Abstract
Background: The COVID-19 pandemic prompted extensive vaccination efforts globally, yet in the Philippines, many families remained unvaccinated. Caregivers are key decision-makers for family vaccination, but evidence on factors influencing their own vaccine uptake is limited. Methods: A cross-sectional survey of primary caregivers was conducted in low COVID-19 vaccine uptake regions in the Philippines from July to October 2023 using a validated questionnaire. Multivariable logistic regression identified enablers and barriers to vaccine uptake. Results: Among 775 respondents, 72.3% completed primary vaccination, 3.3% had incomplete vaccination, and 24.4% were unvaccinated. Key factors for vaccination included self, family, and community protection, and the influence of government regulations. Distrust in vaccine safety was the main barrier. Positive associations with vaccine uptake were found for age [30–45 years (aOR = 2.23) and 46–59 years (aOR = 2.84)], education [secondary (aOR = 2.25) and tertiary (aOR = 4.93)], and employment (aOR = 1.99). Confidence in vaccine safety (aOR = 1.92), vaccine effectiveness (aOR = 2.23), and satisfaction with vaccination efforts (aOR = 2.39) were additional enablers. Disagreement with restrictions on the unvaccinated was a barrier (aOR = 0.31). Conclusions: This study identified multiple factors influencing COVID-19 vaccination among primary caregivers in low uptake areas of the Philippines. Interventions addressing perceptions about vaccine safety and effectiveness, particularly among younger and less educated caregivers, may improve public trust and satisfaction with vaccination efforts.
1. Introduction
The COVID-19 pandemic posed unprecedented challenges in the health system globally. Over 4 million cases of COVID-19 were recorded in the Philippines from the beginning of the pandemic in 2020 to the end of 2023. Most cases recorded were in the 20–29 and 30–39 age groups [1]. However, the greatest number of mortalities recorded were in the 65 and above age group. The rapid development of safe and effective vaccines became one of the most important interventions. By 2023, two-thirds (67%) of the global population was vaccinated with a complete primary series of COVID-19 vaccines, but only a third (32%) had received at least one booster dose [2]. In the Philippines, the COVID-19 vaccination was rolled out through a multi-sectoral approach involving different departments, agencies, and non-governmental organizations, experts, and professionals in an effort to provide free, safe, and effective vaccines [3]. The initial or phase 1 roll-out of the vaccine in March 2021 prioritized the population with the highest risk such as the frontline healthcare workers, senior citizens, and adults with comorbidities [4]. Subsequently, the phase 2 roll-out for other essential workers, followed by the phase 3 roll-out for the rest of the population was conducted. Towards the end of 2023, the country reached the WHO target of 70% coverage for the primary series [2]. Vaccination efforts in the Philippines have led to a decrease in the number of new cases per day leading to the declaration of the end of the COVID-19 public health emergency in July 2023 [5]. Despite this achievement, the Philippines only ranked eighth out of the eleven member countries of the Association of South East Asian Nations (ASEAN) in COVID-19 vaccine coverage for the primary series, and last for the booster series [6].
Certain sociodemographic characteristics like age, educational attainment, employment status, and household economic status have been suggested as determinants of COVID-19 vaccine uptake, with substantial heterogeneity and inconsistencies [7,8,9,10]. Aside from these, several other factors influence the uptake of COVID-19 vaccines, such as perceptions on disease risk, perceptions on vaccine safety and effectiveness, the direct and indirect costs of vaccination, and levels of trust in government authorities and healthcare workers [11]. There is a need to better understand the combination of these factors specifically in the Philippines, where challenges in vaccine uptake and confidence have long historical precedence [12].
In the Philippines, primary caregivers of children are often the key decision-makers for the vaccination of the entire household. Most caregivers consider vaccination an integral part of their responsibility for the health of their household members [13]. A better understanding of enablers and barriers to COVID-19 vaccination among primary caregivers will therefore provide much-needed evidence for better targeted public health interventions to increase the uptake of COVID-19 vaccines and other vaccines, in the Philippines. Therefore, in this study, we aimed to identify factors that affect COVID-19 vaccine uptake among primary caregivers in regions with low vaccine uptake.
2. Materials and Methods
A cross-sectional community-level paper-based survey was conducted among primary caregivers from July to October 2023 to determine enablers and barriers of COVID-19 vaccination. In consultation with the Department of Health (DOH)—Public Health Operations Center (PHOC), three regions, namely Regions IV-B (MIMAROPA), V (Bicol), and VIII (Eastern Visayas), were selected as study sites due to lower COVID-19 vaccine coverage as compared to other regions. The selection of these regions was based on the vaccine uptake in August 2022, at which point the study sites had not yet met the target vaccination rate of 70% [2] and had approximately 10–12% booster dose coverage. Employing a multi-stage stratified cluster sampling, regions were further stratified into provinces, municipalities, and barangays (communities). In coordination with the DOH Centers for Health Development (CHD) of each region, two provinces and two municipalities from each province were selected based on low COVID-19 vaccine coverage. Lastly, the Rural Health Units (RHUs) of the identified municipalities selected two barangays as study sites. In total, there were 24 barangays included as study sites. Based on a coverage rate of 10.3%, a design effect of 2, a desired absolute precision of 6%, and adding a 30% buffer, the total study sample size calculated was 768.
Before field visits for data collection, community health workers went from house-to-house in the barangays to recruit primary caregivers residing in the community aged 18 years and above with at least one child aged 0–11 years to take part in the study. The recruited participants were also screened by the research team to ensure that the inclusion criteria were met. Those aged less than 18 years and that were not primary caregivers of children aged 0–11 at the time of the study were excluded. All eligible caregivers present in the venue (e.g., health facility or multipurpose hall) during the actual data collection were included in the study until the quota per barangay needed to meet the sample size per province was attained.
The survey questionnaire was developed in reference to the Centers for Disease Control Vaccine Confidence Survey Question Bank [14] and the WHO-Strategic Advisory Group of Experts (SAGE) Vaccine Hesitancy Matrix Questions [15] and underwent two rounds of face validity testing. Variables collected were sociodemographic characteristics of adults such as age in years, sex (male or female), civil status (single, married, live-in, separated, or widowed), religion (Catholic, other Christian denomination, Islam, and others), educational attainment (elementary, high school, or college level) and employment status (unemployed, student, pensioner, self-employed, or employed). Municipal class as determined by the average annual income of the municipality of the respondents was also collected [16]. Reasons for receiving or declining the vaccine, perceptions on COVID-19 infection and vaccination, and sources of information on vaccination were also collected. Self-reported uptake of COVID-19 vaccines (unvaccinated/incomplete primary series and complete primary series with or without booster) was measured as an outcome variable. Other personally identifiable information (e.g., name, address, and contact details) were not collected to ensure the anonymity of the survey participants.
Two separate logistic regression models, one containing sociodemographic variables, and another containing all statements on perceptions about COVID-19 infection and vaccination were first tested. All variables including missing information on perceptions about COVID-19 infection and vaccination were included in the analysis. Using a backward elimination approach, statistically significant variables (p < 0.05) in each model were retained and combined in a third model for analyses. The final logistic regression model consisted of either variables that were statistically significant (p < 0.05) or were considered essential based on likelihood ratio test (LRT) results (p < 0.05). This model was adjusted to account for the inherent differences in the implementation of vaccination programs at the municipal level. Model parameters were presented as odds ratios (ORs) with 95% confidence intervals (CIs). An assessment of the adherence to model assumptions and the overall model fit was conducted. All analyses were performed in STATA/SE version 15.1 (StataCorp LLC, College Station, TX, USA) [17].
This study was given ethical clearance by the UP Manila Research Ethics Board (UPMREB).
3. Results
A total of 775 caregivers participated in the survey. The respondents, aged 18 to 73 with a median age of 32 years, 752 (97.0%) were females, 689 (90.1%) were married or in a live-in relationship, 649 (83.7%) were Catholics, 461 (59.5%) were from higher income municipalities, 668 (82.5%) had elementary or high school education, and 455 (58.7%) were unemployed (Table 1).

Table 1.
Sociodemographic characteristics among all survey respondents (n = 775) *.
Among the respondents, 560 (72.3%) completed the primary series with or without booster doses. There were 586 (75.6%) respondents who received at least one dose of the COVID-19 vaccine, while 189 (24.4%) were unvaccinated (Table 2).
Table 2.
COVID-19 vaccination status among all survey respondents (n = 775).
Among the 586 respondents who received at least one dose of COVID-19 vaccine, the protection of self, family, and community was the leading reason for vaccination (93%), followed by the influence of government-mandated regulations and restrictions (40.6%) (Table 3). The most common reason (81.4%) for non-vaccination was distrust in vaccine safety including fear of side effects (Table 3). Among the 3.3% of respondents with an incomplete primary vaccine series, fear of side effects was the main reason (23.1%) stated for not pursuing full vaccination (Table 3).
Table 3.
Reasons for complete, incomplete, and non-vaccination for COVID-19.
Among caregivers with complete primary series, DOH announcements (72.1%), mass media outlets (56.3%), and local government units (LGUs)/health centers and healthcare workers (HCWs) (51.4%) were identified as the main sources of information on COVID-19 vaccination. Conversely, those unvaccinated or who received incomplete primary series obtained information from mass media outlets (64.7%) and the DOH (46.5%), but with social media (38.1%) among their top three information sources (Table 4).
Table 4.
Sources on information on COVID-19 vaccination *.
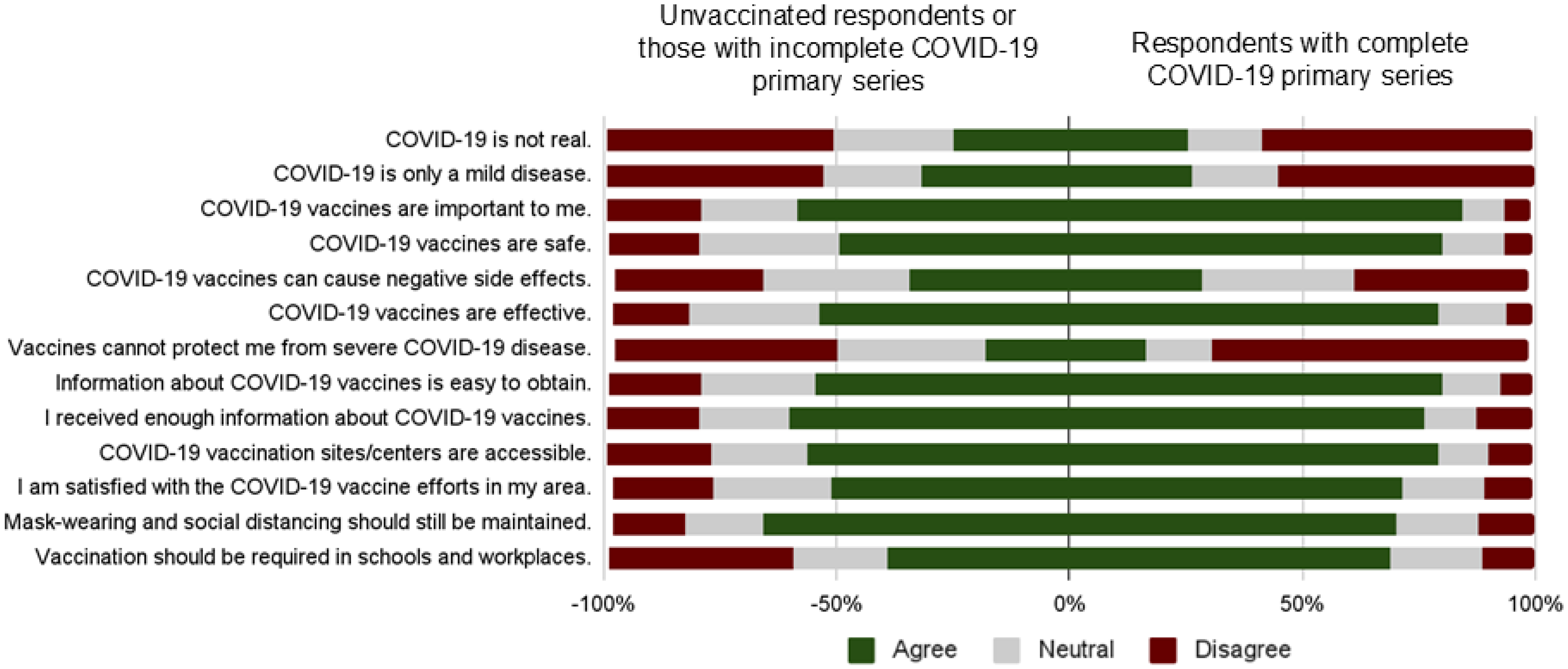
The majority of respondents who completed the primary series considered COVID-19 vaccines to be important (84.5%) and safe (80%). A significant proportion were also satisfied with COVID-19 vaccine efforts in their area (80%) (Figure 1). A third of the respondents who were unvaccinated or received an incomplete primary series thought that COVID-19 vaccines can cause negative side effects (34.4%). They were also of the opinion that COVID-19 is only a mild disease (31.7%) and is not real (24.7%) (Figure 1).
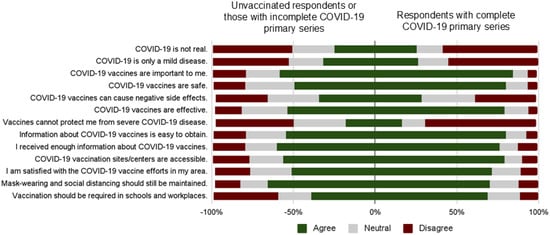
Figure 1.
Perceptions on COVID-19 infection and vaccination among respondents with or without complete COVID-19 primary vaccination.
The logistic regression analyses showed that the odds of completing a primary series of COVID-19 vaccination increases with older age [30–45 years (aOR = 2.23; 95% CI 1.49–3.35) and 46–59 years (aOR = 2.84; 95% CI 1.36–5.95)], higher education level [secondary (aOR = 2.25; 95% CI 1.47–3.43) and tertiary (aOR = 4.93; 95% CI 2.37–19.27)], and being employed (aOR = 1.99; 95% CI 1.24–3.19). Some perceptions about COVID-19 vaccination related to vaccine safety, effectiveness, COVID-19 vaccination efforts, and policies were also associated with the said outcome. Perceptions which served as enablers of COVID-19 vaccination included agreement with the following statements: “COVID-19 vaccines are safe.” (aOR = 1.92, 95% CI 1.16–3.18) and “I am satisfied with COVID-19 efforts in my area.” (aOR = 2.39, 95% CI 1.14–4.06). Disagreement with the statement “Vaccines cannot protect me from severe COVID-19 disease.” also served as enabler (aOR = 2.23, 95% CI 1.38–3.63) of having a primary series of COVID-19 vaccination. On the other hand, a significant barrier to COVID-19 vaccination was related to practical issues. Those who disagreed with the statement “Vaccination should be required in schools and workplaces.” had significantly lower odds (aOR = 0.31, 95% CI 0.18–0.55) of completing the primary series of COVID-19 vaccination compared to those who were neutral to the statement (Table 5).
Table 5.
Factors associated with COVID-19 vaccine uptake (n = 775).
4. Discussion
This study explored the enablers and barriers of COVID-19 vaccine uptake among primary caregivers. The most important factors influencing the uptake of vaccines were identified as age, educational attainment, and employment status, as well as vaccine confidence, satisfaction with COVID-19 efforts, and agreement with vaccination-related policies. The top reasons for completing the COVID-19 primary series were the protection of self, family, and community; influence of government-mandated regulations; and recommendation of family, friends, and neighbors. Conversely, commonly cited reasons for non-vaccination included distrust in vaccine safety or a fear of side effects, a lack of time, and being pregnant.
The study sites were considered to have lower vaccine coverage since they did not meet the national target. However, 75.6% of the respondents received at least one dose of COVID-19 vaccine. This may be attributed to the difference between the period wherein the baseline data were obtained (August 2022) and the period of data collection (July–October 2023). The most common reasons for vaccination were the protection of self, family, and community and the influence of government-mandated regulations. Similar to other studies [18,19], these results suggest that the respondents value the protection provided by the vaccines. The findings also highlighted the positive effect of governance across various administrative levels. Governmental interventions play a crucial role in improving COVID-19 vaccination rates [20,21], but such measures need to be implemented prudently where ethical norms are safeguarded [21]. Other reasons for vaccination were recommendations from family, friends, and neighbors. Individuals were motivated to get vaccinated by observing others including relatives, neighbors, and prominent people, such as community leaders, receive their COVID-19 vaccines. This highlights the role of an individual’s social network in shaping actions and behaviors [22]. The provision of incentives was also a motivating factor for some adults to submit themselves to vaccination. One of the strategies employed in some low- and middle-income countries to increase vaccine acceptance was to provide financial or non-financial rewards [11].
In contrast, a minority (24.4%) were unvaccinated against COVID-19. The primary reason for their decision was distrust in vaccine safety or a fear of side effects. This hesitation could be attributed to the novelty of the vaccine, potentially compounded by previous controversies such as the Dengvaxia issue [23]. Supporting evidence from other countries also revealed that concerns about the adverse effects of COVID-19 vaccines were among the top reasons for vaccine hesitancy [24,25,26]. While a lack of time was reported by only a small fraction, it notably emerged as another reason for non-vaccination among respondents, aligning with findings from another study [27]. Furthermore, being pregnant was also a reason for non-vaccination. This can be attributed to the characteristics of the respondents in this study, being predominantly females. In a similar study, pregnancy was viewed as a barrier for COVID-19 vaccination since respondents were uncertain about the effects of the vaccine on their fetuses [22].
In this study, the majority of respondents who completed the COVID-19 primary series had a high perceived need of vaccination (84.5%) and believed that COVID-19 vaccines are safe (80%). Most of them also showed satisfaction with COVID-19 vaccination efforts in their area (80%). The common sources of information for these respondents included the DOH and LGUs/health centers and HCWs, which is similar to findings from other studies [28,29]. This shows that there is a high level of confidence in health authorities, including HCWs, and government agencies. These information sources played a role in shaping their perceptions on COVID-19 infection and vaccination [30].
On the other hand, a significant proportion of respondents who were unvaccinated or received an incomplete COVID-19 primary series had low vaccine confidence (34.4%) and low perceived disease risk (31.7%). The rapid development of COVID-19 vaccines raised questions about their safety and long-term side effects and might have contributed to the low vaccine confidence. Concerns on side effects like blood clots and fertility issues experienced by family members or friends further added to vaccine hesitancy [31,32]. Low perceived disease risk can stem from individuals believing they are healthy enough to easily combat the virus and no longer view COVID-19 as a significant threat [31]. The perceptions of unvaccinated respondents may have been shaped by social media, being one of the primary sources of information, where misinformation and disinformation is being proliferated.
In the logistic regression analysis, sociodemographic characteristics positively associated with COVID-19 vaccine uptake were older age, specifically the 46–59 years of age group, higher educational attainment, and being employed. Older respondents were more inclined to be part of the employed population subjected to mandatory vaccination protocols during the pandemic. Employment was consistently an enabler of vaccine uptake as vaccination was mandatory for employees during the pandemic, as seen in other studies [8,9,33]. While older age has been identified as a contributing factor to higher vaccine uptake in various studies [10], some studies found that it was a barrier [7,8], possibly due to poor health (e.g., the presence of more chronic conditions) and concerns about vaccine side effects [34]. Higher educational attainment may have contributed to respondents’ better understanding of the benefits of novel COVID-19 vaccines, potentially enabling vaccine uptake.
Other enablers found to be significant in this study were vaccine confidence, satisfaction with the implementation of the COVID-19 vaccination program, and agreement with making vaccination a requirement. These findings were consistent with other studies [35,36,37], highlighting the importance of public trust in vaccines, policies, and governance.
The main limitation of this study is the non-random selection of study sites, which may have affected the generalizability of our findings. Another limitation is the representativeness of the study, as certain regions were excluded, despite having low vaccine uptake, due to logistical constraints and safety concerns in conducting the study. Potential bias may have occurred due to the gender distribution of the respondents being predominantly female. This is due to the inclusion criteria of being a primary caregiver to children aged 0–11. Social desirability bias may have occurred as respondents completed the survey in the presence of the research team and their peers, thereby, providing expected answers. The vaccination status of the respondents was self-reported as medical records or proofs of vaccination were not presented during the conduct of the survey. Geographic differences between the study sites were not explored further as only the municipal class was used as a variable. Other geographic factors (e.g., urban/rural, population density, and the remoteness of the location) were not obtained. Vaccine preferences were also not elaborated as the limited supply of vaccines during the roll-out left people with no choice but to accept what was available in the vaccination center. Lastly, the directionality of the relationship between the beliefs regarding vaccination and vaccine uptake could not confirmed due to the cross-sectional study design.
Despite these limitations, this study identified the multifaceted factors influencing COVID-19 vaccination uptake among adults in the Philippines, underscoring the pivotal role of governance, social influence, and individual perceptions. It highlights the need for targeted interventions addressing vaccine hesitancy among specific demographic groups while emphasizing the importance of fostering public trust, satisfaction with vaccination efforts, and alignment with vaccination policies to enhance overall vaccine confidence and coverage. This constitutes important evidence for enhancing vaccination policy and roll-out in preparation for future outbreaks or pandemics.
5. Conclusions
This study highlights the enablers and barriers of COVID-19 vaccine uptake among primary caregivers in regions in the Philippines with low vaccine uptake. Perceptions on the benefits and the safety of vaccines play a large role in the decision of the respondents to vaccinate. Satisfaction with the implementation of vaccination programs was also highlighted as an enabling factor. We recommend that health promotion and education must be timely and must focus on key messaging that highlights benefits and addresses misconceptions regarding safety concerns including the possible side effects of vaccination. The findings of this study on COVID-19 vaccine uptake may provide evidence for strategies for enhancing vaccine confidence during the introduction of novel vaccines and the threat of future pandemics.
Author Contributions
E.R., M.M.L., P.J.A.-C., S.N.D., J.K., F.V., V.B.J. and M.D. designed this study; E.R., P.J.A.-C., M.M.L., A.A., S.N.D., M.L., Y.F. and J.Z.R. collected and verified the data; E.R., P.J.A.-C., A.A., Y.F., J.Z.R. and F.V. analyzed the data; E.R. and A.A. wrote the original draft. All authors were involved in the interpretation of the study results, review and revision of drafts, and approval of the article prior to submission. All authors have read and agreed to the published version of the manuscript.
Funding
The study is funded by the DFAT Australian Expert Technical Assistance Program (AETAP), in collaboration with the Australian Regional Immunisation Alliance (ARIA).
Institutional Review Board Statement
This study was given ethical clearance by the UPMREB (UPMREB approval number 2023-0321-01).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors express their gratitude to the DOH central office and its regional offices in regions IV-B, V, and VIII, as well as the provincial health offices, rural health units, and the local government authorities in the specific provinces and municipalities selected as study sites for their assistance in facilitating the data collection and validation forums conducted in the study. Additionally, the authors extend their appreciation to Anna Marie Demeterio for her invaluable administrative support and assistance in data collection.
Conflicts of Interest
The authors declare that they have no competing interests.
Abbreviations
The following abbreviations are used in this manuscript:
| COVID-19 | Coronavirus disease |
| aOR | Adjusted odds ratio |
| WHO | World Health Organization |
| ASEAN | Association of South East Asian Nations |
| DOH | Department of Health |
| PHOC | Public Health Operations Center |
| MIMAROPA | Mindoro, Marinduque, Romblon, and Palawan |
| CHD | Centers for Health Development |
| RHUs | Rural Health Units |
| SAGE | Strategic Advisory Group of Experts |
| LRT | Likelihood ratio test |
| ORs | Odds ratio |
| Cis | Confidence intervals |
| UPMREB | University of the Philippines Manila Research Ethics Board |
| LGUs | Local government units |
| HCWs | Healthcare workers |
References
- Department of Health—Philippines. COVID-19 Case Tracker. 2025. Available online: https://doh.gov.ph/diseases/covid-19/covid-19-case-tracker/ (accessed on 25 June 2025).
- WHO. WHO COVID-19 Dashboard. Available online: https://data.who.int/dashboards/covid19/vaccines (accessed on 23 April 2024).
- DOH. The Philippine National Deployment and Vaccination Plan for COVID-19. 2021. Available online: https://www.covidlawlab.org/wp-content/uploads/2021/02/Phillipines_2020.01_The-Philippine-National-COVID-19-Vaccination-Deployment-Plan_EN.pdf (accessed on 23 April 2024).
- Department of Health—Philippines. Department Memorandum No. 20210099: Interim Guidance on COVID-19 Case Management. August 2023. Available online: https://doh.gov.ph/wp-content/uploads/2023/08/dm2021-0099.pdf (accessed on 25 June 2025).
- Republic of the Philippines. Proclamation No. 297, s. 2023: Lifting of the State of Public Health Emergency Throughout the Philippines Due to COVID-19. 21 July 2023. Available online: https://www.officialgazette.gov.ph/2023/07/21/proclamation-no-297-s-2023/ (accessed on 25 June 2025).
- ASEAN Biodiaspora Virtual Center. COVID-19 and Mpox Situational Review in the ASEAN Region. 2023. Available online: https://asean.org/wp-content/uploads/2023/03/COVID-19-and-Mpox_Situational-Report_ASEAN-BioDiaspora-Regional-Virtual-Center_13Mar2023.pdf (accessed on 23 April 2024).
- Tejero, L.M.S.; Seva, R.; Petelo Ilagan, B.; Almajose, K.L. Determinants of COVID-19 vaccination decision among Filipino adults. BMC Public Health 2023, 23, 851. [Google Scholar] [CrossRef] [PubMed]
- Marzo, R.R.; Sami, W.; Alam, M.Z.; Acharya, S.; Jermsittiparsert, K.; Songwathana, K.; Pham, N.T.; Respati, T.; Faller, E.M.; Baldonado, A.M.; et al. Hesitancy in COVID-19 vaccine uptake and its associated factors among the general adult population: A cross-sectional study in six Southeast Asian countries. Trop. Med. Health 2022, 50, 4. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.L.; Leung, A.W.Y.; Chung, O.M.H.; Chien, W.T. Factors influencing COVID-19 vaccination uptake among community members in Hong Kong: A cross-sectional online survey. BMJ Open 2022, 12, e058416. [Google Scholar] [CrossRef] [PubMed]
- Gram, M.A.; Moustsen-Helms, I.R.; Valentiner-Branth, P.; Emborg, H.D. Sociodemographic differences in Covid-19 vaccine uptake in Denmark: A nationwide register-based cohort study. BMC Public Health 2023, 23, 391. [Google Scholar] [CrossRef]
- Moola, S.; Gudi, N.; Nambiar, D.; Dumka, N.; Ahmed, T.; Sonawane, I.R.; Kotwal, A. A rapid review of evidence on the determinants of and strategies for COVID-19 vaccine acceptance in low- and middle-income countries. J. Glob. Health 2021, 11, 05027. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Larson, H.J.; Hartigan-Go, K.; de Figueiredo, A. Vaccine confidence plummets in the Philippines following dengue vaccine scare: Why it matters to pandemic preparedness. Hum. Vaccines Immunother. 2019, 15, 625–627. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ulmido, M.L.; Reñosa, M.D.; Wachinger, J.; Endoma, V.; Landicho-Guevarra, J.; Landicho, J.; Bravo, T.A.; Aligato, M.; McMahon, S.A. Conflicting and complementary notions of responsibility in caregiver’s and Health Care Workers’ vaccination narratives in the Philippines. J. Glob. Health 2024, 14, 04016. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention [CDC]. Vaccine Confidence Survey Question Bank. 2021. Available online: https://content.sph.harvard.edu/wwwhsph/sites/84/2021/07/CDC-Vaccine-Confidence-Survey-Question-Bank.pdf (accessed on 25 June 2025).
- Domek, G.J.; O’Leary, S.T.; Bull, S.; Bronsert, M.; Contreras-Roldan, I.L.; Bolaños Ventura, G.A.; Kempe, A.; Asturias, E.J. Measuring vaccine hesitancy: Field testing the WHO SAGE Working Group on Vaccine Hesitancy survey tool in Guatemala. Vaccine 2018, 36, 5273–5281. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Republic of the Philippines. Republic Act No. 11964: Institutionalizing the Automatic Income Classification of Provinces, Cities, and Municipalities. 26 October 2023. Available online: https://elibrary.judiciary.gov.ph/thebookshelf/showdocs/2/96834 (accessed on 25 June 2025).
- StataCorp. Stata 18 Base Reference Manual; Stata Press: College Station, TX, USA, 2023. [Google Scholar]
- Rani, M.D.M.; Mohamed, N.A.; Solehan, H.M.; Ithnin, M.; Ariffien, A.R.; Isahak, I. Assessment of acceptability of the COVID-19 vaccine based on the health belief model among Malaysians-A qualitative approach. PLoS ONE 2022, 17, e0269059. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Machida, M.; Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; Kikuchi, H.; et al. Acceptance of a COVID-19 Vaccine in Japan during the COVID-19 Pandemic. Vaccines 2021, 9, 210. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bauer, S.; Contreras, S.; Dehning, J.; Linden, M.; Iftekhar, E.; Mohr, S.B.; Olivera-Nappa, A.; Priesemann, V. Relaxing restrictions at the pace of vaccination increases freedom and guards against further COVID-19 waves. PLoS Comput. Biol. 2021, 17, e1009288. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The unintended consequences of COVID-19 vaccine policy: Why mandates, passports and restrictions may cause more harm than good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Afrifa-Anane, G.F.; Larbi, R.T.; Addo, B.; Agyekum, M.W.; Kyei-Arthur, F.; Appiah, M.; Agyemang, C.O.; Sakada, I.G. Facilitators and barriers to COVID-19 vaccine uptake among women in two regions of Ghana: A qualitative study. PLoS ONE 2022, 17, e0272876. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mendoza, R.U.; Dayrit, M.M.; Alfonso, C.R.; Ong, M.M.A. Public trust and the COVID-19 vaccination campaign: Lessons from the Philippines as it emerges from the Dengvaxia controversy. Int. J. Health Plann Manag. 2021, 36, 2048–2055. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Utami, A.; Margawati, A.; Pramono, D.; Nugraheni, A.; Pramudo, S.G. Determinant Factors of COVID-19 Vaccine Hesitancy Among Adult and Elderly Population in Central Java, Indonesia. Patient Prefer. Adherence 2022, 16, 1559–1570. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nomura, S.; Eguchi, A.; Yoneoka, D.; Kawashima, T.; Tanoue, Y.; Murakami, M.; Sakamoto, H.; Maruyama-Sakurai, K.; Gilmour, S.; Shi, S.; et al. Reasons for being unsure or unwilling regarding intention to take COVID-19 vaccine among Japanese people: A large cross-sectional national survey. Lancet Reg. Health West. Pac. 2021, 14, 100223. [Google Scholar] [CrossRef]
- Lau, J.F.W.; Woon, Y.L.; Leong, C.T.; Teh, H.S. Factors influencing acceptance of the COVID-19 vaccine in Malaysia: A web-based survey. Osong Public Health Res. Perspect. 2021, 12, 361–373. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Okubo, R.; Yoshioka, T.; Ohfuji, S.; Matsuo, T.; Tabuchi, T. COVID-19 Vaccine Hesitancy and Its Associated Factors in Japan. Vaccines 2021, 9, 662. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Purvis, R.S.; Moore, R.; Willis, D.E.; Hallgren, E.; McElfish, P.A. Factors influencing COVID-19 vaccine decision-making among hesitant adopters in the United States. Hum. Vaccines Immunother. 2022, 18, 2114701. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gehrau, V.; Fujarski, S.; Lorenz, H.; Schieb, C.; Blöbaum, B. The impact of health information exposure and source credibility on COVID-19 vaccination intention in Germany. Int. J. Environ. Res. Public Health 2021, 18, 4678. [Google Scholar] [CrossRef]
- Park, S.; Massey, P.M.; Stimpson, J.P. Primary Source of Information About COVID-19 as a Determinant of Perception of COVID-19 Severity and Vaccine Uptake: Source of Information and COVID-19. J. Gen. Intern. Med. 2021, 36, 3088–3095. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Williams, S.; Dienes, K. Public attitudes to COVID-19 vaccines: A qualitative study. MedRxiv 2021. [Google Scholar] [CrossRef]
- Denford, S.; Mowbray, F.; Towler, L.; Wehling, H.; Lasseter, G.; Amlôt, R.; Oliver, I.; Yardley, L.; Hickman, M. Exploration of attitudes regarding uptake of COVID-19 vaccines among vaccine hesitant adults in the UK: A qualitative analysis. BMC Infect. Dis. 2022, 22, 407. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 vaccine in Southeast Asia: A cross-sectional study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Zhang, D.; Zhou, W.; Poon, P.K.; Kwok, K.O.; Chui, T.W.; Hung, P.H.Y.; Ting, B.Y.T.; Chan, D.C.; Wong, S.Y. Vaccine resistance and hesitancy among older adults who live alone or only with an older partner in community in the early stage of the fifth wave of COVID-19 in Hong Kong. Vaccines 2022, 10, 1118. [Google Scholar] [CrossRef]
- Ng, J.W.J.; Vaithilingam, S.; Nair, M.; Hwang, L.-A.; Musa, K.I. Key predictors of COVID-19 vaccine hesitancy in Malaysia: An integrated framework. PLoS ONE 2022, 17, e0268926. [Google Scholar] [CrossRef]
- Patwary, M.M.; Bardhan, M.; Disha, A.S.; Hasan, M.; Haque, M.Z.; Sultana, R.; Hossain, M.R.; Browning, M.H.E.M.; Alam, M.A.; Sallam, M. Determinants of COVID-19 vaccine acceptance among the adult population of Bangladesh using the health belief model and the theory of planned behavior model. Vaccines 2021, 9, 1393. [Google Scholar] [CrossRef]
- Sprengholz, P.; Korn, L.; Eitze, S.; Felgendreff, L.; Siegers, R.; Goldhahn, L.; De Bock, F.; Huebl, L.; Böhm, R.; Betsch, C. Attitude toward a mandatory COVID-19 vaccination policy and its determinants: Evidence from serial cross-sectional surveys conducted throughout the pandemic in Germany. Vaccine 2022, 40, 7370–7377. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).