
The Cost-Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine in Seven Chinese Cities

 ,
,
Abstract
:1. Introduction
2. Methods
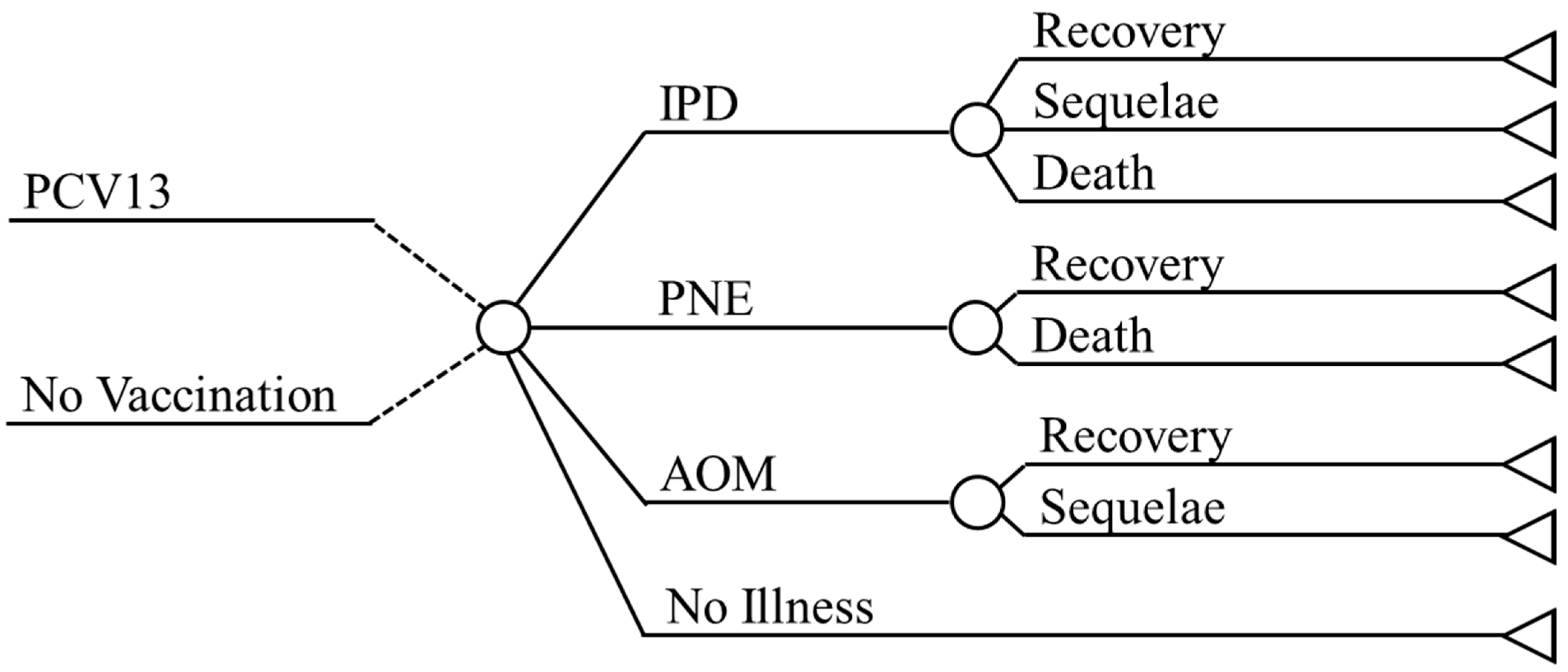
2.1. Approach
2.2. Demographic Inputs
2.3. Epidemiologic Inputs
2.4. Vaccine Effectiveness
2.5. Direct Costs
2.6. Quality of Life
2.7. Analysis
3. Results
3.1. Base Case Results
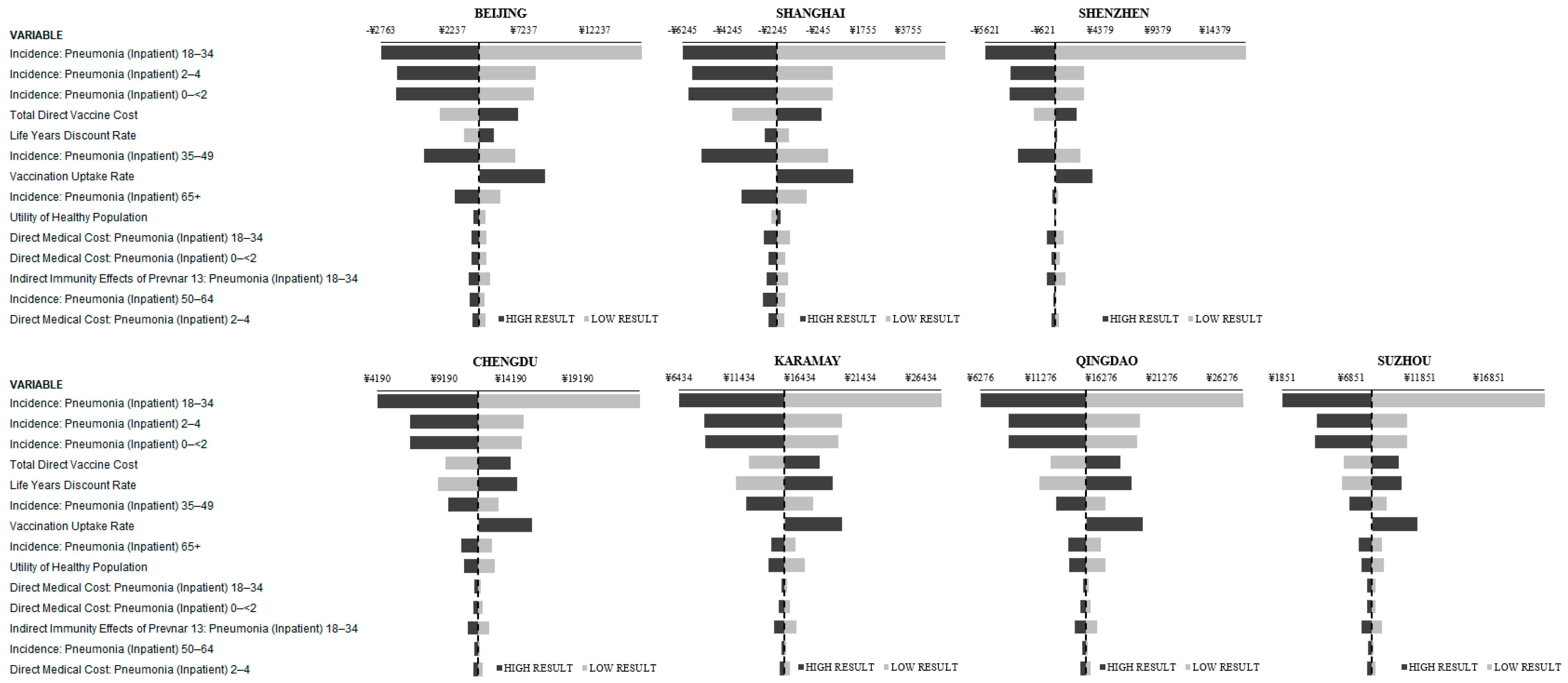
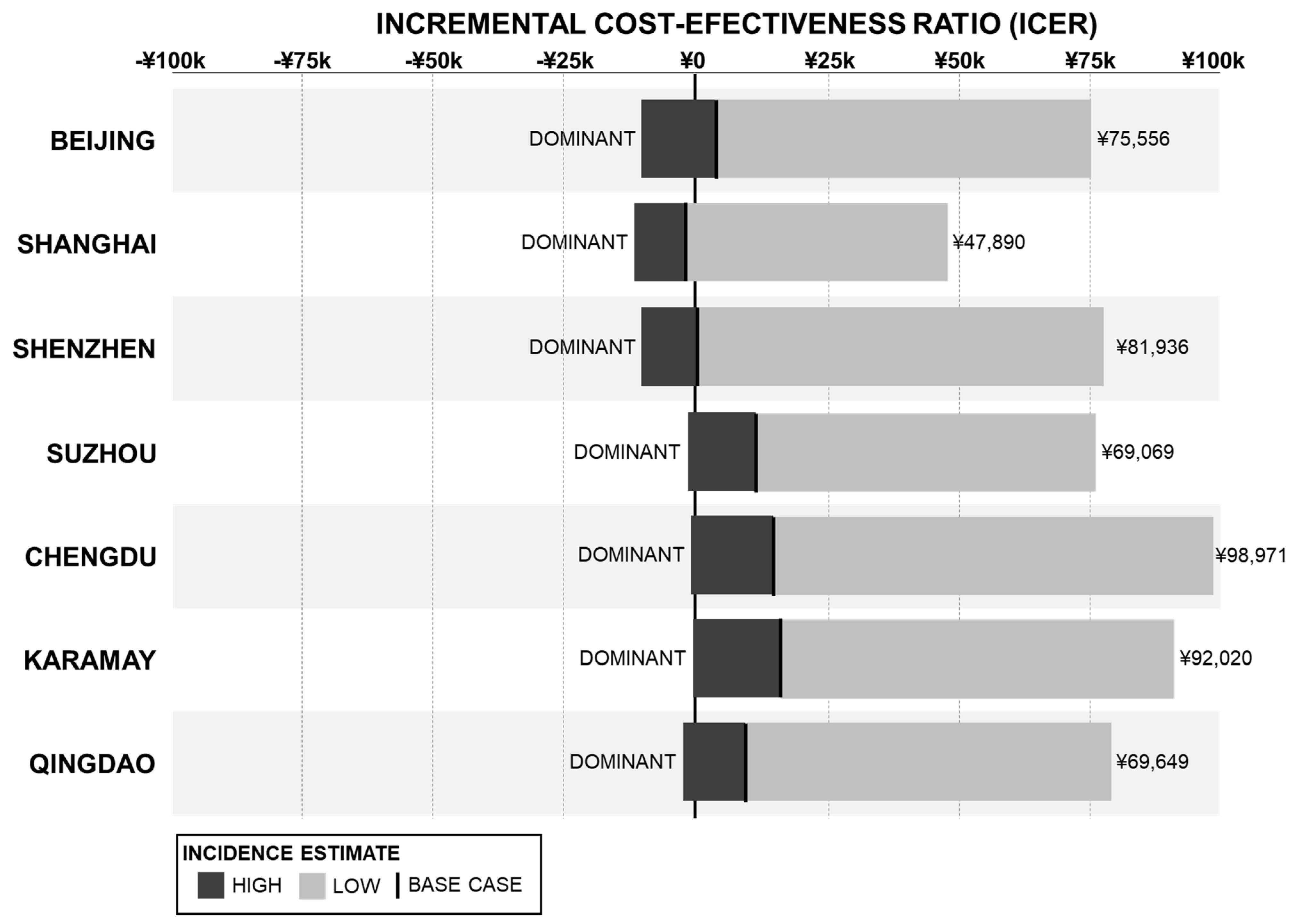
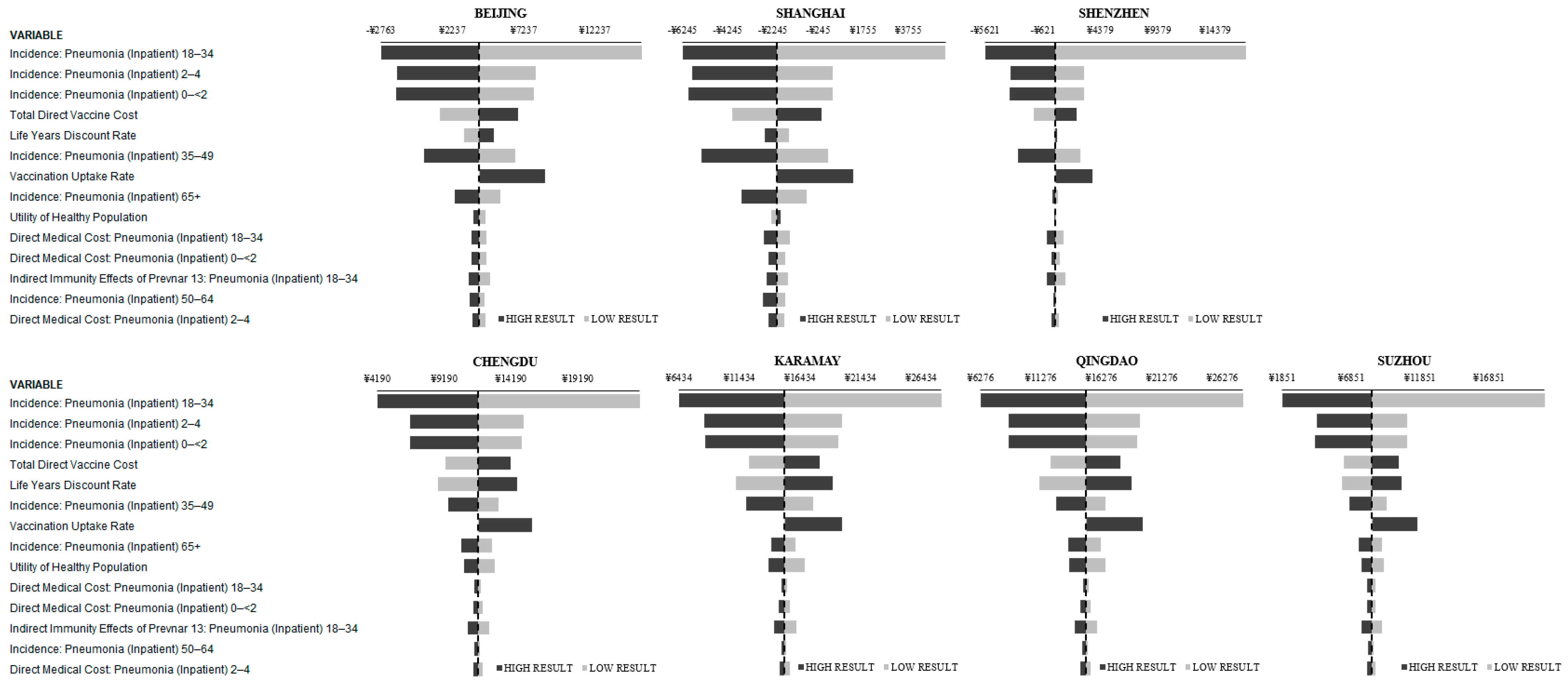
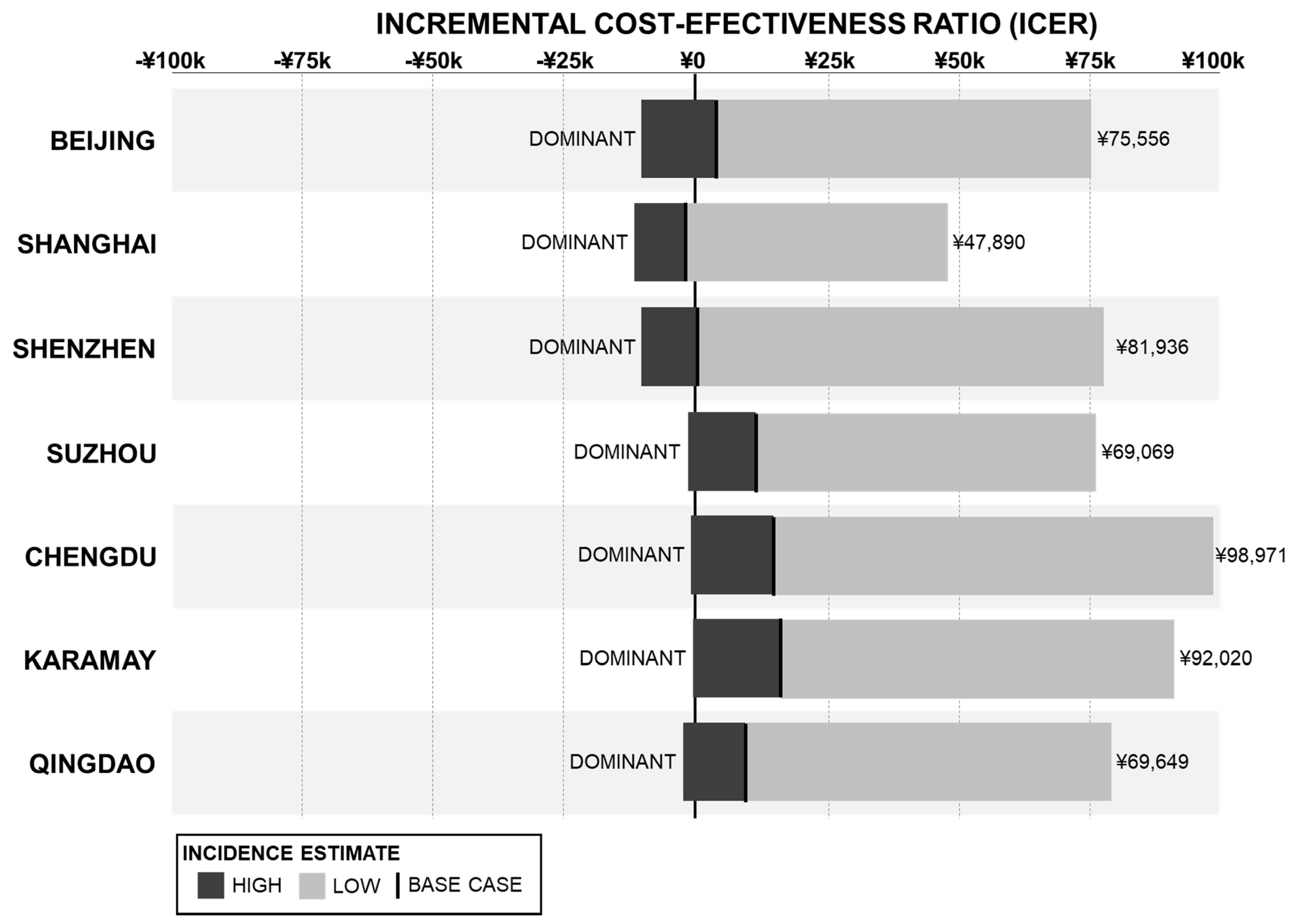
3.2. Incidence Rate Analysis
3.3. DE-Only Scenario
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Estimated Hib and Pneumococcal Deaths for Children under 5 Years of Age. 2008. Available online: http://www.who.int/immunization/monitoring_surveillance/burden/estimates/Pneumo_hib/en/ (accessed on 23 April 2021).
- Ceyhan, M.; Ozsurekci, Y.; Aykac, K.; Hacibedel, B.; Ozbilgili, E. Economic burden of pneumococcal infections in children under 5 years of age. Hum. Vaccines Immunother. 2018, 14, 106–110. [Google Scholar] [CrossRef] [Green Version]
- O'Brien, K.L.; Wolfson, L.J.; Watt, J.P.; Henkle, E.; Deloria-Knoll, M.; McCall, N.; Lee, E.; Mulholland, K.; Levine, O.S.; Cherian, T. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: Global estimates. Lancet 2009, 374, 893–902. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. China. Available online: http://www.healthdata.org/china (accessed on 14 April 2020).
- Yao, K.H.; Yang, Y.H. Streptococcus pneumoniae diseases in Chinese children: Past, present and future. Vaccine 2008, 26, 4425–4433. [Google Scholar] [CrossRef]
- Chen, Y.; Deng, W.; Wang, S.-M.; Mo, Q.-M.; Jia, H.; Wang, Q.; Li, S.-G.; Li, X.; Yao, B.-D.; Liu, C.-J.; et al. Burden of pneumonia and meningitis caused by Streptococcus pneumoniae in China among children under 5 years of age: A systematic literature review. PLoS ONE 2011, 6, e27333. [Google Scholar] [CrossRef] [PubMed]
- Rudan, I.; Boschi-Pinto, C.; Biloglav, Z.; Mulholland, K.; Campbell, H. Epidemiology and etiology of childhood pneumonia. Bull. World Health Organ. 2008, 86, 408–416. [Google Scholar] [CrossRef] [Green Version]
- Mondiale de la Santé, O.; World Health Organization. Pneumococcal conjugate vaccines in infants and children under 5 years of age: WHO position paper–February 2019. Wkly. Epidemiol. Rec. 2019, 94, 85–104. [Google Scholar]
- Grijalva, C.; Nuorti, J.P.; Arbogast, P.G.; Martin, S.W.; Edwards, K.M.; Griffin, M.R. Decline in pneumonia admissions after routine childhood immunisation with pneumococcal conjugate vaccine in the USA: A time-series analysis. Lancet 2007, 369, 1179–1186. [Google Scholar] [CrossRef]
- Dinleyici, E.C.; Yargic, Z.A. Pneumococcal conjugated vaccines: Impact of PCV-7 and new achievements in the postvaccine era. Expert Rev. Vaccines 2008, 7, 1367–1394. [Google Scholar] [CrossRef]
- Zhou, F.; Shefer, A.; Kong, Y.; Nuorti, J.P. Trends in acute otitis media-related health care utilization by privately insured young children in the United States, 1997–2004. Pediatrics 2008, 121, 253–260. [Google Scholar] [CrossRef]
- Rose, M.; Zielen, S. Impact of infant immunization programs with pneumococcal conjugate vaccine in Europe. Expert Rev. Vaccines 2009, 8, 1351–1364. [Google Scholar] [CrossRef] [PubMed]
- PPilishvili, T.; Lexau, C.; Farley, M.M.; Hadler, J.; Harrison, L.H.; Bennett, N.M.; Reingold, A.; Thomas, A.; Schaffner, W.; Craig, A.S.; et al. Sustained reductions in invasive pneumococcal disease in the era of conjugate vaccine. J. Infect. Dis. 2010, 201, 32–41. [Google Scholar] [CrossRef]
- Simonsen, L.; Taylor, R.J.; Schuck-Paim, C.; Lustig, R.; Haber, M.; Klugman, K.P. Effect of 13-valent pneumococcal conjugate vaccine on admissions to hospital 2 years after its introduction in the USA: A time series analysis. Lancet Respir. Med. 2014, 2, 387–394. [Google Scholar] [CrossRef]
- Zhu, F.; Hu, Y.; Li, J.; Ye, Q.; Young, M.M.; Zhou, X.; Chen, Z.; Yan, B.; Liang, J.Z.; Gruber, W.C.; et al. Immunogenicity and safety of 13-valent pneumococcal conjugate vaccine compared with 7-valent pneumococcal conjugate vaccine among healthy infants in China. Pediatric Infect. Dis. J. 2016, 35, 999–1010. [Google Scholar] [CrossRef]
- Wu, D.B.C.; Chaiyakunapruk, N.; Chong, H.Y.; Beutels, P. Choosing between 7-, 10-and 13-valent pneumococcal conjugate vaccines in childhood: A review of economic evaluations (2006–2014). Vaccine 2015, 33, 1633–1658. [Google Scholar] [CrossRef] [PubMed]
- Maurer, K.A.; Chen, H.-F.; Wagner, A.L.; Hegde, S.T.; Patel, T.; Boulton, M.L.; Hutton, D.W. Cost-effectiveness analysis of pneumococcal vaccination for infants in China. Vaccine 2016, 34, 6343–6349. [Google Scholar] [CrossRef] [PubMed]
- Mo, X.; Tobe, R.G.; Liu, X.; Mori, R. Cost-effectiveness and health benefits of pediatric 23-valent pneumococcal polysaccharide vaccine, 7-valent pneumococcal conjugate vaccine and forecasting 13-valent pneumococcal conjugate vaccine in China. Pediatric Infect. Dis. J. 2016, 35, e353–e361. [Google Scholar] [CrossRef]
- Shen, K.; Wasserman, M.; Liu, D.; Yang, Y.H.; Yang, J.; Guzauskas, G.F.; Wang, B.C.; Hilton, B.; Farkouh, R. Estimating the cost-effectiveness of an infant 13-valent pneumococcal conjugate vaccine national immunization program in China. PLoS ONE 2018, 13, e0201245. [Google Scholar] [CrossRef]
- Zhou, H.; He, J.; Wu, B.; Che, D. Cost-effectiveness analysis of routine 13-valent pneumococcal conjugate vaccinations in Chinese infants. Hum. Vaccines Immunother. 2018, 14, 1444–1452. [Google Scholar] [CrossRef]
- Earnshaw, S.R.; McDade, C.L.; Zanotti, G.; Farkouh, R.A.; Strutton, D. Cost-effectiveness of 2 + 1 dosing of 13-valent and 10-valent pneumococcal conjugate vaccines in Canada. BMC Infect. Dis. 2012, 12, 101. [Google Scholar] [CrossRef] [Green Version]
- Klok, R.M.; Lindkvist, R.-M.; Ekelund, M.; Farkouh, R.A.; Strutton, D.R. Cost-effectiveness of a 10- versus 13- valent pneumococcal conjugate vaccine in Denmark and Sweden. Clin. Ther. 2013, 35, 119–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mucino-Ortega, E.; Mould-Quevedo, J.F.; Farkouh, R.; Strutton, D. Economic evaluation of an infant immunization program in Mexico, based on 13-valent pneumococcal conjugated vaccines. Value Health 2011, 14 (5 Suppl. 1), S65–S70. [Google Scholar] [CrossRef] [Green Version]
- Strutton, D.R.; Farkouh, R.A.; Earnshaw, S.R.; Hwang, S.; Theidel, U.; Kontodimas, S.; Klok, R.; Papanicolaou, S. Cost-effectiveness of 13-valent pneumococcal conjugate vaccine: Germany, Greece, and The Netherlands. J. Infect. 2012, 64, 54–67. [Google Scholar] [CrossRef]
- Wasserman, M.; Mendoza, C.F.; Grajales, A.G.; Palacios, M.G.; Di Fusco, M. Cost-effectiveness of the 13-valent (PCV13) versus 10-valent (PCV10) pneumococcal conjugate vaccines as part of routine infant pneumococcal vaccination in Mexico. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Brinkhoff T 2019 City Population—Population Statistics in Maps and Charts for Cities, Agglomerations and Administrative Divisions of All Countries of the World. Available online: https://citypopulation.de/ (accessed on 23 January 2020).
- Hu, S.; Shi, Q.; Chen, C.I.; Caldwell, R.; Wang, B.; Du, L.; He, J.; Roberts, C.S. Estimated public health impact of nationwide vaccination of infants with 7-valent pneumococcal conjugate vaccine (PCV7) in China. Int. J. Infect. Dis. 2014, 26, 116–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldwell, R.; Roberts, C.S.; An, Z.; Chen, C.I.; Wang, B. The health and economic impact of vaccination with 7-valent pneumococcal vaccine (PCV7) during an annual influenza epidemic and influenza pandemic in China. BMC Infect. Dis. 2015, 15, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Che, D.; Zhou, H.; He, J.; Wu, B. Modeling the impact of the 7-valent pneumococcal conjugate vaccine in Chinese infants: An economic analysis of a compulsory vaccination. BMC Health Serv. Res. 2014, 14, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Wang, H.; Chen, M.; Sun, Z.; Zhao, R.; Zhang, L.; Wang, H.; Zhang, H.; Wang, L.; Chu, Y.; et al. Serotype distribution and antimicrobial resistance patterns of Streptococcus pneumoniae isolated from children in China younger than 5 years. Diagn. Microbiol. Infect. Dis. 2008, 61, 256–263. [Google Scholar] [CrossRef]
- Yao, K.H.; Wang, L.B.; Zhao, G.M.; Zheng, Y.J.; Deng, L.; Huang, J.F.; Wang, J.X.; Zhao, R.Z.; Deng, Q.L.; Hu, Y.H.; et al. Pneumococcal serotype distribution and antimicrobial resistance in Chinese children hospitalized for pneumonia. Vaccine 2011, 29, 2296–2301. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, W.P.; Yothers, G.; Dagan, R.; Kilpi, T.; Pelton, S.I.; Cohen, R.; Jacobs, M.R.; Kaplan, S.L.; Levy, C.; Lopez, E.L.; et al. Multinational study of pneumococcal serotypes causing acute otitis media in children. Pediatric Infect. Dis. J. 2002, 21, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Shi, Q.; Song, S.; Du, L.; He, J.; Chen, C.-I.; Caldwell, R.; Wang, B.; Roberts, C.S. Estimating the cost-effectiveness of the 7-valent pneumococcal conjugate vaccine in Shanghai, China. Value Health Reg. Issues 2014, 3, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, S.B.; Shinefield, H.R.; Ling, S.; Hansen, J.; Fireman, B.; Spring, D.; Noyes, J.; Lewis, E.; Ray, P.; Lee, J.; et al. Effectiveness of heptavalent pneumococcal conjugate vaccine in children younger than five years of age for prevention of pneumonia. Pediatric Infect. Dis. J. 2002, 21, 810–815. [Google Scholar] [CrossRef]
- Ray, G.T.; Whitney, C.G.; Fireman, B.H.; Ciuryla, V.; Black, S.B. Cost-effectiveness of pneumococcal conjugate vaccine: Evidence from the first 5 years of use in the United States incorporating herd effects. Pediatric Infect. Dis. J. 2006, 25, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Fireman, B.; Black, S.B.; Shinefield, H.R.; Lee, J.; Lewis, E.; Ray, P. Impact of the pneumococcal conjugate vaccine on otitis media. Pediatric Infect. Dis. J. 2003, 22, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.R.; Link-Gelles, R.; Schaffner, W.; Lynfield, R.; Lexau, C.; Bennett, N.M.; Petit, S.; Zansky, S.M.; Harrison, L.H.; Reingold, A.; et al. Effect of use of 13-valent pneumococcal conjugate vaccine in children on invasive pneumococcal disease in children and adults in the USA: Analysis of multisite, population-based surveillance. Lancet Infect. Dis. 2015, 15, 301–309. [Google Scholar] [CrossRef] [Green Version]
- Moore, M.R.; Link-Gelles, R.; Schaffner, W.; Lynfield, R.; Holtzman, C.; Harrison, L.H.; Zansky, S.M.; Rosen, J.B.; Reingold, A.; Scherzinger, K.; et al. Effectiveness of 13-valent pneumococcal conjugate vaccine for prevention of invasive pneumococcal disease in children in the USA: A matched case-control study. Lancet Respir. Med. 2016, 4, 399–406. [Google Scholar] [CrossRef]
- Waight, P.A.; Andrews, N.J.; Ladhani, S.N.; Sheppard, C.L.; Slack, M.P.E.; Miller, E. Effect of the 13-valent pneumococcal conjugate vaccine on invasive pneumococcal disease in England and Wales 4 years after its introduction: An observational cohort study. Lancet Infect. Dis. 2015, 15, 535–543. [Google Scholar] [CrossRef] [Green Version]
- Zhu, F.; Hu, Y.; Li, J.; Ye, Q.; Young, M.M.; Liang, J.Z.; Gruber, W.C.; Giardina, P.C.; Scott, D.A. Immunogenicity and Safety of the 13-Valent Pneumococcal Conjugate Vaccine Administered in a 3+ 1 versus 2+ 1 Dose Schedule Among Infants in China. Pediatric Infect. Dis. J. 2019, 38, 1150–1158. [Google Scholar] [CrossRef]
- Jiangsu Development and Reform Commission. Notice of the Provincial Development and Reform Commission of the Provincial Department of Finance on the Approval of Vaccination Service Fees. 2020. Available online: http://fzggw.jiangsu.gov.cn/art/2020/11/13/art_284_9578645.html (accessed on 9 November 2020).
- Development and Reform Commission of Shenzhen Municipality. Notice of the Guangdong Provincial Development and Reform Commission of the Guangdong Provincial Department of Finance on Extending the Fee Schedule of Vaccination Services for Non-Immunization Programs. 2021. Available online: http://fgw.sz.gov.cn/ztzl/zdlyxxgkzl/xzsyxsf/content/post_8577013.html (accessed on 9 November 2020).
- Beijing Price Monitoring Center. Notice of the Beijing Municipal Development and Reform Commission, the Beijing Municipal Health and Family Planning Commission and the Beijing Municipal Human Resources and Social Security Bureau on Setting the Price of the Second Type of Vaccination Service for Beijing Municipality (Beijing Municipal Development and Reform [2018] No. 362). 2018. Available online: http://www.beijingprice.cn/c/2018-03-06/502119.shtml (accessed on 9 November 2020).
- Sichuan Provincial Development and Reform Commission. Notice on the Fee Schedule of Vaccination Services and Its Related Issues (Sichuan Provincial Development and Reform [2018] No. 331). 2018. Available online: http://fgw.sc.gov.cn/sfgwsjd/c100030/2018/7/13/9878686f8a1744ca8f2b3257760b6c63.shtml (accessed on 9 November 2020).
- Qingdao Municipal Health Commission. Notice on Forwarding the “Notice of the Shandong Provincial Development and Reform Commission of the Shandong Provincial Department of Finance on the Fee Schedule of Vaccination Services for Non-Immunization Programs”. 2021. Available online: http://wsjkw.qingdao.gov.cn/n28356065/n32563139/n32563141/n32564190/210511193304387443.html (accessed on 10 November 2021).
- Qingdao Municipal Price Bureau. Notice of Qingdao Municipal Price Bureau and Qingdao Municipal Health and Family Planning Commission on Forwarding the “Notice of Shandong Provincial Price Bureau and Shandong Provincial Health and Family Planning Commission on Issues Concerning Storage and Transportation Fees for Type II Vaccines”. 2018. Available online: http://www.qingdao.gov.cn/n172/n24624151/n24629915/n24629929/n24629943/180126093021355736.html (accessed on 10 November 2021).
- Melegaro, A.; Edmunds, W. Cost-effectiveness analysis of pneumococcal conjugate vaccination in England and Wales. Vaccine 2004, 22, 4203–4214. [Google Scholar] [CrossRef]
- Morrow, A.; De Wals, P.; Petit, G.; Guay, M.; Erickson, L.J. The burden of pneumococcal disease in the Canadian population before routine use of the seven-valent pneumococcal conjugate vaccine. Can. J. Infect. Dis. Med Microbiol. 2007, 18, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- China Guidelines for Pharmacoeconomic Evaluations Working Group. China Guidelines for Pharmacoeconomic Evaluations. December 2020. Available online: https://tools.ispor.org/PEguidelines/source/China-Guidelines-for-Pharmacoeconomic-Evaluations-2020.pdf (accessed on 5 November 2021).
- European Medicines Agency (EMA). Prevenar 13: EPAR–Product Information. 26 March 2020. Available online: https://www.ema.europa.eu/documents/product-information/prevenar-13-epar-product-information_en.pdf (accessed on 2 September 2020).
- Stoecker, C.; Hampton, L.M.; Link-Gelles, R.; Messonnier, M.L.; Zhou, F.; Moore, M.R. Cost-effectiveness of using 2 vs. 3 primary doses of 13-valent pneumococcal conjugate vaccine. Pediatrics 2013, 132, e324–e332. [Google Scholar] [CrossRef] [Green Version]
- Davis, S.M.; Knoll, M.D.; Kassa, H.T.; O’Brien, K.L. Impact of pneumococcal conjugate vaccines on nasopharyngeal carriage and invasive disease among unvaccinated people: Review of evidence on indirect effects. Vaccine 2013, 32, 133–145. [Google Scholar] [CrossRef]
- Metcalf, B.J.; Gertz, R.E., Jr.; Gladstone, R.A.; Walker, H.; Sherwood, L.K.; Jackson, D.; Li, Z.; Law, C.; Hawkins, P.A.; Chochua, S.; et al. Strain features and distributions in pneumococci from children with invasive disease before and after 13 valent conjugate vaccine implementation in the United States. Clin. Microbiol. Infect. 2016, 22, 60.e9–60.e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Incidence (per 100,000) | 0–2 | 2–4 | 5–17 | 18–34 | 35–49 | 50–64 | 65+ |
|---|---|---|---|---|---|---|---|
| Pneumococcal Bacteremia † [17,18,19,20,27,28,29] | 5.03 (1.40–10.20) | 5.75 (1.98–9.47) | 16.64 (0.48–48.81) | 4.81 (0.54–12.48) | 4.50 (0.24–12.59) | 3.54 (0.50–9.21) | 14.57 (0.57–36.00) |
| Pneumococcal Meningitis † [17,18,19,20,27,28,29] | 2.49 (0.65–5.10) | 1.59 (0.31–4.73) | 5.14 (0.24–14.59) | 1.43 (0.12–3.83) | 1.41 (0.08–4.02) | 1.20 (0.09–3.41) | 2.37 (0.06–6.88) |
| Pneumonia | |||||||
| Inpatient † [18,19,20,27,28] | 8969 (2949–19,719) | 8740 (2681–19,710) | 4675 (334–13,027) | 788 (110–2116) | 497 (111–1190) | 656 (305–1221) | 2661 (1856–3700) |
| Outpatient † [18,19,20] | 12,797 (1568–24,027) | 15,749 (1642–29,857) | 3644 (643–6646) | 771 (186–1355) | 662 (166–1158) | 1035 (138–1931) | 3405 (147–6663) |
| Otitis Media | |||||||
| Mild † [18,19,20] | 9147 (2.32–16,762) | 8746 (29.45–15,531) | 2002 (24.87–3978) | 626 (5.39–1247) | 767 (5.89–1528) | 948 (3.17–1892) | 1043 (1.63–2085) |
| Moderate to Severe † [18,19,20] | 2793 (15.53–4472) | 2650 (105–3953) | 494 (98.43–889) | 72.16 (10.62–134) | 130 (8.39–252) | 174 (4.99–343) | 182 (2.19–361) |
| † CHIRA 2013–2015 | |||||||
| Pre-PCV13 Serotype Coverage | Base Case | ||||||
| Pneumococcal Bacteremia [30] | 0.87 | ||||||
| Pneumococcal Meningitis [30] | 0.87 | ||||||
| Pneumonia | |||||||
| Inpatient [31] | 0.92 | ||||||
| Outpatient [31] | 0.92 | ||||||
| Otitis Media | |||||||
| Mild [32] | 0.82 | ||||||
| Moderate to Severe [32] | 0.82 | ||||||
| Case Fatality Ratio | 0–2 | 2–4 | 5–17 | 18–34 | 35–49 | 50–64 | 65+ |
| Pneumococcal Bacteremia [17,33] | 0.04 | 0.01 | 0.05 | 0.05 | 0.06 | 0.06 | 0.06 |
| Pneumococcal Meningitis [17,33] | 0.14 | 0.03 | 0.04 | 0.00 | 0.12 | 0.00 | 0.02 |
| Inpatient Pneumonia [17,33] | 0.01 | 0.01 | 0.01 | 0.06 | 0.06 | 0.01 | 0.16 |
| Direct Effects | 0–2 | 2–4 | |||||
| Pneumococcal Bacteremia [34] | 0.94 | 0.94 | |||||
| Pneumococcal Meningitis [34] | 0.94 | 0.94 | |||||
| Pneumonia | |||||||
| Inpatient [34,35] | 0.29 | 0.29 | |||||
| Outpatient [34,35] | 0.07 | 0.07 | |||||
| Otitis Media | |||||||
| Mild [36] | 0.08 | 0.08 | |||||
| Moderate to Severe [36] | 0.17 | 0.17 | |||||
| INDIRECT EFFECT | 0–2 | 2–4 | 5–17 | 18–34 | 35–49 | 50–64 | 65+ |
| Pneumococcal Bacteremia [14,37,38] | 0.64 | 0.64 | 0.53 | 0.32 | 0.32 | 0.18 | 0.12 |
| Pneumococcal Meningitis [14,37,38] | 0.64 | 0.64 | 0.53 | 0.32 | 0.32 | 0.18 | 0.12 |
| Inpatient Pneumonia [14,37,38] | 0.22 | 0.17 | 0.00 | 0.12 | 0.05 | 0.02 | 0.03 |
| Direct Medical Costs | 0–2 | 2–4 | 5–17 | 18–34 | 35–49 | 50–64 | 65+ |
|---|---|---|---|---|---|---|---|
| Pneumococcal Bacteremia | |||||||
| Tier 1 | ¥695 | ¥2450 | ¥542 | ¥408 | ¥901 | ¥1407 | ¥2147 |
| National | ¥695 | ¥2450 | ¥542 | ¥408 | ¥901 | ¥1407 | ¥2147 |
| Pneumococcal Meningitis | |||||||
| Tier 1 | ¥377 | ¥87 | ¥321 | ¥3131 | ¥356 | ¥4640 | ¥13,587 |
| National | ¥25,602 | ¥5315 | ¥6967 | ¥13,105 | ¥5988 | ¥9345 | ¥6427 |
| Pneumonia | |||||||
| Inpatient | |||||||
| Tier 1 | ¥5470 | ¥3942 | ¥6030 | ¥11,372 | ¥29,034 | ¥17,567 | ¥31,486 |
| National | ¥4618 | ¥3101 | ¥3348 | ¥5140 | ¥5090 | ¥7518 | ¥11,820 |
| Outpatient | |||||||
| Tier 1 | ¥232 | ¥233 | ¥271 | ¥433 | ¥538 | ¥566 | ¥639 |
| National | ¥195 | ¥205 | ¥194 | ¥253 | ¥277 | ¥353 | ¥430 |
| Otitis Media | |||||||
| Mild | |||||||
| Tier 1 | ¥69 | ¥117 | ¥123 | ¥214 | ¥246 | ¥376 | ¥312 |
| National | ¥144 | ¥114 | ¥116 | ¥166 | ¥167 | ¥209 | ¥174 |
| Moderate to Severe | |||||||
| Tier 1 | ¥2269 | ¥3221 | ¥3050 | ¥3769 | ¥3143 | ¥4768 | ¥3569 |
| National | ¥2269 | ¥3221 | ¥3050 | ¥3769 | ¥3143 | ¥4768 | ¥3569 |
| Source: CHIRA 2013–2015 |
| TIER-1 CITIES | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beijing | Shanghai | Shenzhen | ||||||||||
| VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | ||||
| Cases of Pneumococcal Disease 1 | ||||||||||||
| Pneumococcal Bacteremia | 0.86 | 1.18 | −0.33 | 1.16 | 1.61 | −0.45 | 0.43 | 0.65 | −0.22 | |||
| Pneumococcal Meningitis | 0.23 | 0.33 | −0.10 | 0.31 | 0.44 | −0.13 | 0.13 | 0.20 | −0.07 | |||
| Pneumonia (Inpatient) | 248.80 | 283.21 | −34.41 | 326.51 | 361.70 | −35.19 | 136.24 | 153.68 | −17.44 | |||
| Pneumonia (Outpatient) | 345.32 | 350.96 | −5.63 | 423.44 | 428.60 | −5.16 | 167.06 | 169.60 | −2.54 | |||
| Otitis Media (Mild) | 69.28 | 72.83 | −3.55 | 63.47 | 66.72 | −3.25 | 31.22 | 32.82 | −1.60 | |||
| Otitis Media (Mod./Sev.) | 19.82 | 22.13 | −2.31 | 18.16 | 20.28 | −2.12 | 8.93 | 9.97 | −1.04 | |||
| Total Cases | 684.31 | 730.64 | −46.33 | 833.05 | 879.35 | −46.29 | 344.01 | 366.92 | −22.91 | |||
| Total Deaths | 12.74 | 13.56 | −0.82 | 17.27 | 18.32 | −1.05 | 4.30 | 4.75 | −0.45 | |||
| Total QALYs Lost | 135.95 | 147.96 | −12.01 | 181.87 | 196.75 | −14.88 | 66.20 | 73.86 | −7.66 | |||
| Costs 2 | ||||||||||||
| Vaccine Cost | ¥331.06 | ¥0.00 | ¥331.06 | ¥295.11 | ¥0.00 | ¥295.11 | ¥149.19 | ¥0.0 | ¥149.19 | |||
| Pneumococcal Bacteremia | ¥1.01 | ¥1.30 | −¥0.30 | ¥1.36 | ¥1.74 | −¥0.38 | ¥0.30 | ¥0.45 | −¥0.15 | |||
| Pneumococcal Meningitis | ¥0.96 | ¥1.16 | −¥0.19 | ¥1.29 | ¥1.55 | −¥0.26 | ¥0.28 | ¥0.37 | −¥0.09 | |||
| Pneumonia (Inpatient) | ¥3706.33 | ¥3979.43 | −¥273.11 | ¥4966.81 | ¥5282.32 | −¥315.51 | ¥1461.90 | ¥1598.34 | −¥136.44 | |||
| Pneumonia (Outpatient) | ¥140.62 | ¥141.93 | −¥1.31 | ¥179.26 | ¥180.46 | −¥1.20 | ¥59.07 | ¥59.66 | −¥0.59 | |||
| Otitis Media (Mild) | ¥46.40 | ¥46.75 | −¥0.35 | ¥58.79 | ¥59.10 | −¥0.32 | ¥20.94 | ¥21.10 | −¥0.16 | |||
| Otitis Media (Mod./Sev.) | ¥157.75 | ¥164.40 | −¥6.65 | ¥188.84 | ¥194.93 | −¥6.09 | ¥76.32 | ¥79.32 | −¥3.00 | |||
| Total Cost | ¥4384.13 | ¥4334.97 | ¥49.16 | ¥5691.46 | ¥5720.11 | −¥28.65 | ¥1768.01 | ¥1759.24 | ¥8.76 | |||
| ICER | ¥4093 | DOMINANT | ¥1145 | |||||||||
| Other Cities | ||||||||||||
| Chengdu | Karamay | Qingdao | Suzhou | |||||||||
| VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | |
| Cases of Pneumococcal Disease 1 | ||||||||||||
| Pneumococcal Bacteremia | 0.80 | 1.13 | −0.34 | 0.02 | 0.03 | −0.01 | 0.43 | 0.62 | −0.19 | 0.51 | 0.73 | −0.22 |
| Pneumococcal Meningitis | 0.21 | 0.32 | −0.10 | 0.01 | 0.01 | 0.00 | 0.12 | 0.17 | −0.06 | 0.14 | 0.21 | −0.07 |
| Pneumonia (Inpatient) | 241.40 | 266.76 | −25.36 | 6.73 | 7.54 | −0.81 | 136.13 | 152.15 | −16.02 | 152.21 | 168.37 | −16.16 |
| Pneumonia (Outpatient) | 304.27 | 308.25 | −3.98 | 8.63 | 8.77 | −0.14 | 176.60 | 179.28 | −2.68 | 190.24 | 192.62 | −2.38 |
| Otitis Media (Mild) | 49.00 | 51.51 | −2.51 | 1.69 | 1.78 | −0.09 | 32.94 | 34.63 | −1.69 | 29.29 | 30.79 | −1.50 |
| Otitis Media (Mod./Sev.) | 14.02 | 15.65 | −1.63 | 0.48 | 0.54 | −0.06 | 9.43 | 10.52 | −1.10 | 8.38 | 9.36 | −0.98 |
| Total Cases | 609.69 | 643.61 | −33.92 | 17.56 | 18.67 | −1.10 | 355.65 | 377.37 | −21.72 | 380.78 | 402.08 | −21.30 |
| Total Deaths | 11.16 | 11.84 | −0.68 | 0.26 | 0.28 | −0.02 | 6.14 | 6.51 | −0.38 | 7.01 | 7.47 | −0.46 |
| Total QALYs Lost | 119.53 | 129.24 | −9.71 | 3.03 | 3.30 | −0.27 | 65.12 | 70.55 | −5.43 | 78.79 | 85.66 | −6.87 |
| Costs 2 | ||||||||||||
| Vaccine Cost | ¥235.76 | ¥0.00 | ¥235.76 | ¥7.80 | ¥0.00 | ¥7.80 | ¥159.37 | ¥0.00 | ¥159.37 | ¥139.00 | ¥0.00 | ¥139.00 |
| Pneumococcal Bacteremia | ¥0.89 | ¥1.17 | −¥0.28 | ¥0.02 | ¥0.03 | −¥0.01 | ¥0.50 | ¥0.65 | −¥0.16 | ¥0.54 | ¥0.72 | −¥0.17 |
| Pneumococcal Meningitis | ¥1.82 | ¥2.71 | −¥0.89 | ¥0.05 | ¥0.07 | −¥0.03 | ¥0.99 | ¥1.49 | −¥0.50 | ¥1.23 | ¥1.82 | −¥0.59 |
| Pneumonia (Inpatient) | ¥1358.27 | ¥1473.49 | −¥115.21 | ¥34.69 | ¥38.19 | −¥3.50 | ¥763.06 | ¥834.15 | −¥71.09 | ¥844.59 | ¥918.43 | −¥73.84 |
| Pneumonia (Outpatient) | ¥82.22 | ¥83.02 | −¥0.80 | ¥2.20 | ¥2.23 | −¥0.03 | ¥47.23 | ¥47.77 | −¥0.54 | ¥51.01 | ¥51.49 | −¥0.48 |
| Otitis Media (Mild) | ¥29.69 | ¥30.00 | −¥0.32 | ¥0.85 | ¥0.86 | −¥0.01 | ¥16.96 | ¥17.17 | −¥0.21 | ¥18.94 | ¥19.13 | −¥0.19 |
| Otitis Media (Mod./Sev.) | ¥135.57 | ¥140.27 | −¥4.70 | ¥3.97 | ¥4.13 | −¥0.16 | ¥79.35 | ¥82.51 | −¥3.16 | ¥84.39 | ¥87.20 | −¥2.81 |
| Total Cost | ¥1844.21 | ¥1730.66 | ¥113.55 | ¥49.58 | ¥45.52 | ¥4.06 | ¥1067.45 | ¥983.74 | ¥83.71 | ¥1139.71 | ¥1078.79 | ¥60.92 |
| ICER | ¥11,693 | ¥15,132 | ¥15,422 | ¥8862 | ||||||||
| Cities | Vaccination Rate | Price per Dose | Service/Transplantation FEE/DOSE | Vaccination Doses | ICER | GDP per Capita | ICER/GDP | Cost-Effective? |
|---|---|---|---|---|---|---|---|---|
| Beijing | 70% | ¥698 | ¥25 | 4 | ¥4093 | ¥164,000(2019) | 0.025 | Yes |
| 3 | Dominant | ----- | Yes | |||||
| Shanghai | 70% | ¥698 | ¥5.5 | 4 | Dominant | ¥157,300 (2019) | ----- | Yes |
| 3 | Dominant | ----- | Yes | |||||
| Shenzhen | 70% | ¥698 | ¥25 | 4 | ¥1145 | ¥203,489(2019) | 0.006 | Yes |
| 3 | Dominant | ----- | Yes | |||||
| Chengdu | 70% | ¥698 | ¥30 | 4 | ¥11,693 | ¥103,386 (2019) | 0.113 | Yes |
| 3 | ¥5624 | 0.054 | Yes | |||||
| Karamay | 70% | ¥698 | ¥0 | 4 | ¥15,132 | ¥145,798 (2017) | 0.104 | Yes |
| 3 | ¥7870 | 0.054 | Yes | |||||
| Qingdao | 70% | ¥698 | ¥34 | 4 | ¥15,422 | ¥124,282 (2019) | 0.124 | Yes |
| 3 | ¥8082 | 0.065 | Yes | |||||
| Suzhou | 70% | ¥698 | ¥20 | 4 | ¥8862 | ¥174,129 (2018) | 0.051 | Yes |
| 3 | ¥3807 | 0.022 | Yes |
| TIER-1 Cities | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beijing | Shanghai | Shenzhen | ||||||||||
| VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | ||||
| Cases of Pneumococcal Disease 1 | ||||||||||||
| Pneumococcal Bacteremia | 1.16 | 1.18 | −0.03 | 1.59 | 1.61 | −0.02 | 0.64 | 0.65 | −0.01 | |||
| Pneumococcal Meningitis | 0.32 | 0.33 | −0.01 | 0.43 | 0.44 | −0.01 | 0.19 | 0.20 | 0.00 | |||
| Pneumonia (Inpatient) | 268.70 | 283.21 | −14.51 | 348.41 | 361.70 | −13.29 | 147.14 | 153.68 | −6.54 | |||
| Pneumonia (Outpatient) | 345.32 | 350.96 | −5.63 | 423.44 | 428.60 | −5.16 | 167.06 | 169.60 | −2.54 | |||
| Otitis Media (Mild) | 69.28 | 72.83 | −3.55 | 63.47 | 66.72 | −3.25 | 31.22 | 32.82 | −1.60 | |||
| Otitis Media (Mod./Sev.) | 19.82 | 22.13 | −2.31 | 18.16 | 20.28 | −2.12 | 8.93 | 9.97 | −1.04 | |||
| Total Cases | 704.61 | 730.64 | −26.03 | 855.50 | 879.35 | −23.85 | 355.19 | 366.92 | −11.73 | |||
| Total Deaths | 13.48 | 13.56 | −0.08 | 18.25 | 18.32 | −0.07 | 4.71 | 4.75 | −0.04 | |||
| Total QALYs Lost | 146.37 | 147.96 | −1.59 | 195.29 | 196.75 | −1.46 | 73.14 | 73.86 | −0.72 | |||
| Costs2 | ||||||||||||
| Vaccine Cost | ¥331.06 | ¥0.00 | ¥331.06 | ¥295.11 | ¥0.00 | ¥295.11 | ¥149.19 | ¥0.0 | ¥149.19 | |||
| Pneumococcal Bacteremia | ¥1.26 | ¥1.30 | ¥0.05 | ¥1.70 | ¥1.74 | −¥0.04 | ¥0.43 | ¥0.45 | −¥0.02 | |||
| Pneumococcal Meningitis | ¥1.15 | ¥1.16 | ¥0.00 | ¥1.55 | ¥1.55 | ¥0.00 | ¥0.37 | ¥0.37 | ¥0.00 | |||
| Pneumonia (Inpatient) | ¥3913.23 | ¥3979.43 | −¥66.20 | ¥5221.67 | ¥5282.32 | −¥60.65 | ¥1568.51 | ¥1598.34 | −¥29.83 | |||
| Pneumonia (Outpatient) | ¥140.62 | ¥141.93 | −¥1.31 | ¥179.26 | ¥180.46 | −¥1.20 | ¥59.07 | ¥59.66 | −¥0.59 | |||
| Otitis Media (Mild) | ¥46.40 | ¥46.75 | −¥0.35 | ¥58.79 | ¥59.10 | −¥0.32 | ¥20.94 | ¥21.10 | −¥0.16 | |||
| Otitis Media (Mod./Sev.) | ¥157.75 | ¥164.40 | −¥6.65 | ¥188.84 | ¥194.93 | −¥6.09 | ¥76.32 | ¥79.32 | −¥3.00 | |||
| Total Cost | ¥4591.48 | ¥4334.97 | ¥256.51 | ¥5946.91 | ¥5720.11 | ¥226.81 | ¥1874.84 | ¥1759.24 | ¥115.59 | |||
| ICER | ¥161,237 | ¥155,625 | ¥161,237 | |||||||||
| Other Cities | ||||||||||||
| Chengdu | Karamay | Qingdao | Suzhou | |||||||||
| VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | VACC. | NO VACC. | INCR. | |
| Cases of Pneumococcal Disease 1 | ||||||||||||
| Pneumococcal Bacteremia | 1.11 | 1.13 | −0.02 | 0.03 | 0.03 | 0.00 | 0.61 | 0.62 | −0.01 | 0.72 | 0.73 | −0.01 |
| Pneumococcal Meningitis | 0.31 | 0.32 | 0.00 | 0.01 | 0.01 | 0.00 | 0.17 | 0.17 | 0.00 | 0.20 | 0.21 | 0.00 |
| Pneumonia (Inpatient) | 256.49 | 266.76 | −6.54 | 7.19 | 7.54 | −0.35 | 145.25 | 152.15 | −6.90 | 162.24 | 168.37 | −6.13 |
| Pneumonia (Outpatient) | 304.27 | 308.25 | −2.54 | 8.63 | 8.77 | −0.14 | 176.60 | 179.28 | −2.68 | 190.24 | 192.62 | −2.38 |
| Otitis Media (Mild) | 49.00 | 51.51 | −1.60 | 1.69 | 1.78 | −0.09 | 32.94 | 34.63 | −1.69 | 29.29 | 30.79 | −1.50 |
| Otitis Media (Mod./Sev.) | 14.02 | 15.65 | −1.04 | 0.48 | 0.54 | −0.06 | 9.43 | 10.52 | −1.10 | 8.38 | 9.36 | −0.98 |
| Total Cases | 625.20 | 643.61 | −11.73 | 18.03 | 18.67 | −0.64 | 364.99 | 377.37 | −12.38 | 391.07 | 402.08 | −11.01 |
| Total Deaths | 11.79 | 11.84 | −0.04 | 0.28 | 0.28 | 0.00 | 6.48 | 6.51 | −0.04 | 7.44 | 7.47 | −0.03 |
| Total QALYs Lost | 128.11 | 129.24 | 0.72 | 3.26 | 3.30 | −0.04 | 69.79 | 70.55 | −0.76 | 84.99 | 85.66 | −0.67 |
| Costs 2 | ||||||||||||
| Vaccine Cost | ¥235.76 | ¥0.00 | ¥235.76 | ¥7.80 | ¥0.00 | ¥7.80 | ¥159.37 | ¥0.00 | ¥159.37 | ¥139.00 | ¥0.00 | ¥139.00 |
| Pneumococcal Bacteremia | ¥1.14 | ¥1.17 | −¥0.03 | ¥0.03 | ¥0.03 | ¥0.00 | ¥0.63 | ¥0.65 | −¥0.02 | ¥0.70 | ¥0.72 | −¥0.02 |
| Pneumococcal Meningitis | ¥2.61 | ¥2.71 | −¥0.10 | ¥0.07 | ¥0.07 | ¥0.00 | ¥1.42 | ¥1.49 | −¥0.07 | ¥1.76 | ¥1.82 | −¥0.06 |
| Pneumonia (Inpatient) | ¥1435.34 | ¥1473.49 | −¥38.14 | ¥36.88 | ¥38.19 | −¥1.32 | ¥808.51 | ¥834.15 | −¥25.65 | ¥895.63 | ¥918.43 | −¥22.80 |
| Pneumonia (Outpatient) | ¥82.22 | ¥83.02 | −¥0.80 | ¥2.20 | ¥2.23 | −¥0.03 | ¥47.23 | ¥47.77 | −¥0.54 | ¥51.01 | ¥51.49 | −¥0.48 |
| Otitis Media (Mild) | ¥29.69 | ¥30.00 | −¥0.32 | ¥0.85 | ¥0.86 | −¥0.01 | ¥16.96 | ¥17.17 | −¥0.21 | ¥18.94 | ¥19.13 | −¥0.19 |
| Otitis Media (Mod./Sev.) | ¥135.57 | ¥140.27 | −¥4.70 | ¥3.97 | ¥4.13 | −¥0.16 | ¥79.35 | ¥82.51 | −¥3.16 | ¥84.39 | ¥87.20 | −¥2.81 |
| Total Cost | ¥1922.32 | ¥1730.66 | ¥191.65 | ¥51.79 | ¥45.52 | ¥6.28 | ¥1113.46 | ¥983.74 | ¥129.72 | ¥1191.43 | ¥1078.79 | ¥112.64 |
| ICER | ¥170,345 | ¥161,710 | ¥171,496 | ¥167,466 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Wang, H.; Furnback, W.; Wang, B.C.M.; Zhu, S.; Dong, P. The Cost-Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine in Seven Chinese Cities. Vaccines 2021, 9, 1368. https://doi.org/10.3390/vaccines9111368
Li Y, Wang H, Furnback W, Wang BCM, Zhu S, Dong P. The Cost-Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine in Seven Chinese Cities. Vaccines. 2021; 9(11):1368. https://doi.org/10.3390/vaccines9111368
Chicago/Turabian StyleLi, Yan, Huaqing Wang, Wesley Furnback, Bruce C. M. Wang, Shuiqing Zhu, and Peng Dong. 2021. "The Cost-Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine in Seven Chinese Cities" Vaccines 9, no. 11: 1368. https://doi.org/10.3390/vaccines9111368
APA StyleLi, Y., Wang, H., Furnback, W., Wang, B. C. M., Zhu, S., & Dong, P. (2021). The Cost-Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine in Seven Chinese Cities. Vaccines, 9(11), 1368. https://doi.org/10.3390/vaccines9111368