Measles Immunization Policies and Vaccination Coverage in EU/EEA Countries over the Last Decade




Abstract
1. Introduction
2. Materials and Methods
3. Results
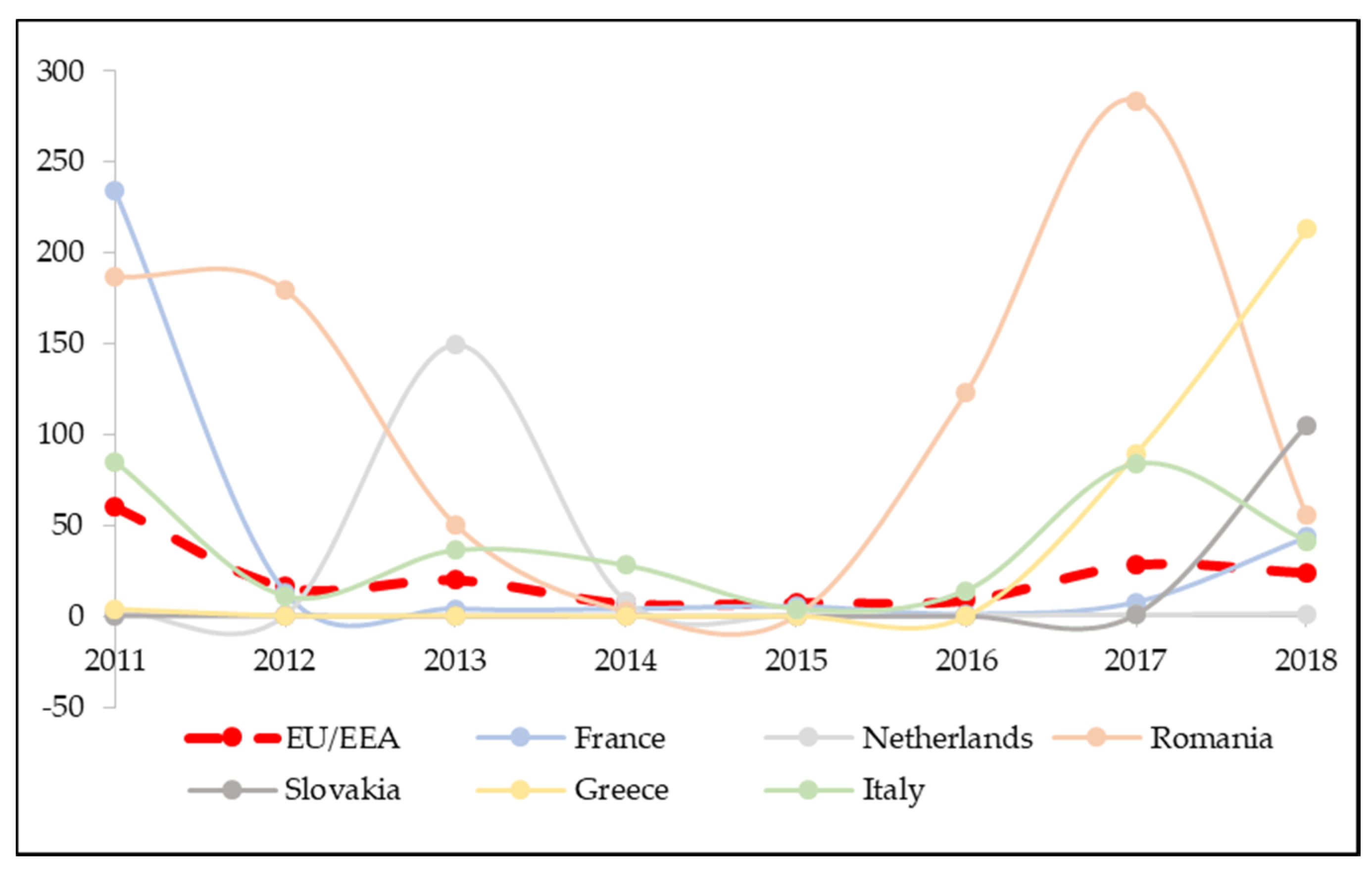
3.1. Incidence of Measles in Europe
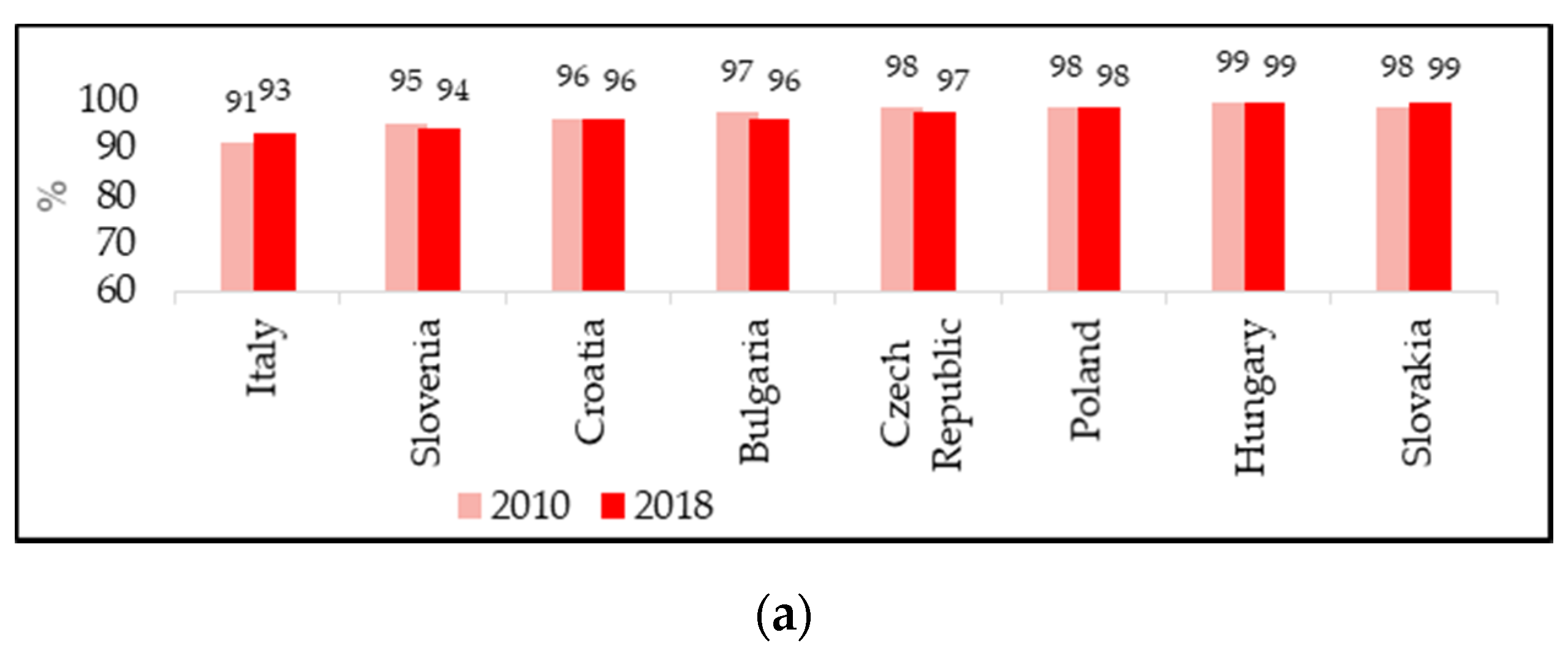
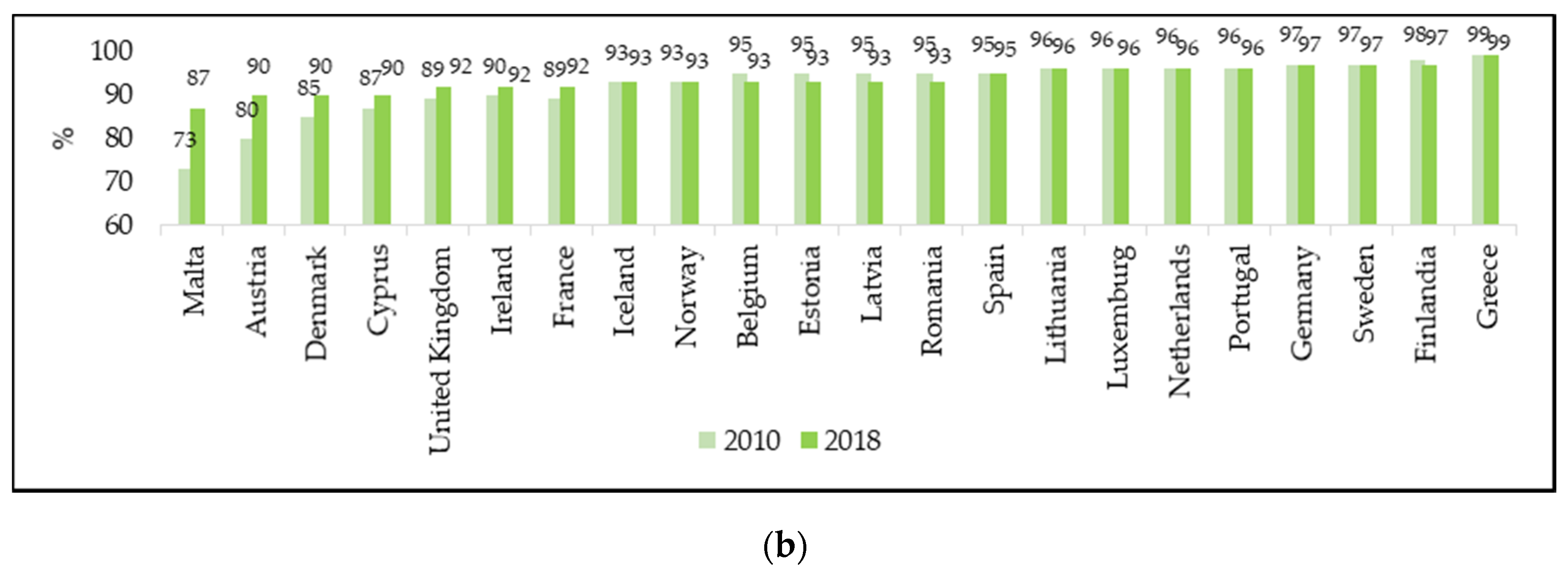
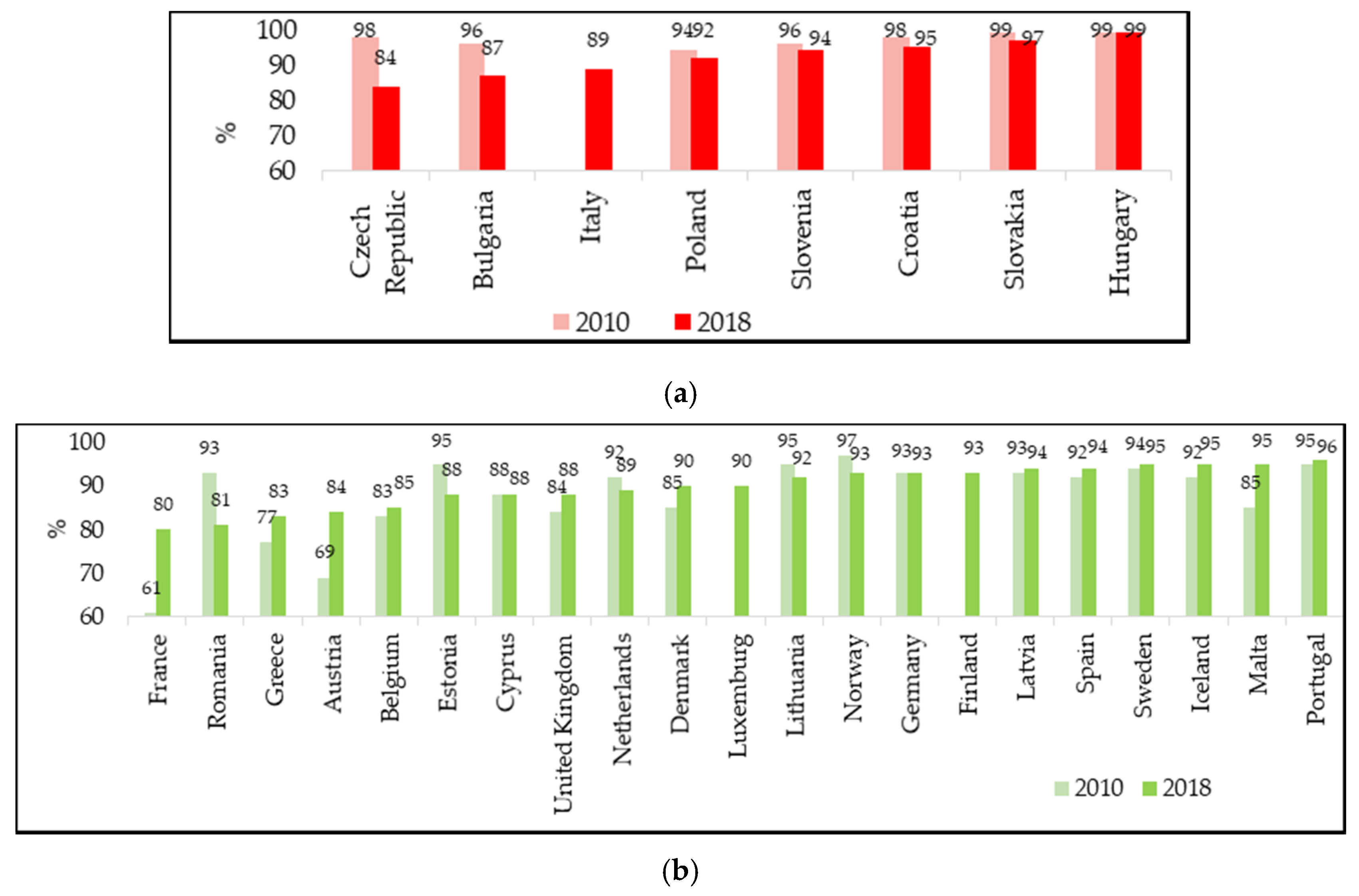
3.2. Measles Vaccination Coverage in Europe
3.3. Comparison between Countries with Different Vaccination Policies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Global Measles and Rubella Strategic Plan: 2012–2020; WHO Press: Geneva, Switzerland, 2012; ISBN 978-92-4-150339-6. [Google Scholar]
- Orenstein, W.A.; Cairns, L.; Hinman, A.; Nkowane, B.; Olivé, J.-M.; Reingold, A.L. Measles and Rubella Global Strategic Plan 2012–2020 midterm review report: Background and summary. Vaccine 2018, 36, A35–A42. [Google Scholar] [CrossRef]
- Magurano, F.; Baggieri, M.; Mazzilli, F.; Bucci, P.; Marchi, A.; Nicoletti, L. MoRoNet Group Measles in Italy: Viral strains and crossing borders. Int. J. Infect. Dis. 2019, 79, 199–201. [Google Scholar] [CrossRef]
- Komitova, R.; Kevorkyan, A.; Boykinova, O.; Krumova, S.; Atanasova, M.; Raycheva, R.; Stoilova, Y.; Kunchey, A. Difficulties in achieving and maintaining the goal of measles elimination in Bulgaria. Rev. D’Épidémiol. Santé Publique 2019, 67, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Rovida, F.; Brianese, N.; Piralla, A.; Sarasini, A.; Girello, A.; Giardina, F.; Cassaniti, I.; Fornabaio, C.; Seminari, E.; Monteverdi, A.; et al. Outbreak of measles genotype H1 in Northern Italy originated from a case imported from Southeast Asia, 2017. Clin. Microbiol. Infect. 2019, 25, 526–528. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Publications & Data. Available online: https://www.ecdc.europa.eu/en/publications-data (accessed on 10 December 2019).
- WHO. New Measles Surveillance Data from WHO. Available online: http://www.who.int/immunization/newsroom/new-measles-data-august-2019/en/ (accessed on 10 December 2019).
- MacDonald, N.E. SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Who Is at Risk for Measles in the EU/EEA? Identifying Susceptible Groups to Close Immunity Gaps towards Measles Elimination. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/RRA-Measles-EU-EEA-May-2019.pdf (accessed on 10 December 2019).
- ECDC. Vaccine Scheduler. Available online: https://vaccine-schedule.ecdc.europa.eu/ (accessed on 10 December 2019).
- Haverkate, M.; D’Ancona, F.; Giambi, C.; Johansen, K.; Lopalco, P.L.; Cozza, V.; Appelgren, E. On behalf of the VENICE project gatekeepers and contact points. Mandatory and recommended vaccination in the EU, Iceland and Norway: Results of the VENICE 2010 survey on the ways of implementing national vaccination programmes. Euro Surveill. 2012, 17, 20183. [Google Scholar] [CrossRef] [PubMed]
- WHO. Measles and Rubella Surveillance Data. Available online: http://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/active/measles_monthlydata/en/ (accessed on 10 December 2019).
- Anonymous. Slovakia: Measles Epidemic Spreads Again. Available online: https://spectator.sme.sk/c/22018568/measles-epidemic-spreads-in-eastern-slovakia-again.html (accessed on 10 December 2019).
- Sowa, P.M. Governance of Hospital in Central and Eastern Europe; Springer: Singapore, 2016; ISBN 978-981-287-765-9. [Google Scholar]
- Ministero della Salute. Vaccinazioni dell’età Pediatrica e dell’Adolescente-Coperture Vaccinali. Available online: http://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=20 (accessed on 10 December 2019).
- Patel, M.K. Progress toward Regional Measles Elimination—Worldwide, 2000–2018. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1323. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. Decreto legge 7 giugno 2017, n. 73, Disposizioni urgenti in materia di prevenzione vaccinale, come modificato dalla Legge di conversione 31 luglio 2017, n. 119. G.U. Serie Generale n.182 del 05/08/2017. Available online: https://www.gazzettaufficiale.it/eli/id/2017/08/05/17A05515/sg (accessed on 10 December 2019).
- Trentini, F.; Poletti, P.; Melegaro, A.; Merler, S. The introduction of ‘No jab, No school’ policy and the refinement of measles immunisation strategies in high-income countries. BMC Med. 2019, 17, 86. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. Piano Nazionale Prevenzione Vaccinale 2017–2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 10 December 2019).
- Società Italiana di Farmacologia. I Vaccini e le Vaccinazioni. Available online: https://sif-website.s3.amazonaws.com/uploads/document/attachment/24/sif_position_paper_vaccini_vaccinazioni_feb17.pdf (accessed on 10 December 2019).
- MacDonald, N.E.; Harmon, S.; Dube, E.; Steenbeek, A.; Crowcroft, N.; Opel, D.J.; Faour, D.; Leask, J.; Butler, R. Mandatory infant & childhood immunization: Rationales, issues and knowledge gaps. Vaccine 2018, 36, 5811–5818. [Google Scholar] [PubMed]
- Omer, S.B.; Betsch, C.; Leask, J. Mandate vaccination with care. Nature 2019, 571, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Aquino, F.; Donzelli, G.; De Franco, E.; Privitera, G.; Lopalco, P.L.; Carducci, A. The web and public confidence in MMR vaccination in Italy. Vaccine 2017, 35, 4494–4498. [Google Scholar] [CrossRef] [PubMed]
- Tavoschi, L.; Quattrone, F.; De Vita, E.; Lopalco, P.L. Impact of mandatory law on vaccine hesitancy spectrum: The case of measles vaccine catch-up activities in Tuscany, Italy. Vaccine 2019, 37, 7201–7202. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Public Health Romania. Measles Situation Reports in Romania. Available online: http://www.cnscbt.ro/index.php/informari-saptamanale/rujeola-1 (accessed on 10 December 2019).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Measles Cases per Million | |||||||
|---|---|---|---|---|---|---|---|---|
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | |
| Austria | 12 | 2.3 | 8.9 | 13.3 | 35.2 | 3.1 | 10.9 | 8.8 |
| Belgium | 51 | 3.9 | 3.4 | 6.3 | 4.2 | 7.1 | 32.5 | 10.6 |
| Bulgaria | 21 | 0.1 | 2.2 | 0 | 0 | 0.1 | 23.2 | 1.8 |
| Croatia | n.a. | n.a. | 0.2 | 3.3 | 51.6 | 1.0 | 1.7 | 5.5 |
| Cyprus | 0 | 1.2 | 0 | 11.6 | 0 | 0 | 3.5 | 17.6 |
| Czech Republic | 2 | 2.1 | 1.3 | 21.1 | 0.9 | 0.7 | 13.8 | 19.1 |
| Denmark | 15 | 0.4 | 3.0 | 5.2 | 1.6 | 0.5 | 0.7 | 1.4 |
| Estonia | 5 | 3.0 | 1.5 | 0 | 3.0 | 1.5 | 0.8 | 7.6 |
| Finland | 5 | 0.9 | 0.4 | 0.6 | 0.2 | 0.7 | 1.8 | 2.7 |
| France | 234 | 13.2 | 4.2 | 4.1 | 5.5 | 1.2 | 7.8 | 43.5 |
| Germany | 20 | 2.0 | 21.7 | 5.4 | 30.5 | 4.0 | 11.3 | 6.6 |
| Greece | 4 | 0.3 | 0.3 | 0.1 | 0.1 | 0 | 89.7 | 212.9 |
| Hungary | 1 | 0.2 | 0.1 | 0 | 0 | 0 | 3.7 | 1.4 |
| Iceland | 0 | 0 | 0 | 3.1 | 0 | 3.0 | 9.0 | 0 |
| Ireland | 68 | 23.9 | 12.4 | 9.1 | 1.5 | 9.3 | 5.3 | 18.8 |
| Italy | 85 | 11.2 | 36.4 | 28.1 | 4.1 | 14.2 | 84.0 | 41.5 |
| Latvia | 0.4 | 1.3 | 0 | 17.8 | 0 | 0 | 0 | 12.8 |
| Lithuania | 2 | 0.6 | 11.6 | 3.7 | 17.0 | 7.6 | 0.7 | 10.5 |
| Luxemburg | 12 | 3.9 | 0 | 3.7 | 0 | 0 | 6.9 | 6.8 |
| Malta | 10 | 0 | 4.8 | 0 | 2.4 | 0 | 0 | 10.9 |
| Netherlands | 3 | 0.6 | 149.4 | 8.6 | 0.4 | 0.4 | 0.9 | 1.4 |
| Norway | 8 | 0.8 | 1.6 | 0.6 | 2.7 | 0 | 0.2 | 2.3 |
| Poland | 1 | 1.6 | 2.2 | 2.9 | 1.2 | 3.5 | 1.7 | 8.9 |
| Portugal | 0.2 | 0.7 | 0.1 | 0 | 0 | 0 | 3.3 | 16.6 |
| Romania | 187 | 179.5 | 50.3 | 2.6 | 0.2 | 123.1 | 283.8 | 55.3 |
| Slovakia | 0.4 | 0.2 | 0 | 0 | 0 | 0 | 1.1 | 105.2 |
| Slovenia | 11 | 1 | 0.5 | 25.3 | 8.7 | 0.5 | 3.4 | 4.4 |
| Spain | 43 | 9.7 | 2.7 | 3.3 | 1 | 0.8 | 3.5 | 4.8 |
| Sweden | 3 | 3.2 | 5.5 | 2.7 | 2.3 | 0.3 | 4.2 | 4.3 |
| United Kingdom | 17 | 30.4 | 30.7 | 2.1 | 1.4 | 8.7 | 4.3 | 14.5 |
| EU/EEA | 60 | 16.2 | 20.1 | 7.1 | 7.7 | 9.0 | 28.3 | 23.9 |
| Country | Variation in Vaccination Coverage for the Second Dose of Measles-Containing Vaccine (%) | ||
|---|---|---|---|
| 2010–2018 | 2010–2016 | 2016–2018 | |
| Czech Republic | −14 | −5 | −9 |
| Romania | −12 | −17 | +5 |
| Bulgaria | −9 | −8 | −1 |
| Estonia | −7 | −3 | −4 |
| Norway | −4 | −6 | +2 |
| Netherlands | −3 | −1 | −2 |
| Croatia | −3 | −2 | −1 |
| Lithuania | −3 | −3 | 0 |
| Poland | −2 | −1 | −1 |
| Slovakia | −2 | −2 | 0 |
| Slovenia | −2 | −3 | +1 |
| Cyprus | 0 | 0 | 0 |
| Germany | 0 | 0 | 0 |
| Hungary | 0 | 0 | 0 |
| Sweden | +1 | +1 | 0 |
| Portugal | +1 | 0 | +1 |
| Latvia | +1 | −4 | +5 |
| Spain | +2 | +3 | −1 |
| Belgium | +2 | +2 | 0 |
| Iceland | +3 | +3 | 0 |
| United Kingdom | +4 | +5 | −1 |
| Denmark | +5 | 0 | +5 |
| Greece | +6 | +6 | 0 |
| Malta | +10 | +1 | +9 |
| Austria | +15 | +20 | −5 |
| France | +19 | +19 | 0 |
| Luxemburg | n.a. | n.a. | +4 |
| Italy | n.a. | n.a. | +7 |
| Finland | n.a. | n.a. | +8 |
| Ireland | n.a. | n.a. | n.a. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montalti, M.; Kawalec, A.; Leoni, E.; Dallolio, L. Measles Immunization Policies and Vaccination Coverage in EU/EEA Countries over the Last Decade. Vaccines 2020, 8, 86. https://doi.org/10.3390/vaccines8010086
Montalti M, Kawalec A, Leoni E, Dallolio L. Measles Immunization Policies and Vaccination Coverage in EU/EEA Countries over the Last Decade. Vaccines. 2020; 8(1):86. https://doi.org/10.3390/vaccines8010086
Chicago/Turabian StyleMontalti, Marco, Anna Kawalec, Erica Leoni, and Laura Dallolio. 2020. "Measles Immunization Policies and Vaccination Coverage in EU/EEA Countries over the Last Decade" Vaccines 8, no. 1: 86. https://doi.org/10.3390/vaccines8010086
APA StyleMontalti, M., Kawalec, A., Leoni, E., & Dallolio, L. (2020). Measles Immunization Policies and Vaccination Coverage in EU/EEA Countries over the Last Decade. Vaccines, 8(1), 86. https://doi.org/10.3390/vaccines8010086