Sex-Specific Differences in HLA Antibodies after Pneumococcal Vaccination in Kidney Transplant Recipients

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Vaccine
2.3. Determination of HLA and MICA Antibodies
2.4. Determination of Antibodies Against Pneumococci
2.5. Statistical Analysis
3. Results
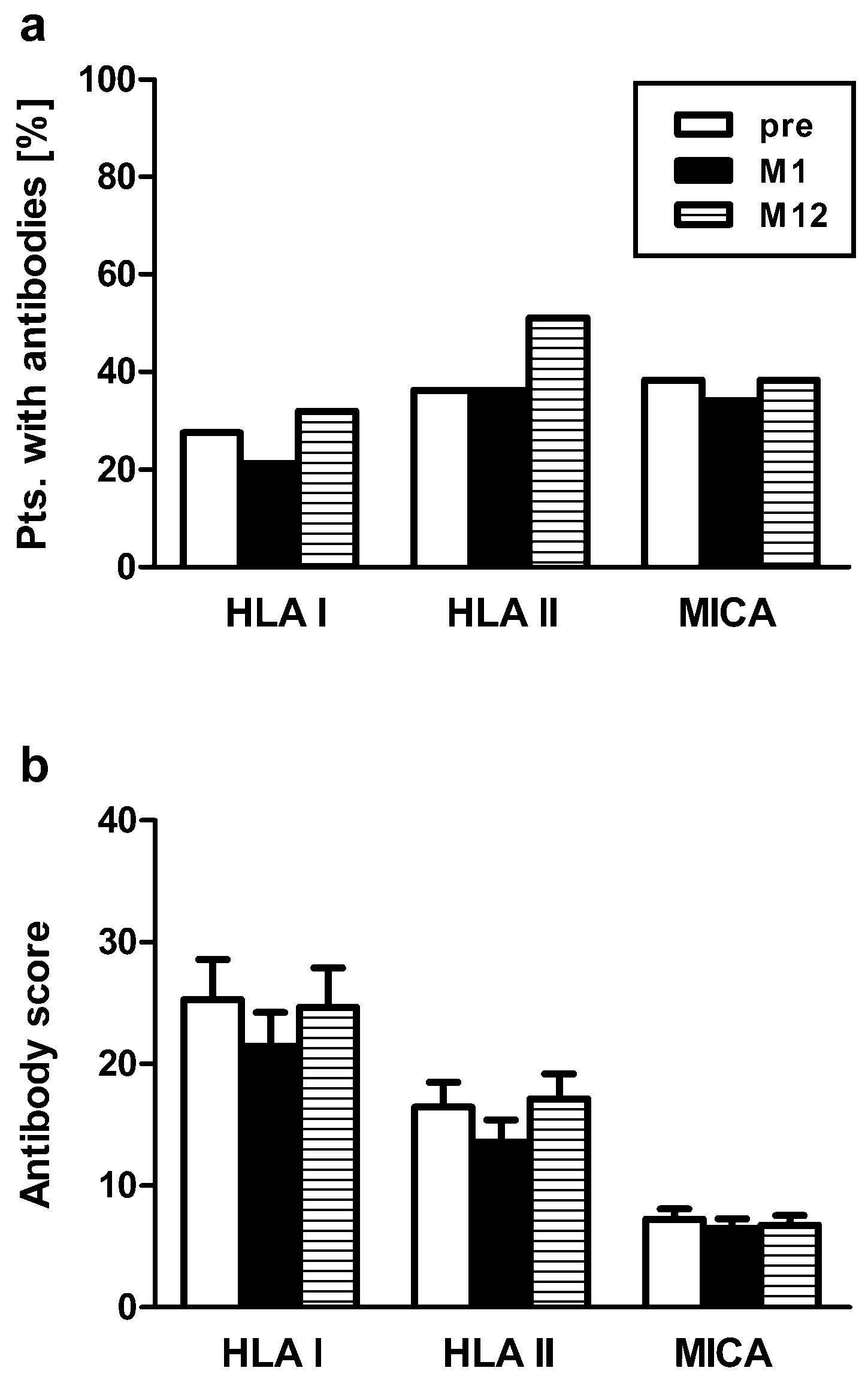
3.1. HLA and MICA Antibodies After Pneumococcal Vaccination
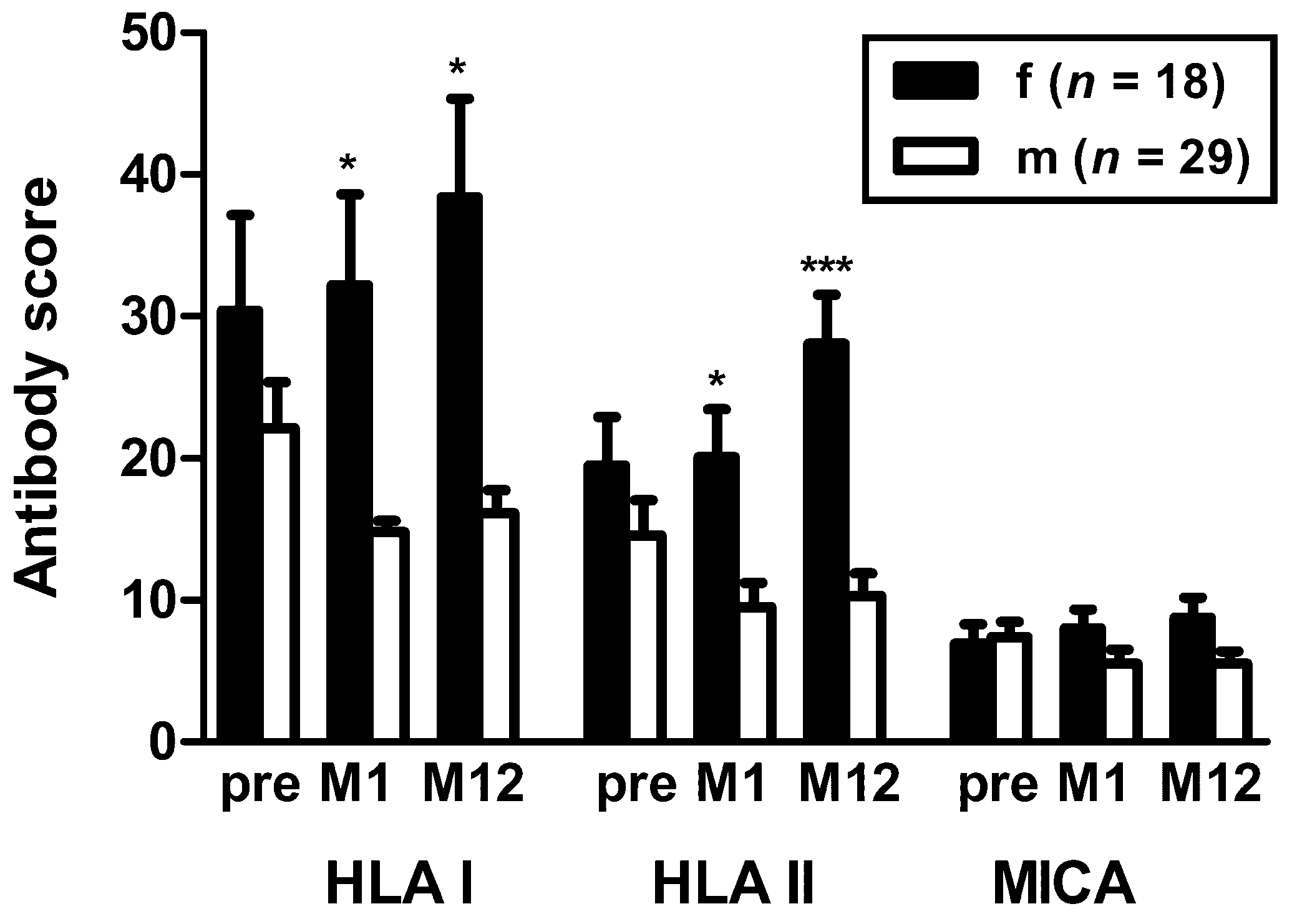
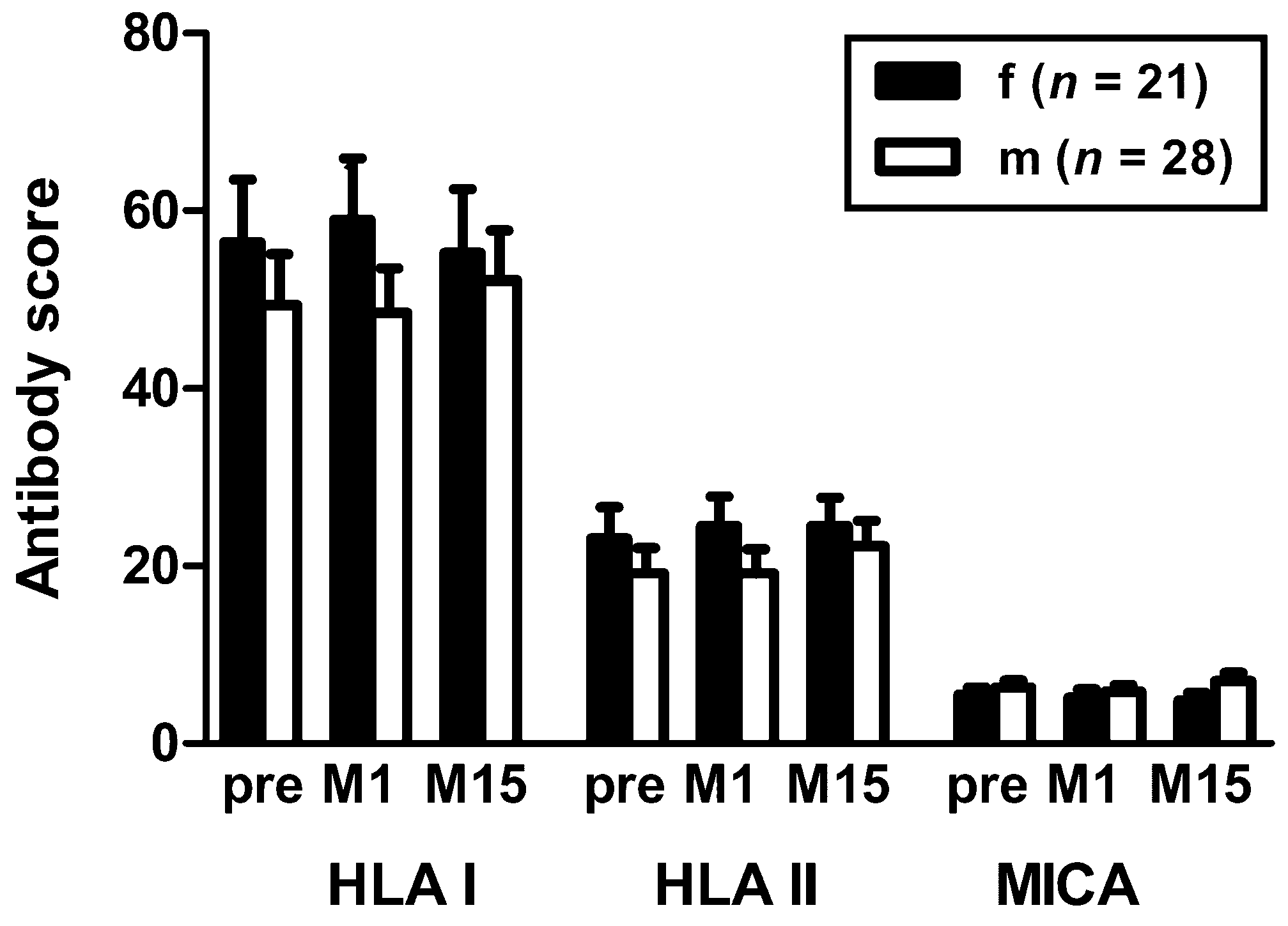
3.2. Sex-Specific Differences in HLA Antibodies
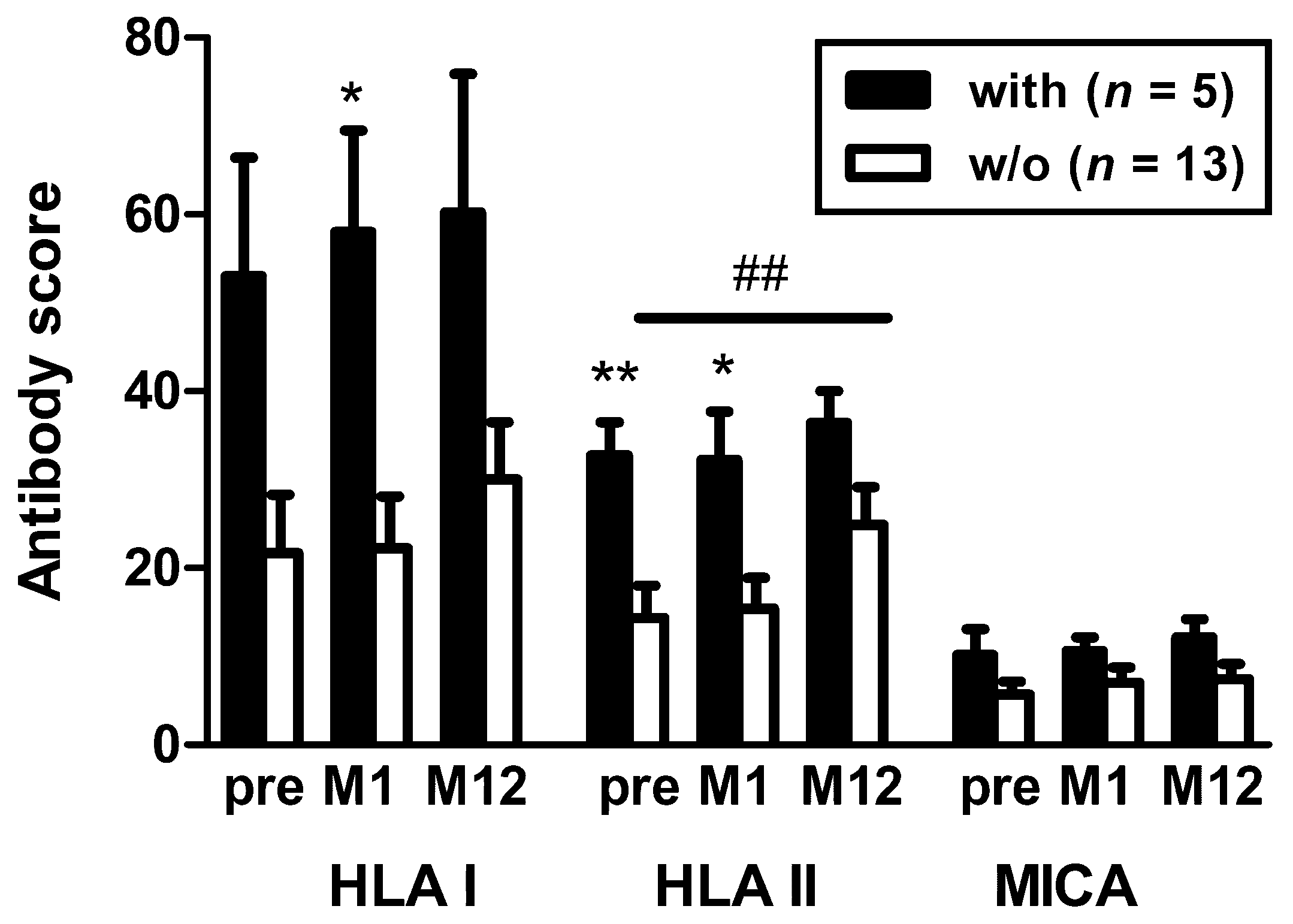
3.3. Correlation of Additional Clinical Parameters and Antibodies
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Simell, B.; Auranen, K.; Kayhty, H.; Goldblatt, D.; Dagan, R.; O’Brien, K.L. Pneumococcal Carriage Group. The fundamental link between pneumococcal carriage and disease. Expert Rev. Vaccines 2012, 11, 841–855. [Google Scholar] [CrossRef]
- Klugman, K.P.; Chien, Y.W.; Madhi, S.A. Pneumococcal pneumonia and influenza: A deadly combination. Vaccine 2009, 27 (Suppl. 3), C9–C14. [Google Scholar] [CrossRef] [PubMed]
- National Vaccine Program Office. Adult Immunization Plans. Available online: http://www.hhs.gov/nvpo/national-adult-immunization-plan/ (accessed on 19 June 2019).
- Arora, S.; Kipp, G.; Bhanot, N.; Sureshkumar, K.K. Vaccinations in kidney transplant recipients: Clearing the muddy waters. World J. Transplant. 2019, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Use of 13-Valent Pneumococcal Conjugate Vaccine and 23-Valent Pneumococcal Polysaccharide Vaccine for Adults with Immunocompromising Conditions: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2012, 61, 816–819. [Google Scholar]
- Robert-Koch-Institut. Wissenschaftliche Begründung für die Aktualisierung der Empfehlungen zur Indikationsimpfung gegen Pneumokokken für Risikogruppen. Epid. Bull. 2016, 37, 385–406. [Google Scholar]
- Bonten, M.J.; Huijts, S.M.; Bolkenbaas, M.; Webber, C.; Patterson, S.; Gault, S.; van Werkhoven, C.H.; van Deursen, A.M.; Sanders, E.A.; Verheij, T.J.; et al. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N. Engl. J. Med. 2015, 372, 1114–1125. [Google Scholar] [CrossRef]
- Hurst, F.P.; Lee, J.J.; Jindal, R.M.; Agodoa, L.Y.; Abbott, K.C. Outcomes associated with influenza vaccination in the first year after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2011, 6, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Scharpe, J.; Evenepoel, P.; Maes, B.; Bammens, B.; Claes, K.; Osterhaus, A.D.; Vanrenterghem, Y.; Peetermans, W.E. Influenza vaccination is efficacious and safe in renal transplant recipients. Am. J. Transplant. 2008, 8, 332–337. [Google Scholar] [CrossRef]
- Connolly, J.; Douglas, J.; Kumar, R.; Middleton, D.; McEvoy, J.; Nelson, S.; McGeown, M.G. Letter: Influenza virus vaccination and renal transplant rejection. Br. Med. J. 1974, 1, 638. [Google Scholar] [CrossRef]
- Cainelli, F.; Vento, S. Infections and solid organ transplant rejection: A cause-and-effect relationship? Lancet Infect. Dis. 2002, 2, 539–549. [Google Scholar] [CrossRef]
- Candon, S.; Thervet, E.; Lebon, P.; Suberbielle, C.; Zuber, J.; Lima, C.; Charron, D.; Legendre, C.; Chatenoud, L. Humoral and cellular immune responses after influenza vaccination in kidney transplant recipients. Am. J. Transplant. 2009, 9, 2346–2354. [Google Scholar] [CrossRef] [PubMed]
- Brakemeier, S.; Schweiger, B.; Lachmann, N.; Glander, P.; Schonemann, C.; Diekmann, F.; Neumayer, H.H.; Budde, K. Immune response to an adjuvanted influenza A H1N1 vaccine (Pandemrix((R))) in renal transplant recipients. Nephrol. Dial. Transplant. 2012, 27, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Lindemann, M.; Heinemann, F.M.; Horn, P.A.; Witzke, O. Vaccination against Streptococcus pneumoniae does not induce antibodies against HLA or MICA in clinically stable kidney transplant recipients. Hum. Immunol. 2013, 74, 1267–1270. [Google Scholar] [CrossRef] [PubMed]
- Marino, L.; Alberu, J.; Morales-Buenrostro, L.E. Influenza Immunization and the Generation of Anti-HLA and Anti-MICA Antibodies in Patients with Renal Failure and in Kidney Transplant Recipients. Clin. Transpl. 2016, 32, 161–171. [Google Scholar] [PubMed]
- Broeders, N.E.; Hombrouck, A.; Lemy, A.; Wissing, K.M.; Racape, J.; Gastaldello, K.; Massart, A.; Van Gucht, S.; Weichselbaum, L.; De Mul, A.; et al. Influenza A/H1N1 vaccine in patients treated by kidney transplant or dialysis: A cohort study. Clin. J. Am. Soc. Nephrol. 2011, 6, 2573–2578. [Google Scholar] [CrossRef] [PubMed]
- Mond, J.J.; Lees, A.; Snapper, C.M. T cell-independent antigens type 2. Annu. Rev. Immunol. 1995, 13, 655–692. [Google Scholar] [CrossRef] [PubMed]
- Dendle, C.; Stuart, R.L.; Polkinghorne, K.R.; Balloch, A.; Kanellis, J.; Ling, J.; Kummrow, M.; Moore, C.; Thursky, K.; Buttery, J.; et al. Seroresponses and safety of 13-valent pneumococcal conjugate vaccination in kidney transplant recipients. Transpl. Infect. Dis. 2018, 20, e12866. [Google Scholar] [CrossRef]
- David-Neto, E.; Triboni, A.H.; Ramos, F.; Agena, F.; Galante, N.Z.; Altona, M.; Lemos, F.B.; Sapienza, M.T.; Nahas, W.C. Evaluation of MDRD4, CKD-EPI, BIS-1, and modified Cockcroft-Gault equations to estimate glomerular filtration rate in the elderly renal-transplanted recipients. Clin. Transplant. 2016, 30, 1558–1563. [Google Scholar] [CrossRef]
- Heinemann, F.M. HLA Genotyping and Antibody Characterization Using the Luminex Multiplex Technology. Transfus. Med. Hemother. 2009, 36, 273–278. [Google Scholar] [CrossRef]
- Heinemann, F.M.; Roth, I.; Rebmann, V.; Arnold, M.L.; Witzke, O.; Wilde, B.; Spriewald, B.M.; Grosse-Wilde, H. Immunoglobulin isotype-specific characterization of anti-human leukocyte antigen antibodies eluted from explanted renal allografts. Hum. Immunol. 2007, 68, 500–506. [Google Scholar] [CrossRef]
- Lindemann, M.; Lenz, V.; Nyadu, B.; Heinemann, F.M.; Heinold, A.; Guberina, H.; Eisenberger, U.; Lachmann, N.; Schonemann, C.; Kribben, A.; et al. Effect of ABO incompatibility on T-cell flow cytometry cross-match results prior to living donor kidney transplantation. Cytom. B Clin. Cytom. 2018, 94, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Adey, D.B. Women and kidney transplantation. Adv. Chronic. Kidney Dis. 2013, 20, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Picascia, A.; Grimaldi, V.; Sabia, C.; Napoli, C. Comprehensive assessment of sensitizing events and anti-HLA antibody development in women awaiting kidney transplantation. Transpl. Immunol. 2016, 36, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Chowdhry, M.; Makroo, R.N.; Singh, M.; Kumar, M.; Thakur, Y.; Sharma, V. Role of Anti-MICA Antibodies in Graft Survival of Renal Transplant Recipients of India. J. Immunol. Res. 2018, 2018, 3434050. [Google Scholar] [CrossRef]
- Klein, S.L. Sex influences immune responses to viruses, and efficacy of prophylaxis and treatments for viral diseases. Bioessays 2012, 34, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Bernin, H.; Fehling, H.; Marggraff, C.; Tannich, E.; Lotter, H. The cytokine profile of human NKT cells and PBMCs is dependent on donor sex and stimulus. Med. Microbiol. Immunol. 2016, 205, 321–332. [Google Scholar] [CrossRef]
- Di Benedetto, S.; Derhovanessian, E.; Steinhagen-Thiessen, E.; Goldeck, D.; Muller, L.; Pawelec, G. Impact of age, sex and CMV-infection on peripheral T cell phenotypes: Results from the Berlin BASE-II Study. Biogerontology 2015, 16, 631–643. [Google Scholar] [CrossRef]
- Villacres, M.C.; Longmate, J.; Auge, C.; Diamond, D.J. Predominant type 1 CMV-specific memory T-helper response in humans: Evidence for gender differences in cytokine secretion. Hum. Immunol. 2004, 65, 476–485. [Google Scholar] [CrossRef]
- Lindemann, M.; Korth, J.; Sun, M.; Xu, S.; Struve, C.; Werner, K.; Dornieden, T.; Horn, P.A.; Witzke, O.; Wilde, B. The Cytomegalovirus-Specific IL-21 ELISpot Correlates with Allograft Function of Kidney Transplant Recipients. Int. J. Mol. Sci. 2018, 19, 3945. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Boef, A.G.C.; van der Klis, F.R.M.; Berbers, G.A.M.; Buisman, A.M.; Sanders, E.A.M.; Kemmeren, J.M.; van der Ende, A.; de Melker, H.E.; Rots, N.Y.; Knol, M.J. Differences by sex in IgG levels following infant and childhood vaccinations: An individual participant data meta-analysis of vaccination studies. Vaccine 2018, 36, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Giefing-Kroll, C.; Berger, P.; Lepperdinger, G.; Grubeck-Loebenstein, B. How sex and age affect immune responses, susceptibility to infections, and response to vaccination. Aging Cell 2015, 14, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Burrows, S.R.; Silins, S.L.; Khanna, R.; Burrows, J.M.; Rischmueller, M.; McCluskey, J.; Moss, D.J. Cross-reactive memory T cells for Epstein-Barr virus augment the alloresponse to common human leukocyte antigens: Degenerate recognition of major histocompatibility complex-bound peptide by T cells and its role in alloreactivity. Eur. J. Immunol. 1997, 27, 1726–1736. [Google Scholar] [CrossRef]
- Kumar, D.; Welsh, B.; Siegal, D.; Chen, M.H.; Humar, A. Immunogenicity of pneumococcal vaccine in renal transplant recipients—Three year follow-up of a randomized trial. Am. J. Transplant. 2007, 7, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Willcocks, L.C.; Chaudhry, A.N.; Smith, J.C.; Ojha, S.; Doffinger, R.; Watson, C.J.; Smith, K.G. The effect of sirolimus therapy on vaccine responses in transplant recipients. Am. J. Transplant. 2007, 7, 2006–2011. [Google Scholar] [CrossRef]
- Morel, S.; Didierlaurent, A.; Bourguignon, P.; Delhaye, S.; Baras, B.; Jacob, V.; Planty, C.; Elouahabi, A.; Harvengt, P.; Carlsen, H.; et al. Adjuvant System AS03 containing alpha-tocopherol modulates innate immune response and leads to improved adaptive immunity. Vaccine 2011, 29, 2461–2473. [Google Scholar] [CrossRef]
- Kedl, J.D.; Kedl, R.M. How squalene GLAdly helps generate antigen-specific T cells via antigen-carrying neutrophils and IL-18. Eur. J. Immunol. 2015, 45, 376–379. [Google Scholar] [CrossRef]
- Locke, J.E.; Zachary, A.A.; Warren, D.S.; Segev, D.L.; Houp, J.A.; Montgomery, R.A.; Leffell, M.S. Proinflammatory events are associated with significant increases in breadth and strength of HLA-specific antibody. Am. J. Transplant. 2009, 9, 2136–2139. [Google Scholar] [CrossRef]
- Terasaki, P.I. A personal perspective: 100-year history of the humoral theory of transplantation. Transplantation 2012, 93, 751–756. [Google Scholar] [CrossRef]
- Iwaki, Y.; Terasaki, P.I. Sensitization effect. Clin. Transpl. 1986, 257–265. Available online: https://www.ncbi.nlm.nih.gov/pubmed/3154413 (accessed on 19 June 2019).
- Terasaki, P.I. Humoral theory of transplantation. Am. J. Transpl. 2003, 3, 665–673. [Google Scholar] [CrossRef]
- Cai, J.; Qing, X.; Tan, J.; Terasaki, P.I. Humoral theory of transplantation: Some hot topics. Br. Med. Bull. 2013, 105, 139–155. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sellares, J.; de Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F. Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am. J. Transplant. 2012, 12, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Jedlicka, A.; Pekosz, A. The Xs and Y of immune responses to viral vaccines. Lancet Infect. Dis. 2010, 10, 338–349. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Females (n = 18) | Males (n = 29) |
|---|---|---|
| Median age (range), years 1 | 52 (25–67) | 57 (21–73) |
| Median interval TX-vaccination (range), months | 52 (9–260) | 49 (4–413) |
| Donor sex (female/male/unknown 2) | 9/8/1 | 12/17/0 |
| Deceased/living donor | 13/5 | 24/5 |
| Relation between recipient and living donor | ||
| Brother/Sister | 1 | 1 |
| Father/Mother | 1 | 1 |
| Spouse/Partner | 2 | 2 |
| Other | 1 | 1 |
| HLA mismatches 2,3 (mean ± SD) | 2.3 ± 1.9 | 2.3 ± 1.8 |
| HLA antibody status prior to TX | ||
| Current PRA, no. | ||
| <5% | 14 | 27 |
| ≥5% [values] | 3 [5; 20; 30%] | 2 [10; 20%] |
| Unknown 2 | 1 | 0 |
| Highest PRA, no. | ||
| <5% | 12 | 27 |
| ≥5% [values] | 5 [6; 15; 34; 60; 70%] | 2 [10; 20%] |
| Unknown 2 | 1 | 0 |
| Cold ischemic time 2 | ||
| (hours, mean ± SD) | 11.5 ± 7.4 | 11.3 ± 7.9 |
| Median serum creatinine (range), mg/dl | ||
| Pre vaccination | 1.7 (0.9–3.4) | 1.7 (1.2–4.9) |
| Month 1 post vaccination | 1.8 (1.0–3.3) | 1.6 (1.0–5.1) |
| Month 12 post vaccination | 1.8 (0.9–4.4) | 1.6 (1.0–3.0) |
| Median eGFR (range), ml/min/1.73 m2 | ||
| Pre vaccination | 42 (25–84) | 37 (11–89) |
| Month 1 post vaccination | 42 (20–78) | 36 (11–90) |
| Month 12 post vaccination | 45 (19–89) | 41 (13–85) |
| Immunosuppression, no. 1 | ||
| CsA + MMF + CS | 4 | 5 |
| CsA + CS | 1 | 0 |
| TAC + MMF + CS | 6 | 12 |
| TAC + ECU + CS | 2 | 0 |
| TAC + EVR + CS | 0 | 1 |
| TAC + MMF | 1 | 1 |
| TAC + CS | 1 | 7 |
| AZA + CS | 0 | 1 |
| MMF + EVR + CS | 1 | 2 |
| MMF + BEL + CS | 1 | 0 |
| MMF only | 1 | 0 |
| Kidney transplantation, no. | ||
| 1st | 15 | 26 |
| 2nd | 3 | 2 |
| 3rd | 0 | 1 |
| Rejections after vaccination, no. 4 | ||
| Antibody-mediated rejection 5 | 1 6 | 0 |
| Cellular 5 | 0 | 1 7 |
| Allograft loss, no. 4 | 3 | 2 |
| Antibody Pattern | n Patients with This Pattern | ||||
| pre | M1 | M12 | HLA I | HLA II | MICA |
| ø | ø | ø | 24 | 17 | 20 |
| ø | ø | + | 6 | 8 | 7 |
| ø | + | ø | 2 | 3 | 1 |
| ø | + | + | 2 | 2 | 1 |
| + | ø | ø | 5 | 2 | 3 |
| + | ø | + | 2 | 3 | 1 |
| + | + | ø | 1 | 1 | 5 |
| + | + | + | 5 | 11 | 9 |
| Antibody score pre-M1 | HLA I | HLA II | MICA | ||
| ↑ | 11 | 10 | 6 | ||
| = | 21 | 23 | 26 | ||
| ↓ | 15 | 14 | 15 | ||
| Antibody Pattern | % of Females with This Pattern | % of Males with This Pattern | ||||||
| pre | M1 | M12 | HLA I | HLA II | MICA | HLA I | HLA II | MICA |
| ø | ø | ø | 28 | 11 | 33 | 66 | 52 | 48 |
| ø | ø | + | 22 | 22 | 17 | 7 | 14 | 14 |
| ø | + | ø | 6 | 11 | 6 | 3 | 3 | 0 |
| ø | + | + | 11 | 6 | 6 | 0 | 3 | 0 |
| + | ø | ø | 0 | 0 | 6 | 17 | 7 | 7 |
| + | ø | + | 6 | 6 | 0 | 3 | 7 | 3 |
| + | + | ø | 6 | 0 | 6 | 0 | 3 | 14 |
| + | + | + | 22 | 44 | 28 | 3 | 10 | 14 |
| Antibody score pre - M1 | HLA I | HLA II | MICA | HLA I | HLA II | MICA | ||
| ↑ | 39 | 39 | 33 | 14 | 10 | 0 | ||
| = | 50 | 44 | 50 | 41 | 52 | 59 | ||
| ↓ | 11 | 17 | 17 | 45 | 38 | 41 | ||
| ID | HLA I | HLA II | MICA | ||||||
|---|---|---|---|---|---|---|---|---|---|
| pre | M1 | M12 | pre | M1 | M12 | pre | M1 | M12 | |
| #1 | 12 | 24 | 24 | 36 | 40 | 40 | 2 | 8 | 12 |
| #2 | 96 | 96 | 96 | 26 | 12 | 22 | 16 | 9 | 16 |
| #3 | 46 | 53 | 28 | 40 | 40 | 40 | 12 | 12 | 5 |
| #4 | 57 | 60 | 57 | 40 | 40 | 40 | 5 | 8 | 12 |
| #5 | 54 | 57 | 96 | 22 | 29 | 40 | 16 | 16 | 16 |
| Antibody Pattern | % of Females with This Pattern | % of Males with This Pattern | ||||||
| pre | M1 | M12 | HLA I | HLA II | MICA | HLA I | HLA II | MICA |
| ø | ø | ø | 28 | 33 | 72 | 21 | 45 | 55 |
| ø | ø | + | 0 | 6 | 0 | 3 | 14 | 10 |
| ø | + | ø | 17 | 6 | 0 | 3 | 0 | 3 |
| ø | + | + | 0 | 0 | 11 | 7 | 3 | 0 |
| + | ø | ø | 0 | 6 | 6 | 3 | 0 | 3 |
| + | ø | + | 11 | 0 | 6 | 3 | 3 | 0 |
| + | + | ø | 0 | 6 | 6 | 7 | 0 | 7 |
| + | + | + | 61 | 61 | 17 | 48 | 31 | 17 |
| Antibody score pre - M1 | HLA I | HLA II | MICA | HLA I | HLA II | MICA | ||
| ↑ | 22 | 33 | 17 | 41 | 21 | 17 | ||
| = | 56 | 67 | 83 | 28 | 55 | 55 | ||
| ↓ | 39 | 17 | 17 | 28 | 21 | 24 | ||
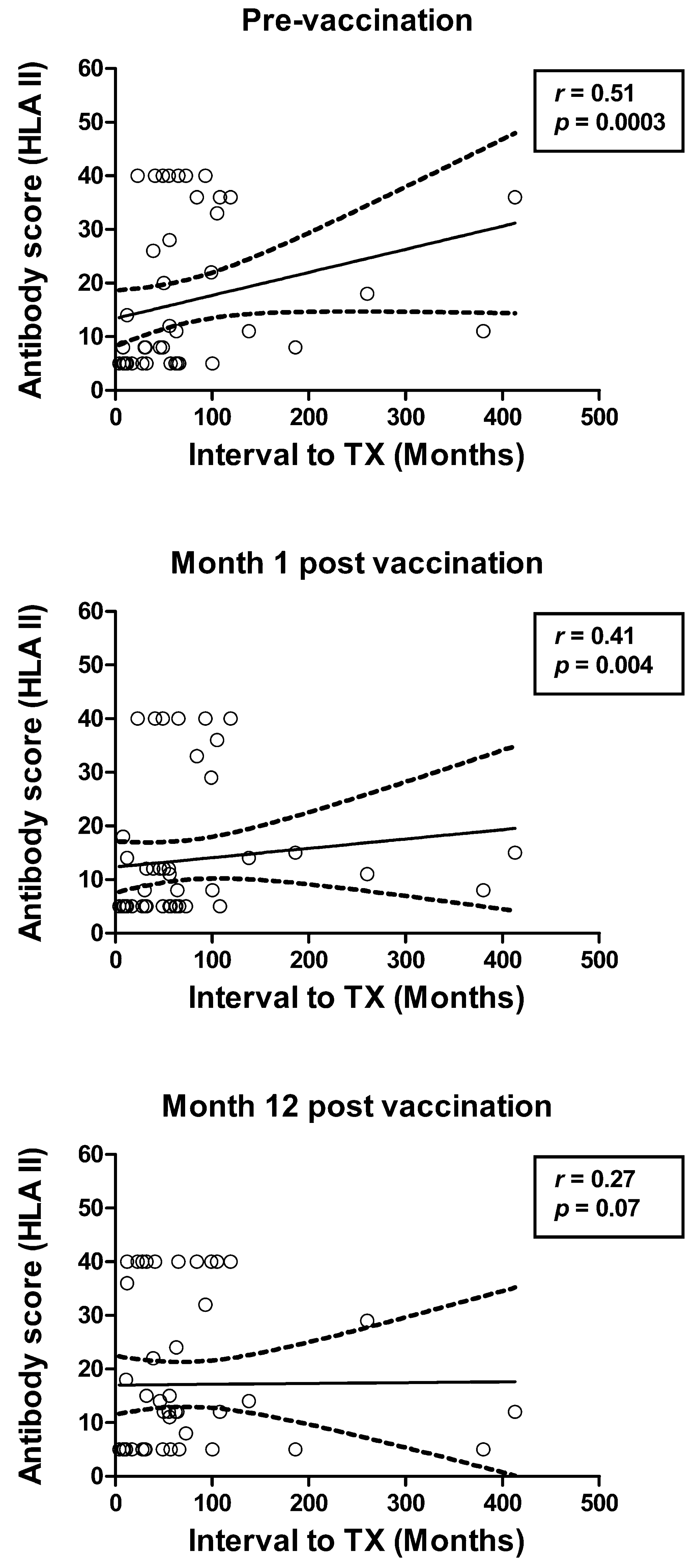
| Antibody Specificity | r | p |
|---|---|---|
| HLA class I | ||
| Pre | 0.26 | 0.08 |
| M1 | 0.31 * | 0.03 |
| M12 | 0.19 | 0.19 |
| HLA class II | ||
| Pre | 0.51 * | 0.0003 |
| M1 | 0.41 * | 0.004 |
| M12 | 0.27 | 0.07 |
| MICA | ||
| Pre | 0.25 | 0.09 |
| M1 | 0.30 * | 0.04 |
| M12 | 0.14 | 0.35 |
| Antibody Specificity | PRA ≥ 5% (n = 7) | PRA < 5% (n = 39) | p |
| HLA class I | |||
| Pre | 53.7 * | 20.5 | 0.01 |
| M1 | 46.0 * | 16.8 | 0.04 |
| M12 | 50.9 | 20.3 | 0.053 |
| HLA class II | |||
| Pre | 29.3 * | 14.4 | 0.02 |
| M1 | 24.9 * | 11.5 | 0.048 |
| M12 | 28.4 | 15.4 | 0.07 |
| MICA | |||
| Pre | 11.3 | 6.6 | 0.052 |
| M1 | 9.7 | 6.0 | 0.1 |
| M12 | 10.9 | 6.2 | 0.08 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindemann, M.; Oesterreich, S.; Wilde, B.; Eisenberger, U.; Muelling, N.; Horn, P.A.; Heinemann, F.M.; Witzke, O. Sex-Specific Differences in HLA Antibodies after Pneumococcal Vaccination in Kidney Transplant Recipients. Vaccines 2019, 7, 84. https://doi.org/10.3390/vaccines7030084
Lindemann M, Oesterreich S, Wilde B, Eisenberger U, Muelling N, Horn PA, Heinemann FM, Witzke O. Sex-Specific Differences in HLA Antibodies after Pneumococcal Vaccination in Kidney Transplant Recipients. Vaccines. 2019; 7(3):84. https://doi.org/10.3390/vaccines7030084
Chicago/Turabian StyleLindemann, Monika, Simon Oesterreich, Benjamin Wilde, Ute Eisenberger, Nils Muelling, Peter A. Horn, Falko M. Heinemann, and Oliver Witzke. 2019. "Sex-Specific Differences in HLA Antibodies after Pneumococcal Vaccination in Kidney Transplant Recipients" Vaccines 7, no. 3: 84. https://doi.org/10.3390/vaccines7030084
APA StyleLindemann, M., Oesterreich, S., Wilde, B., Eisenberger, U., Muelling, N., Horn, P. A., Heinemann, F. M., & Witzke, O. (2019). Sex-Specific Differences in HLA Antibodies after Pneumococcal Vaccination in Kidney Transplant Recipients. Vaccines, 7(3), 84. https://doi.org/10.3390/vaccines7030084