Determinants of Vaccination Uptake in Risk Populations: A Comprehensive Literature Review

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
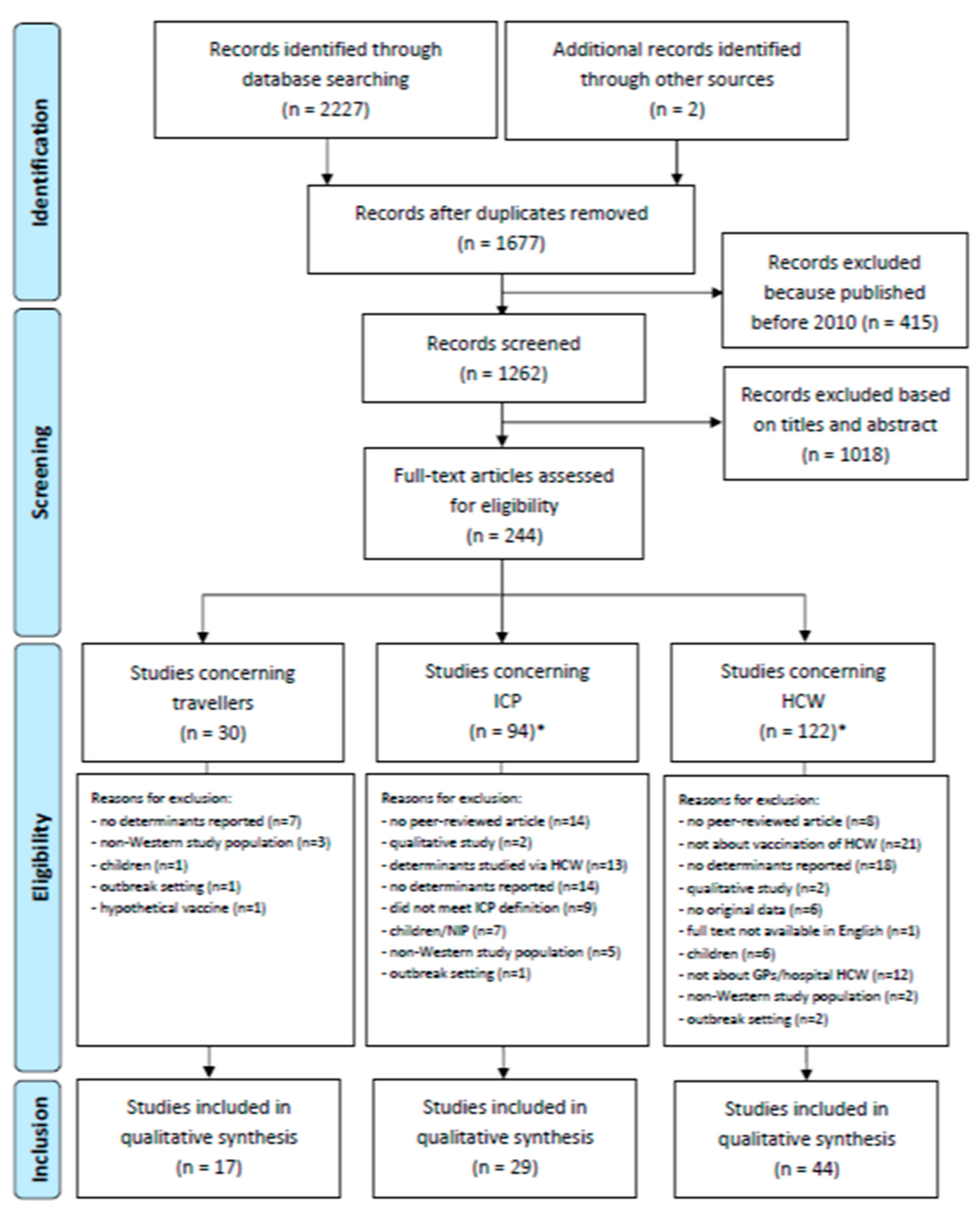
2.2. Study Selection
2.3. Data Extraction
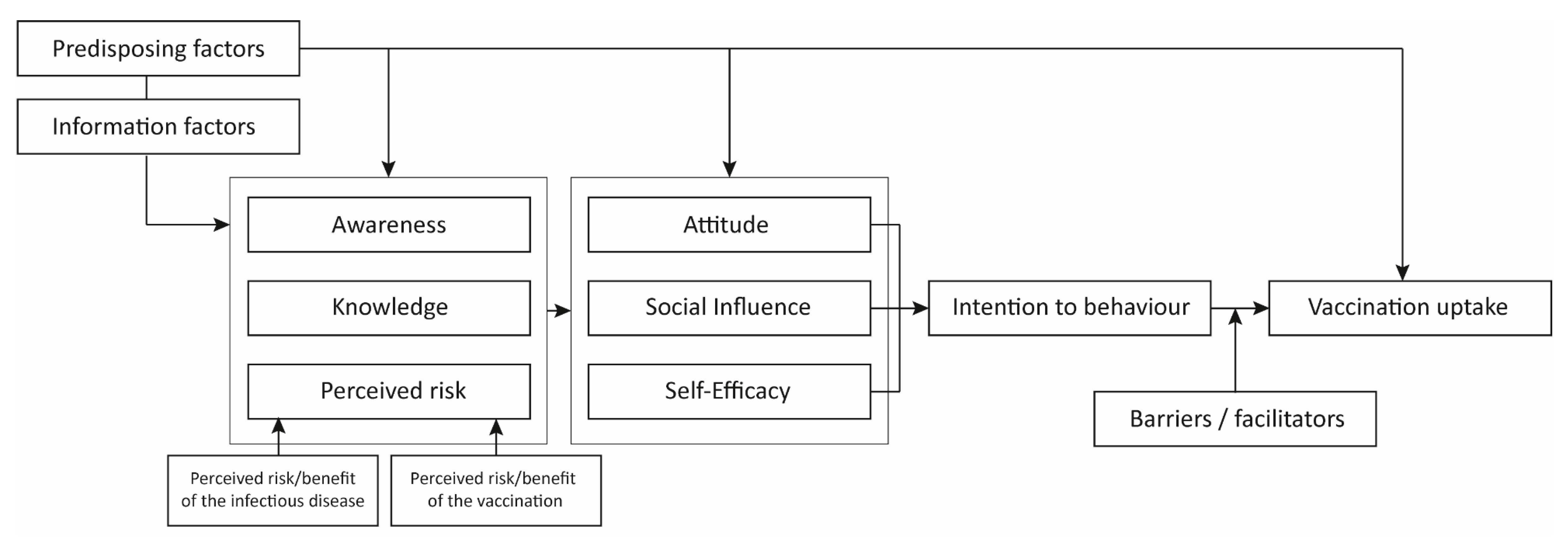
2.4. Labelling of Determinants
3. Results
3.1. Vaccination Uptake Among Travellers
3.1.1. Predisposing Factors
3.1.2. Information Factors
3.1.3. Cognitive Determinants
3.1.4. Barriers and Facilitators
3.2. Vaccination Uptake among Immunocompromised Patients
3.2.1. Predisposing Factors
3.2.2. Information Factors
3.2.3. Cognitive Determinants
3.2.4. Barriers and Facilitators
3.3. Vaccination Uptake among Healthcare Workers
3.3.1. Predisposing Factors
3.3.2. Information Factors
3.3.3. Cognitive Determinants
3.3.4. Barriers and Facilitators
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Poland, G.A.; Whitaker, J.A.; Poland, C.M.; Ovsyannikova, I.G.; Kennedy, R.B. Vaccinology in the third millennium: Scientific and social challenges. Curr. Opin. Virol. 2016, 17, 116–125. [Google Scholar] [CrossRef]
- WHO. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/feature-stories/ten-threats-to-global-health-in-2019 (accessed on 19 May 2020).
- Phadke, V.K.; Bednarczyk, R.A.; Salmon, D.A.; Omer, S.B. Association between vaccine refusal and vaccine-preventable diseases in the united states: A review of measles and pertussis. JAMA 2016, 315, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- WHO. New Measles Surveillance Data for 2019. Available online: https://www.who.int/immunization/newsroom/measles-data-2019/en/ (accessed on 6 February 2020).
- Kohn, M.; Schaffner, W. Vaccinating adults with chronic disease: We can do better. Vaccine 2017, 35, 3431–3432. [Google Scholar] [CrossRef] [PubMed]
- WHO. Life Expectancy and Healthy Life Expectancy. Available online: https://apps.who.int/gho/data/view.main.SDG2016LEXREGv?lang=en (accessed on 23 June 2020).
- Harpaz, R.; Dahl, R.; Dooling, K. The prevalence of immunocompromised adults: United States, 2013. Open Forum Infect. Dis. 2016, 3, 1439. [Google Scholar] [CrossRef]
- UNWTO. International Tourism Highlights. Available online: https://www.e-unwto.org/doi/pdf/10.18111/9789284421152 (accessed on 23 June 2020).
- Gautret, P.; Botelho-Nevers, E.; Brouqui, P.; Parola, P. The spread of vaccine-preventable diseases by international travellers: A public-health concern. Clin. Microbiol. Infect. 2012, 18 (Suppl. 5), 77–84. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Haviari, S.; Bénet, T.; Saadatian-Elahi, M.; André, P.; Loulergue, P.; Vanhems, P. Vaccination of healthcare workers: A review. Hum. Vaccines Immunother. 2015, 11, 2522–2537. [Google Scholar] [CrossRef] [PubMed]
- Angus, K.; Carnis, G.; Purves, R.; Bryce, S.; MacDonald, L.; Gordon, R. Systematic Literature Review to Examine the Evidence for the Effectiveness of Interventions that Use Theories and Models of Behaviour Change: Towards the Prevention and Control of Communicable Diseases; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2013. [Google Scholar]
- Knops-Dullens, T.; de Vries, N.; de Vries, H. Reasons for non-attendance in cervical cancer screening programmes: An application of the integrated model for behavioural change. Eur. J. Cancer Prev. 2007, 16, 436–445. [Google Scholar] [CrossRef]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (axis). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of Planned Behavior In Organizational Behavior and Human Decision Processes; Academic Press, Inc.: Cambridge, MA, USA, 1991; Volume 50, pp. 179–211. [Google Scholar]
- Bandura, A. Social Cognitive Theory. Available online: https://www.sciencedirect.com/topics/immunology-and-microbiology/social-cognitive-theory (accessed on 31 December 2019).
- Balaban, V.; Stauffer, W.; Hammad, A.; Afgarshe, M.; Abd-Alla, M.; Ahmed, Q.; Memish, Z.; Saba, J.; Harton, E.; Palumbo, G.; et al. Predictors of protective behaviors among american travelers to the 2009 hajj. J. Epidemiol. Global Health 2013, 3, 187–196. [Google Scholar] [CrossRef]
- Barasheed, O.; Rashid, H.; Heron, L.; Ridda, I.; Haworth, E.; Nguyen-Van-Tam, J.; Dwyer, D.E.; Booy, R. Influenza vaccination among australian hajj pilgrims: Uptake, attitudes, and barriers. J. Travel Med. 2014, 21, 384–390. [Google Scholar] [CrossRef]
- Duffy, M.R.; Reed, C.; Edelson, P.J.; Blumensaadt, S.; Crocker, K.; Griggs, A.; Biggerstaff, B.J.; Delorey, M.J.; Hayes, E.B.; Fischer, M. A survey of us travelers to Asia to assess compliance with recommendations for the use of japanese encephalitis vaccine. J. Travel Med. 2013, 20, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Frew, G.; McGeorge, E.; Grant, S.; de Wildt, G. Hepatitis b: A cross-sectional survey of knowledge, attitudes and practices amongst backpackers in thailand. Travel Med. Infect. Dis 2017, 15, 57–62. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Goodman, A.L.; Masuet-Aumatell, C.; Halbert, J.; Zuckerman, J.N. Awareness of meningococcal disease among travelers from the united kingdom to the meningitis belt in africa. Am. J. Trop. Med. Hyg. 2014, 91, 281–286. [Google Scholar] [CrossRef]
- Herbinger, K.H.; Nothdurft, H.D.; Prymula, R. Online survey: Knowledge about risks, prevention and consequences of infections with hbv among travellers from four european countries. Curr. Med. Res. Opin. 2011, 27, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Heywood, A.E.; Nothdurft, H.; Tessier, D.; Moodley, M.; Rombo, L.; Marano, C.; De Moerlooze, L. Pre-travel advice, attitudes and hepatitis a and b vaccination rates among travellers from seven countries†. J. Travel Med. 2016, 24, taw069. [Google Scholar] [CrossRef][Green Version]
- Igreja, R.; Barros, K.; Teodósio, R. Attitudes on vaccination among portuguese travelers and brazilian migrants: A pilot study in portugal. Acta Med. Saliniana 2019, 49, 1–3. [Google Scholar]
- Lammert, S.M.; Rao, S.R.; Jentes, E.S.; Fairley, J.K.; Erskine, S.; Walker, A.T.; Hagmann, S.H.; Sotir, M.J.; Ryan, E.T.; LaRocque, R.C. Refusal of recommended travel-related vaccines among U.S. International travellers in global travepinet. J. Travel Med. 2016, 24, taw075. [Google Scholar] [CrossRef]
- Paudel, P.; Raina, C.; Zwar, N.; Seale, H.; Worth, H.; Sheikh, M.; Heywood, A.E. Risk activities and pre-travel health seeking practices of notified cases of imported infectious diseases in Australia. J. Travel Med. 2017, 24, tax044. [Google Scholar] [CrossRef]
- Pavli, A.; Katerelos, P.; Maltezou, H.C. Meningococcal disease awareness and meningoccocal vaccination among Greek students planning to travel abroad. Int. J. Adolesc. Med. Health 2019, 31. [Google Scholar] [CrossRef]
- Pfeil, A.; Mütsch, M.; Hatz, C.; Szucs, T.D. A cross-sectional survey to evaluate knowledge, attitudes and practices (kap) regarding seasonal influenza vaccination among european travellers to resource-limited destinations. BMC Public Health 2010, 10, 402. [Google Scholar] [CrossRef]
- Selcuk, E.B.; Kayabas, U.; Binbasioglu, H.; Otlu, B.; Bayindir, Y.; Bozdogan, B.; Karatas, M. Travel health attitudes among turkish business travellers to african countries. Travel Med. Infect. Dis 2016, 14, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.M.; Njeru, J.W.; Jacobson, D.J.; Wilson, P.M.; Chun, F.; Marcelin, J.R.; Springer, D.J.; Wieland, M.L.; Sia, I.G. Pre-travel health care utilization among travelers who visit friends and relatives. Int. J. Travel. Med. Global Health 2017, 5, 53–59. [Google Scholar] [CrossRef][Green Version]
- Tashani, M.; Alfelali, M.; Azeem, M.I.; Fatema, F.N.; Barasheed, O.; Alqahtani, A.S.; Tekin, H.; Rashid, H.; Booy, R. Barriers of vaccinations against serious bacterial infections among australian hajj pilgrims. Postgrad. Med. 2016, 128, 541–547. [Google Scholar] [CrossRef]
- Wiemken, T.L.; Carrico, R.M.; Kelley, R.R.; Binford, L.E.; Peyrani, P.; Ford, K.D.; Welch, V.; Ramirez, J.A. Understanding why low-risk patients accept vaccines: A socio-behavioral approach. BMC Res. Notes 2015, 8, 813. [Google Scholar] [CrossRef] [PubMed]
- Yanni, E.A.; Marano, N.; Han, P.; Edelson, P.J.; Blumensaadt, S.; Becker, M.; Dwyer, S.; Crocker, K.; Daley, T.; Davis, X.; et al. Knowledge, attitudes, and practices of us travelers to asia regarding seasonal influenza and h5n1 avian influenza prevention measures. J. Travel Med. 2010, 17, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Akin, S.; Dizdar, O.; Ozisik, L.; Tanriover, M.D.; Kamisli, S.; Erman, M.; Hayran, M. Vaccination attitudes among patients with cancer receiving chemotherapy. UHOD Uluslar. Hematol. Onkol. Derg. 2016, 26, 167–172. [Google Scholar] [CrossRef]
- Althoff, K.N.; Anastos, K.; Nelson, K.E.; Celentano, D.D.; Sharp, G.B.; Greenblatt, R.M.; French, A.L.; Diamond, D.J.; Holman, S.; Young, M.; et al. Predictors of reported influenza vaccination in hiv-infected women in the united states, 2006–2007 and 2007–2008 seasons. Prev. Med. 2010, 50, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Battistella, C.; Quattrin, R.; Celotto, D.; d’Angelo, M.; Fabbro, E.; Brusaferro, S.; Agodi, A.; Astengo, M.; Baldo, V.; Baldovin, T.; et al. Factors predicting influenza vaccination adherence among patients in dialysis: An italian survey. Hum. Vaccines Immunother. 2019, 15, 2434–2439. [Google Scholar] [CrossRef]
- Chehab, G.; Richter, J.G.; Brinks, R.; Fischer-Betz, R.; Winkler-Rohlfing, B.; Schneider, M. Vaccination coverage in systemic lupus erythematosus-a cross-sectional analysis of the german long-term study (lula cohort). Rheumatology 2018, 57, 1439–1447. [Google Scholar] [CrossRef]
- Chin-Yee, B.H.; Monkman, K.; Hussain, Z.; Minuk, L.A. Attitudes toward vaccination for pandemic h1n1 and seasonal influenza in patients with hematologic malignancies. J. Supportive Oncol. 2011, 9, 156–160. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Fresard, A.; Lucht, F.; Botelho-Nevers, E. Vaccine coverage in plwh: Disparities and potential impact of vaccine hesitancy. Hum. Vaccines Immunother. 2019, 15, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Haroon, M.; Adeeb, F.; Eltahir, A.; Harney, S. The uptake of influenza and pneumococcal vaccination among immunocompromised patients attending rheumatology outpatient clinics. Jt. Bone Spine 2011, 78, 374–377. [Google Scholar] [CrossRef] [PubMed]
- Harrison, N.; Poeppl, W.; Herkner, H.; Tillhof, K.D.; Grabmeier-Pfistershammer, K.; Rieger, A.; Forstner, C.; Burgmann, H.; Lagler, H. Predictors for and coverage of influenza vaccination among HIV-positive patients: A cross-sectional survey. HIV Med. 2017, 18, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Harrison, N.; Poeppl, W.; Miksch, M.; Machold, K.; Kiener, H.; Aletaha, D.; Smolen, J.S.; Forstner, C.; Burgmann, H.; Lagler, H. Predictors for influenza vaccine acceptance among patients with inflammatory rheumatic diseases. Vaccine 2018, 36, 4875–4879. [Google Scholar] [CrossRef]
- Lachenal, F.; Sebban, C.; Duruisseaux, M.; Biron, P.; Blay, J.Y.; Ghesquières, H. Influenza vaccination in patients with haematologic malignancies: Analysis of practices in 200 patients in a single center. Bull. Cancer 2010, 97, E33–E36. [Google Scholar] [CrossRef]
- Loubet, P.; Kernéis, S.; Groh, M.; Loulergue, P.; Blanche, P.; Verger, P.; Launay, O. Attitude, knowledge and factors associated with influenza and pneumococcal vaccine uptake in a large cohort of patients with secondary immune deficiency. Vaccine 2015, 33, 3703–3708. [Google Scholar] [CrossRef]
- Loubet, P.; Verger, P.; Abitbol, V.; Peyrin-Biroulet, L.; Launay, O. Pneumococcal and influenza vaccine uptake in adults with inflammatory bowel disease in france: Results from a web-based study. Dig. Liver Dis. 2018, 50, 563–567. [Google Scholar] [CrossRef]
- Malhi, G.; Rumman, A.; Thanabalan, R.; Croitoru, K.; Silverberg, M.S.; Hillary Steinhart, A.; Nguyen, G.C. Vaccination in inflammatory bowel disease patients: Attitudes, knowledge, and uptake. J. Crohn’s Colitis 2015, 9, 439–444. [Google Scholar] [CrossRef]
- Miller, P.D.E.; Forster, A.S.; De Silva, T.I.; Leonard, H.; Anthias, C.; Mayhew, M.; Klammer, M.; Paskar, S.; Hurst, E.; Peggs, K.; et al. Sociodemographic and psychological determinants of influenza vaccine intention among recipients of autologous and allogeneic haematopoietic stem cell transplant: A cross-sectional survey of uk transplant recipients using a modified health belief model. BMJ Open 2018, 8, e021222. [Google Scholar] [CrossRef]
- Mouthon, L.; Mestre, C.; Bérezné, A.; Poiraudeau, S.; Marchand, C.; Guilpain, P.; Guillevin, L.; Launay, O. Low influenza vaccination rate among patients with systemic sclerosis. Rheumatology 2010, 49, 600–606. [Google Scholar] [CrossRef][Green Version]
- Narula, N.; Dhillon, A.S.; Chauhan, U.; Marshall, J.K. An audit of influenza vaccination status in adults with inflammatory bowel disease. Can. J. Gastroenterol. 2012, 26, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.T.T.; Lindegaard, H.; Hendricks, O.; Friis-Møller, N. Factors associated with influenza and pneumococcal vaccine uptake among rheumatoid arthritis patients in denmark invited to participate in a pneumococcal vaccine trial (immunovax_ra). Scand. J. Rheumatol. 2017, 46, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Poeppl, W.; Lagler, H.; Raderer, M.; Sperr, W.R.; Zielinski, C.; Herkner, H.; Burgmann, H. Influenza vaccination perception and coverage among patients with malignant disease. Vaccine 2015, 33, 1682–1687. [Google Scholar] [CrossRef] [PubMed]
- Price, S.A.; Podczervinski, S.; MacLeod, K.; Helbert, L.; Pergam, S.A. Understanding influenza vaccination rates and reasons for refusal in caregivers and household contacts of cancer patients. Am. J. Infect. Control. 2019, 47, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Restivo, V.; Vizzini, G.; Mularoni, A.; Di Benedetto, C.; Gioè, S.M.; Vitale, F. Determinants of influenza vaccination among solid organ transplant recipients attending sicilian reference center. Hum. Vaccines Immunother. 2017, 13, 346–350. [Google Scholar] [CrossRef]
- Ruiz-Cuesta, P.; González-Alayón, C.; Jurado-García, J.; Iglesias-Flores, E.M.; Barranco-Quintana, J.L.; García-García, L.; Salgueiro-Rodríguez, I.M.; Benitez-Cantero, J.M.; García-Sánchez, V. Adherence to a predefined vaccination program in patients with inflammatory bowel disease. Gastroenterol. Hepatol. 2016, 39, 385–392. [Google Scholar] [CrossRef]
- Sadlier, M.; Sadlier, C.; Alani, A.; Ahmad, K.; Bergin, C.; Ramsay, B. Poor adherence to vaccination guidelines in dermatology patients on immunosuppressive therapies: An issue that needs addressing. Br. J. Dermatol. 2015, 173, 288–289. [Google Scholar] [CrossRef]
- Sandler, D.S.; Ruderman, E.M.; Brown, T.; Lee, J.Y.; Mixon, A.; Liss, D.T.; Baker, D.W. Understanding vaccination rates and attitudes among patients with rheumatoid arthritis. Am. J. Manag. Care 2016, 22, 161–167. [Google Scholar]
- Savage, J.; Muller, F.; Ormerod, A.D. Awareness and uptake of recommended vaccines among immunosuppressed patients. J. R. Coll. Phys. Edinb. 2011, 41, 202–205. [Google Scholar] [CrossRef]
- Struijk, G.H.; Lammers, A.J.J.; Brinkman, R.J.; Lombarts, M.J.M.H.; van Vugt, M.; van der Pant, K.A.M.I.; ten Berge, I.J.M.; Bemelman, F.J. Immunization after renal transplantation: Current clinical practice. Transplant. Infect. Dis. 2015, 17, 192–200. [Google Scholar] [CrossRef]
- Teich, N.; Klugmann, T.; Tiedemann, A.; Holler, B.; Mössner, J.; Liebetrau, A.; Schiefke, I. Vaccination coverage in immunosuppressed patients: Results of a regional health services research study. Dtsch. Arztebl. Int. 2011, 108, 105–111. [Google Scholar] [PubMed]
- Urun, Y.; Akbulut, H.; Demirkazik, A.; Cay Senler, F.; Utkan, G.; Onur, H.; Icli, F. Perception about influenza and pneumococcal vaccines and vaccination coverage among patients with malignancies and their family members. J. Balk. Union Oncol. 2013, 18, 511–515. [Google Scholar]
- Waszczuk, K.; Waszczuk, E.; Szenborn, L. Can we better protect patients with inflammatory bowel disease against infections—Patient attitude and personal immunization knowledge. Acta Gastro Enterol. Belg. 2018, 81, 257–261. [Google Scholar]
- Wilckens, V.; Kannengiesser, K.; Hoxhold, K.; Frenkel, C.; Kucharzik, T.; Maaser, C. The immunization status of patients with ibd is alarmingly poor before the introduction of specific guidelines. Scand. J. Gastroenterol. 2011, 46, 855–861. [Google Scholar] [CrossRef]
- Akan, H.; Yavuz, E.; Yayla, M.E.; Külbay, H.; Kaspar, E.; Zahmacioğlu, O.; Badur, S. Factors affecting uptake of influenza vaccination among family physicians. Vaccine 2016, 34, 1712–1718. [Google Scholar] [CrossRef]
- Asma, S.; Akan, H.; Uysal, Y.; Poçan, A.G.; Sucakli, M.H.; Yengil, E.; Gereklioğlu, Ç.; Korur, A.; Başhan, İ.; Erdogan, A.F.; et al. Factors effecting influenza vaccination uptake among health care workers: A multi-center cross-sectional study. BMC Infect. Dis. 2016, 16, 192. [Google Scholar] [CrossRef]
- Boey, L.; Bral, C.; Roelants, M.; De Schryver, A.; Godderis, L.; Hoppenbrouwers, K.; Vandermeulen, C. Attitudes, believes, determinants and organisational barriers behind the low seasonal influenza vaccination uptake in healthcare workers—A cross-sectional survey. Vaccine 2018, 36, 3351–3358. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Santomauro, F.; Porchia, B.R.; Niccolai, G.; Pellegrino, E.; Bonanni, P.; Lorini, C. Beliefs and opinions of health care workers and students regarding influenza and influenza vaccination in tuscany, central italy. Vaccines 2015, 3, 137–147. [Google Scholar] [CrossRef]
- Castilla, J.; Martínez-Baz, I.; Godoy, P.; Toledo, D.; Astray, J.; García, S.; Mayoral, J.M.; Martín, V.; González-Candelas, F.; Guevara, M.; et al. Trends in influenza vaccine coverage among primary healthcare workers in spain, 2008–2011. Prev Med. 2013, 57, 206–211. [Google Scholar] [CrossRef]
- Çiftci, F.; Şen, E.; Demir, N.; Çiftci, O.; Erol, S.; Kayacan, O. Beliefs, attitudes, and activities of healthcare personnel about influenza and pneumococcal vaccines. Hum. Vaccines Immunother. 2018, 14, 111–117. [Google Scholar] [CrossRef]
- Costantino, C.; Ledda, C.; Genovese, C.; Contrino, E.; Vitale, E.; Maida, C.M.; Squeri, R.; Vitale, F.; Rapisarda, V. Immunization status against measles of health-care workers operating at three sicilian university hospitals: An observational study. Vaccines 2019, 7, 175. [Google Scholar] [CrossRef] [PubMed]
- Dedoukou, X.; Nikolopoulos, G.; Maragos, A.; Giannoulidou, S.; Maltezou, H.C. Attitudes towards vaccination against seasonal influenza of health-care workers in primary health-care settings in greece. Vaccine 2010, 28, 5931–5933. [Google Scholar] [CrossRef] [PubMed]
- deSante, J.E.; Caplan, A.; Shofer, F.; Behrman, A.J. Physician attitudes towards influenza immunization and vaccine mandates. Vaccine 2010, 28, 2517–2521. [Google Scholar] [CrossRef]
- Domínguez, A.; Godoy, P.; Castilla, J.; Soldevila, N.; Toledo, D.; Astray, J.; Mayoral, J.M.; Tamames, S.; García-Gutiérrez, S.; González-Candelas, F.; et al. Knowledge of and attitudes to influenza vaccination in healthy primary healthcare workers in spain, 2011–2012. PLoS ONE 2013, 8, e81200. [Google Scholar] [CrossRef] [PubMed]
- Durando, P.; Alicino, C.; Dini, G.; Barberis, I.; Bagnasco, A.M.; Iudici, R.; Zanini, M.; Martini, M.; Toletone, A.; Paganino, C.; et al. Determinants of adherence to seasonal influenza vaccination among healthcare workers from an italian region: Results from a cross-sectional study. BMJ Open 2016, 6, e010779. [Google Scholar] [CrossRef]
- Ehrenstein, B.P.; Hanses, F.; Blaas, S.; Mandraka, F.; Audebert, F.; Salzberger, B. Perceived risks of adverse effects and influenza vaccination: A survey of hospital employees. Eur. J. Public Health 2010, 20, 495–499. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Giese, C.; Mereckiene, J.; Danis, K.; O’Donnell, J.; O’Flanagan, D.; Cotter, S. Low vaccination coverage for seasonal influenza and pneumococcal disease among adults at-risk and health care workers in ireland, 2013: The key role of gps in recommending vaccination. Vaccine 2016, 34, 3657–3662. [Google Scholar] [CrossRef] [PubMed]
- Gramegna, A.; Dellafiore, S.; Contarini, M.; Blasi, F.; Aliberti, S.; Tosatto, R.; Mantero, M. Knowledge and attitudes on influenza vaccination among italian physicians specialized in respiratory infections: An italian respiratory society (sip/irs) web-based survey. J. Prev. Med. Hyg. 2018, 59, E128–E131. [Google Scholar]
- Gutknecht, P.; Winiarski, T.; Trzeciak, B.G.; Molisz, A.; Pietrzykowska, M.; Nowicka-Sauer, K.; Siebert, J. Opinions and behavior of family doctors concerning vaccinating against influenza. Fam. Med. Prim. Care Rev. 2016, 18, 241–243. [Google Scholar] [CrossRef]
- Hagemeister, M.; Stock, N.; Ludwig, T.; Heuschmann, P.; Vogel, U. Self-reported influenza vaccination rates and attitudes towards vaccination among health care workers: Results of a survey in a german university hospital. Public Health 2018, 154, 102–109. [Google Scholar] [CrossRef]
- Harrison, N.; Brand, A.; Forstner, C.; Tobudic, S.; Burgmann, K.; Burgmann, H. Knowledge, risk perception and attitudes toward vaccination among austrian health care workers: A cross-sectional study. Hum. Vaccines Immunother. 2016, 12, 2459–2463. [Google Scholar] [CrossRef] [PubMed]
- Hopman, C.E.; Riphagen-Dalhuisen, J.; Looijmans-van den Akker, I.; Frijstein, G.; Van der Geest-Blankert, A.D.J.; Danhof-Pont, M.B.; De Jager, H.J.; Bos, A.A.; Smeets, E.; De Vries, M.J.T.; et al. Determination of factors required to increase uptake of influenza vaccination among hospital-based healthcare workers. J. Hosp. Infect. 2011, 77, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Hulo, S.; Nuvoli, A.; Sobaszek, A.; Salembier-trichard, A. Knowledge and attitudes towards influenza vaccination of health care workers in emergency services. Vaccine 2017, 35, 205–207. [Google Scholar] [CrossRef] [PubMed]
- Johansen, L.J.; Stenvig, T.; Wey, H. The decision to receive influenza vaccination among nurses in north and south dakota. Public Health Nurs. 2012, 29, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Kalemaki, D.; Karakonstantis, S.; Galanakis, E.; Lionis, C. Vaccination coverage of general practitioners: A cross-sectional study from greece. Public Health 2020, 181, 110–113. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J.; Salo, P.; Lindfelt, M.; Oksanen, T.; Kivimäki, M.; Soveri, A. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among finnish healthcare workers. PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- Kisic-Tepavcevic, D.; Kanazir, M.; Gazibara, T.; Maric, G.; Makismovic, N.; Loncarevic, G.; Pekmezovic, T. Predictors of hepatitis B vaccination status in healthcare workers in Belgrade, Serbia, December 2015. Eurosurveillance 2017, 22, 30515. [Google Scholar] [CrossRef]
- Lehmann, B.A.; Ruiter, R.A.C.; van Dam, D.; Wicker, S.; Kok, G. Sociocognitive predictors of the intention of healthcare workers to receive the influenza vaccine in belgian, dutch and german hospital settings. J. Hosp. Infect. 2015, 89, 202–209. [Google Scholar] [CrossRef]
- Maridor, M.; Ruch, S.; Bangerter, A.; Emery, V. Skepticism toward emerging infectious diseases and influenza vaccination intentions in nurses. J. Health Commun. 2017, 22, 386–394. [Google Scholar] [CrossRef]
- Napolitano, F.; Bianco, A.; D’Alessandro, A.; Papadopoli, R.; Angelillo, I.F. Healthcare workers’ knowledge, beliefs, and coverage regarding vaccinations in critical care units in italy. Vaccine 2019, 37, 6900–6906. [Google Scholar] [CrossRef]
- Nowrouzi-Kia, B.; McGeer, A. External cues to action and influenza vaccination among post-graduate trainee physicians in Toronto, Canada. Vaccine 2014, 32, 3830–3834. [Google Scholar] [CrossRef] [PubMed]
- Pielak, K.L.; McIntyre, C.C.; Tu, A.W.; Remple, V.P.; Halperin, B.; Buxton, J.A. Identifying attitudes, beliefs and reported practices of nurses and doctors as immunization providers. J. Adv. Nurs. 2010, 66, 1602–1611. [Google Scholar] [CrossRef] [PubMed]
- Prematunge, C.; Corace, K.; McCarthy, A.; Nair, R.C.; Roth, V.; Suh, K.N.; Garber, G. Qualitative motivators and barriers to pandemic vs. Seasonal influenza vaccination among healthcare workers: A content analysis. Vaccine 2014, 32, 7128–7134. [Google Scholar] [CrossRef] [PubMed]
- Quan, K.; Tehrani, D.M.; Dickey, L.; Spiritus, E.; Hizon, D.; Heck, K.; Samuelson, P.; Kornhauser, E.; Zeitany, R.; Mancia, S.; et al. Voluntary to mandatory: Evolution of strategies and attitudes toward influenza vaccination of healthcare personnel. Infect. Control Hosp. Epidemiol. 2012, 33, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Rabensteiner, A.; Buja, A.; Regele, D.; Fischer, M.; Baldo, V. Healthcare worker’s attitude to seasonal influenza vaccination in the south tyrolean province of italy: Barriers and facilitators. Vaccine 2018, 36, 535–544. [Google Scholar] [CrossRef]
- Real, K.; Kim, S.; Conigliaro, J. Using a validated health promotion tool to improve patient safety and increase health care personnel influenza vaccination rates. Am. J. Infect. Control 2013, 41, 691–696. [Google Scholar] [CrossRef]
- Rebmann, T.; Wright, K.S.; Anthony, J.; Knaup, R.C.; Peters, E.B. Seasonal influenza vaccine compliance among hospital-based and nonhospital-based healthcare workers. Infect. Control Hosp. Epidemiol. 2012, 33, 243–249. [Google Scholar] [CrossRef]
- Scatigna, M.; Fabiani, L.; Micolucci, G.; Santilli, F.; Mormile, P.; Giuliani, A.R. Attitudinal variables and a possible mediating mechanism for vaccination practice in health care workers of a local hospital in l’aquila (Italy). Hum. Vaccines Immunother. 2017, 13, 198–205. [Google Scholar] [CrossRef]
- Surtees, T.C.; Teh, B.W.; Slavin, M.A.; Worth, L.J. Factors contributing to declination of annual influenza vaccination by healthcare workers caring for cancer patients: An australian experience. Vaccine 2018, 36, 1804–1807. [Google Scholar] [CrossRef]
- Taddei, C.; Ceccherini, V.; Niccolai, G.; Porchia, B.R.; Boccalini, S.; Levi, M.; Tiscione, E.; Santini, M.G.; Baretti, S.; Bonanni, P.; et al. Attitude toward immunization and risk perception of measles, rubella, mumps, varicella, and pertussis in health care workers working in 6 hospitals of florence, italy 2011. Hum. Vaccin Immunother. 2014, 10, 2612–2622. [Google Scholar] [CrossRef]
- Tanguy, M.; Boyeau, C.; Pean, S.; Marijon, E.; Delhumeau, A.; Fanello, S. Acceptance of seasonal and pandemic a (h1n1) 2009 influenza vaccination by healthcare workers in a french teaching hospital. Vaccine 2011, 29, 4190–4194. [Google Scholar] [CrossRef] [PubMed]
- Vallée-Tourangeau, G.; Promberger, M.; Moon, K.; Wheelock, A.; Sirota, M.; Norton, C.; Sevdalis, N. Motors of influenza vaccination uptake and vaccination advocacy in healthcare workers: Development and validation of two short scales. Vaccine 2018, 36, 6540–6545. [Google Scholar] [CrossRef] [PubMed]
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; Raude, J.; Pulcini, C.; Peretti-Watel, P. Vaccine hesitancy among general practitioners and its determinants during controversies: A national cross-sectional survey in france. EBioMedicine 2015, 2, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Vírseda, S.; Restrepo, M.A.; Arranz, E.; Magán-Tapia, P.; Fernández-Ruiz, M.; de la Cámara, A.G.; Aguado, J.M.; López-Medrano, F. Seasonal and pandemic a (h1n1) 2009 influenza vaccination coverage and attitudes among health-care workers in a spanish university hospital. Vaccine 2010, 28, 4751–4757. [Google Scholar] [CrossRef]
- Wicker, S.; Zielen, S.; Rose, M.A. Obstacles in the motivation of health care workers for pertussis vaccination. Procedia Vaccinol. 2010, 2, 104–106. [Google Scholar] [CrossRef]
- Wilson, R.; Scronias, D.; Zaytseva, A.; Ferry, M.A.; Chamboredon, P.; Dubé, E.; Verger, P. Seasonal influenza self-vaccination behaviours and attitudes among nurses in southeastern france. Hum. Vaccines Immunother. 2019, 15, 2423–2433. [Google Scholar] [CrossRef]
- Wilson, R.; Zaytseva, A.; Bocquier, A.; Nokri, A.; Fressard, L.; Chamboredon, P.; Carbonaro, C.; Bernardi, S.; Dubé, E.; Verger, P. Vaccine hesitancy and self-vaccination behaviors among nurses in southeastern france. Vaccine 2020, 38, 1144–1151. [Google Scholar] [CrossRef]
- Zhang, J.; While, A.E.; Norman, I.J. Nurses’ knowledge and risk perception towards seasonal influenza and vaccination and their vaccination behaviours: A cross-sectional survey. Int. J. Nurs. Stud. 2011, 48, 1281–1289. [Google Scholar] [CrossRef]
- Zhang, J.; While, A.E.; Norman, I.J. Seasonal influenza vaccination knowledge, risk perception, health beliefs and vaccination behaviours of nurses. Epidemiol. Infect. 2012, 140, 1569–1577. [Google Scholar] [CrossRef]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and gender differences in the outcomes of vaccination over the life course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef]
- ECDC. Vaccine Hesitancy among Healthcare Workers and Their Patients in Europe—A Qualitative Study; ECDC: Stockholm, Sweden, 2015.
- Van Beek, J.; Veenhoven, R.H.; Bruin, J.P.; van Boxtel, R.A.J.; de Lange, M.M.A.; Meijer, A.; Sanders, E.A.M.; Rots, N.Y.; Luytjes, W. Influenza-like illness incidence is not reduced by influenza vaccination in a cohort of older adults, despite effectively reducing laboratory-confirmed influenza virus infections. J. Infect. Dis. 2017, 216, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Hobson-West, P. ‘Trusting blindly can be the biggest risk of all’: Organised resistance to childhood vaccination in the UK. Sociol. Health Illn. 2007, 29, 198–215. [Google Scholar] [CrossRef] [PubMed]
- Poltorak, M.; Leach, M.; Fairhead, J.; Cassell, J. ‘Mmr talk’ and vaccination choices: An ethnographic study in Brighton. Soc. Sci Med. 2005, 61, 709–719. [Google Scholar] [CrossRef] [PubMed]
- Stahl, J.P.; Cohen, R.; Denis, F.; Gaudelus, J.; Martinot, A.; Lery, T.; Lepetit, H. The impact of the web and social networks on vaccination. New challenges and opportunities offered to fight against vaccine hesitancy. Méd. Maladies Infect. 2016, 46, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Mollema, L.; Staal, J.M.; van Steenbergen, J.E.; Paulussen, T.G.W.M.; de Melker, H.E. An exploratory qualitative assessment of factors influencing childhood vaccine providers’ intention to recommend immunization in the netherlands. BMC Public Health 2012, 12, 128. [Google Scholar] [CrossRef] [PubMed]
- Heinrich-Morrison, K.; McLellan, S.; McGinnes, U.; Carroll, B.; Watson, K.; Bass, P.; Worth, L.J.; Cheng, A.C. An effective strategy for influenza vaccination of healthcare workers in australia: Experience at a large health service without a mandatory policy. BMC Infect. Dis. 2015, 15, 42. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef]
- Horne, Z.; Powell, D.; Hummel, J.E.; Holyoak, K.J. Countering antivaccination attitudes. Proc. Natl. Acad. Sci. USA 2015, 112, 10321–10324. [Google Scholar] [CrossRef]
- Riphagen-Dalhuisen, J.; Burgerhof, J.G.; Frijstein, G.; van der Geest-Blankert, A.D.; Danhof-Pont, M.B.; de Jager, H.J.; Bos, A.A.; Smeets, E.E.; de Vries, M.J.; Gallee, P.M.; et al. Hospital-based cluster randomised controlled trial to assess effects of a multi-faceted programme on influenza vaccine coverage among hospital healthcare workers and nosocomial influenza in The Netherlands, 2009 to 2011. Eurosurveillance 2013, 18, 20512. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Study Design | Enrolment Period | Enrolment Site | Sample Size | Study Population | Theoretical Framework | Outcome Measures * | Vaccination Coverage | Quality Score ** |
|---|---|---|---|---|---|---|---|---|---|
| Balaban, 2013 [16] | Pre- and post-travel surveys | 2009 | USA | 186 | American Hajj pilgrims | None | Seasonal influenza | - | Low |
| Barasheed, 2014 [17] | Cross-sectional survey | 2011–2012 | Mina (Mecca) | 966 | Australian Hajj pilgrims | None | Influenza | 62% | High |
| Duffy, 2013 [18] | Cross-sectional survey | 2007 (Aug.–Sept.) | United States | 1691 | American travellers to Asia | None | JE | 11% | Medium |
| Frew, 2017 [19] | Cross-sectional survey | 2015 (Feb.–March) | Ferry ports of 2 popular islands, Thailand | 1680 | Backpackers from Europe, Canada, Australia and New-Zealand (94%) | None (KAP) | HBV | 31% completed series | High |
| Goodman, 2014 [20] | Online cross-sectional survey | 2010 (Feb.) | UK | 302 | Travellers to the meningitis belt of Africa in last 3 years or planned to do so next 6 months | None | MenAWCY | 30% | Medium |
| Herbinger, 2011 [21] | Online cross-sectional survey | 2009 (Dec.) | Netherlands, Czech Republic, Spain, Sweden | 4203 | Travellers to countries of moderate or high prevalence for HBV in the last 5 years | None | HBV | 39% in the previous 5 years | Medium |
| Heywood, 2016 [22] | Online cross-sectional survey | 2014 (Aug.–Oct.) | Australia, Finland, Germany, Norway, Sweden, UK, Canada | 27,386 | Travellers (18–65 years) who travelled to HAV endemic countries in Africa, Asia, South/Central America in the last 3 years | None | HAV/HBV | 27% for 3-dose combined HAV and HBV and 37% for 2-dose monovalent HAV schedules | Medium |
| Igreja, 2019 [23] | Cross-sectional survey | 2019 (May–June) | Travel Clinic, Lisbon, Portugal | 55 | Portuguese travellers | None | Attitudes to vaccinations in general | - | Low |
| Lammert, 2016 [24] | Retrospective study | 2012–2014 | clinics from Global TravEpiNet, USA | 24,478 | International travellers who sought pre-travel health advice | None | Refusal rates of recommended vaccines and reasons | 25% refused one or more recommended vaccine(s) | High |
| Paudel, 2017 [25] | Prospective enhanced surveillance study | 2013 (Feb–2014 (Jan.) | Australia | 180 | confirmed cases of typhoid, paratyphoid, measles, HAV, HEV, chikungunya, malaria | None | Seeking pre-travel advice and uptake | 25% sought pre-travel advice and 16% got vaccinated | Medium |
| Pavli, 2019 [26] | Cross-sectional survey by email | 2015 (Nov.)–2016 (Mar.) | Greece | 231 | Greek (non-healthcare) students from 36 universities, planning to study abroad | None | Men, intention to vaccinate | 23% vaccinated, 15% intention | Medium |
| Pfeil, 2010 [27] | 2 cross-sectional surveys | 2009 (Jan.–Feb.), 2010 (Jan.) | Centre for Travel Health, Zurich, Switzerland | 623 | Travellers to a resource-limited destination | None (KAP) | Seasonal (and pandemic) influenza | 14% seasonal influenza | High |
| Selcuk, 2016 [28] | Cross-sectional survey | 2013 (July) | Istanbul Ataturk Airport, Istanbul, Turkey | 124 | Turkish travellers to Africa | None | Recommended for destination | 53% vaccinated pre-travel | Medium |
| Tan, 2017 [29] | Retrospective cohort study | 2012 (Jan.)–2013 (Dec.) | Mayo Clinic Travel and Tropical Medicine Clinic, Minnesota, USA | 2073 | Children and adults who sought pre-travel advice (19% VFR) | None | Documented receipt or positive serology or completion of series | 94% men in VFR, 12% rabies in VFR | High |
| Tashani, 2016 [30] | Cross-sectional survey | 2014–2015 | Immunization clinic, Sydney, Australia | 300 | Travellers (>18 year) planning to attend Hajj | None | Pneu and DTP when recommended | 17% pneu, 14% DTP | Medium |
| Wiemken, 2015 [31] | Cross-sectional study | 2013 (Nov.)–2014 (July) | University of Louisville, Travel Clinic, USA | 183 | American travellers before their consultation | TPB | Intention to get vaccinated | Not given | High |
| Yanni, 2010 [32] | Pre- and post-travel surveys | 2008 (June–Sept.) | Departure lounges at airports in New York, Chicago, Los Angeles, and San Francisco | 1301 (pre) (337 post) | American travellers who will travel to Asia | KAP | Influenza | 41% | High |
| Akin, 2016 [33] | Cross-sectional survey | 2015 (July–Sep.) | Daycare chemotherapy unit of Hacettepe University Cancer Institute, Ankara, Turkey | 229 | Adult patients with cancer receiving chemotherapy | None | Adult vaccination coverage (influenza, tetanus, hepatitis, pneu) | 54% were vaccinated at least once, only 9% after cancer diagnosis | Medium |
| Althoff, 2010 [34] | Nested influenza study (interview administered surveys) | 2006–2007 and 2007–2008 | 5 cities in the USA | 1462 | HIV+ women | HBM | Influenza | 55–57% of women reported vaccination (about 44% not vaccinated) | Medium |
| Battistella, 2019 [35] | Cross-sectional observational study | 2017 (Jan.–July) | 7 large dialysis services, Italy | 703 | Dialysis patients | None | Influenza | 58% adherence | High |
| Chehab, 2018 [36] | Cross-sectional study (in longitudinal cohort) | 2012 (Nov.)–2013 (Oct.) | Germany | 579 | SLE patients (48% on IS) | None | Influenza, tetanus, pneu, men and previous refusal | 45% influenza (last year); 65% tetanus; 32% pneu; 6% men | High |
| Chin-Yee, 2011 [37] | Cohort study (one time follow-up) | 2009 (Oct.)–2010 (Mar.) | Tertiary care cancer center, Canada | 129 | Patients with hematologic malignancies (92% chemotherapy, 76% in past 3 mo) | None | Seasonal influenza (and pandemic) | 57% seasonal influenza | Medium |
| Gagneux-Brunon, 2019 [38] | Cross-sectional survey | Unknown | France | 468 | HIV+ patients | None | Pneu, HAV, HBV, seasonal influenza | 30% IPD; 24% HAV; 64% HBV; 40% influenza | Low |
| Haroon, 2011 [39] | Cross-sectional survey (audit) | 2009 (Sept.) | Outpatient clinics, tertiary university hospital, Ireland | 110 | Rheumatology patients on IS | None | Seasonal influenza and pneu | 34% influenza; 11% pneu; 11% both | Medium |
| Harrison, 2017 [40] | Cross-sectional survey | 2015 (Aug.–June) | HIV out-patient department of the University Hospital of Vienna, Austria | 455 | HIV patients | None | Seasonal influenza | 12% influenza | Medium |
| Harrison, 2018 [41] | Cross-sectional survey | 2017 (July–Oct.) | Outpatient clinic, Medical University of Vienna, Austria | 490 | Inflammatory rheumatic disease patients on IS | None | Seasonal influenza | 25% influenza | Medium |
| Lachenal, 2010 [42] | Cross-sectional survey (standardized questionnaire) | 2008 (Jan.) | Centre Léon-Bérard, Lyon, France | 200 | Patients with haematological malignancies (hospitalized or at outpatient clinic) | None | Influenza | 26% | Medium |
| Loubet, 2015 [43] | Self-reported cross-sectional survey | 2013 (Summer) | AVNIR, a group of associations whose goal is to support ICP, France | 3653 | 79% autoimmune, 13% SOT, 8% treated for hematological malignancies. 85% on IS. | KAP | Influenza and pneu | 59% seasonal influenza and 49% pneu | Medium |
| Loubet, 2018 [44] | Self-reported cross-sectional survey | 2015 (Dec.)–2016 (March) | AFA, national association of patients with IBD, France | 199 | IBD patients (62% receiving IS) | KAP | Influenza and pneu | 34% influenza, 38% pneu | Medium |
| Malhi, 2015 [45] | Cross-sectional survey (self-reported, paper-based) | 2013 (Sept)–2014 (Jan.) | IBD Clinic or Endoscopy Suite at Mount Sinai Hospital, Toronto, Canada | 305 | IBD patients (53% using biologicals/steroids) | None | Influenza, pneu, HAV, HBV, VZV, men, HVZ, HPV | 61% influenza, 10% pneu, 61% HBV, 52% HAV, 26% VZV, 21% men, 5% HZV, 11% HPV | High |
| Miller, 2018 [46] | Cross-sectional survey | 2016 (June–Sept.) | 3 tertiary autologous and allogeneic HSCT centres, UK | 93 | HSCT patients (79% autologous) | adjusted HBM | Intention to receive seasonal influenza | 76% expressed high intent | High |
| Mouthon, 2010 [47] | Cross-sectional survey (standardized questionnaires) | 2006 and 2007 | Dept. Of Internal Medicine, Cochin Hospital, France | 177 | Patients with systemic sclerosis | None | Influenza | 39% (last year) | Medium |
| Narula, 2012 [48] | Cross-sectional survey | 2010 (May–Aug.) | McMaster University Medical Centre Digestive Disease Clinic, Canada | 250 | IBD patients (63% on IS) | None | Seasonal (and H1N1) influenza | 25% seasonal influenza | High |
| Nguyen, 2017 [49] | Cross-sectional survey with invitation RCT for new pneu vaccine) | 2014 (Oct.–Nov.) | Outpatients clinic of rheumatology at 2 hospitals in Graasten, Denmark | 192 | RA patients | None | Influenza and pneu | 59% seasonal influenza ever, 49% last year, 6% pneu | High |
| Poeppl, 2015 [50] | Cross-sectional survey | 2013 (July)–2013 (Oct.) | Outpatient departments of the General Hospital Vienna, Austria | 444 | Patients with malignancies (55% solid tumours, 22% haematological malignancy, and 17% had no diagnosed malignancy) | None | Influenza | 18% influenza last year | Medium |
| Price, 2019 [51] | Cross-sectional survey | 2014 (June–July) | Cancer center providing ambulatory care, USA | 703 | Patients (83%) (and caregivers and family (17%) of patients) treated for malignancies | None | Influenza | Patients 72%, caregivers 71% (last year) | Medium |
| Restivo, 2017 [52] | Prospective observational study | 2014 (Oct.)–2015 (April) | SOT Reference Center in Palermo, Sicilia, Italy | 82 | SOT recipients during hospital admission for transplantation | None | Influenza | 38% | Medium |
| Ruiz-Cuesta, 2016 [53] | Prospective observational study | 2012 (Jan.–March) | Reina Sofía University Hospital, Córdoba, Spain | 153 | IBD (50% UC, 50% CD) patients (>14 years old), 34% on biologicals/corticosteroids | None | HAV, HBV, VZV, MMR assessed by registry | 84% | Medium |
| Sadlier, 2015 [54] | Retrospective study, with provider-delivered survey | 2014 (Jan.–Feb.) | Tertiary university hospital in Ireland | 170 | Dermatology patients prescribed systemic IS | None | Influenza and pneu | 38% seasonal influenza last year, 21% pneu last 5 years, 18% both. | Medium |
| Sandler, 2016 [55] | Cross-sectional, telephone survey | 2013 (July–Sept.) | Memorial Medical Center in Chicago, USA | 102 | RA patients (85–91% taking IS) | None | Self-reported and EHR influenza, pneu, and HZV | 79% influenza last season, 54% pneu and 8% HZV | High |
| Savage, 2011 [56] | Retrospective audit | 2010 (Aug.–Oct.) | Outpatient dermatology clinics in Aberdeen RoyalInfirmary, Scotland | 87 | Immunocompromised dermatology patients | None | Influenza and pneu | 70% influenza (last year), 22% pneu | Medium |
| Struijk, 2015 [57] | Cross-sectional survey | Unknown | Renal Transplant Unit, Academic Medical Center, Amsterdam, NL | 526 | 77% renal transplant recipients (and their nephrologists) | KAB | Influenza, tetanus, pneumococci, HAV, HBV | 56% influenza, 15–30% tetanus, 0–5% pneu, 5–30% HAV, 10–20% HBV | High |
| Teich, 2011 [58] | Cross-sectional survey | 2009 (April–Sept.) | Germany | 203 | IBD patients who had not received vaccination counseling ≥1 year (54% on IS) | None | Vaccinations in general | 67% tetanus (<10 years), 21% pertussis, 28% seasonal influenza, 9% pneu | High |
| Urun, 2013 [59] | Cross-sectional survey (with face-to-face interviews) | 2012 (Jan.–March) | Medical Oncology Department of Ankara University Faculty of Medicine, Turkey | 359 | Patients with malignancies | None | Influenza and pneu | 17% influenza 4% pneumococcal | Medium |
| Waszczuk, 2018 [60] | Cross-sectional survey (self-completed) | Unknown | Wrowclaw, Poland | 195 | IBD patients (70% on IS) | None | Influenza, HBV and pneu | HBV 55%; Tdap 12%; HAV 7%; annual influenza 6%; VZV/HZV 3%, and pneu 2% | High |
| Wilckens, 2011 [61] | Cross-sectional survey | 2009 (April–Oct.) | IBD outpatients’ clinic, a tertiary referral center, Lueneburg, Germany | 102 | IBD patients (57% CD, 91% on IS) | None | Vaccinations in general | 19% influenza, 3% pneumoccous, 22% HBV, 5% VZV, 55% MMR, and 63% tetanus. Of those who had traveled, 9% HAV and 1% YF | High |
| Akan, 2016 [62] | Cross-sectional study | 2014 (June–Sept.) | family health care centres in Turkey | 596 | GPs | used, name not mentioned | Seasonal influenza | 27% | High |
| Asma, 2016 [63] | Cross-sectional study | 2015 (Jan.) | 6 university hospitals in Turkey | 642 | 177 (28%) physicians and 448 (71%) nurses | None | Seasonal influenza | 9% | Medium |
| Boey, 2018 [64] | Cross-sectional study | 2015 (Nov.–Dec.) | 13 hospitals and 14 nursing homes in Belgium | 5141 | 4506 hospital staff, 635 HCW nursing home staff. | HBM, HIM and ASE | Seasonal influenza | 2014: 62% (hospital) 2015: 65% (hospital) | High |
| Bonaccorsi, 2015 [65] | Cross-sectional study | 2010 (Oct.–Nov.) | Careggi University Teaching Hospital, Florance, Italy | 2576 | 10% physicians, 39% nurses, 23% students, 4% health care assistant, 15% other | None | Seasonal influenza | 18% | Medium |
| Castilla, 2013 [66] | Cross-sectional study | 2012 (Mar.–May) | PHC workers, Spain | 1956 | 47% GP, 10% paediatricians, 43% nurses | None | Seasonal influenza | 52–61% (2008–2011) | High |
| Ciftci, 2018 [67] | Cross-sectional study | 2015 (Sept.–Dec.) | University Hospital, Ankara, Turkey | 470 | Tertiary healthcare setting (18% physicians, 29% nurses, 11% assistants, 23% auxillary, 9% paramedics, 10% secretaries) | None | Seasonal influenza | 27% | High |
| Costantino, 2019 [68] | Cross sectional study | Influenza seasons 2016–2019 | University Hospital of Palermo, Italy | 1237 | Hospital HCW that had not received influenza vaccination | None | Seasonal influenza | 0% | High |
| Dedoukou, 2010 [69] | Cross-sectional study | 2018 (Oct.–Nov.) | 76 PHCs in Greece | 1617 | PHC: 35% physicians, 32% nurses, 23% paramedical/technical, 8% administrative | None | Seasonal influenza | 41% | Medium |
| deSante, 2010 [70] | Cross-sectional study | 2009 (Apr.) | 2 tertiary care hospitals in Pennsylvania, USA | 227 | House officers and attending physicians in emergency/internal medicine depts. | None | Seasonal influenza | 94% | Medium |
| Dominguez, 2013 [71] | Cross-sectional study | 2012 (Mar.–May) | PHC workers in 7 Spanish regions | 1749 | Familiy physician (47%), paediatrician (10%), nurses (43%). | None | Seasonal influenza | 51% | High |
| Durando, 2016 [72] | Cross-sectional study | 2013 (Oct.)–2014 (Apr.) | San Martino Teaching Hospital/Scientific Research Institute, Italy | 830 | HCW | None | Seasonal influenza | 26% | High |
| Ehrenstein, 2010 [73] | Cross-sectional study | 2006 (Feb.) | Tertiary care university hospital in Germany | 652 | HCW (physicians 36%, nurses 42%, administrators 22%) | None | Seasonal influenza | 34% | Medium |
| Giese, 2016 [74] | Cross-sectional study | 2013 | Ireland | 164 | HCW in a study group of Irish residents | None | Seasonal influenza | 28% | Medium |
| Gramegna, 2018 [75] | Cross-sectional study | 2016 | Italy | 144 | Italian Respiratory Society members | Seasonal influenza | 55% | Medium | |
| Gutknecht, 2016 [76] | Cross-sectional study | 2016 (Feb.–Mar.) | Poland | 77 | Physicians | None | Seasonal influenza | - | Low |
| Hagemeister, 2018 [77] | Cross-sectional study | 2015 (June-July) | University Hospital Würzburg, Germany | 677 | Physicians and nursing staff | None | Seasonal influenza | 55% | Medium |
| Harrison, 2016 [78] | Cross-sectional study | - | Vienna General Hospital, Austria | 116 | Nursing staff | None | HAV/HBV, DTP/Tdap, MMR, influenza, VZV, men, pneu | Seasonal influenza: 42%; Measles: 60% | Medium |
| Hopman, 2010 [79] | Cross-sectional study | 2008 (Nov.–Dec.) | All 8 University Medical Centers in NL | 1238 | HCW at medium and high risk for influenza | HBM, BIM, ASE | Seasonal influenza | 38% | Medium |
| Hulo, 2017 [80] | Cross-sectional study | 2014 | University Hospital Lille, France | 344 | HCW in the emergency departments and the IC units | None | Seasonal influenza | 18% | Medium |
| Johansen, 2012 [81] | Cross-sectional study | 2007 (May) | North and South Dakota | 155 | Randomly selected nurses (52% hospital, 13% clinic, 12% long term) | Triandis | Seasonal influenza | - | Medium |
| Kalemaki, 2020 [82] | Cross-sectional study | - | Crete, Greece | 260 | GPs | None | Seasonal influenza, measlesHBV, Tdap | Seasonal influenza 57%; Measles 26% HBV 68%; Tdap 47% | High |
| Karlsson, 2019 [83] | Cross-sectional study | - | Public hospitals in Finland | 2962 | Hospital personnel who may work with vaccinations (14% physicians) | None | Seasonal influenza | - | High |
| Kisic-Tepavcevic, 2017 [84] | Cross-sectional study | 2015 (Dec.) | Clinical Centre of Serbia, Belgrade, Serbia | 352 | HCW | None | HBV | 66% | High |
| Lehmann, 2015 [85] | Cross-sectional study | 2013 (Feb.–Apr.) | 20 hospitals in Belgium, Germany and NL | 1022 | 56% nurse, 15% physicians, 14% paramedics | None | Seasonal influenza | Total: 37%; Netherlands: 28%; Belgium: 53%; Germany: 36% | High |
| Maridor, 2017 [86] | Cross-sectional study | 2013 | 3 medium-sized, non-teaching hospitals, Switzerland | 252 | Nursing staff | None | Seasonal influenza | 58% | Medium |
| Napolitano, 2019 [87] | Cross-sectional study | 2018 (Sept.–Nov.) | 8 hospitals in Italy | 531 | Random sample of HCWs (29% physicians, 59% nurses) | None | HBV, influenza, MMR, VZV, pertussis | HBV: 98%; DTP: 91%; MMR: 64%; VZV: 59%; TBC: 50%; Influenza: 30%; Men C: 41% | High |
| Nowrouzi, 2014 [88] | Cross-sectional study | 2011 (Sept.–Nov.) | University of Toronto | 963 | Medical trainee’s (post graduate) | HBM | Seasonal (and pandemic) influenza | Seasonal influenza 69–76% (2008–2010) | High |
| Pielak, 2010 [89] | Cross-sectional study | 2005 (Apr.) | British Columbia, Canada | 719 | Immunization nurses of all health units and all physicians that administer vaccinations | TPB | Seasonal influenza | - | High |
| Prematunge, 2014 [90] | Cross-sectional study | 2010 (June) | Tertiary care hospital Ontario, Canada | 3275 | 35% nurse, 5% physician, 11% allied HCW’s, 22% administrative/clerical | None | Seasonal (and pandemic) influenza | Seasonal influenza: 74% | Medium |
| Quan, 2012 [91] | Retrospective cohort study | 2006–2011 | University of California Irvine Healthcare | 32,808 | all HCWs | None | Seasonal influenza | 44–92% (2007–2011) | Medium |
| Rabensteiner, 2018 [92] | Cross-sectional study | 2016 (Oct.–Dec.) | South Tyearolean Health Service, Italy | 4091 | 13% physicians, 20% administrative, 67% sanitary or executive non-medical staff | None | Seasonal influenza | 10% | High |
| Real, 2013 [93] | Cross-sectional study | - | Academic medical center in Lexington, USA | 318 | 80% clinical, 20% non-clinical | RPA | Seasonal influenza | 66% already received the vaccination or planned to get one soon | Medium |
| Rebmann, 2012 [94] | Cross-sectional study | 2011 (Apr.–June) | Saint Louis region, USA | 3188 | 54% non-hospital HCW, 46 % hospital HCW | None | Seasonal (and pandemic) influenza | 2010/11: 79% | High |
| Scatigna, 2017 [95] | Cross-sectional study | 2015 (Apr.–May) | San Salvatore Hospital, L’Aquila, Italy | 334 | Nurses 53%, physicians 23%, other 24% | None | HBV, influenza, MMR, VZV | - | Medium |
| Surtees, 2018 [96] | Cross-sectional study | 2016 | Tertiary referral hospital in Victoria, Australia | 1835 | HCW | None | Seasonal influenza | 97% | High |
| Taddei, 2014 [97] | Cross-sectional study | 2011 (June–Oct.) | 6 public hospitals in Florence, Italy | 436 | 59% nurses, 21% physicians, 13% nursing assistants, and 7% were midwives | None | MMR, VZV, Pertussis | 11% measles, 7% mumps, 17% rubella, 2% VZV, 7% pertussis | Medium |
| Tanguy, 2011 [98] | Cross-sectional study | 2009 (Nov.)–2010 (Feb.) | Tertiary care centre in Pays de la Loire Region, France | 532 | 24% medical staff, 65% nursing staff, 11% ancillary staff | None | Seasonal (and pandemic) influenza | 22% | Medium |
| Vallée-Tourange, 2018 [99] | Cross-sectional study | 2014 (June–July) | A single metropolitan hospital group, UK | 784 | 11% physicians, 36% nurses, 30% allied health professionals, 17% assistants | CME | Seasonal influenza | - | Medium |
| Verger, 2016 [100] | Cross-sectional study | 2014 (Apr.–July) | France | 1582 | GPs | None | Seasonal influenza, DTP, HBV | 72% influenza, 84% DTP, 86% HBV | High |
| Virseda, 2010 [101] | Cross-sectional study | 2009 (Dec.)–2010 (Jan.) | University Hospital 12 de Octubre, Madrid, Spain | 527 | HCW (23% physician, 29% nurse, 19% nursing assistant, 29% ancillary staff) | None | Seasonal (and pandemic) influenza | 50% | Medium |
| Wicker, 2010 [102] | Cross-sectional study | 2010 (Jan–May) | Frankfurt University Hospital, Germany | 1504 | Physicians 26%, nurses 35%, other HCW 23%, students 16% | None | Pertussis | 22% in last 10 years | Medium |
| Wilson, 2019 [103] | Cross-sectional study | Influenza seasons 2015–2017 | Southeast France | 1539 | 74% hospital nurses, 26% community nurses | None | Seasonal influenza | Both seasons: 24% at least one season: 34% | Medium |
| Wilson, 2020 [104] | Cross-sectional study | 2017–2018 | Southeast France | 1539 | 74% hospital nurses, 26% community nurses | None | Mandatory and recommended vaccines in France | 96% BCG, 73% DTP (<10 years), 61% HBV, 58% pertussis, 64% measles, 39% VZV, 27% seasonal influenza (last year) | Medium |
| Zhang, 2011 [105] and 2012 [106] | Cross-sectional study | 2010 (May-Oct.) | University Hospital London | 522 | Qualified nurses (79% working in hospital | None | Seasonal influenza | 36% | Medium |


 (double caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥50% of the population;
(double caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥50% of the population;  (double caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥50% of the population; ⌃ (caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥10% of the population; ⌄ (caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥10% of the population. * determinants were studied in relation to intention to be vaccinated instead of vaccination uptake. The following abbreviations are used (in alphabetical order): CD = Crohn’s Disease; DTP = diphtheria, tetanus, poliomyelitis; GP = general practitioner; HAV = hepatitis A virus; HBV = hepatitis B virus; HCW = healthcare workers; HIV = human immunodefiency virus; HSCT = hematological stem cell transplantation; HZV = herpes zoster virus; IBD = inflammatory bowel disease; IS = immunosuppressants; JE = Japanese encephalitis; Men = meningococcal disease; MMR = measles, mumps, rubella; Pneu = pneumococcal disease; Tdap = tetanus, diphtheria, acellular pertussis; SOT = solid organ transplantation; VFR = travellers visiting friends and relatives; VZV = varicella zoster virus; YF = yellow fever.
(double caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥50% of the population; ⌃ (caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥10% of the population; ⌄ (caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥10% of the population. * determinants were studied in relation to intention to be vaccinated instead of vaccination uptake. The following abbreviations are used (in alphabetical order): CD = Crohn’s Disease; DTP = diphtheria, tetanus, poliomyelitis; GP = general practitioner; HAV = hepatitis A virus; HBV = hepatitis B virus; HCW = healthcare workers; HIV = human immunodefiency virus; HSCT = hematological stem cell transplantation; HZV = herpes zoster virus; IBD = inflammatory bowel disease; IS = immunosuppressants; JE = Japanese encephalitis; Men = meningococcal disease; MMR = measles, mumps, rubella; Pneu = pneumococcal disease; Tdap = tetanus, diphtheria, acellular pertussis; SOT = solid organ transplantation; VFR = travellers visiting friends and relatives; VZV = varicella zoster virus; YF = yellow fever.
 (double caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥50% of the population; (double caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥50% of the population; ⌃ (caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥10% of the population; ⌄ (caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥10% of the population. The following abbreviations are used (in alphabetical order): CD = Crohn’s Disease; DTP = diphtheria, tetanus, poliomyelitis; GP = general practitioner; HAV = hepatitis A virus; HBV = hepatitis B virus; HCW = healthcare workers; HIV = human immunodefiency virus; HSCT = hematological stem cell transplantation; HZV = herpes zoster virus; IBD = inflammatory bowel disease; IS = immunosuppressants; JE = Japanese encephalitis; Men = meningococcal disease; MMR = measles, mumps, rubella; Pneu = pneumococcal disease; Tdap = tetanus, diphtheria, acellular pertussis; SOT = solid organ transplantation; VFR = travellers visiting friends and relatives. VZV = varicella zoster virus, YF = yellow fever.
(double caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥50% of the population; (double caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥50% of the population; ⌃ (caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥10% of the population; ⌄ (caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥10% of the population. The following abbreviations are used (in alphabetical order): CD = Crohn’s Disease; DTP = diphtheria, tetanus, poliomyelitis; GP = general practitioner; HAV = hepatitis A virus; HBV = hepatitis B virus; HCW = healthcare workers; HIV = human immunodefiency virus; HSCT = hematological stem cell transplantation; HZV = herpes zoster virus; IBD = inflammatory bowel disease; IS = immunosuppressants; JE = Japanese encephalitis; Men = meningococcal disease; MMR = measles, mumps, rubella; Pneu = pneumococcal disease; Tdap = tetanus, diphtheria, acellular pertussis; SOT = solid organ transplantation; VFR = travellers visiting friends and relatives. VZV = varicella zoster virus, YF = yellow fever. (double caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥50% of the population; (double caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥50% of the population; ⌃ (caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥10% of the population; ⌄ (caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥10% of the population. pRisk = perceived risk. pRisk of infection (S/P): S = self; P = patient. The following abbreviations are used (in alphabetical order): CD = Crohn’s Disease; DTP = diphtheria, tetanus, poliomyelitis; GP = general practitioner; HAV = hepatitis A virus; HBV = hepatitis B virus; HCW = healthcare workers; HIV = human immunodefiency virus; HSCT = hematological stem cell transplantation; HZV = herpes zoster virus; IBD = inflammatory bowel disease; IS = immunosuppressants; JE = Japanese encephalitis; Men = meningococcal disease; MMR = measles, mumps, rubella; Pneu = pneumococcal disease; Tdap = tetanus, diphtheria, acellular pertussis; SOT = solid organ transplantation; VFR = travellers visiting friends and relatives. VZV = varicella zoster virus, YF = yellow fever.
(double caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥50% of the population; (double caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥50% of the population; ⌃ (caret pointing upwards) significance was not tested, but determinant was positively linked to vaccination uptake in ≥10% of the population; ⌄ (caret pointing downwards) significance was not tested, but determinant was negatively linked to vaccination uptake in ≥10% of the population. pRisk = perceived risk. pRisk of infection (S/P): S = self; P = patient. The following abbreviations are used (in alphabetical order): CD = Crohn’s Disease; DTP = diphtheria, tetanus, poliomyelitis; GP = general practitioner; HAV = hepatitis A virus; HBV = hepatitis B virus; HCW = healthcare workers; HIV = human immunodefiency virus; HSCT = hematological stem cell transplantation; HZV = herpes zoster virus; IBD = inflammatory bowel disease; IS = immunosuppressants; JE = Japanese encephalitis; Men = meningococcal disease; MMR = measles, mumps, rubella; Pneu = pneumococcal disease; Tdap = tetanus, diphtheria, acellular pertussis; SOT = solid organ transplantation; VFR = travellers visiting friends and relatives. VZV = varicella zoster virus, YF = yellow fever.© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doornekamp, L.; van Leeuwen, L.; van Gorp, E.; Voeten, H.; Goeijenbier, M. Determinants of Vaccination Uptake in Risk Populations: A Comprehensive Literature Review. Vaccines 2020, 8, 480. https://doi.org/10.3390/vaccines8030480
Doornekamp L, van Leeuwen L, van Gorp E, Voeten H, Goeijenbier M. Determinants of Vaccination Uptake in Risk Populations: A Comprehensive Literature Review. Vaccines. 2020; 8(3):480. https://doi.org/10.3390/vaccines8030480
Chicago/Turabian StyleDoornekamp, Laura, Leanne van Leeuwen, Eric van Gorp, Helene Voeten, and Marco Goeijenbier. 2020. "Determinants of Vaccination Uptake in Risk Populations: A Comprehensive Literature Review" Vaccines 8, no. 3: 480. https://doi.org/10.3390/vaccines8030480
APA StyleDoornekamp, L., van Leeuwen, L., van Gorp, E., Voeten, H., & Goeijenbier, M. (2020). Determinants of Vaccination Uptake in Risk Populations: A Comprehensive Literature Review. Vaccines, 8(3), 480. https://doi.org/10.3390/vaccines8030480