
The 2024 Annual Meeting of the Essential Programmes on Immunization Managers in Central Africa: A Peer Learning Platform

 , , , ,
, , , ,  , and
, and
Abstract
1. Introduction
2. Conference Section
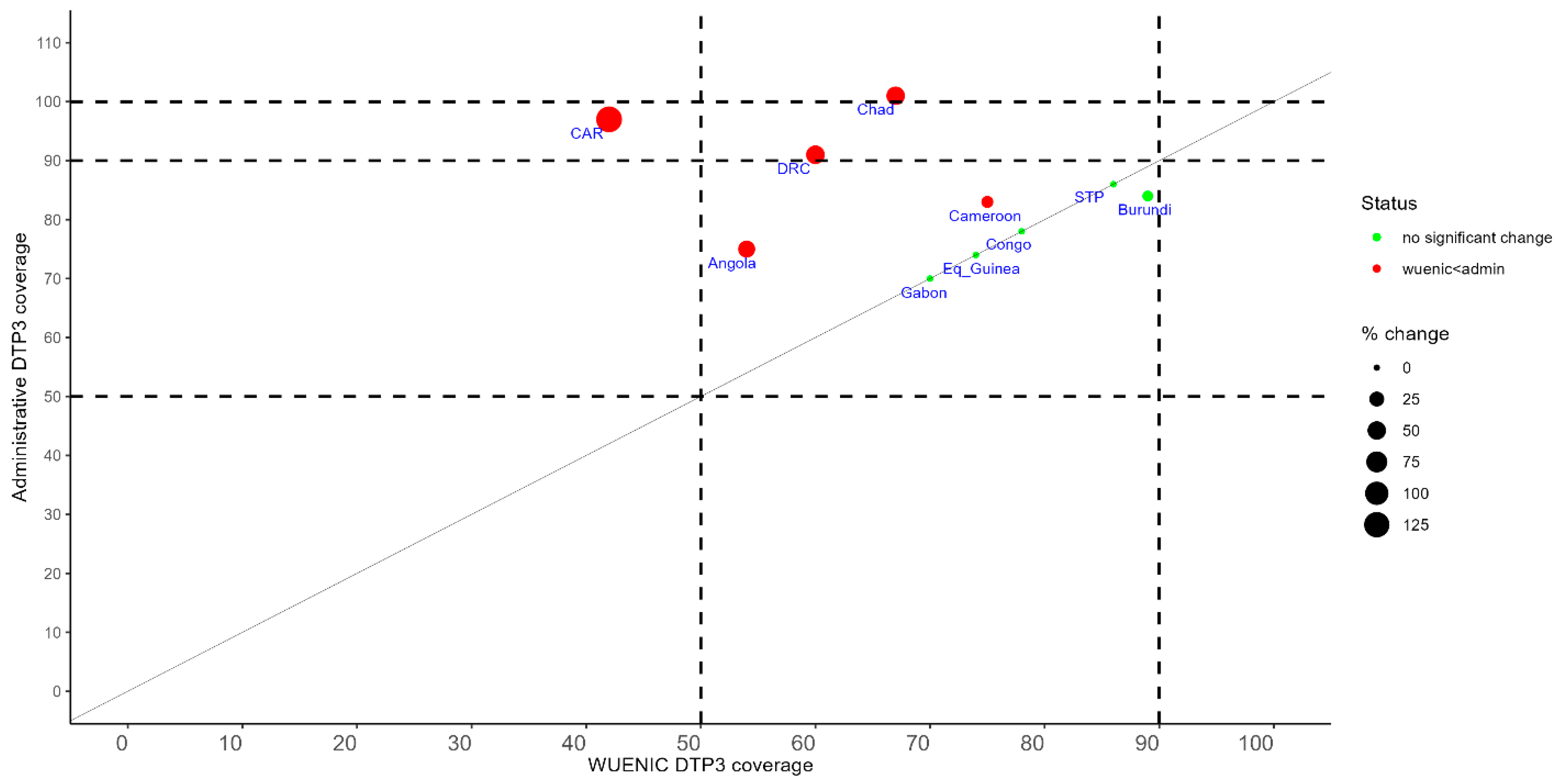
2.1. Routine Immunization Data Use to Inform Decisions
2.2. Efforts to Reduce the Burden of Zero-Dose Children
2.3. Introduction of New Vaccines
3. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. 50th Anniversary of the Expanded Programme on Immunization (EPI). Available online: https://www.who.int/news-room/events/detail/2024/01/01/default-calendar/50th-anniversary-of-the-expanded-programme-on-immunization-(epi) (accessed on 11 January 2025).
- World Health Organization. Immunization Data. Available online: https://immunizationdata.who.int/global?topic=&location= (accessed on 11 January 2025).
- World Health Organization. The Big Catch-Up: An Essential Immunization Recovery Plan for 2023 and Beyond. Available online: https://www.who.int/publications/i/item/9789240075511 (accessed on 11 January 2025).
- World Health Organization. WHO/UNICEF Estimates of National Immunization Coverage. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/immunization-coverage/who-unicef-estimates-of-national-immunization-coverage (accessed on 4 March 2025).
- Mboussou, F.; Nkamedjie, P.; Oyaole, D.; Farham, B.; Atagbaza, A.; Nsasiirwe, S.; Costache, A.; Brooks, D.; Wiysonge, C.S.; Impouma, B. Rapid assessment of data systems for COVID-19 vaccination in the WHO African Region. Epidemiol. Infect. 2024, 152, e50. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Assessing and Improving the Accuracy of Target Population Estimates for Immunization Coverage. Available online: https://www.who.int/publications/m/item/assessing-and-improving-the-accuracy-of-target-population-estimates-for-immunization-coverage (accessed on 18 January 2025).
- World Health Organization. WHO Recommends Groundbreaking Malaria Vaccine for Children at Risk. Available online: https://www.who.int/news/item/06-10-2021-who-recommends-groundbreaking-malaria-vaccine-for-children-at-risk (accessed on 2 February 2025).
- World Health Organization. WHO Recommends R21/Matrix-M Vaccine for Malaria Prevention in Updated Advice on Immunization. Available online: https://www.who.int/news/item/02-10-2023-who-recommends-r21-matrix-m-vaccine-for-malaria-prevention-in-updated-advice-on-immunization (accessed on 2 February 2025).
- O’Brien, K.L.; Lemango, E. The big catch-up in immunisation coverage after the COVID-19 pandemic: Progress and challenges to achieving equitable recovery. Lancet 2023, 402, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Gavi, the Vaccine Alliance. Cameroon’s Historic Malaria Vaccine Introduction Shows Signs of Success, on Year on. Available online: https://www.gavi.org/vaccineswork/cameroons-historic-malaria-vaccine-introduction-shows-signs-success-one-year (accessed on 5 March 2025).
- Gavi, the Vaccine Alliance. Human Papillomavirus Vaccine Support. Available online: https://www.gavi.org/types-support/vaccine-support/human-papillomavirus (accessed on 18 January 2025).
- Haddison, E.; Tambasho, A.; Kouamen, G.; Ngwafor, R. Vaccinators’ Perception of HPV Vaccination in the Saa Health District of Cameroon. Front. Public Health 2022, 9, 748910. [Google Scholar] [CrossRef] [PubMed]
- Adamu, A.A.; Ndwandwe, D.; Jalo, R.I.; Ndoutabe, M.; Wiysonge, C.S. Peer learning in immunisation programmes. Lancet 2024, 404, 334–335. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Country | Surviving Infants (2019–2023 Cohorts) | # Zero-Dose Children | # Under-Immunized Children | # Zero-Dose and Under-Immunized Children | % of All Zero-Dose and Under-Immunized Children in Central Africa |
|---|---|---|---|---|---|
| Angola | 6,389,000 | 2,468,000 | 744,000 | 3,212,000 | 23 |
| Burundi | 2,200,000 | 119,000 | 57,000 | 176,000 | 1 |
| Cameroon | 4,503,000 | 1,088,000 | 243,000 | 1,331,000 | 10 |
| Central African Republic | 1,054,000 | 485,000 | 127,000 | 612,000 | 4 |
| Chad | 3,683,000 | 818,000 | 743,000 | 1,561,000 | 11 |
| Congo | 899,000 | 172,000 | 34,000 | 206,000 | 1 |
| Democratic Republic of Congo | 19,920,000 | 3,636,000 | 3,050,000 | 6,686,000 | 48 |
| Equatorial Guinea | 258,000 | 59,000 | 25,000 | 84,000 | 1 |
| Gabon | 334,000 | 93,000 | 15,000 | 108,000 | 1 |
| São Tomé and Príncipe | 31,000 | 2000 | - | 2000 | 0 |
| Total | 39,271,000 | 8,940,000 | 5,038,000 | 13,978,000 | 100 |
| Country | Malaria Vaccine Introduction | HPV Vaccine Introduction |
|---|---|---|
| Angola | Not yet planned | Planned in 2025 |
| Burundi | Planned in 2025 | Planned in 2025 |
| Cameroon | Introduced in January 2024 | Introduced in 2020 |
| Chad | Planned in October 2024 | Not yet planned |
| Central African Republic | Planned in September 2025 | Not yet Planned |
| Congo | Not yet planned | Not yet planned |
| Democratic Republic of Congo | Planned in October 2024 | Planned in 2026 |
| Equatorial Guinea | Demonstration in 2024; introduction planned in 2026 | Not yet planned |
| Gabon | Not yet planned | Not yet planned |
| São Tomé and Príncipe | Not yet planned | Introduced in 2021 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mboussou, F.; Mulumba, A.; Traore, C.; Conteh-Nordman, F.; Ndoula, S.T.; Mbailamen, A.D.; Bizimana, J.C.; Akani, C.; Vuo-Masembe, Y.; Farham, B.; et al. The 2024 Annual Meeting of the Essential Programmes on Immunization Managers in Central Africa: A Peer Learning Platform. Vaccines 2025, 13, 301. https://doi.org/10.3390/vaccines13030301
Mboussou F, Mulumba A, Traore C, Conteh-Nordman F, Ndoula ST, Mbailamen AD, Bizimana JC, Akani C, Vuo-Masembe Y, Farham B, et al. The 2024 Annual Meeting of the Essential Programmes on Immunization Managers in Central Africa: A Peer Learning Platform. Vaccines. 2025; 13(3):301. https://doi.org/10.3390/vaccines13030301
Chicago/Turabian StyleMboussou, Franck, Audry Mulumba, Celestin Traore, Florence Conteh-Nordman, Shalom Tchokfe Ndoula, Antoinette Demian Mbailamen, Jean Claude Bizimana, Christian Akani, Yolande Vuo-Masembe, Bridget Farham, and et al. 2025. "The 2024 Annual Meeting of the Essential Programmes on Immunization Managers in Central Africa: A Peer Learning Platform" Vaccines 13, no. 3: 301. https://doi.org/10.3390/vaccines13030301
APA StyleMboussou, F., Mulumba, A., Traore, C., Conteh-Nordman, F., Ndoula, S. T., Mbailamen, A. D., Bizimana, J. C., Akani, C., Vuo-Masembe, Y., Farham, B., Nimpa, M. M., Gaha, T. N., Morand, M., Rey, L., Danovaro-Holliday, M. C., Wiysonge, C. S., & Impouma, B. (2025). The 2024 Annual Meeting of the Essential Programmes on Immunization Managers in Central Africa: A Peer Learning Platform. Vaccines, 13(3), 301. https://doi.org/10.3390/vaccines13030301