
COVID-19 Vaccine Acceptance in Azuay Province, Ecuador: A Cross-Sectional Online Survey

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
Data Processing and Analysis
3. Results
3.1. Participants’ Characteristics
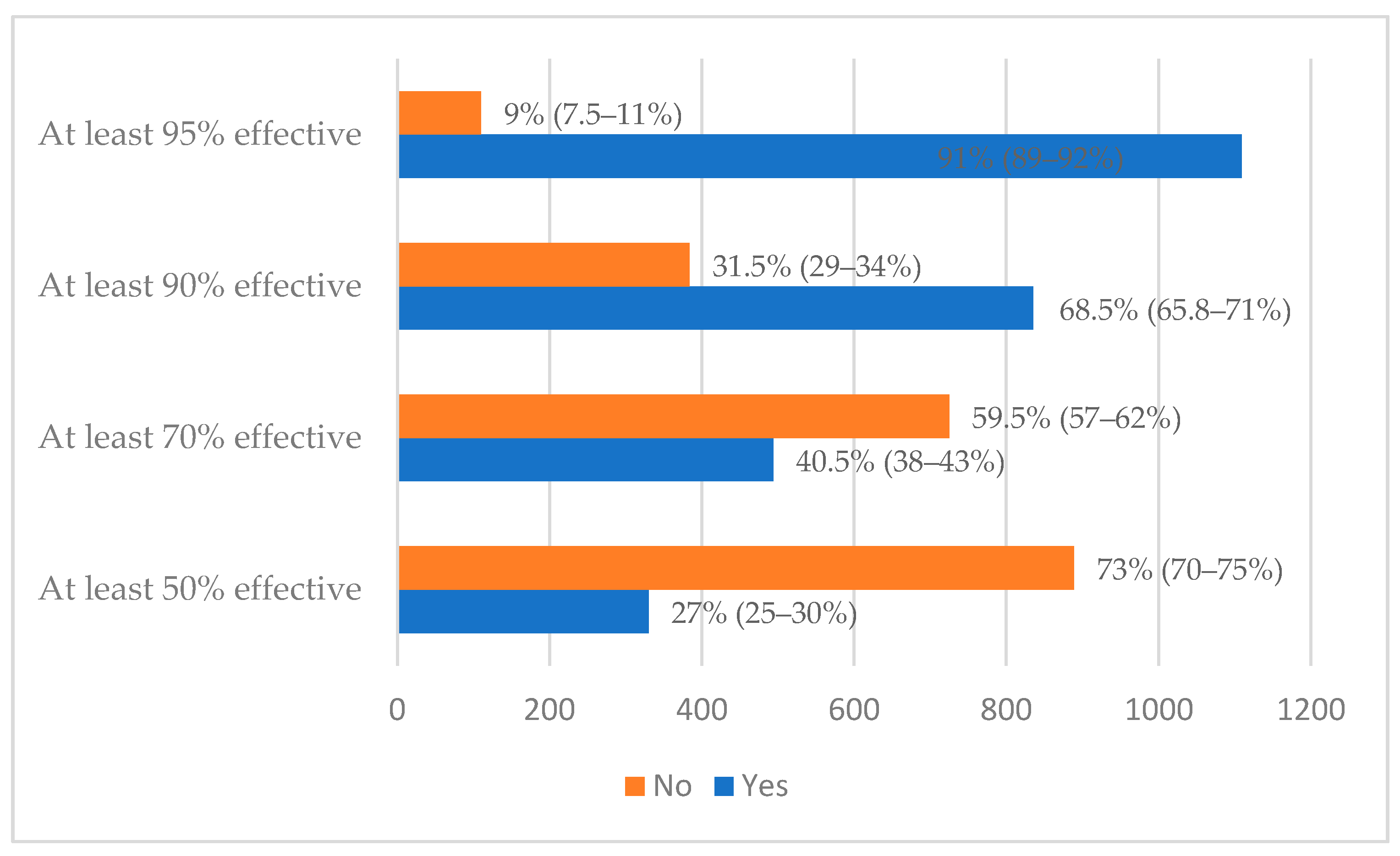
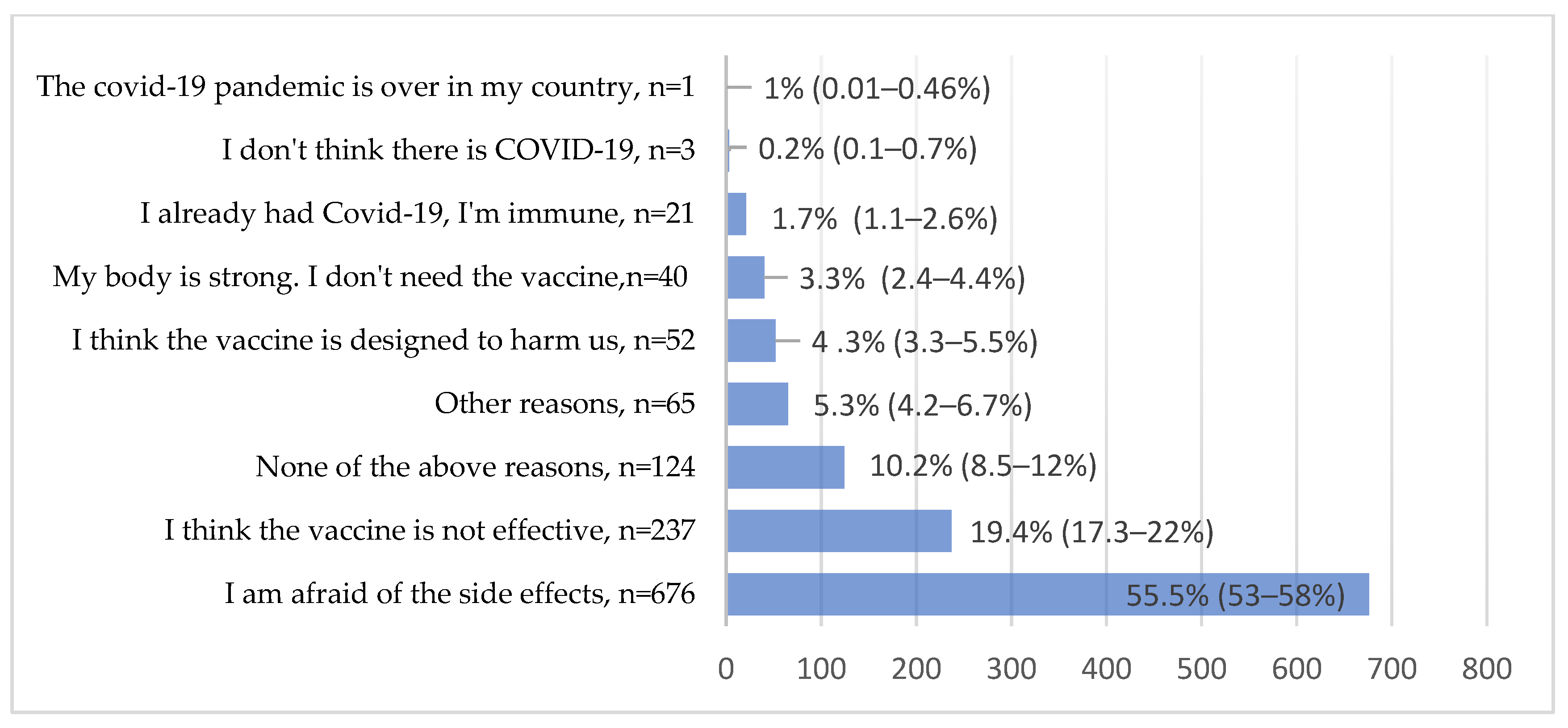
3.2. Vaccine Acceptance
3.3. Determinants of COVID-19 Vaccine Acceptance
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update on COVID-19. 20 April 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---20-april-2021 (accessed on 23 April 2021).
- Ministerio de Salud Pública del Ecuador. Situación nacional por COVID-19. [Report]. 2021 Updated 2020 April 9. Available online: https://www.gestionderiesgos.gob.ec/wp-content/uploads/2021/04/INFOGRAFIA-NACIONALCOVID19-COE-NACIONAL-08h00-09042021.pdf (accessed on 23 April 2021).
- World Health Organization. COVID-19 Strategy Update. 2021. Available online: https://www.who.int/publications/m/item/covid-19-strategy-update (accessed on 23 April 2021).
- Chen, W. Promise and challenges in the development of COVID-19 vaccines. Hum. Vaccines Immunother. 2020, 16, 2604–2608. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Tracker. 2021 Updated 2021 April 5. Available online: https://covid19.trackvaccines.org/vaccines/ (accessed on 23 April 2021).
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Holder, J.; Tracking Coronavirus Vaccinations around the World. The New York Times, 9 April 2020. Available online: https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html (accessed on 9 April 2021).
- Gavi. 2021 updated 2020 April 8. Available online: https://www.gavi.org/covax-facility (accessed on 23 April 2021).
- Ministerio de Salud Pública del Ecuador. Plan Vacunarse. [Website]. 2021. Available online: https://www.planvacunarse.ec/#vacunas-contratadas (accessed on 23 April 2021).
- Ministerio de Salud Pública del Ecuador. Vacunados COVID-19. 2021 updated 2020 April 8. Available online: https://www.salud.gob.ec/vacunados-covid-19/ (accessed on 23 April 2021).
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key Guidelines in Developing a Pre-Emptive COVID-19 Vaccination Uptake Promotion Strategy. Int. J. Environ. Res. Public Health 2020, 17, 5893. [Google Scholar] [CrossRef] [PubMed]
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pan-demic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- Sarasty, O.; Carpio, C.E.; Hudson, D.; Guerrero-Ochoa, P.A.; Borja, I. The demand for a COVID-19 vaccine in Ecuador. Vaccine 2020, 38, 8090–8098. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Leng, A.; Maitland, E.; Wang, S.; Nicholas, S.; Liu, R.; Wang, J. Individual preferences for COVID-19 vaccination in China. Vaccine 2021, 39, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Xu, R.H.; Wong, E.L.; Hung, C.; Feng, D.; Feng, Z.; Yeoh, E.; Wong, S.Y. Public preference for COVID-19 vaccines in China: A discrete choice experiment. Health Expect. 2020, 23, 1543–1578. [Google Scholar] [CrossRef] [PubMed]
- Mannan, D.K.A.; Farhana, K.M. Knowledge, Attitude and Acceptance of a COVID-19 Vaccine: A Global Cross-Sectional Study. Int. Res. J. Bus. Soc. Sci. 2020, 6, 23. [Google Scholar]
- Kaplan, R.M.; Milstein, A. Influence of a COVID-19 vaccine’s effectiveness and safety profile on vaccination acceptance. Proc. Natl. Acad. Sci. USA 2021, 118, 2021726118. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated With US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef]
- Matos, C.C.d.S.A.; Gonçalves, B.A.; Couto, M.T. Vaccine hesitancy in the global south: Towards a critical perspective on global health. Glob. Public Health 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Guzman-Holst, A.; DeAntonio, R.; Prado-Cohrs, D.; Juliao, P. Barriers to vaccination in Latin America: A systematic literature review. Vaccine 2020, 38, 470–481. [Google Scholar] [CrossRef]
- Megget, K. Even covid-19 can’t kill the anti-vaccination movement. BMJ 2020, 369, m2184. [Google Scholar] [CrossRef]
- Bono, S.; Villela, E.F.D.M.; Siau, C.; Chen, W.; Pengpid, S.; Hasan, M.; Sessou, P.; Ditekemena, J.; Amodan, B.; Hosseinipour, M.; et al. Factors Affecting COVID-19 Vaccine Acceptance: An International Survey among Low- and Middle-Income Countries. Vaccines 2021, 9, 515. [Google Scholar] [CrossRef]
- Dubov, A.; Phung, C. Nudges or mandates? The ethics of mandatory flu vaccination. Vaccine 2015, 33, 2530–2535. [Google Scholar] [CrossRef]
- Betsch, C.; Renkewitz, F.; Betsch, T.; Ulshöfer, C. The Influence of Vaccine-critical Websites on Perceiving Vaccination Risks. J. Health Psychol. 2010, 15, 446–455. [Google Scholar] [CrossRef]
- Thomson, A.; Robinson, K.; Vallée-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joint CDC and FDA Statement on Johnson & Johnson COVID-19 Vaccine [press release]. 2021. Available online: https://stacks.cdc.gov/view/cdc/105057 (accessed on 9 April 2021).
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Salazar, P.; Link, N.; Lamarca, K.; Santillana, M. High coverage COVID-19 mRNA vaccination rapidly controls SARS-CoV-2 transmission in Long-Term Care Facilities. Res Sq. 2021. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Response | Place of Residence | ||
|---|---|---|---|---|
| Rural | Suburban | Urban | ||
| Sex | Male, n (%) | 84 (40.6%) | 85 (53.8%) | 357 (41.8%) |
| Female, n (%) | 123 (59.4%) | 73 (46.2%) | 497 (58.2%) | |
| Age | Mean (SD) | 26.68 (10.04) | 27.8 (10.6) | 33.5 (13.3) |
| Education | Secondary, n (%) | 73 (35.3%) | 53 (33.5%) | 174 (20.4%) |
| Undergraduate degree, n (%) | 106 (51.2%) | 67 (42.4%) | 376 (44%) | |
| Postgraduate degree, n (%) | 28 (13.5%) | 38 (24.1%) | 304 (35.6%) | |
| Current socio-economic situation | Lower income, n (%) | 51 (24.6%) | 22 (13.9%) | 101 (11.8%) |
| Lower middle income, n (%) | 128 (61.8%) | 93 (58.9%) | 434 (50.8%) | |
| Upper middle income, n (%) | 27 (13%) | 43 (27.2%) | 310 (36.3%) | |
| Higher income, n (%) | 1 (0.5%) | 0 (0%) | 9 (1.1%) | |
| Student or worker in the healthcare sector | No, n (%) | 120 (58%) | 105 (66.5%) | 520 (60.9%) |
| Yes, n (%) | 87 (42%) | 53 (33.5%) | 334 (39.1%) | |
| Source of information | Family, n (%) | 3 (1.4%) | 6 (3.8%) | 18 (2.1%) |
| Health workers, n (%) | 122 (58.9%) | 87 (55.1%) | 556 (65.1%) | |
| None, n (%) | 16 (7.7%) | 10 (6.3%) | 55 (6.4%) | |
| Radio/TV, n (%) | 26 (12.6%) | 20 (12.7%) | 88 (10.3%) | |
| Social media, n (%) | 27 (13%) | 20 (12.7%) | 72 (8.4%) | |
| Other, n (%) | 13 (6.3%) | 15 (9.5%) | 65 (7.6%) | |
| Presence of underlying disease | No, n (%) | 183 (88.4%) | 145 (91.8%) | 730 (85.5%) |
| Yes, n (%) | 24 (11.6%) | 13 (8.2%) | 124 (14.5%) | |
| Have you been tested for COVID-19? | Negative result | 77 (37.2%) | 66 (41.8%) | 398 (46.6%) |
| Positive result | 17 (8.2%) | 16 (10.1%) | 96 (11.2%) | |
| Not tested | 113 (54.6%) | 76 (48.1%) | 360 (42.2%) | |
| How worried/fearful are you about getting infected or re-infected by the coronavirus? | Not at all concerned, n (%) | 12 (5.8%) | 11 (7.0%) | 62 (7.3%) |
| A little worried, n (%) | 36 (17.4%) | 24 (15.2%) | 122 (14.3%) | |
| Moderately worried, n (%) | 81 (39.1%) | 47 (29.7%) | 295 (34.5%) | |
| Very worried, n (%) | 48 (23.2%) | 53 (33.5%) | 240 (28.1%) | |
| Extremely worried, n (%) | 30 (14.5%) | 23 (14.6%) | 135 (15.8%) | |
| Opinions about COVID-19 vaccines | ||||
| In your opinion, can COVID-19 infection be prevented with a vaccine? | ||||
| No, n (%) | 87 (42%) | 47 (29.8%) | 249 (29.1%) | |
| Yes, n (%) | 120 (58%) | 111 (70.3%) | 605 (70.8%) | |
| In your understanding, is there currently an effective vaccine against COVID-19? | ||||
| No, n (%) | 110 (53.1%) | 67 (42.5%) | 348 (40.7%) | |
| Yes, n (%) | 97 (46.9%) | 91 (57.6%) | 506 (59.3%) | |
| Can someone be re-infected with coronavirus after recovering from a previous COVID-19 infection? | ||||
| No, n (%) | 30 (14.5%) | 19 (12%) | 99 (11.6%) | |
| Yes, n (%) | 177 (85.5%) | 139 (88%) | 755 (88.4%) | |
| Covariates | Crude OR(95% CI) | Adjusted OR (95% CI) Full Model | p-Value |
|---|---|---|---|
| Age | 1.05 (1.04–1.07) | 1.04 (1.03–1.06) | <0.001 |
| Gender | |||
| Male | Ref | Ref | |
| Female | 0.85 (0.67–1.08) | 0.88 (0.67–1.15) | 0.345 |
| Education | |||
| Secondary | Ref | Ref | |
| Undergraduate | 1.62 (1.22–2.16) | 1.34 (0.98–1.82) | 0.067 |
| Postgraduate | 4.42 (3.13–6.25) | 1.85 (1.17–2.93) | 0.008 |
| Student healthcare worker | |||
| No | Ref | Ref | |
| Yes | 1.19 (0.94–1.52) | 1.22 (0.93–1.59) | 0.151 |
| Status of infection | |||
| Negative | Ref | Ref | |
| Positive | 1.80 (1.15–2.81) | 2.13 (1.32–3.44) | 0.001 |
| Results not known | 0.88 (0.69–1.13) | 1.23 (0.93–1.62) | 0.151 |
| Level of worry about status | |||
| Not worried | Ref | Ref | |
| A little worried | 1.98 (1.17–3.33) | 1.92 (1.08–3.40) | 0.025 |
| Moderately concerned | 1.69 (1.06–2.70) | 1.58 (0.94–2.64) | 0.081 |
| Very worried | 3.15 (1.93–5.13) | 3.02 (1.77–5.17) | <0.001 |
| Extremely worried | 3.26 (1.91–5.56) | 3.40 (1.89–6.10) | <0.001 |
| Presence of underlying disease | |||
| No | Ref | Ref | |
| Yes | 1.25 (0.87–1.78) | 0.71 (0.48–1.06) | 0.093 |
| Can COVID-19 infection be prevented with a vaccine? | |||
| No | |||
| Yes | Ref | Ref | |
| 2.31 (1.80–2.97) | 1.80 (1.33–2.44) | <0.001 | |
| In your understanding, is there currently an effective vaccine against COVID-19? | |||
| No | Ref | ||
| Yes | Ref | 1.34 (1.12–1.79) | |
| 2.03 (1.60–2.57) | 0.047 | ||
| Area of residency | |||
| Rural | Ref | Ref | |
| Suburban | 1.08 (0.71–1.64) | 0.87 (0.55–1.36) | 0.529 |
| Urban | 1.76 (1.29–2.40) | 1.16 (0.83–1.63) | 0.379 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaramillo-Monge, J.; Obimpeh, M.; Vega, B.; Acurio, D.; Boven, A.; Verhoeven, V.; Colebunders, R. COVID-19 Vaccine Acceptance in Azuay Province, Ecuador: A Cross-Sectional Online Survey. Vaccines 2021, 9, 678. https://doi.org/10.3390/vaccines9060678
Jaramillo-Monge J, Obimpeh M, Vega B, Acurio D, Boven A, Verhoeven V, Colebunders R. COVID-19 Vaccine Acceptance in Azuay Province, Ecuador: A Cross-Sectional Online Survey. Vaccines. 2021; 9(6):678. https://doi.org/10.3390/vaccines9060678
Chicago/Turabian StyleJaramillo-Monge, Julio, Michael Obimpeh, Bernardo Vega, David Acurio, Annelies Boven, Veronique Verhoeven, and Robert Colebunders. 2021. "COVID-19 Vaccine Acceptance in Azuay Province, Ecuador: A Cross-Sectional Online Survey" Vaccines 9, no. 6: 678. https://doi.org/10.3390/vaccines9060678
APA StyleJaramillo-Monge, J., Obimpeh, M., Vega, B., Acurio, D., Boven, A., Verhoeven, V., & Colebunders, R. (2021). COVID-19 Vaccine Acceptance in Azuay Province, Ecuador: A Cross-Sectional Online Survey. Vaccines, 9(6), 678. https://doi.org/10.3390/vaccines9060678