Maximization of Livestock Anthrax Vaccination Coverage in Bangladesh: An Alternative Approach


 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
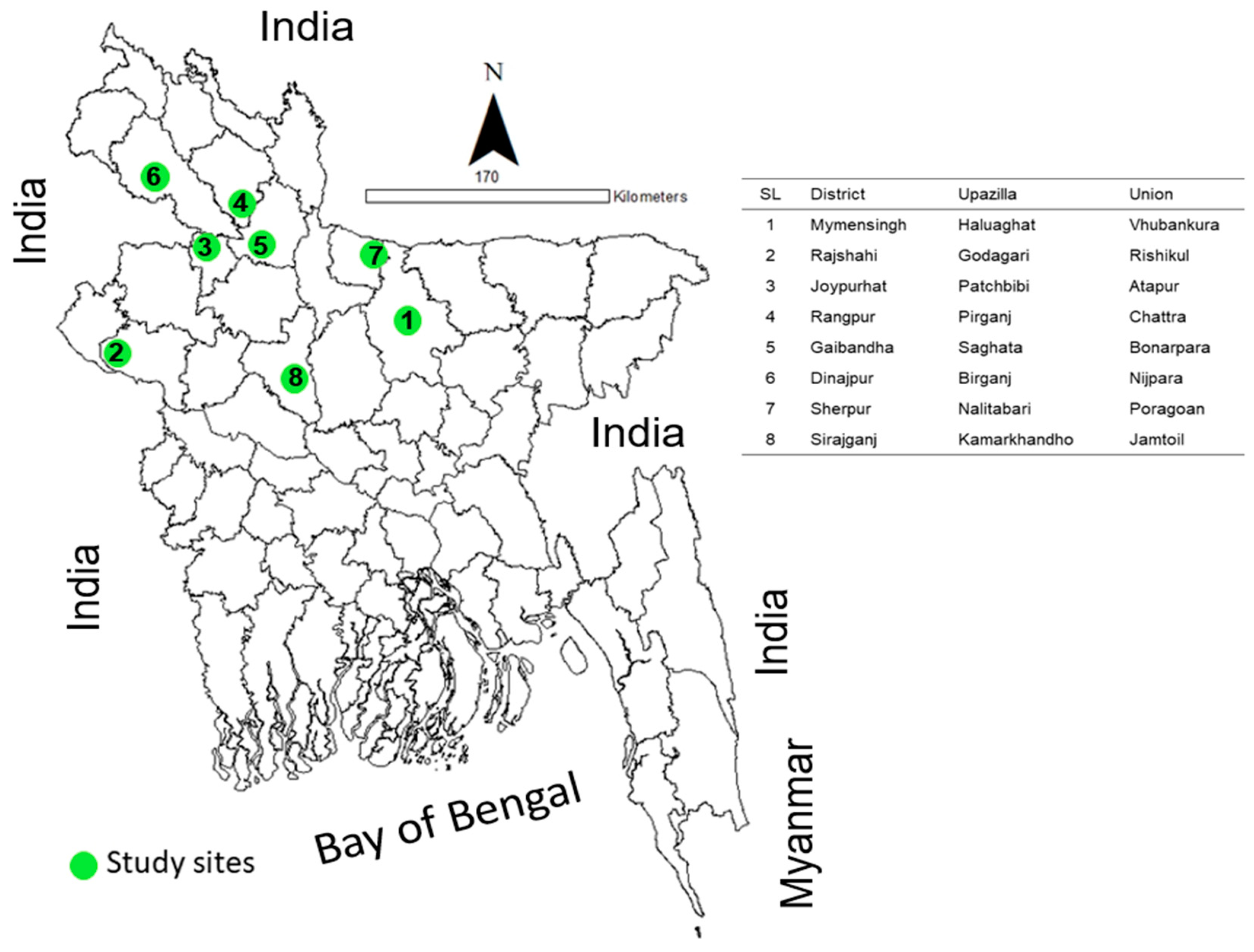
2.2. Study Sites
2.3. Anthrax Vaccine Used for Mass Vaccination
2.4. Organization of Campaigns and Vaccinated Campaign for Cattle
2.5. Livestock Census
2.6. Focus Group Discussion
2.7. Key Informer Interview
2.8. Validation of FGD Findings
2.9. Quantitative and Qualitative Data Analysis
3. Results
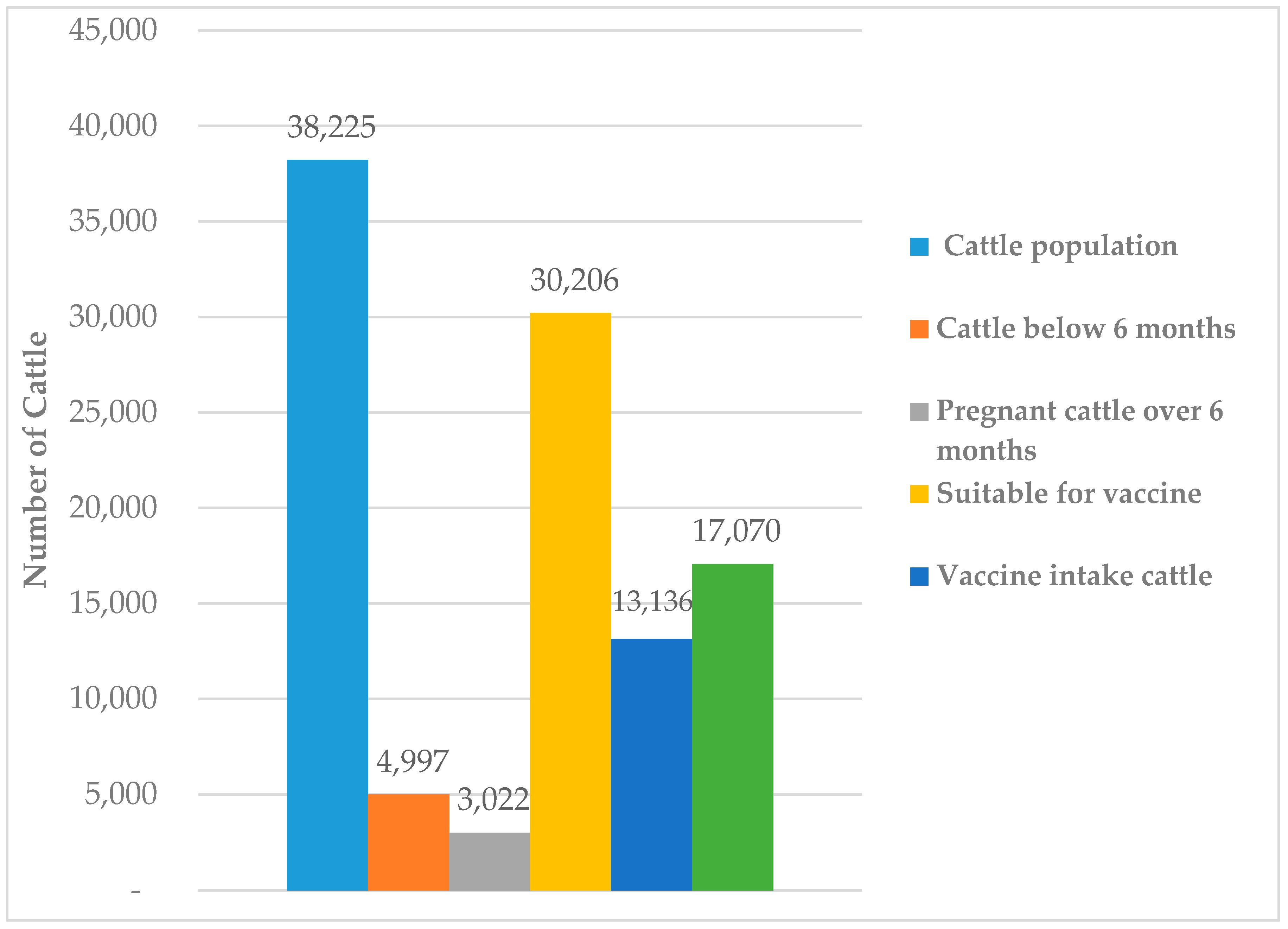
3.1. Livestock Anthrax Vaccination Rate
3.2. Barriers to Vaccine Uptake
3.3. Recommendations to Maximize Vaccine Uptake
3.4. Validation of the FGD Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Department of Livestock Services, (DLS). Livestock Economy at a Glance. Department of Livestock Services, Ministry of Fisheries and Livestock, Government of the People’s Republic of Bangladesh. Available online: http://dls.portal.gov.bd/sites/default/files/files/dls.portal.gov.bd/page/ee5f4621_fa3a_40ac_8bd9_898fb8ee4700/Livestock%20Economy%20at%20a%20glance%20%20%282017-2018%29.pdf (accessed on 25 March 2020).
- Ehizibolo, D.; Ehizibolo, P.; Ehizibolo, E.; Sugun, M.; Idachaba, S. The control of neglected zoonotic diseases in Nigeria through animal intervention. Afr. J. Biomed. Res. 2011, 14, 81–88. [Google Scholar]
- Okello, A.L.; Gibbs, E.P.J.; Vandersmissen, A.; Welburn, S.C. One Health and the neglected zoonoses: Turning rhetoric into reality. Vet. Rec. 2011, 169, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Mondal, S.P.; Yamage, M. A retrospective study on the epidemiology of anthrax, foot and mouth disease, haemorrhagic septicaemia, peste des petits ruminants and rabies in Bangladesh, 2010–2012. PLoS ONE 2014, 9, e104435. [Google Scholar] [CrossRef] [PubMed]
- Hugh-Jones, M.; Blackburn, J. The ecology of Bacillus anthracis. Mol. Asp. Med. 2009, 30, 356–367. [Google Scholar] [CrossRef]
- Woods, C.W.; Ospanov, K.; Myrzabekov, A.; Favorov, M.; Plikaytis, B.; Ashford, D.A. Risk factors for human anthrax among contacts of anthrax-infected livestock in Kazakhstan. Am. J. Trop. Med. Hyg. 2004, 71, 48–52. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Human anthrax associated with an epizootic among livestock-North Dakota, 2000. MMWR Morb. Mortal. Wkly. Rep. 2001, 50, 677–680. [Google Scholar]
- Ndiva Mongoh, M.; Hearne, R.; Khaitsa, M. Private and public economic incentives for the control of animal diseases: The case of anthrax in livestock. Transbound. Emerg. Dis. 2008, 55, 319–328. [Google Scholar] [CrossRef]
- Chakraborty, A.; Khan, S.U.; Hasnat, M.A.; Parveen, S.; Islam, M.S.; Mikolon, A.; Chakraborty, R.K.; Ahmed, B.-N.; Ara, K.; Haider, N. Anthrax outbreaks in Bangladesh, 2009–2010. Am. J. Trop. Med. Hyg. 2012, 86, 703–710. [Google Scholar] [CrossRef]
- Siddiqui, M.A.; Khan, M.A.H.; Ahmed, S.S.; Anwar, K.S.; Akhtaruzzaman, S.M.; Salam, M.A. Recent outbreak of cutaneous anthrax in Bangladesh: Clinico-demographic profile and treatment outcome of cases attended at Rajshahi Medical College Hospital. BMC Res. Notes 2012, 5, 464. [Google Scholar] [CrossRef]
- Asanella, A.; Garofolo, G.; Hossain, M.J.; Shamsuddin, M.; Blackburn, J.; Hugh-Jones, M. Bangladesh anthrax outbreaks are probably caused by contaminated livestock feed. Epidemiol. Infect. 2013, 141, 1021–1028. [Google Scholar] [CrossRef]
- Islam, M.S.; Hossain, M.J.; Mikolon, A.; Parveen, S.; Khan, M.S.U.; Haider, N.; Chakraborty, A.; Titu, A.M.N.; Rahman, M.W.; Sazzad, H.M. Risk practices for animal and human anthrax in Bangladesh: An exploratory study. Infect. Ecol. Epidemiol. 2013, 3, 21356. [Google Scholar] [CrossRef] [PubMed]
- Hassan, J.; Ahsan, M.M.; Rahman, M.B.; Chowdhury, S.M.Z.H.; Parvej, M.S.; Nazir, K.N.H. Factors associated with repeated outbreak of anthrax in Bangladesh: Qualitative and quantitative study. J. Adv. Vet. Anim. Res. 2015, 2, 158–164. [Google Scholar] [CrossRef]
- World Health Organization. WHO Working Group Meeting on Anthrax Control and Research, with Special Reference to National Programme Development in Africa, Mongu, Zambia, 22–28 September 1992; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Siamudaala, V.M.; Bwalya, J.M.; Munang’andu, H.M.; Sinyangwe, P.G.; Banda, F.; Mweene, A.S.; Takada, A.; Kida, H. Ecology and epidemiology of anthrax in cattle and humans in Zambia. Jpn. J. Vet. Res. 2006, 54, 15–23. [Google Scholar] [PubMed]
- Hang’ombe, M.B.; Mwansa, J.C.; Muwowo, S.; Mulenga, P.; Kapina, M.; Musenga, E.; Squarre, D.; Mataa, L.; Thomas, S.Y.; Ogawa, H. Human-animal anthrax outbreak in the Luangwa valley of Zambia in 2011. Trop. Dr. 2012, 42, 136–139. [Google Scholar] [CrossRef]
- Turnbull, P.; Hugh-Jones, M.; Cosivi, O. World Health Organization activities on anthrax surveillance and control. J. Appl. Microbiol. 1999, 87, 318–320. [Google Scholar] [CrossRef]
- World Health Organization. WHO Working Group Meeting on Anthrax Control and Research, with Special Reference to National Program Development in Africa, Mongu, Zambia, 22–28 September 1992. In Proceedings of the Apresentado em: WHO Working Group Meeting on Anthrax Control and Research, Mongu, Zambia, 22–28 September 1992. [Google Scholar]
- Rosanna, A.; Michela, S.; Massimiliano, F.; Michela, I.; Adelia, D.; Antonio, F. Development of a Sterne-based complement fixation test to monitor the humoral response induced by anthrax vaccines. Front. Microbiol. 2016, 7, 19. [Google Scholar] [CrossRef]
- Dipti, M.; Rashid, M.; Ferdoush, M.; Roy, P.; Khan, M.; Hossain, M. Morphological and immunological characterization of anthrax vaccine in cattle. Bangladesh J. Vet. Med. 2013, 11, 43–49. [Google Scholar] [CrossRef]
- Roy, P.R.; Rashid, M.; Ferdoush, M.; Dipti, M.; Chowdury, M.; Mostofa, M.; Roy, S.; Khan, M.; Hossain, M. Biochemical and immunological characterization of anthrax spore vaccine in goat. Bangladesh J. Vet. Med. 2013, 11, 151–157. [Google Scholar] [CrossRef]
- Friedman, A.; Yakubu, A.-A. Anthrax epizootic and migration: Persistence or extinction. Math. Biosci. 2013, 241, 137–144. [Google Scholar] [CrossRef]
- Pantha, B.; Day, J.; Lenhart, S. Optimal control applied in an Anthrax epizootic model. J. Biol. Syst. 2016, 24, 495–517. [Google Scholar] [CrossRef]
- Osman, S.; Makinde, O.D.; Theuri, D.M. Mathematical modelling of transmission dynamics of anthrax in human and animal population. Math. Theory Model. 2018, 8, 47–67. [Google Scholar]
- Saadullah, M. Smallholder dairy production and marketing in Bangladesh. In Smallholder Dairy Production and Marketing-Opportunities and Constraints; NDDB (National Dairy Development Board) and ILRI (International Livestock Research Institute): Nairobi, Kenya, 2002; pp. 7–21. [Google Scholar]
- Shamsuddin, M.; Goodger, W.; Hossein, M.; Bennett, T.; Nordlund, K. A survey to identify economic opportunities for smallholder dairy farms in Bangladesh. Trop. Anim. Health Prod. 2006, 38, 131. [Google Scholar] [CrossRef] [PubMed]
- Rume, F.I.; Affuso, A.; Serrecchia, L.; Rondinone, V.; Manzulli, V.; Campese, E.; Di Taranto, P.; Biswas, P.K.; Ahsan, C.R.; Yasmin, M. Genotype analysis of Bacillus anthracis strains circulating in Bangladesh. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Thapa, N.K.; Tenzin, K.W.; Tshering Dorji, M.; Dorjee, J.; Marston, C.K.; Hoffmaster, A.R. Investigation and control of anthrax outbreak at the human–animal interface, Bhutan, 2010. Emerg. Infect. Dis. 2014, 20, 1524. [Google Scholar] [CrossRef] [PubMed]
- Gunaseelan, L.; Rishikesavan, R.; Adarsh, T.; Hamilton, R.B.E.; Kaneene, J. Temporal and geographical distribution of animal anthrax in Tamil Nadu state, India. Tamilnadu J. Vet. Anim. Sci. 2011, 7, 277–284. [Google Scholar]
- Sekar, N.; Shah, N.K.; Abbas, S.S.; Kakkar, M. Research options for controlling zoonotic disease in India, 2010–2015. PLoS ONE 2011, 6. [Google Scholar] [CrossRef]
- Yin, D.-P.; Wang, H.-Q.; Cao, L.-Q. Summary of EPI Vaccine all the World in 2006. Chin. J. Vaccines Immun. 2007, 3, 290–296. [Google Scholar]
- Ekanem, E.E. A 10-year review of morbidity from childhood preventable diseases in nigeria: How successful is the expanded programme of immunization (EPI)? J. Trop. Pediatr. 1988, 34, 323–328. [Google Scholar] [CrossRef]
- Dean, A.G. Epi Info and Epi Map: Current status and plans for Epi Info 2000. J. Public Health Manag. Pract. 1999, 5, 54–56. [Google Scholar] [CrossRef]
- Rahman, S.; Begum, I.A.; Alam, M.J. Livestock in Bangladesh: Distribution, growth, performance and potential. Livest. Res. Rural Dev. 2014, 26, 233–238. [Google Scholar]
- Riise, J.; Kryger, K.; Seeberg, D.; Christensen, P. Impact of smallholder poultry production in Bangladesh–12 years experience with Danida supported livestock projects in Bangladesh. Danida Minist. Foreign Aff. Cph. Den. 2005. preprint. [Google Scholar]
- Islam, M.; Samad, M. Mortality in chicks associated with economic impact and prospect of layer chick rearer package programme of the participatory livestock development project in Bangladesh. Int. J. Poult. Sci. 2004, 3, 119–123. [Google Scholar]
- Birtha, P.S. Technological Change in India’s Livestock Subsector: Evidence and Issues. In Proceedings of the Technology options for sustainable livestock production in India: Proceedings of the Workshop on Documentation, Adoption, and Impact of Livestock Technologies in India, ICRISAT, Patancheru, India, 18–19 January 2001; National Centre for Agricultural Economics: New Delhi, India; Policy Research and International Crops Research Institute for the Semi-Arid Tropics: Andhra Pradesh, India; p. 20. [Google Scholar]
- Kang, G.; Gunaseelan, L.; Abbas, K. Epidemiological dynamics of bovine brucellosis in India. Ann. Glob. Health 2015, 81, 127–128. [Google Scholar] [CrossRef]
- Kenyanjui, M.B.; Sheikh-Ali, M.; Ghaffar, A. Observations on cattle dairy breeds in Pakistan; need to curb unseen economic losses through control of mastitis and endemic diseases. J. Agric. Environ. Int. Dev. (JAEID) 2009, 103, 155–172. [Google Scholar]
- Ghaffar, A.; Ashfaq, F. Sustainable Goat Farming for Livelihood Improvement in Pakistan: Opportunities, Constrains, and Potential. In Sustainable Goat Farming for Livelihood Improvement in South Asia; SAARC Agriculture Centre: Dhaka, Bangladesh, 2017; pp. 69–98. [Google Scholar]
- Mushtaq, M.H.; Khattak, I.; Haqb, N.; Awan, F. Mass Vaccination and Surveillance Reduced the Burden of Foot and Mouth Disease. Veterinaria 2014, 2, 1–5. [Google Scholar]
- Nadeem, M.; Hussain, I.; Ahmad, T.; Qureshi, A.S.; Yousaf, A. Effect of Prophylactic Application of Levamisole in Buffalo-Calves Immunized with Haemorragic Septicemia Vaccine. Rev. Vet. 2010, 21, 447–450. [Google Scholar]
- Ahmed, B.-N.; Sultana, Y.; Fatema, D.; Ara, K.; Begum, N.; Mostanzid, S.; Jubayer, S. Anthrax: An emerging zoonotic disease in Bangladesh. Bangladesh J. Med. Microbiol. 2010, 4, 46–50. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| District | Spot | Cattle Population (MEAN ± SE) | Under 6 Months (MEAN ± SE) | Pregnant over 6 Months (MEAN ± SE) | Available Cattle for Vaccination (MEAN ± SE) | Actual Vaccinated (MEAN ± SE) | Unvaccinated (MEAN ± SE) | Percentage (%) |
|---|---|---|---|---|---|---|---|---|
| Mymensingh | 9 | 601 ± 68 | 74 ± 12 | 59 ± 9 | 468 ± 60 | 229 ± 31 | 239 ± 39 | 49 |
| Rajshahi | 9 | 542 ± 47 | 45 ± 6 | 33 ± 3 | 464 ± 48 | 205 ± 14 | 259 ± 41 | 47 |
| Joypurhat | 9 | 379 ± 53 | 60 ± 4 | 35 ± 5 | 284 ± 47 | 120 ± 17 | 164 ± 31 | 44 |
| Rangpur | 9 | 466 ± 44 | 72 ± 6 | 38 ± 3 | 356 ± 39 | 151 ± 14 | 205 ± 41 | 42 |
| Gaibandha | 9 | 633 ± 43 | 71 ± 8 | 45 ± 7 | 517 ± 49 | 206 ± 24 | 311 ± 33 | 40 |
| Dinajpur | 9 | 483 ± 34 | 75 ± 13 | 44 ± 3 | 364 ± 41 | 151 ± 15 | 213 ± 34 | 41 |
| Sherpur | 9 | 528 ± 59 | 88 ± 5 | 41 ± 3 | 399 ± 53 | 192 ± 25 | 207 ± 31 | 48 |
| Sirajganj | 9 | 613 ± 35 | 67 ± 6 | 37 ± 3 | 509 ± 32 | 203 ± 18 | 306 ± 28 | 39 |
| Location | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total | Percentage (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Information on FGDs | - | - | - | - | - | - | - | - | - | - |
| Number of FGDs | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 24 | - |
| Total number of participants | 24 | 27 | 21 | 33 | 33 | 24 | 24 | 30 | 216 | - |
| Recommendations identified | Number of participants identifying recommendation | - | ||||||||
| Individual Home delivery service | 18 | 18 | 9 | 27 | 18 | 9 | 18 | 9 | 126 | 58.33 |
| Arrange anthrax vaccination campaigns every 6 months | 9 | 18 | 9 | 9 | 27 | 9 | 9 | 27 | 117 | 54.16 |
| Inform farmers about the anthrax disease and how to control it | 9 | - | 9 | - | - | - | - | 9 | 27 | 12.5 |
| Inform farmers about the benefits of vaccination | 9 | - | - | - | 18 | 9 | 9 | 9 | 54 | 25 |
| Carry out additional research to study potential causes of reduction in milk production post-vaccination, and find solutions to the problem | - | 9 | - | - | - | 9 | - | 9 | 27 | 12.5 |
| Investigate whether or not vaccination causes infertility in animals | - | - | - | - | - | - | 9 | - | 9 | 4.16 |
| Investigate why swelling at the site of vaccination occurs and how it can be controlled | - | 9 | - | - | - | 9 | - | 9 | 27 | 12.5 |
| Study the causes of fever in animals after vaccination | - | - | 9 | - | - | - | 9 | - | 18 | 8.33 |
| Investigate apparent vaccination failure, leading to the reoccurrence of disease even after vaccination | 9 | 9 | 9 | 9 | 9 | 9 | - | - | 54 | 25 |
| Increase the number of veterinarians, vaccinators or skilled staff | 18 | 9 | 9 | 18 | 9 | 9 | 18 | 9 | 99 | 45.83 |
| Establish a reliable cold chain to store and transport vaccines | 9 | 9 | - | - | - | - | 9 | 9 | 36 | 16.66 |
| Properly store and follow the expiry date of vaccines in Upazilla livestock office | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 72 | 33.33 |
| Carry out research to produce vaccines that can be stored at room temperature (thermostable/thermotolerant). | 9 | 9 | 9 | - | - | - | - | - | 27 | 12.5 |
| Free of charge vaccinations | - | - | - | 9 | - | - | - | - | 9 | 4.16 |
| Increase collaboration of Livestock Local vaccinators with veterinarians and Livestock department | 9 | - | - | - | - | - | - | 9 | 18 | 8.33 |
| Impose fine or punishment if failing to vaccinate | - | 9 | - | - | - | 9 | - | - | 18 | 8.33 |
| Involve law enforcing agencies and local administration | - | - | - | 9 | - | - | 9 | - | 18 | 8.33 |
| Location | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | Total | Percentage (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Information on Validation Workshop | - | - | - | - | - | - | - | - | - | - |
| Number of validation workshop | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | - |
| Total number of participants | 57 | 53 | 52 | 54 | 48 | 47 | 51 | 39 | 401 | - |
| Recommendations identified | Number of participants identifying recommendation | - | ||||||||
| Vaccine should be more effective | 12 | 20 | 8 | 13 | 7 | 6 | 18 | 8 | 92 | 22.9 |
| Lack of knowledge and poor attitude by cattle farmers | 6 | 6 | 7 | 8 | 5 | 4 | 7 | 3 | 46 | 11.4 |
| Farmer are not willing to pay the vaccination cost | 6 | 5 | 6 | 8 | 10 | 4 | 1 | 2 | 42 | 10.5 |
| Lack of Coordination between demand and vaccine supply | 12 | 4 | 5 | 3 | - | 7 | 10 | 5 | 46 | 11.2 |
| Shortage of Manpower in Livestock sector | 13 | 10 | 14 | 7 | 9 | 8 | 23 | 6 | 90 | 22.5 |
| Poor extension services | 11 | 18 | 6 | 18 | 11 | 13 | 2 | 6 | 85 | 21.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarker, M.S.A.; El Zowalaty, M.E.; Shahid, M.A.H.; Sarker, M.A.; Rahman, M.B.; Järhult, J.D.; Nazir, K.H.M.N.H. Maximization of Livestock Anthrax Vaccination Coverage in Bangladesh: An Alternative Approach. Vaccines 2020, 8, 435. https://doi.org/10.3390/vaccines8030435
Sarker MSA, El Zowalaty ME, Shahid MAH, Sarker MA, Rahman MB, Järhult JD, Nazir KHMNH. Maximization of Livestock Anthrax Vaccination Coverage in Bangladesh: An Alternative Approach. Vaccines. 2020; 8(3):435. https://doi.org/10.3390/vaccines8030435
Chicago/Turabian StyleSarker, M. Shahjahan A., Mohamed E. El Zowalaty, M. Ahosanul Haque Shahid, M. Asaduzzaman Sarker, M. Bahanur Rahman, Josef D. Järhult, and K. H. M. Nazmul Hussain Nazir. 2020. "Maximization of Livestock Anthrax Vaccination Coverage in Bangladesh: An Alternative Approach" Vaccines 8, no. 3: 435. https://doi.org/10.3390/vaccines8030435
APA StyleSarker, M. S. A., El Zowalaty, M. E., Shahid, M. A. H., Sarker, M. A., Rahman, M. B., Järhult, J. D., & Nazir, K. H. M. N. H. (2020). Maximization of Livestock Anthrax Vaccination Coverage in Bangladesh: An Alternative Approach. Vaccines, 8(3), 435. https://doi.org/10.3390/vaccines8030435