Influence of Prior Influenza Vaccination on Current Influenza Vaccine Effectiveness in Children Aged 1 to 5 Years

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Information Collection
2.3. Laboratory Testing
2.4. Statistical Analyses
3. Result
3.1. Characteristics of the Cases and Controls in This Study
3.2. Clinical Symptoms of the Cases and Controls in This Study
3.3. Current Season VE against Any Influenza
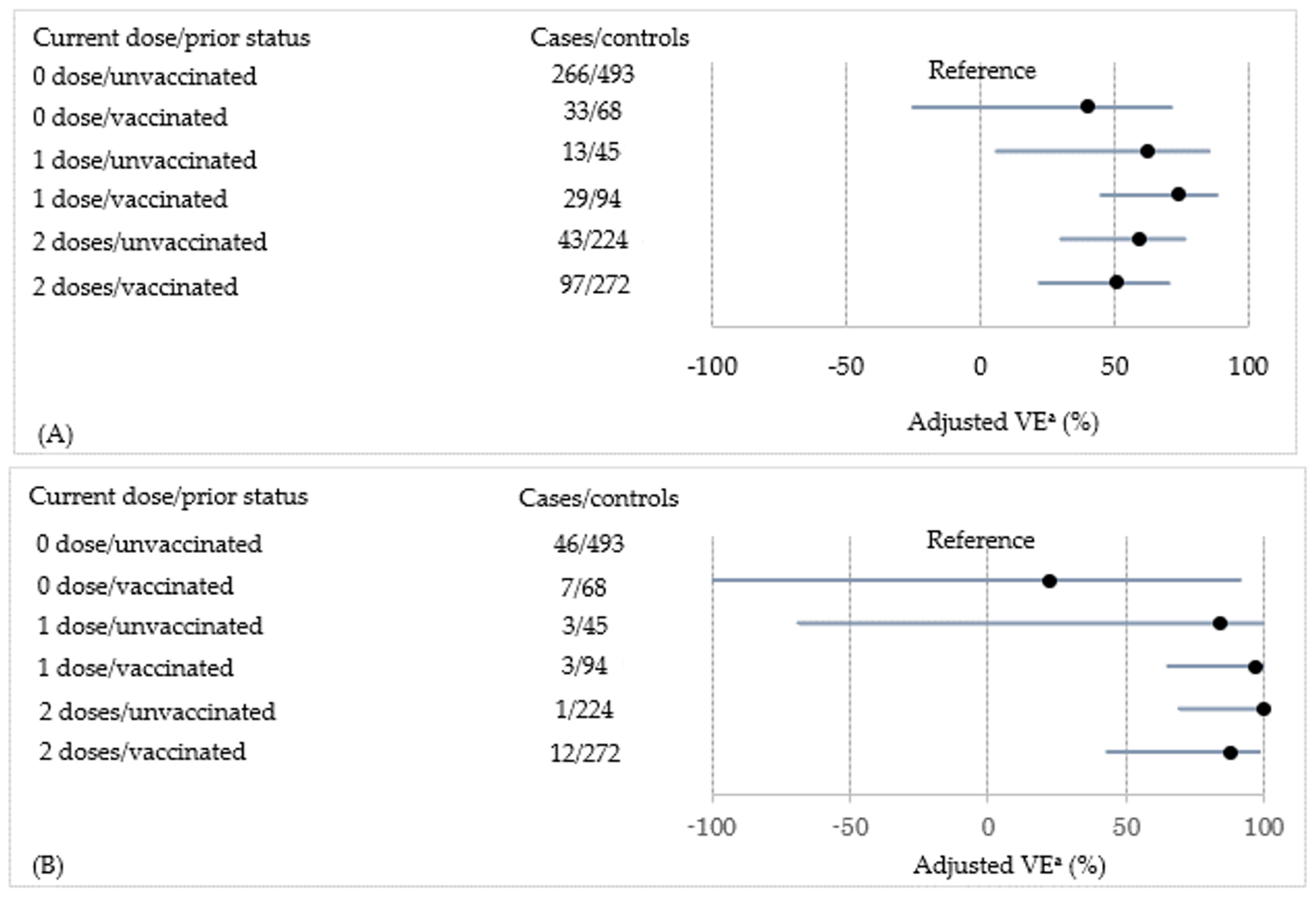
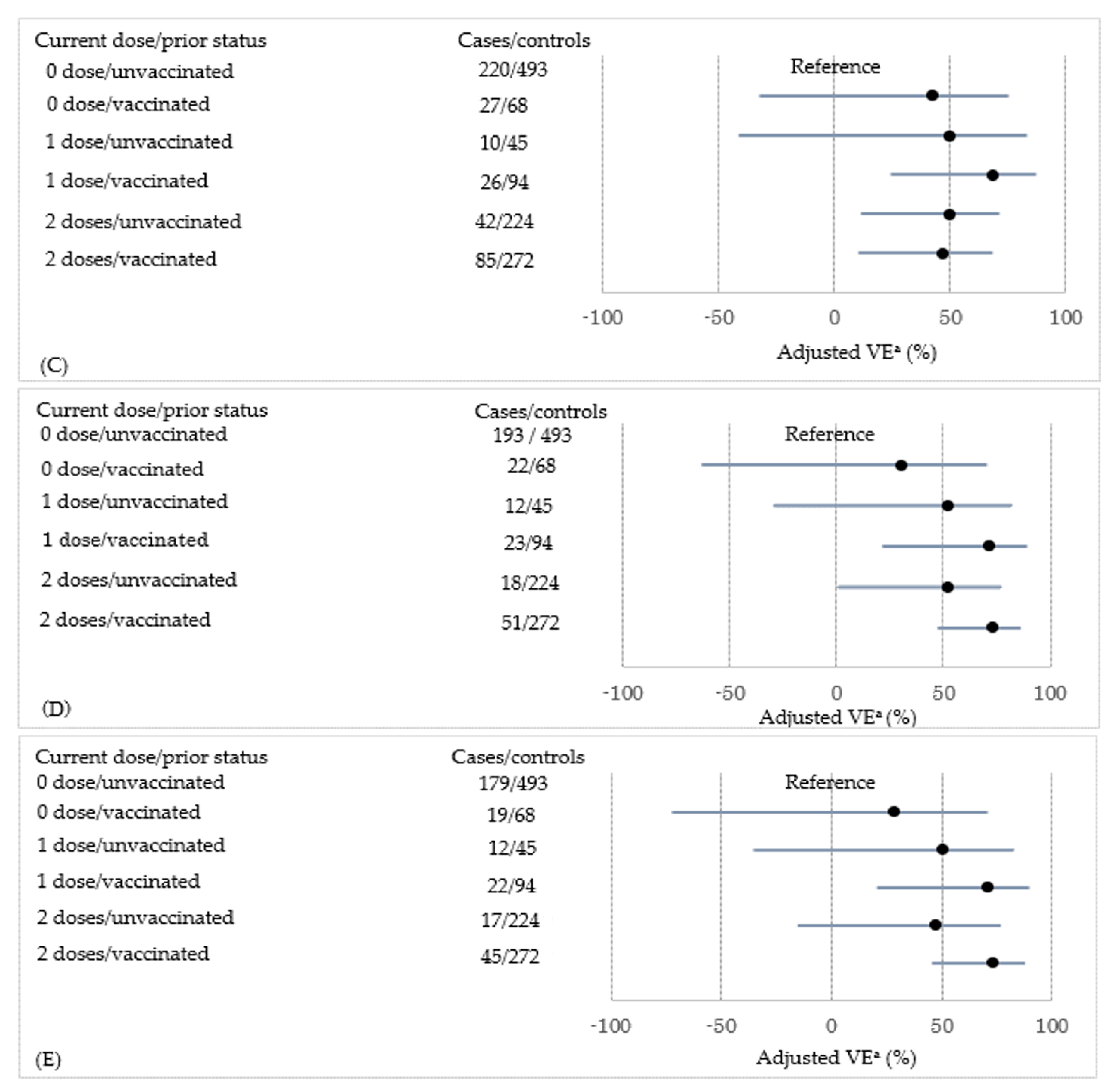
3.4. VE against Any Influenza According to the Current Vaccination Dose and Prior Vaccination Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Vaccines against influenza WHO position paper—November 2012. Wkly. Epidemiol. Rec. 2012, 87, 461–476. [Google Scholar]
- Hokins, T.W.; Davies, J.R.; Smith, A.J.; Allchin, A.; Miller, C.L. Assessment of inactivated influenza-A vaccine after three outbreak of influenza A at Christ’s Hospital. Lancet 1979, 313, 33–35. [Google Scholar] [CrossRef]
- Keitel, W.A.; Cate, T.R.; Couch, R.B.; Huggins, L.L.; Hess, K.R. Efficacy of repeated annual immunization with inactivated influenza virus vaccines over a five year period. Vaccine 1997, 15, 1114–1122. [Google Scholar] [CrossRef]
- Beyer, W.E.; de Bruijin, I.A.; Palache, A.M.; Westendrop, R.G.; Osterhaus, A.D. Protection against influenza after annually repeated vaccination: A meta-analysis of serologic and field studies. Arch. Intern. Med. 1999, 159, 182–188. [Google Scholar] [CrossRef]
- Mclean, H.Q.; Thompson, M.G.; Sundaram, M.E.; Meece, J.K.; McClure, D.L.; Fridrich, T.C.; Belongia, E.A. Impact of repeated vaccination on vaccine effectiveness against influenza A (H3N2) and B during 8 seasons. Clin. Infect. Dis. 2014, 59, 1375–1385. [Google Scholar] [CrossRef]
- Ohmit, S.E.; Petrie, J.G.; Malosh, R.E.; Fry, A.M.; Thompson, M.G.; Monto, A.S. Influenza vaccine effectiveness in households with children during the 2012–2013 season: Assessment of prior vaccination and serologic susceptibility. J. Infect. Dis. 2015, 211, 1519–1528. [Google Scholar] [CrossRef]
- Ohta, A.; Murakami, Y.; Hashimoto, S.; Nagai, M.; Kawado, M.; Izumida, M.; Tada, Y.; Shigematsu, M.; Yasui, Y.; Taniguchi, K. Epidemics of influenza and pediatric diseases observed in infectious disease surveillance in Japan, 1999–2005. J. Epidemiol. 2007, 17 (Suppl. S), 14–22. [Google Scholar] [CrossRef] [PubMed]
- Nakauchi, M.; Yasui, Y.; Miyoshi, T.; Minagawa, H.; Tanaka, T.; Tashiro, T.; Kageyama, T. One-step real-time reverse transcription-PCR assays for detecting and subtyping pandemic influenza A/H1N1 2009, seasonal influenza A/H1N1, and seasonal influenza A/H3N2 viruses. J. Virol. Methods 2011, 171, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Nakauchi, M.; Takayama, I.; Takahashi, H.; Oba, K.; Kubo, H.; Kaida, A.; Tashiro, M.; Kageyama, T. Real-time RT–PCR assays for discriminating influenza B virus Yamagata and Victoria lineages. J. Virol. Methods 2014, 205, 110–115. [Google Scholar] [CrossRef]
- Skowronski, D.M.; Chambers, C.; Sabaiduc, S.; Serres, G.D.; Winter, A.L.; Dickinson, J.A.; Krajden, M.; Gubbay, J.B.; Drews, S.J.; Martineau, C.; et al. A perfect storm: Impact of genomic variation and serial vaccination on low influenza vaccine effectiveness during the 2014–2015 season. Clin. Infect. Dis. 2016, 63, 21–32. [Google Scholar] [CrossRef]
- Belongia, E.A.; Skowronski, D.M.; Mclean, H.Q.; Chambers, C.; Sundaram, M.E.; Serres, G.D. Repeated influenza vaccination and vaccine effectiveness. Expert Rev. Vaccines 2017, 16, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Shinjoh, M.; Sugaya, N.; Yamaguchi, Y.; Iibuchi, N.; Kamimaki, I.; Goto, A.; Kobayashi, H.; Kobayashi, Y.; Shibata, M.; Tamaoka, S.; et al. Inactivated influenza vaccine effectiveness and an analysis of repeated vaccination for children during the 2016/17 season. Vaccine 2018, 36, 5510–5518. [Google Scholar] [CrossRef]
- Kwong, J.C.; Chung, H.; Jung, J.K.H.; Buchan, S.A.; Campigotto, A.; Campitelli, M.A.; Crowcroft, N.S.; Gubbay, J.B.; Karnauchow, T.; Katz, K.; et al. The impact of repeated vaccination using 10-year vaccination history on protection against in older adults: A test-negative design study across the 2010/11 to 2015/16 influenza seasons in Ontario, Canada. Eur. Surveill. 2020, 25, 1900245. [Google Scholar] [CrossRef]
- Ramsay, L.C.; Buchan, S.A.; Stirling, R.G.; Cowling, B.J.; Feng, S.; Kwong, J.C.; Warshawsky, B.F. The impact of repeated vaccination on influenza vaccine effectiveness: A systematic review and meta-analysis. BMC Med. 2019, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Song, J.Y.; Noh, J.Y.; Lee, J.S.; Wie, S.H.; Kim, Y.K.; Lee, J.; Jeong, H.W.; Kim, S.W.; Lee, S.H.; Park, K.H.; et al. Effectiveness of repeated influenza vaccination among the elderly population with high annual vaccine uptake rates during the three consecutive A/H3N2 epidemics. Vaccine 2020, 38, 318–322. [Google Scholar] [CrossRef]
- Saito, N.; Komori, K.; Suzuki, M.; Morimoto, K.; Kishikawa, T.; Yasaka, T.; Ariyoshi, K. Negative impact of prior influenza vaccination on current influenza vaccination among people infected and not infected in prior season: A test-negative case–control study in Japan. Vaccine 2017, 35, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Caspard, H.; Heikkinen, T.; Belshe, R.B.; Ambrose, C. A systematic review of the efficacy of live attenuated influenza vaccine upon revaccination of children. Hum. Vaccines Immunother. 2016, 12, 1721–1727. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cheng, A.C.; Macartney, K.K.; Waterer, G.W.; Kotsimbos, T.; Kelly, P.M.; Blyth, C.C. Repeated vaccination does not appear to impact upon influenza vaccine effectiveness against hospitalization with confirmed influenza. Clin. Infect. Dis. 2017, 64, 1564–1572. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.S.; Lian, I.B.; Chao, D.Y. A population-based propensity score-matched study to assess the impact of repeated vaccination on vaccine effectiveness for influenza-associated hospitalization among the elderly. Clin. Interv. Aging 2020, 15, 301–312. [Google Scholar] [CrossRef]
- Castilla, J.; Navascués, A.; Casado, I.; Díaz-González, J.; Pérez-García, A.; Fernandino, L.; Martinez-Baz, I.; Aguinaga, A.; Pozo, F.; Ezpeleta, C.; et al. Combined effectiveness of prior and current season influenza vaccination in northern Spain: 2016/17 mid-season analysis. Eur. Surveill 2017, 22, 30465. [Google Scholar] [CrossRef]
- McLean, H.Q.; Caspard, H.; Griffin, M.R.; Gaglani, M.; Peters, T.R.; Poehling, K.A.; Ambrose, C.S.; Belongia, E.A. Association of prior vaccination with influenza vaccine effectiveness in children receiving live attenuated or inactivated vaccine. JAMA Netw. Open 2018, 1, e183742. [Google Scholar] [CrossRef]
- Thompson, M.G.; Naleway, A.; Fry, A.M.; Ball, S.; Spencer, S.M.; Reynolds, S.; Bozeman, S.; Levine, M.; Katz, J.M.; Gaglani, M. Effects of repeated annual inactivated influenza vaccination among healthcare personnel on serum hemagglutinin inhibition antibody response to A/Perth/16/2009 (H3N2)-like virus during 2010–2011. Vaccine 2016, 34, 981–988. [Google Scholar] [CrossRef]
- Sasaki, S.; He, X.S.; Holmes, T.H.; Dekker, C.L.; Kemble, G.W.; Arvin, A.M.; Greenberg, H.B. Influence of prior vaccination on antibody and B-cell responses. PLoS ONE 2008, 3, e2975. [Google Scholar] [CrossRef]
- Kim, J.H.; Mishina, M.; Chung, J.R.; Cole, K.S.; Nowalk, M.P.; Martin, J.M.; Spencer, S.; Flannery, B.; Zimmerman, R.K.; Sambhara, S. Cell-mediated immunity against antigenically drifted influenza A(H3N2) viruses in children during a vaccine mismatch season. J. Infect. Dis. 2016, 214, 1030–1038. [Google Scholar] [CrossRef]
- Bodewes, R.; Fraaij, P.L.; Kreijtz, J.H.; Geelhoed-Mieras, M.M.; Fouchier, R.A.; Osterhaus, A.D.; Rimmelzwaan, G.F. Annual influenza vaccination affects the development of heterosubtypic immunity. Vaccine 2012, 30, 7407–7410. [Google Scholar] [CrossRef]
- Bodewes, R.; Fraaij, P.L.; Geelhoed-Mieras, M.M.; Baalen, C.A.; Tiddens, H.A.; Rossum, A.M.; Klis, F.R.; Fouchier, R.A.; Osterhaus, A.D.; Rimmelzwaan, G.F. Annual vaccination against influenza virus hampers development of virus-specific CD8+ T cell immunity in children. J. Virol. 2011, 85, 11995–12000. [Google Scholar] [CrossRef]
- Ito, K.; Mugitani, A.; Irie, S.; Ishibashi, M.; Takasaki, Y.; Shindo, S.; Yokoyama, T.; Yamashita, Y.; Shibao, K.; Koyanagi, H. Prior vaccinations improve immunogenicity of inactivated influenza vaccine in young children aged 6 months to 3 years: A cohort study. Medicine 2018, 97, e11551. [Google Scholar] [CrossRef]
- Floppa, I.M.; Ferdinands, J.M.; Chung, J.; Flannery, B.; Fry, A.M. Vaccination history as a confounder of studies of influenza vaccine effectiveness. Vaccine X 2019, 1, 100008. [Google Scholar] [CrossRef]
- Valenciano, M.; Kissling, E.; Larrauri, A.; Nunes, B.; Pitigoi, D.; O’Donnell, J.; Reuss, A.; Horvath, J.K.; Paradowska-Stankiewicz, I.; Rizzo, C.; et al. Exploring the effect of previous inactivated influenza vaccination on seasonal influenza vaccine effectiveness against medically attended influenza: Results of the European I-MOVE multicentre test-negative case–control study, 2011/2012–2016/2017. Influenza Other Respir. Viruses 2018, 12, 567–581. [Google Scholar] [CrossRef]
- Kim, S.S.; Flannery, B.; Foppa, I.M.; Chung, J.R.; Nowalk, M.P.; Zimmerman, R.K.; Gaglani, M.; Monto, A.S.; Martin, E.T.; Belongia, E.A.; et al. Effects of prior season vaccination on current season vaccine in the United States flu vaccine effectiveness network, 2012–2013 through 2017–2018. Clin. Infect. Dis. 2021, 73, 497–505. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Cases (n = 799) | Controls (n = 1196) | p-Value a |
|---|---|---|---|
| Male | 430 (54) | 652 (54) | 0.76 |
| Age (years) | |||
| Median (range) | 3 (1–5) | 2 (1–5) | <0.01 |
| Age (years) | |||
| 1 | 136 (17) | 371 (31) | |
| 2 | 143 (18) | 290 (24) | |
| 3 | 159 (20) | 213 (18) | |
| 4 | 191 (24) | 196 (16) | |
| 5 | 170 (21) | 126 (11) | <0.01 |
| Enrolment season | |||
| 2016/17 | 367 (46) | 627 (52) | |
| 2017/18 | 432 (54) | 569 (48) | <0.01 |
| Siblings (present) | 641 (80) | 835 (70) | <0.01 |
| Nursery school (yes) | 662 (83) | 896 (75) | <0.01 |
| Medical comorbidities b | 70 (9) | 130 (11) | 0.12 |
| Number of outpatient visits in last year | |||
| 0–4 | 471 (59) | 549 (46) | |
| 5–9 | 209 (26) | 367 (31) | |
| ≥10 | 119 (15) | 280 (23) | <0.01 |
| Influenza vaccination in prior season | 255 (32) | 434 (36) | 0.04 |
| Vaccinated until the season before the prior season (+) c | 281 (35) | 313 (26) | <0.01 |
| Influenza diagnosis in prior season (+) | 157 (20) | 175 (15) | <0.01 |
| Variables | Cases (n = 799) | Controls (n = 1196) | p-Value a |
|---|---|---|---|
| Maximum body temperature (°C) | |||
| Median (range) | 39.0 (38.0–41.0) | 39.0 (38.0–41.5) | 0.03 |
| Maximum body temperature (°C) | |||
| 38.0–38.9 | 320 (40) | 525 (44) | |
| ≥39.0 | 479 (60) | 671 (56) | 0.09 |
| Cough (+) | 644 (81) | 844 (71) | <0.01 |
| Sore throat (+) | 160 (20) | 183 (15) | <0.01 |
| Runny nose (+) | 712 (89) | 1124 (94) | <0.01 |
| Dyspnea (+) | 122 (15) | 225 (19) | 0.04 |
| Interval between illness onset to enrolment (days) | |||
| Median [range] | 1 (0–6) | 1 (0–7) | <0.01 |
| 0–2 | 762 (95) | 1077 (90) | |
| ≥3 | 37 (5) | 119 (10) | <0.01 |
| Current Dose | Cases (n = 799) | Controls (n = 1196) | Crude VE (95% CI) | Adjusted VE (95% CI) a | Adjusted VE (95% CI) b |
|---|---|---|---|---|---|
| 0 | 513 (64) | 561 (47) | Reference | Reference | Reference |
| 1 | 77 (10) | 139 (12) | 39% (18% to 55%) | 66% (46% to 78%) | 57% (30% to 74%) |
| 2 | 209 (24) | 496 (41) | 54% (44% to 62%) | 60% (47% to 70%) | 51% (32% to 65%) |
| Current Dose | Prior Vaccination | n (%) | Crude VE (95% CI) | Adjusted VE (95% CI) a | Adjusted VE (95% CI) b | |
|---|---|---|---|---|---|---|
| Cases (n = 799) | Controls (n = 1196) | |||||
| 0 | Unvaccinated | 458 (57) | 493 (41) | Reference | Reference | Reference |
| 0 | Vaccinated | 55 (7) | 68 (6) | 13% (−27% to 40%) | 27% (−25% to 57%) | 29% (−25% to 59%) |
| 1 | Unvaccinated | 25 (3) | 45 (4) | 40% (1% to 64%) | 54% (12% to 77%) | 53% (6% to 76%) |
| 1 | Vaccinated | 52 (7) | 94 (8) | 41% (15% to 59%) | 73% (53% to 85%) | 70% (45% to 83%) |
| 2 | Unvaccinated | 61 (8) | 224 (19) | 71% (60% to 79%) | 61% (40% to 74%) | 56% (32% to 72%) |
| 2 | Vaccinated | 148 (19) | 272 (23) | 41% (26% to 54%) | 62% (46% to 74%) | 61% (42% to 73%) |
| Current Vaccination Dose | n (%) | Crude VE (95% CI) | Adjusted VE (95% CI) a | Adjusted VE (95% CI) b | |
|---|---|---|---|---|---|
| Unvaccinated in prior season | Cases (n = 544) | Controls (n = 762) | |||
| 0 | 458 (84) | 493 (65) | Reference | Reference | Reference |
| 1 | 25 (5) | 45 (6) | 40% (1% to 64%) | 44% (−22% to 74%) | 40% (−35% to 73%) |
| 2 | 61 (11) | 224 (29) | 71% (60% to 79%) | 64% (42% to 78%) | 60% (34% to 75%) |
| Vaccinated in prior season | Cases (n = 255) | Controls (n = 434) | |||
| 0 | 55 (22) | 68 (16) | Reference | Reference | Reference |
| 1 | 52 (20) | 94 (22) | 32% (−12% to 58%) | 76% (31% to 91%) | 80% (36% to 94%) |
| 2 | 148 (58) | 272 (62) | 33% (−1% to 55%) | 69% (29% to 87%) | 75% (36% to 90%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, K.; Fukushima, W.; Morikawa, S.; Fujioka, M.; Matsushita, T.; Kubota, M.; Yagi, Y.; Takasaki, Y.; Shindo, S.; Yamashita, Y.; et al. Influence of Prior Influenza Vaccination on Current Influenza Vaccine Effectiveness in Children Aged 1 to 5 Years. Vaccines 2021, 9, 1447. https://doi.org/10.3390/vaccines9121447
Matsumoto K, Fukushima W, Morikawa S, Fujioka M, Matsushita T, Kubota M, Yagi Y, Takasaki Y, Shindo S, Yamashita Y, et al. Influence of Prior Influenza Vaccination on Current Influenza Vaccine Effectiveness in Children Aged 1 to 5 Years. Vaccines. 2021; 9(12):1447. https://doi.org/10.3390/vaccines9121447
Chicago/Turabian StyleMatsumoto, Kazuhiro, Wakaba Fukushima, Saeko Morikawa, Masashi Fujioka, Tohru Matsushita, Megumi Kubota, Yoshina Yagi, Yoshio Takasaki, Shizuo Shindo, Yuji Yamashita, and et al. 2021. "Influence of Prior Influenza Vaccination on Current Influenza Vaccine Effectiveness in Children Aged 1 to 5 Years" Vaccines 9, no. 12: 1447. https://doi.org/10.3390/vaccines9121447
APA StyleMatsumoto, K., Fukushima, W., Morikawa, S., Fujioka, M., Matsushita, T., Kubota, M., Yagi, Y., Takasaki, Y., Shindo, S., Yamashita, Y., Yokoyama, T., Kiyomatsu, Y., Hiroi, S., Nakata, K., Maeda, A., Kondo, K., Ito, K., Kase, T., Ohfuji, S., & Hirota, Y. (2021). Influence of Prior Influenza Vaccination on Current Influenza Vaccine Effectiveness in Children Aged 1 to 5 Years. Vaccines, 9(12), 1447. https://doi.org/10.3390/vaccines9121447