Japanese Mothers’ Intention to HPV Vaccinate Their Daughters: How Has It Changed over Time Because of the Prolonged Suspension of the Governmental Recommendation?


 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Methods for the Fourth Internet Survey
2.2. Comparison with Our Previous Surveys.
2.3. Statistics
2.4. Ethical Statement
3. Results
3.1. Result of the Fourth Internet Survey
3.1.1. Study Targets and Participants’ Characteristics
3.1.2. Correlation between Question and the Intention of Mothers to Inoculate Daughter Under Current Circumstances
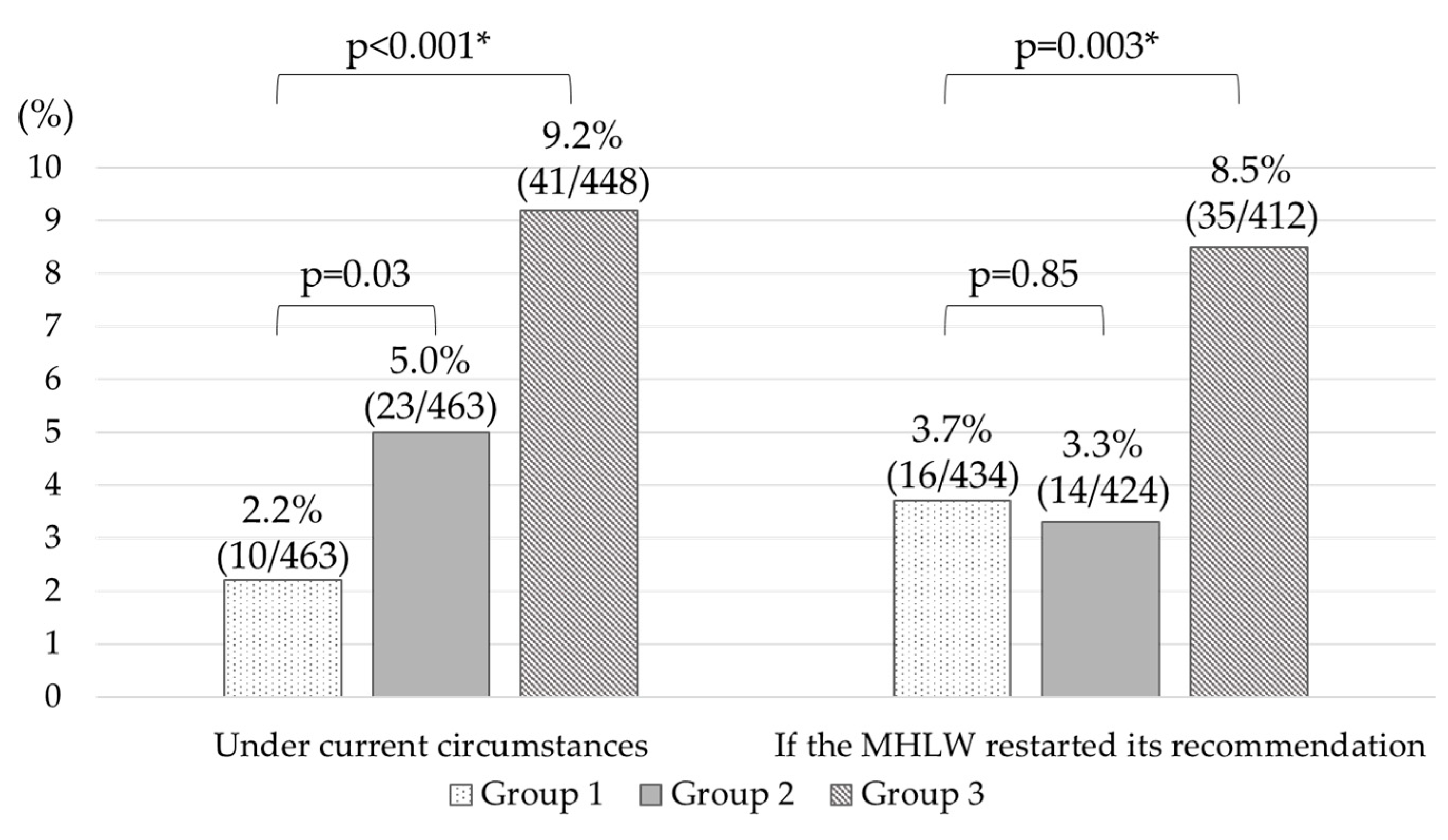
3.1.3. Verification of Leaflet Intervention Effect
3.1.4. Factors That Would Promote Inoculation
3.2. Comparison of Current Results with Those of Previous Surveys
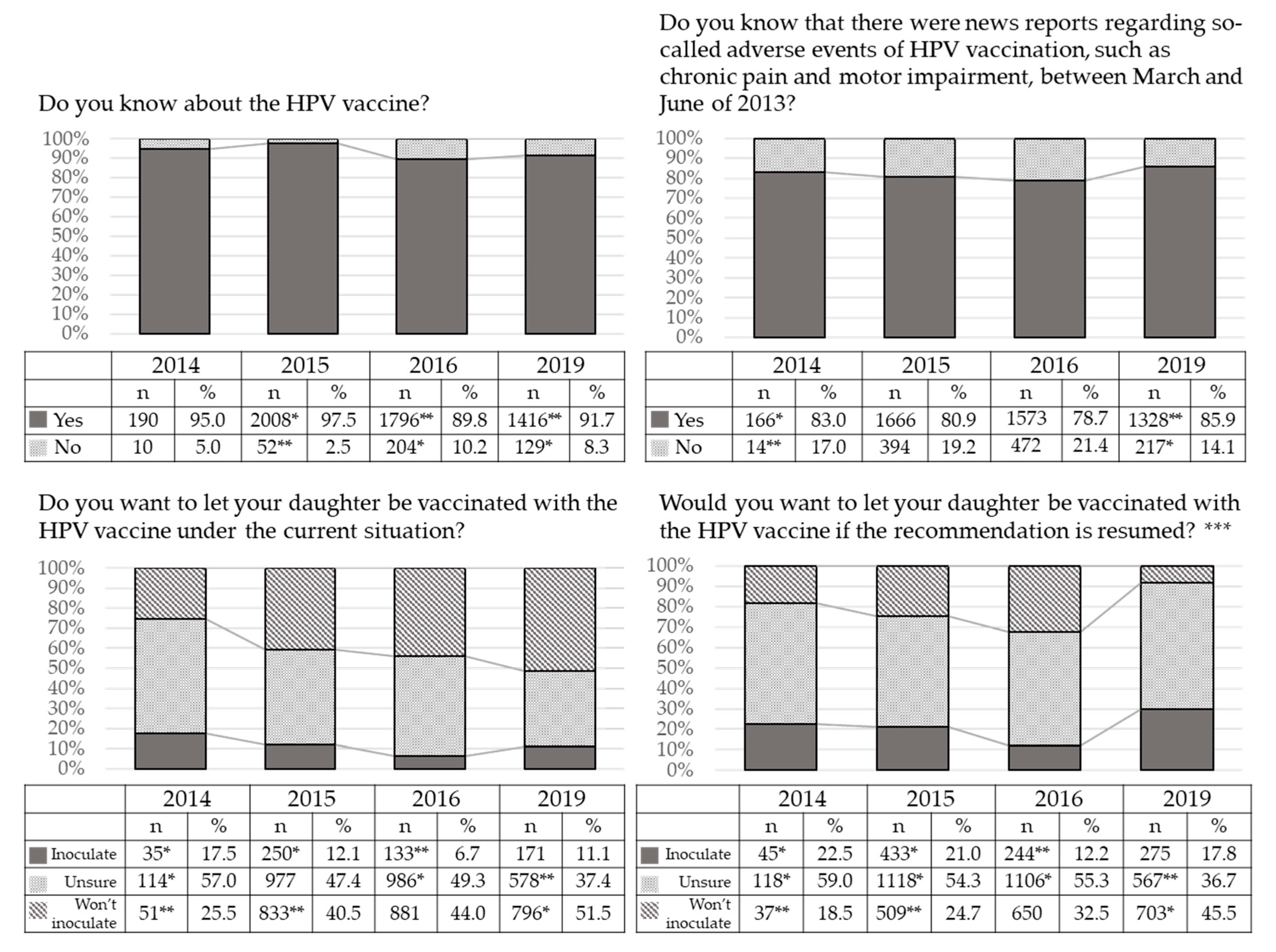
3.2.1. Changes in Response to Each Survey Question Over Time
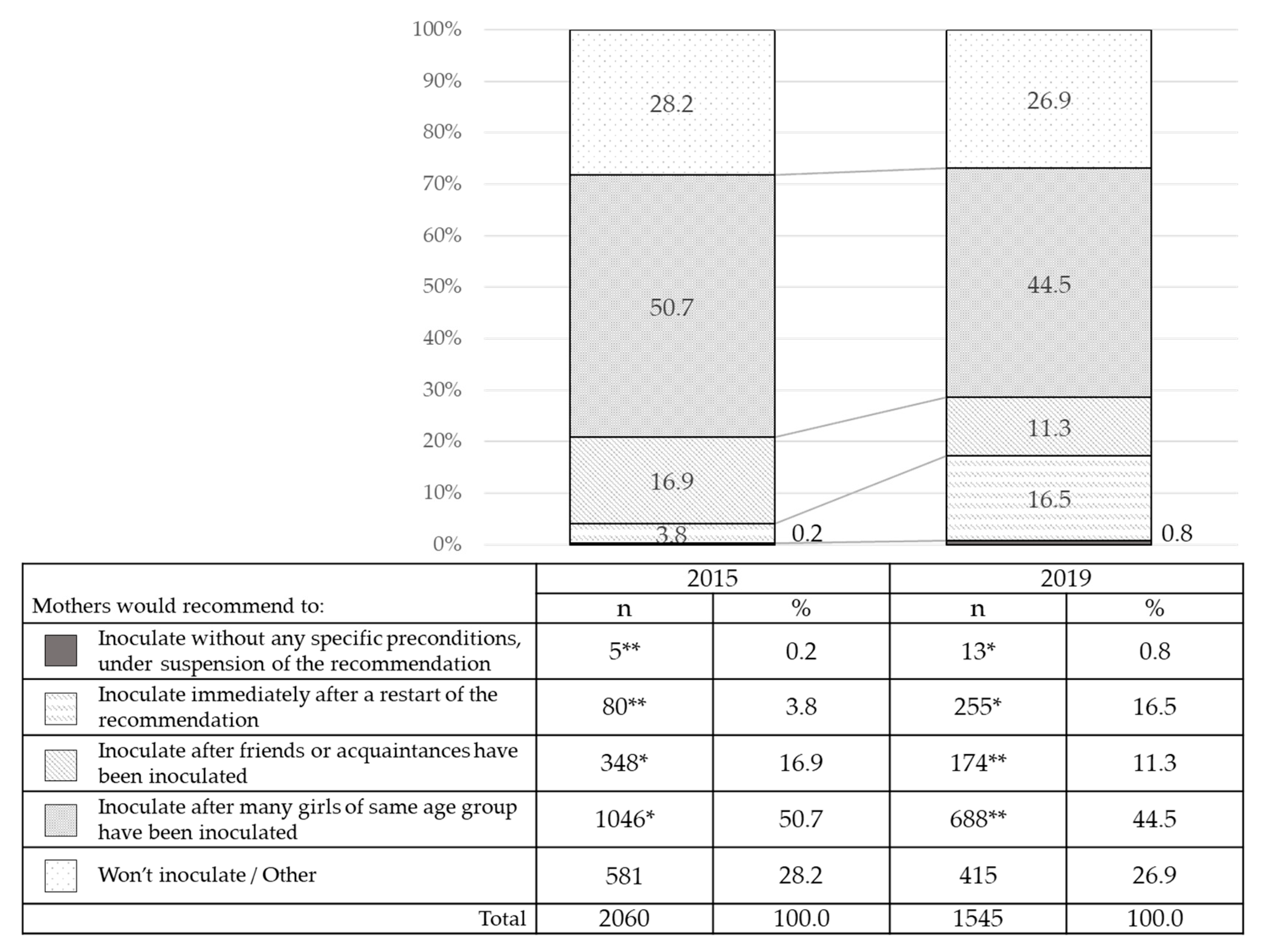
3.2.2. Changes over Time in the Preconditions Mothers Would Require Before Allowing Their Daughters’ HPV Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Health Topics, Cervical Cancer. Available online: https://www.who.int/health-topics/cervical-cancer#tab=tab_2 (accessed on 1 May 2020).
- Hall, M.T.; Simms, K.T.; Lew, J.B.; Smith, M.A.; Brotherton, J.M.; Saville, M.; Frazer, I.H.; Canfell, K. The projected timeframe until cervical cancer elimination in Australia: A modelling study. Lancet Public Health 2019, 4, e19–e27. [Google Scholar] [CrossRef]
- Sipp, D.; Frazer, I.H.; Rasko, J.E.J. No vacillation on HPV vaccination. Cell 2018, 172, 1163–1167. [Google Scholar] [CrossRef] [PubMed]
- Luostarinen, T.; Apter, D.; Dillner, J.; Eriksson, T.; Harjula, K.; Natunen, K.; Paavonen, J.; Pukkala, E.; Lehtinen, M. Vaccination protects against invasive HPV-associated cancers. Int. J. Cancer 2018, 142, 2186–2187. [Google Scholar] [CrossRef] [PubMed]
- Cancer Registry and Statistics. Cancer Information Service, National Cancer Center, Japan. Available online: http://ganjoho.jp/reg_stat/index.html (accessed on 1 May 2020).
- Yagi, A.; Ueda, Y.; Kakuda, M.; Tanaka, Y.; Ikeda, S.; Matsuzaki, S.; Kobayashi, E.; Morishima, T.; Miyashiro, I.; Fukui, K.; et al. Epidemiologic and clinical analysis of cervical cancer using data from the population-based osaka cancer registry. Cancer Res. 2019, 79, 1252–1259. [Google Scholar] [CrossRef] [PubMed]
- The Ministry of Health, Labour and Welfare. Available online: http://www.mhlw.go.jp/bunya/kenkou/kekkaku-kansenshou28/qa_hpv.html (accessed on 1 May 2020).
- Nakagawa, S.; Ueda, Y.; Yagi, A.; Ikeda, S.; Hiramatsu, K.; Kimura, T. Corrected human papillomavirus vaccination rates for each birth fiscal year in Japan. Cancer Sci. 2020, 111, 2156–2162. [Google Scholar] [CrossRef] [PubMed]
- Iwata, S.; Okada, K.; Kawana, K. Expert council on promotion of vaccination. Consensus statement from 17 relevant Japanese academic societies on the promotion of the human papillomavirus vaccine. Vaccine 2017, 35, 2291–2292. [Google Scholar] [CrossRef] [PubMed]
- OECD. OECD Health Statistics 2018. Available online: http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT (accessed on 1 May 2020).
- The Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions 2016. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa16/index.html (accessed on 1 May 2020).
- The Ministry of Health, Labour and Welfare. Arrangement of issues regarding the alleged adverse events. Available online: https://www.mhlw.go.jp/file/05-Shingikai-10601000-Daijinkanboukouseikagakuka-Kouseikagakuka/0000055692_2.pdf#search=%27%E5%8E%9A%E5%8A%B4%E7%9C%81+HPV+%E5%BA%83%E7%AF%84%E3%81%AA%E7%96%BC%E7%97%9B+%E9%81%8B%E5%8B%95%E6%A9%9F%E8%83%BD%E9%9A%9C%E5%AE%B3%27 (accessed on 15 August 2020).
- Egawa-Takata, T.; Ueda, Y.; Morimoto, A.; Yoshino, K.; Kimura, T.; Nishikawa, N.; Sekine, M.; Horikoshi, Y.; Takagi, T.; Enomoto, T. Survey of Japanese mothers of daughters eligible for human papillomavirus vaccination on attitudes about media reports of adverse events and the suspension of governmental recommendation for vaccination. J. Obstet. Gynaecol. Res. 2015, 41, 1965–1971. [Google Scholar] [CrossRef] [PubMed]
- Yagi, A.; Ueda, Y.; Egawa-Takata, T.; Tanaka, Y.; Morimoto, A.; Terai, Y.; Ohmichi, M.; Ichimura, T.; Sumi, T.; Murata, H. Development of an efficient strategy to improve HPV immunization coverage in Japan. BMC Public Health 2016, 16, 1013. [Google Scholar] [CrossRef] [PubMed]
- Yagi, A.; Ueda, Y.; Tanaka, Y.; Nakae, R.; Kakubari, R.; Morimoto, A.; Terai, Y.; Ohmichi, M.; Ichimura, T.; Sumi, T.; et al. Time-dependent changes of the intention of mothers in Japan to inoculate their daughters with the HPV vaccine after suspension of governmental recommendation. Hum. Vaccin. Immunother. 2018, 14, 2497–2502. [Google Scholar] [CrossRef] [PubMed]
- Statistics Bureau, Ministry of Internal Affairs and Communications. Available online: http://www.stat.go.jp/data/kokusei/2015/kekka.html (accessed on 1 May 2020).
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef]
- Cancer Registry and Statistics. Cancer Information Service, National Cancer Center, Japan. FY2016 Grant-in-Aid for Scientific Research (B) (General) Cancer Causes and Contributions to Japanese: Latest Estimates and Future Forecasts. Available online: https://ganjoho.jp/reg_stat/statistics/dl/index.html (accessed on 1 May 2020).
- Corcoran, B.; Clarke, A.; Barrett, T. Rapid response to HPV vaccination crisis in Ireland. Lancet 2018, 391, 2103. [Google Scholar] [CrossRef]
- Hansen, P.R.; Schmidtblaicher, M.; Brewer, N.T. Resilience of HPV vaccine uptake in Denmark: Decline and recovery. Vaccine 2020, 38, 1842–1848. [Google Scholar] [CrossRef] [PubMed]
- UNISEF Human Papillomavirus (HPV) Immunization Coverage Estimate. Available online: https://data.unicef.org/topic/child-health/immunization/ (accessed on 1 May 2020).
- Suzuki, S.; Hosono, A. No association between HPV vaccine and reported post-vaccination symptoms in Japanese young women: Results of the Nagoya study. Papillomavirus Res. 2018, 5, 96–103. [Google Scholar] [CrossRef] [PubMed]
- The Ministry of Health, Labour and Welfare. Available online: https://www.mhlw.go.jp/stf/shingi2/0000208910_00011.html (accessed on 1 May 2020).
- Nagase, Y.; Ueda, Y.; Abe, H.; Yagi, A.; Sawada, M.; Nakagawa, S.; Hiramatsu, K.; Egawa-Takata, T.; Matsuzaki, S.; Kobayashi, E.; et al. Changing attitudes in Japan toward HPV vaccination: A 5-year follow-up survey of obstetricians and gynecologists regarding their current opinions about the HPV vaccine. Hum. Vaccin. Immunother. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Simms, K.T.; Hanley, S.J.B.; Smith, M.A.; Keane, A.; Canfell, K. Impact of HPV vaccine hesitancy on cervical cancer in Japan: A modelling study. Lancet Public Health 2020, 5, e223–e234. [Google Scholar] [CrossRef]
- Ueda, Y.; Yagi, A.; Ikeda, S.; Enomoto, T.; Kimura, T. Beyond resumption of the Japanese Government’s recommendation of the HPV vaccine. Lancet Oncol. 2018, 19, 1563–1564. [Google Scholar] [CrossRef]
- Yagi, A.; Ueda, Y.; Egawa-Takata, T.; Tanaka, Y.; Nakae, R.; Morimoto, A.; Terai, Y.; Ohmichi, M.; Ichimura, T.; Sumi, T.; et al. Realistic fear of cervical cancer risk in Japan depending on birth year. Hum. Vaccin. Immunother. 2017, 13, 1700–1704. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Ueda, Y.; Egawa-Takata, T.; Yagi, A.; Yoshino, K.; Kimura, T. Outcomes for girls without HPV vaccination in Japan. Lancet Oncol. 2016, 17, 868–869. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group 1 | Group 2 | Group 3 | p-Value | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Age | |||||||||
| 30–39 | 87 | 16.9 | 92 | 17.9 | 88 | 17.1 | 0.95 | 267 | 17.3 |
| 40–49 | 373 | 72.4 | 364 | 70.7 | 365 | 70.9 | 1102 | 71.3 | |
| 50 or older | 55 | 10.7 | 59 | 11.4 | 62 | 12.0 | 176 | 11.4 | |
| Household income (Yen) | |||||||||
| Less than 4 million | 95 | 18.5 | 110 | 21.4 | 94 | 18.3 | 0.57 | 299 | 19.4 |
| 4–6 million | 114 | 22.1 | 121 | 23.5 | 124 | 24.1 | 359 | 23.0 | |
| 6–8 million | 94 | 18.3 | 80 | 15.5 | 79 | 15.3 | 253 | 16.4 | |
| Over 8 million | 84 | 16.3 | 75 | 14.6 | 77 | 15.0 | 236 | 15.3 | |
| Don’t know | 45 | 8.7 | 5 | 9.9 | 65 | 12.6 | 161 | 10.5 | |
| Did not reply to question | 83 | 16.1 | 78 | 15.1 | 76 | 14.7 | 237 | 15.4 | |
| Work status | |||||||||
| Full-time job | 97 | 18.9 | 115 | 22.3 | 100 | 19.4 | 0.64 | 312 | 20.2 |
| Housewife | 185 | 35.9 | 193 | 37.5 | 196 | 38.0 | 574 | 37.1 | |
| Part-time job | 220 | 42.7 | 197 | 38.3 | 210 | 40.8 | 627 | 40.6 | |
| Other | 13 | 2.5 | 10 | 1.9 | 9 | 1.8 | 32 | 2.1 | |
| Education level | |||||||||
| Junior High School/High School | 172 | 33.4 | 192 | 37.3 | 162 | 31.5 | 0.39 | 526 | 34.0 |
| Vocational School/Junior College | 216 | 41.9 | 201 | 39.0 | 223 | 43.3 | 640 | 41.0 | |
| University/Graduate school | 127 | 24.7 | 122 | 23.7 | 130 | 25.2 | 379 | 25.0 | |
| Total | 515 | 33.3 | 515 | 33.3 | 515 | 33.3 | 1545 | 100.0 | |
| Inoculate | Unsure | Won’t inoculate | Total | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Do you know that cervical cancer more often affects women in their 20s and 30s? | ||||||||
| Yes | 147 | 86.0 | 450 ** | 77.9 | 679 * | 85.3 | 1,276 | 82.6 |
| No | 24 | 14.0 | 128 * | 37.4 | 117 ** | 14.7 | 269 | 17.4 |
| Do you know about the HPV vaccine? | ||||||||
| Yes | 155 | 90.6 | 508 ** | 87.9 | 753 * | 94.6 | 1416 | 91.7 |
| No | 16 | 9.4 | 70 * | 12.1 | 43 ** | 5.4 | 129 | 8.3 |
| Do you know the HPV vaccine can prevent cervical cancer? | ||||||||
| Yes | 154 | 90.1 | 491 ** | 85.09 | 729 * | 91.6 | 1,374 | 88.9 |
| No | 17 | 9.9 | 87 * | 15.0 | 67 ** | 8.4 | 171 | 11.1 |
| Do you know that there were news reports regarding so-called adverse events of HPV vaccine, such as chronic pain and motor impairment, between March and June in 2013? | ||||||||
| Yes | 120 ** | 91.0 | 464 ** | 80.3 | 774 * | 93.5 | 1,328 | 86.0 |
| No | 51 * | 29.8 | 114 * | 19.7 | 52 ** | 6.5 | 217 | 14.0 |
| Have you ever had cervical cancer screening? | ||||||||
| Yes | 151 | 88.3 | 481 | 83.2 | 685 | 86.1 | 1,317 | 85.2 |
| No | 20 | 11.7 | 97 | 16.8 | 111 | 13.9 | 228 | 14.8 |
| Have you ever received influenza vaccine? | ||||||||
| Yes | 151 | 88.3 | 481 | 83.2 | 685 | 86.1 | 1,317 | 85.2 |
| No | 20 | 11.7 | 97 | 16.8 | 111 | 13.9 | 228 | 14.8 |
| Total | 171 | 11.1 | 578 | 37.4 | 796 | 51.5 | 1545 | 100.0 |
| (MHLW Restarts Recommendation) | Recommendation by Family Doctor | Recommendation by School | Recommendation by Local Government | Inoculation of a Daughter’s Friend | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| Inoculate | (275/1545) | (17.8) | 582/1545 | 37.7 * | 445/1545 | 28.8 | 410/1545 | 26.5 | 478/1545 | 30.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yagi, A.; Ueda, Y.; Masuda, T.; Ikeda, S.; Miyatake, T.; Nakagawa, S.; Hirai, K.; Nakayama, T.; Miyagi, E.; Enomoto, T.; et al. Japanese Mothers’ Intention to HPV Vaccinate Their Daughters: How Has It Changed over Time Because of the Prolonged Suspension of the Governmental Recommendation? Vaccines 2020, 8, 502. https://doi.org/10.3390/vaccines8030502
Yagi A, Ueda Y, Masuda T, Ikeda S, Miyatake T, Nakagawa S, Hirai K, Nakayama T, Miyagi E, Enomoto T, et al. Japanese Mothers’ Intention to HPV Vaccinate Their Daughters: How Has It Changed over Time Because of the Prolonged Suspension of the Governmental Recommendation? Vaccines. 2020; 8(3):502. https://doi.org/10.3390/vaccines8030502
Chicago/Turabian StyleYagi, Asami, Yutaka Ueda, Tatsuo Masuda, Sayaka Ikeda, Takashi Miyatake, Satoshi Nakagawa, Kei Hirai, Tomio Nakayama, Etsuko Miyagi, Takayuki Enomoto, and et al. 2020. "Japanese Mothers’ Intention to HPV Vaccinate Their Daughters: How Has It Changed over Time Because of the Prolonged Suspension of the Governmental Recommendation?" Vaccines 8, no. 3: 502. https://doi.org/10.3390/vaccines8030502
APA StyleYagi, A., Ueda, Y., Masuda, T., Ikeda, S., Miyatake, T., Nakagawa, S., Hirai, K., Nakayama, T., Miyagi, E., Enomoto, T., & Kimura, T. (2020). Japanese Mothers’ Intention to HPV Vaccinate Their Daughters: How Has It Changed over Time Because of the Prolonged Suspension of the Governmental Recommendation? Vaccines, 8(3), 502. https://doi.org/10.3390/vaccines8030502