Hutchinson, P.; Helmy, A. Spectrum of outcomes following traumatic brain injury-relationship between functional impairment and health-related quality of life. Acta Neurochir. 2018, 160, 107–115. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.L.; Dikmen, S.S.; Langlois, J.A.; Selassie, A.W.; Gu, J.K.; Horner, M.D. Self-reported psychosocial health among adults with traumatic brain injury. Arch. Phys. Med. Rehabil. 2006, 87, 953–961. [Google Scholar] [CrossRef]
- Voormolen, D.C.; Polinder, S.; von Steinbuechel, N.; Vos, P.E.; Cnossen, M.C.; Haagsma, J.A. The association between post-concussion symptoms and health-related quality of life in patients with mild traumatic brain injury. Injury 2019, 50, 1068–1074. [Google Scholar] [CrossRef]
- Hu, X.B.; Feng, Z.; Fan, Y.C.; Xiong, Z.Y.; Huang, Q.W. Health-related quality-of-life after traumatic brain injury: A 2-year follow-up study in Wuhan, China. Brain Inj. 2012, 26, 183–187. [Google Scholar] [CrossRef]
- Scholten, A.C.; Haagsma, J.A.; Andriessen, T.M.; Vos, P.E.; Steyerberg, E.W.; van Beeck, E.F.; Polinder, S. Health-related quality of life after mild, moderate and severe traumatic brain injury: Patterns and predictors of suboptimal functioning during the first year after injury. Injury 2015, 46, 616–624. [Google Scholar] [CrossRef]
- Kwok, O.M.; Underhill, A.T.; Berry, J.W.; Luo, W.; Elliott, T.R.; Yoon, M. Analyzing Longitudinal Data with Multilevel Models: An Example with Individuals Living with Lower Extremity Intra-articular Fractures. Rehabil. Psychol. 2008, 53, 370–386. [Google Scholar] [CrossRef]
- Andelic, N.; Sigurdardottir, S.; Schanke, A.K.; Sandvik, L.; Sveen, U.; Roe, C. Disability, physical health and mental health 1 year after traumatic brain injury. Disabil. Rehabil. 2010, 32, 1122–1131. [Google Scholar] [CrossRef]
- Andelic, N.; Perrin, P.B.; Forslund, M.V.; Soberg, H.L.; Sigurdardottir, S.; Sveen, U.; Jerstad, T.; Roe, C. Trajectories of physical health in the first 5 years after traumatic brain injury. J. Neurol. 2015, 262, 523–531. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Hopman, W.M.; Berger, C.; Joseph, L.; Towheed, T.; VandenKerkhof, E.; Anastassiades, T.; Adachi, J.D.; Ioannidis, G.; Brown, J.P.; Hanley, D.A.; et al. The natural progression of health-related quality of life: Results of a five-year prospective study of SF-36 scores in a normative population. Qual. Life Res. 2006, 15, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Snow, K.K.; Kosinski, M.; Gandek, B. SF-36 Health Survey: Manual and Interpretation Guide; New England Medical Center Hospital: Boston, MA, USA, 1993. [Google Scholar]
- Wang, H.M.; Beyer, M.; Gensichen, J.; Gerlach, F.M. Health-related quality of life among general practice patients with differing chronic diseases in Germany: Cross sectional survey. BMC Public Health 2008, 8, 246. [Google Scholar] [CrossRef] [PubMed]
- Marshall, L.F.; Marshall, S.B.; Klauber, M.R.; Van Berkum, C.M.; Eisenberg, H.; Jane, J.A.; Luerssen, T.G.; Marmarou, A.; Foulkes, M.A. The diagnosis of head injury requires a classification based on computed axial tomography. J. Neurotrauma 1992, 9 (Suppl. 1), S287–S292. [Google Scholar]
- Baker, S.P.; O’Neill, B.; Haddon, W., Jr.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Garratt, A.M.; Stavem, K. Measurement properties and normative data for the Norwegian SF-36: Results from a general population survey. Health Qual. Life Outcomes 2017, 15, 51. [Google Scholar] [CrossRef] [PubMed]
- Andelic, N.; Sigurdardottir, S.; Tenovuo, O. Rehabilitation after severe TBI. In Management of Severe Traumatic Brain Injury; Sundstrøm, T., Grände, P.O., Luoto, T., Rosenlund, C., Undén, J., Wester, K., Eds.; Springer: Cham, Switzerland, 2020; pp. 547–556. [Google Scholar]
- Tenovuo, O.; Andelic, N.; Sigurdardottir, S. Long-term follow-up. In Management of Severe Traumatic Brain Injury; Sundstrøm, T., Grände, P.O., Luoto, T., Rosenlund, C., Undén, J., Wester, K., Eds.; Springer: Cham, Switzerland, 2020; pp. 557–561. [Google Scholar]
- Cantor, J.B.; Ashman, T.; Gordon, W.; Ginsberg, A.; Engmann, C.; Egan, M.; Spielman, L.; Dijkers, M.; Flanagan, S. Fatigue after traumatic brain injury and its impact on participation and quality of life. J. Head Trauma Rehabil. 2008, 23, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, G.; Gruen, R.L.; Kaye, A.H. Traumatic brain injury and long-term quality of life: Findings from an Australian study. J. Neurotrauma 2009, 26, 1623–1633. [Google Scholar] [CrossRef] [PubMed]
- Lippert-Gruner, M.; Maegele, M.; Haverkamp, H.; Klug, N.; Wedekind, C. Health-related quality of life during the first year after severe brain trauma with and without polytrauma. Brain Inj. 2007, 21, 451–455. [Google Scholar] [CrossRef]
- Soberg, H.L.; Bautz-Holter, E.; Finset, A.; Roise, O.; Andelic, N. Physical and mental health 10 years after multiple trauma: A prospective cohort study. J. Trauma Acute Care Surg. 2015, 78, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Harfmann, E.J.; deRoon-Cassini, T.A.; McCrea, M.A.; Nader, A.M.; Nelson, L.D. Comparison of Four Quality of Life Inventories for Patients with Traumatic Brain Injuries and Orthopedic Injuries. J. Neurotrauma 2020, 37, 1408–1417. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) | Total n |
|---|---|---|
| Age at injury | 97 | |
| Mean (SD) | 30.3 (10.8) | |
| Gender | 97 | |
| Male | 76 (78.4) | |
| Female | 21 (21.6) | |
| Relationship status | 97 | |
| Partnered | 28 (28.9) | |
| Single | 69 (71.1) | |
| Education level | 96 | |
| ≤12 years | 54 (56.3) | |
| >12 years | 42 (43.8) | |
| Employment status | 97 | |
| Employed | 80 (82.5) | |
| Unemployed | 17 (17.5) | |
| Occupation type | 97 | |
| Blue collar | 46 (47.4) | |
| White collar | 51 (52.6) | |
| Injury cause | 97 | |
| Traffic accident | 58 (59.8) | |
| Fall | 23 (23.7) | |
| Violence/other | 16 (16.5) | |
| Glasgow Coma Scale score | 97 | |
| Mean (SD) | 7.2 (3.2) | |
| Moderate (9–12) | 32 (33.0) | |
| Severe (3–8) | 65 (67.0) | |
| Post-traumatic amnesia duration | 91 | |
| Days, Mean (SD) | 26.0 (30.0) | |
| CT Head Marshall Score | 97 | |
| Score I | 15 (15.5) | |
| Score II | 34 (35.1) | |
| Score III | 38 (39.2) | |
| Score IV | 1 (1.0) | |
| Score V | 9 (9.3) | |
| Score VI | 0 (0.0) | |
| Injury Severity Score | 97 | |
| <16 | 15 (15.5) | |
| ≥16 | 82 (84.5) |
| Model | −2 Log Likelihood |
|---|---|
| PCS | |
| Unconditional Growth Model | 2380.28 |
| Quadratic | 2378.31 |
| Cubic | 2378.08 |
| MCS | |
| Unconditional Growth Model | 2513.52 |
| Quadratic | 2513.07 |
| Cubic | 2513.01 |
| Predictor | b-Weight | SE | p-Value | 95% CI | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Intercept | 39.03 | 2.26 | 0.000 ** | 34.53 | 43.52 |
| Time | 0.65 | 0.11 | 0.000 ** | 0.44 | 0.86 |
| Gender (1 = woman, 0 = man) | −7.22 | 1.87 | 0.000 ** | −1.94 | −3.50 |
| Age | −0.12 | 0.09 | 0.194 | −0.29 | 0.06 |
| Relationship Status (1 = partnered, 0 = single) | −1.55 | 2.03 | 0.448 | −5.59 | 2.49 |
| Education | 0.67 | 1.03 | 0.518 | −1.38 | 2.71 |
| Employment (1 = employed, 0 = unemployed) | 4.98 | 2.04 | 0.016 * | 0.94 | 9.02 |
| Occupational Status (1 = white collar, 0 = blue collar) | 3.48 | 1.77 | 0.052 | −0.03 | 6.99 |
| Glasgow Coma Scale Score | 0.03 | 0.28 | 0.926 | −0.54 | 0.59 |
| Cause of Injury (1 = motor vehicle, 0 = not motor vehicle) | −1.10 | 1.76 | 0.532 | −4.60 | 2.39 |
| Post-Traumatic Amnesia | −0.07 | 0.03 | 0.031 * | −0.13 | −0.01 |
| CT Severity Score | 1.20 | 0.77 | 0.121 | −0.32 | 2.72 |
| Injury Severity Score | 0.07 | 0.06 | 0.293 | −0.06 | 0.19 |
| Predictor | b-Weight | SE | p-Value | 95% CI | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Intercept | 33.35 | 2.69 | 0.000 ** | 28.01 | 38.68 |
| Time | 0.37 | 0.14 | 0.006 * | 0.11 | 0.64 |
| Gender (1 = woman, 0 = man) | −7.60 | 2.21 | 0.001 * | −12.00 | −3.20 |
| Age | −0.13 | 0.11 | 0.230 | −0.34 | 0.08 |
| Relationship Status (1 = partnered, 0 = single) | 3.42 | 2.41 | 0.159 | −1.36 | 8.21 |
| Education | −1.69 | 1.22 | 0.168 | −4.12 | 0.73 |
| Employment (1 = employed, 0 = unemployed) | 11.10 | 2.41 | 0.000 ** | 6.30 | 15.90 |
| Occupational Status (1 = white collar, 0 = blue collar) | 3.36 | 2.09 | 0.112 | −0.80 | 7.51 |
| Glasgow Coma Scale Score | 0.08 | 0.34 | 0.819 | −0.59 | 0.74 |
| Cause of Injury (1 = motor vehicle, 0 = not motor vehicle) | −0.83 | 2.08 | 0.692 | −4.97 | 3.31 |
| Post-Traumatic Amnesia | 0.02 | 0.04 | 0.652 | −0.05 | 0.09 |
| CT Severity Score | −0.33 | 0.91 | 0.721 | −2.13 | 1.48 |
| Injury Severity Score | 0.15 | 0.08 | 0.051 | 0.00 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forslund, M.V.; Perrin, P.B.; Sigurdardottir, S.; Howe, E.I.; van Walsem, M.R.; Arango-Lasprilla, J.C.; Lu, J.; Aza, A.; Jerstad, T.; Røe, C.; et al. Health-Related Quality of Life Trajectories across 10 Years after Moderate to Severe Traumatic Brain Injury in Norway. J. Clin. Med. 2021, 10, 157. https://doi.org/10.3390/jcm10010157
Forslund MV, Perrin PB, Sigurdardottir S, Howe EI, van Walsem MR, Arango-Lasprilla JC, Lu J, Aza A, Jerstad T, Røe C, et al. Health-Related Quality of Life Trajectories across 10 Years after Moderate to Severe Traumatic Brain Injury in Norway. Journal of Clinical Medicine. 2021; 10(1):157. https://doi.org/10.3390/jcm10010157
Chicago/Turabian StyleForslund, Marit V., Paul B. Perrin, Solrun Sigurdardottir, Emilie I. Howe, Marleen R. van Walsem, Juan Carlos Arango-Lasprilla, Juan Lu, Alba Aza, Tone Jerstad, Cecilie Røe, and et al. 2021. "Health-Related Quality of Life Trajectories across 10 Years after Moderate to Severe Traumatic Brain Injury in Norway" Journal of Clinical Medicine 10, no. 1: 157. https://doi.org/10.3390/jcm10010157
APA StyleForslund, M. V., Perrin, P. B., Sigurdardottir, S., Howe, E. I., van Walsem, M. R., Arango-Lasprilla, J. C., Lu, J., Aza, A., Jerstad, T., Røe, C., & Andelic, N. (2021). Health-Related Quality of Life Trajectories across 10 Years after Moderate to Severe Traumatic Brain Injury in Norway. Journal of Clinical Medicine, 10(1), 157. https://doi.org/10.3390/jcm10010157