Emergency Management of Pelvic Bleeding


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
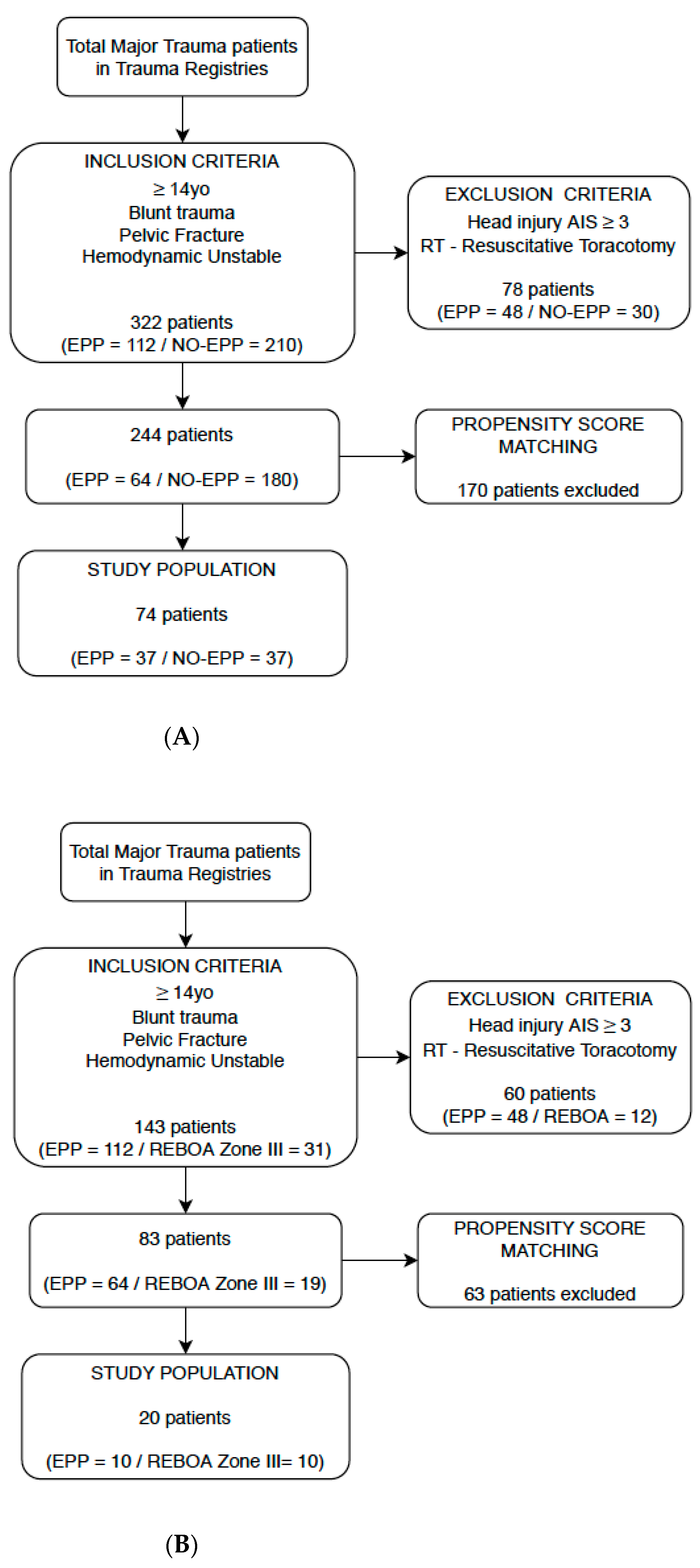
2.2. Study Population
2.3. Treatment Protocol
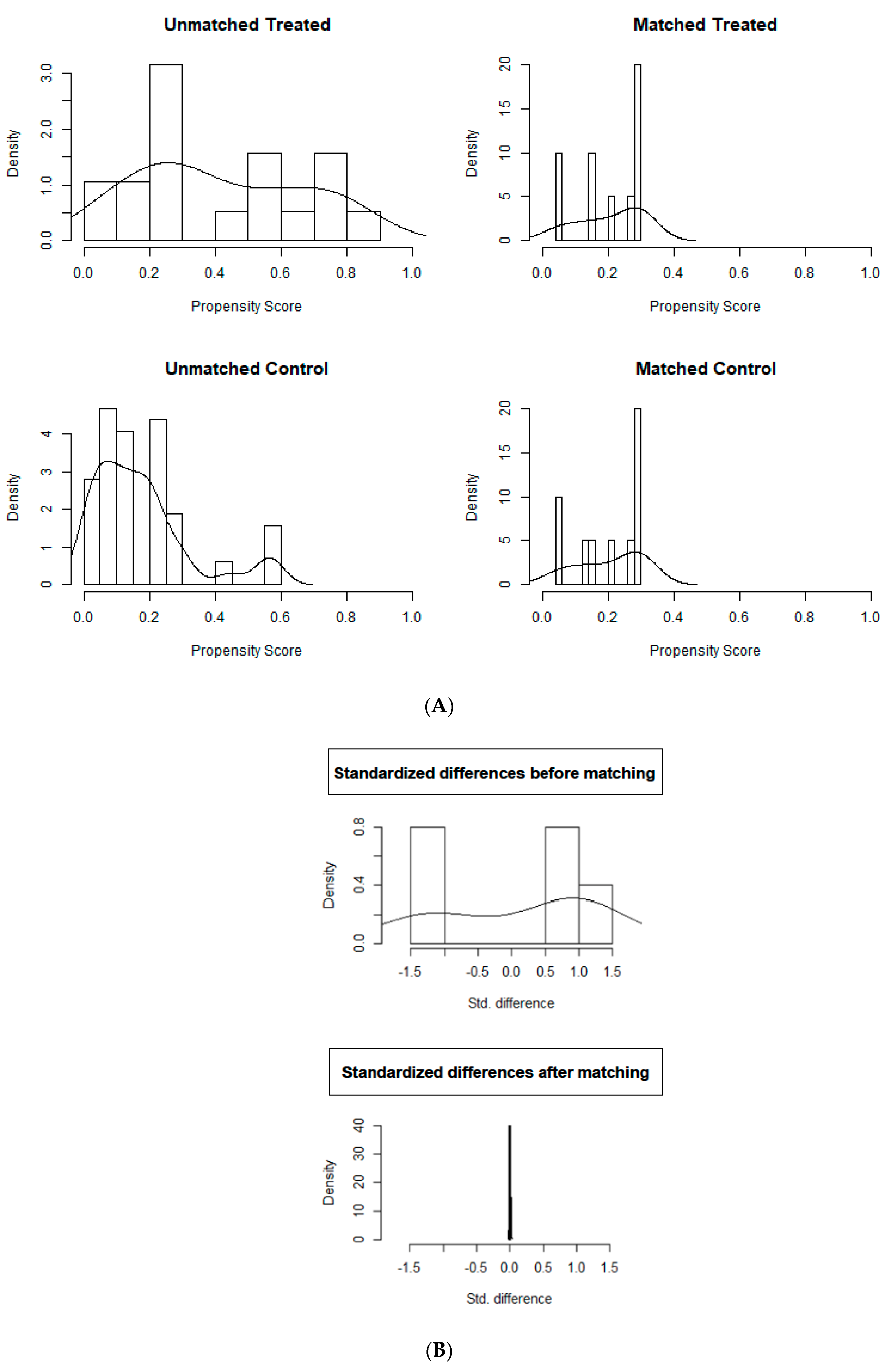
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Reporting Checklist
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coccolini, F.; Stahel, P.F.; Montori, G.; Biffl, W.; Hörer, T.; Catena, F.; Kluger, Y.; Moore, E.E.; Peitzman, A.B.; Ivatury, R.R.; et al. Pelvic trauma: WSES classification and guidelines. World J. Emerg. Surg. 2017, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Cullinane, D.C.; Schiller, H.J.; Zielinski, M.D.; Bilaniuk, J.W.; Collier, B.R.; Como, J.; Holevar, M.; Sabater, E.A.; Andrew Sems, S.; Matthew Vassy, W.; et al. Eastern Association for the Surgery of Trauma practice management guidelines for hemorrhage in pelvic fracture—update and systematic review. J. Trauma Acute Care Surg. 2011, 71, 1850–1868. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.L.; Brasel, K.J.; Karmy-Jones, R.; Rowell, S.; Schreiber, M.A.; Shatz, D.V.; Albrecht, R.M.; Cohen, M.J.; DeMoya, M.A.; Biffl, W.L.; et al. Western Trauma Association critical decision in trauma: Management of pelvic fracture with hemodynamic instability—2016 updates. J. Trauma Acute Care Surg. 2016, 81, 1171–1174. [Google Scholar] [CrossRef] [PubMed]
- Costantini, T.W.; Coimbra, R.; Holcomb, J.B.; Podbielski, J.M.; Catalano, R.D.; Blackburn, A.; Scalea, T.M.; Stein, D.M.; Williams, L.; Conflitti, J.; et al. Pelvic fracture pattern predicts the need for hemorrhage control intervention—results of an AAST multi-institutional study. J. Trauma Acute Care Surg. 2017, 82, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Tosounidis, T.I.; Giannoudis, P.V. Pelvic fractures presenting with hemodynamic instability: Treatment options and outcomes. Surgeon 2013, 11, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Croce, M.A.; Magnotti, L.J.; Savage, S.; Wood, G.W.; Fabian, T.C. Emergent Pelvic Fixation in Patient with Exsanguinating Pelvic Fractures. J. Am. Coll. Surg. 2007, 204, 935–939. [Google Scholar] [CrossRef] [PubMed]
- Scaglione, M.; Parchi, P.D.; DiGrandi, G.; Latessa, M.; Guido, G. External fixation in pelvic fractures. Musculoskelet. Surg. 2010, 94, 63–70. [Google Scholar] [CrossRef]
- Tesoriero, R.B.; Bruns, B.R. Angiographic embolization for hemorrhage following pelvic fracture: Is it “time” for a paradigm shift? J. Trauma Acute Care Surg. 2017, 82, 18–26. [Google Scholar] [CrossRef]
- Osborn, P.M.; Smith, W.R.; Moore, E.E.; Cothren, C.C.; Morgan, S.; Williams, N.A.E.; Stahel, P.F. Direct retroperitoneal pelvic packing versus pelvic angiography: A comparison of two management protocols for haemodynamically unstable pelvic fractures. Injury 2009, 40, 54–60. [Google Scholar] [CrossRef]
- Cothren, C.C.; Osborn, P.M.; Moore, E.E.; Morgan, S.J.; Johnson, J.L.; Smith, W.R. Preperitoneal pelvic packing for hemodynamically unstable pelvic fractures: A paradigm shift. J. Trauma Acute Care Surg. 2007, 62, 834–842. [Google Scholar] [CrossRef]
- Chiara, O.; Di Fratta, E.; Mariani, A.; Michaela, B.; Prestini, L.; Sammartano, F.; Cimbanassi, S. Efficacy of extra-peritoneal pelvic packing in hemodynamically unstable pelvic fractures, a propensity score analysis. World J. Emerg. Surg. 2016, 11, 22. [Google Scholar] [CrossRef] [PubMed]
- Burlew, C.C.; Moore, E.E.; Stahel, P.F.; Geddes, A.E.; Wagenaar, A.E.; Pieracci, F.M.; Fox, C.J.; Campion, E.M.; Johnson, J.L.; Mauffrey, C. Preperitoneal pelvic packing reduces mortality in patients with life-threatening hemorrhage due to unstable pelvic fractures. J. Trauma Acute Care Surg. 2017, 82, 233. [Google Scholar] [CrossRef] [PubMed]
- Brenner, M.; Teeter, W.; Hoehn, M.; Pasley, J.; Hu, P.; Yang, S.; Romagnoli, A.; Diaz, J.; Stein, D.; Scalea, T. Use of resuscitative endovascular balloon occlusion of the aorta for proximal aortic control in patients with severe hemorrhage and arrest. JAMA Surg. 2018, 153, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Morrison, J.J.; Percival, T.J.; Markov, N.P.; Villamaria, C.; Scott, D.J.; Saches, K.A.; Spencer, J.R.; Rasmussen, T.E. Aortic balloon occlusion is effective in controlling pelvic hemorrhage. J. Surg. Res. 2012, 177, 341–347. [Google Scholar] [CrossRef]
- Do, W.S.; Forte, D.M.; Sheldon, R.R.; Weiss, J.B.; Barron, M.R.; Sokol, K.K.; Black, G.E.; Hegge, S.R.; Eckert, M.J.; Martin, M.J. Preperitoneal balloon tamponade and resuscitative endovascular balloon occlusion of the aorta: Alternatives to open packing for pelvic-associated hemorrhage. J. Trauma Acute Care Surg. 2019, 87, 18–26. [Google Scholar] [CrossRef]
- DuBose, J.J.; Scalea, T.M.; Brenner, M.; Skiada, D.; Inaba, K.; Cannon, J.; Moore, L.; Holcomb, J.; Turay, D.; Arbabi, C.N. The AAST prospective Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry: Data on contemporary utilization and outcomes of aortic occlusion and resuscitative balloon occlusion of the aorta (REBOA). J. Trauma Acute Care Surg. 2016, 81, 409–419. [Google Scholar] [CrossRef]
- Frassini, S.S.; Gupta, S.S.; Granieri, S.S.; Cimbanassi, S.S.; Sammartano, F.F.; Scalea, T.M.; O Chiara, O. Extraperitoneal packing in unstable blunt pelvic trauma: A single-center study. J. Trauma Acute Care Surg. 2020, 88, 597–606. [Google Scholar] [CrossRef]
- Ramenofsky, M.; Bell, R. ATLS: Advanced Trauma Life Support, 10th ed.; Committee on Trauma: Chicago, IL, USA, 2018. [Google Scholar]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for casual effect. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Pearl, J. Understanding propensity scores. In Casuality: Models, Reasoning and Inference, 1st ed.; Cambridge University Press: Cambridge, UK, 2009; p. 348. [Google Scholar]
- Mikdad, S.; Inge van Erpe, A.M.; Moheb, M.E.; Fawley, J.; Saillant, N.; King, D.R.; Kaafarani, H.M.A.; Velmahos, G.; Mendoza, A.E. Pre-Peritoneal Pelvic Packing for Early Hemorrhage Control Reduces Mortality Compared to Resuscitative Endovascular Balloon Occlusion of the Aorta in Severe Blunt Pelvic Trauma Patients: A National-wide Analysis. Injury 2020. paper published ahead of print. [Google Scholar] [CrossRef]
- Reitano, E.; Granieri, S.; Frassini, S.; Sammartano, F.; Cimbanassi, S.; Chiara, O. Infectious complications of extra-peritoneal pelvic packing in emergency room. Updates Surg. 2020. [Google Scholar] [CrossRef]
- Biffl, W.L.; Fox, C.J.; Moore, E. The role of REBOA in the control of exsanguinating torso hemorrhage. J. Trauma Acute Care Surg. 2015, 78, 1054–1058. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, R.; Cestero, R.F.; Suzuki, M.; Funabiki, T.; Sasaki, J. Resuscitative endovascular balloon occlusion of the aorta (REBOA) is associated with improved survival in severely injured patients: A propensity score matching analysis. Am. J. Surg. 2019, 218, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Brenner, M.; Inaba, K.; Aiolfi, A.; DuBose, J.; Fabian, T.; Bee, T.; Holcomb, J.B.; Moore, L.; Skarupa, D.; Scalea, T.M. Resuscitative Endovascular Balloon Occlusion of the Aorta and Resuscitative Thoracotomy in select patients with hemorrhagic shock: Early results from the American Association for the Surgery of Trauma Aortic Occlusion in Resuscitation for Trauma and Acute Care Surgery Registry. J. Am. Coll. Surg. 2018, 226, 730–740. [Google Scholar] [PubMed]
- Madurska, M.; Ross, J.D.; Scalea, T.M.; Morrison, J.J. State-of-the-Art Review—Endovascular Resuscitation. Shock 2020. paper published ahead of print. [Google Scholar] [CrossRef] [PubMed]
- ISS. Linea Guida sulla Gestione Integrata del Trauma Maggiore Dalla Scena dell’evento alla Cura Definitive. 2020. Available online: https://snlg.iss.it (accessed on 1 January 2020).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statements: Guidelines for Reporting Observational Studies. PLOS Med. 2007, 4, 1623–1627. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | No-EPP (n = 37) | EPP (n = 37) | p | ||
|---|---|---|---|---|---|
| Number/Mean | %/SD | Number/Mean | %/SD | ||
| Gender (male) | 27 | 73 | 22 | 59.5 | 0.32 |
| Mechanism of Trauma | <0.001 * | ||||
| Road accident | 27 | 73 | 9 | 24.3 | |
| Fall | 9 | 24.3 | 15 | 40.6 | |
| Pedestrian | 0 | 0 | 9 | 24.3 | |
| Cyclist | 0 | 0 | 4 | 10.8 | |
| Domestic accident | 1 | 2.7 | 0 | 0 | |
| ICU-LOS (days) | 12 | 17.25 | 30.35 | 35.57 | 0.02 * |
| Length of hospitalization | 33.65 | 34.97 | 64 | 55.79 | 0.012 * |
| N. of angioembolizations | 21 | 56.8 | 21 | 56.8 | 1 |
| N. of external fixations | 21 | 56.8 | 27 | 73 | 0.22 |
| Time to hemostatic procedure (mins) ** | 155.9 | 95.11 | 49.43 | 24.97 | <0.001 * |
| SBP in Emergency Department | 82.95 | 27.9 | 65.73 | 17.79 | 0.004 * |
| HR in Emergency Department | 97.32 | 30.53 | 105.03 | 22.83 | 0.33 |
| N. of PRBCs < 24 h | 11.28 | 10.18 | 8.08 | 6.74 | 0.36 |
| RTS | 6.06 | 1.69 | 5.28 | 1.98 | 0.07 |
| Probability of death (TRISS) | 50.69 | 31.75 | 57.02 | 31.12 | 0.33 |
| Deaths ≤ 24 h | 15 | 40.54 | 7 | 18.92 | 0.042 * |
| Total deaths | 16 | 43.24 | 8 | 21.62 | 0.047 * |
| EPP | REBOA | p Value | OR (Odds Ratio) | CI (Confidence Interval) 95% | |||
|---|---|---|---|---|---|---|---|
| Survived | Dead | Survived | Dead | ||||
| OUTCOME 24 h | 8 80.00% | 2 20.00% | 6 60.00% | 4 40.00% | 0.337 | 2.66 | 0.361–19.712 |
| OUTCOME 7 days | 8 80.00% | 2 20.00% | 5 50.00% | 5 50.00% | 0.171 | 4.00 | 0.550–29.096 |
| OUTCOME OVERALL | 7 70.00% | 3 30.00% | 4 40.00% | 6 60.00% | 0.185 | 3.50 | 0.549–22.304 |
| n Patients | MAP PRE-Procedure (mmHg) | MAP POST-Procedure (mmHg) | Δ (mmHg) | p Value | |
|---|---|---|---|---|---|
| EPP-GROUP total | 64 | 49.92 ± 17.12 | 70.05 ± 25.07 | +20.13 | <0.001 |
| EPP-GROUP Survivied | 42/64 | 54.71 ± 22.30 | 79.40 ± 20.04 | +24.69 | <0.001 |
| EPP-GROUP Died | 22/64 | 40.41 ± 14.54 | 52.36 ± 14.88 | +11.95 | 0.06 |
| REBOA-GROUP Total | 19 | 45.42 ± 27.90 | 90.52 ± 39.54 | +45.10 | <0.001 |
| REBOA-GROUP Survived | 10/19 | 58.30 ± 12.32 | 94.70 ± 12.59 | +36.40 | <0.001 |
| REBOA-GROUP Died | 9/19 | 31.11 ± 33.82 | 85.88 ± 57.52 | +54.77 | 0.014 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frassini, S.; Gupta, S.; Granieri, S.; Cimbanassi, S.; Sammartano, F.; Scalea, T.M.; Chiara, O. Emergency Management of Pelvic Bleeding. J. Clin. Med. 2021, 10, 129. https://doi.org/10.3390/jcm10010129
Frassini S, Gupta S, Granieri S, Cimbanassi S, Sammartano F, Scalea TM, Chiara O. Emergency Management of Pelvic Bleeding. Journal of Clinical Medicine. 2021; 10(1):129. https://doi.org/10.3390/jcm10010129
Chicago/Turabian StyleFrassini, Simone, Shailvi Gupta, Stefano Granieri, Stefania Cimbanassi, Fabrizio Sammartano, Thomas M. Scalea, and Osvaldo Chiara. 2021. "Emergency Management of Pelvic Bleeding" Journal of Clinical Medicine 10, no. 1: 129. https://doi.org/10.3390/jcm10010129
APA StyleFrassini, S., Gupta, S., Granieri, S., Cimbanassi, S., Sammartano, F., Scalea, T. M., & Chiara, O. (2021). Emergency Management of Pelvic Bleeding. Journal of Clinical Medicine, 10(1), 129. https://doi.org/10.3390/jcm10010129