
Socio-Demographic Factors Influencing Malaria Vaccine Acceptance for Under-Five Children in a Malaria-Endemic Region: A Community-Based Study in the Democratic Republic of Congo

 , , , , , and
, , , , , and 
Abstract
1. Introduction
2. Materials and Methods
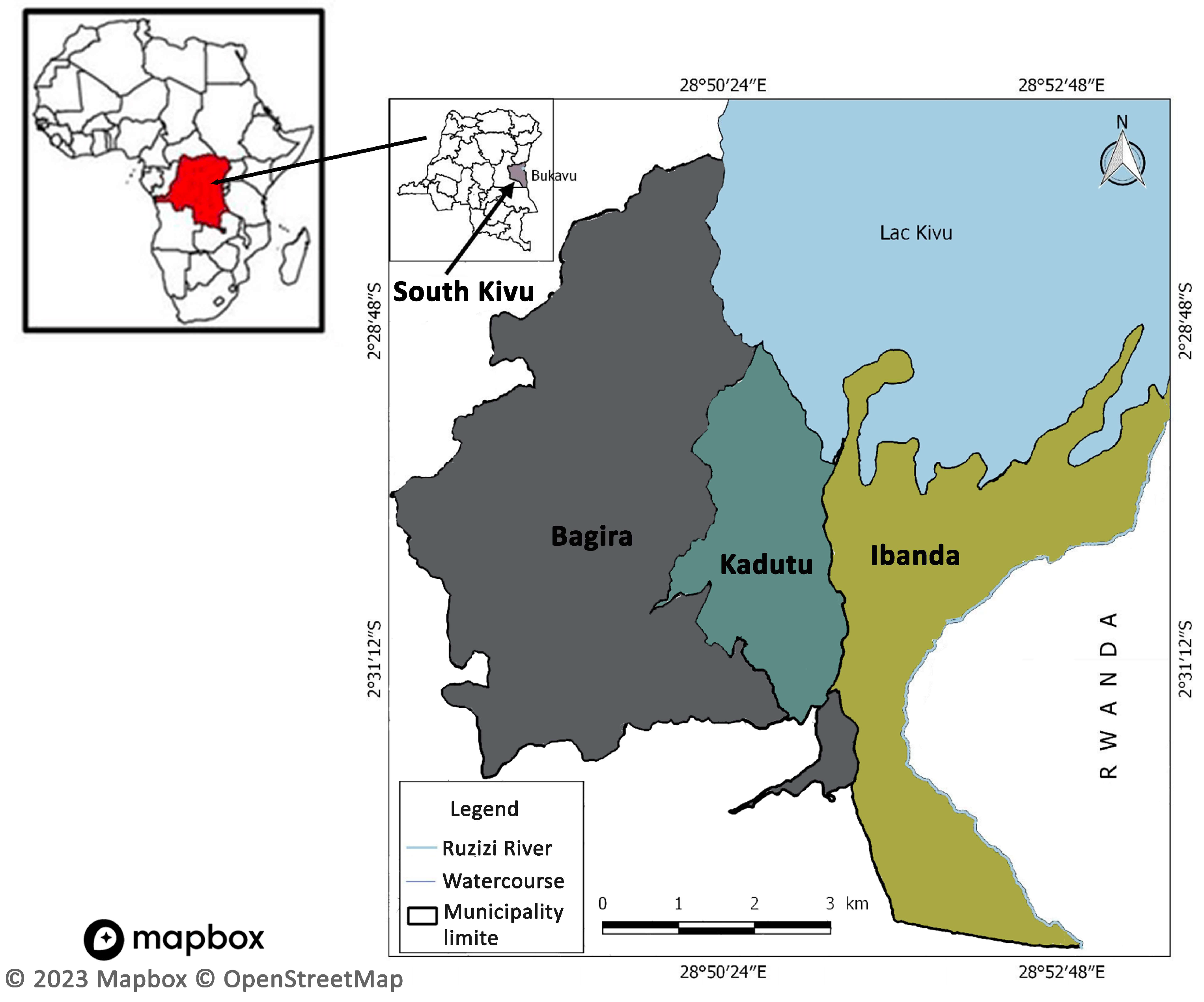
2.1. Study Design, Period, and Setting
2.2. Data Collection Tool
2.3. Outcome Measures
2.4. Independent Measures
2.5. Sample Size
2.6. Statistical Analysis
3. Results
3.1. Knowledge about Malaria Vaccine and Prevalence of Its Acceptability
3.2. Factors Associated with Acceptability of Malaria Vaccine
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Congo, Dem. Rep.|Data. Available online: https://data.worldbank.org/country/CD (accessed on 25 March 2023).
- Democratic Republic of the Congo. Institute for Health Metrics and Evaluation. Published 9 September 2015. Available online: https://www.healthdata.org/democratic-republic-congo (accessed on 25 March 2023).
- U.S. President’s Malaria Initiative Democratic Republic of the Congo Malaria Operational Plan FY 2022. Available online: https://d1u4sg1s9ptc4z.cloudfront.net/uploads/2022/01/FY-2022-DR-Congo-MOP.pdf (accessed on 25 March 2023).
- World Malaria Report 2021. 2021, Volume 263. Available online: https://www.who.int/publications-detail-redirect/9789240040496 (accessed on 25 March 2023).
- Ngatu, N.R.; Kanbara, S.; Renzaho, A.; Wumba, R.; Mbelambela, E.P.; Muchanga, S.M.; Muzembo, B.A.; Leon-Kabamba, N.; Nattadech, C.; Suzuki, T.; et al. Environmental and sociodemographic factors associated with household malaria burden in the Congo. Malar J. 2019, 18, 53. [Google Scholar] [CrossRef] [PubMed]
- Panzi, E.K.; Okenge, L.N.; Kabali, E.H.; Tshimungu, F.; Dilu, A.K.; Mulangu, F.; Kandala, N.B. Geo-Climatic Factors of Malaria Morbidity in the Democratic Republic of Congo from 2001 to 2019. Int. J. Environ. Res. Public Health. 2022, 19, 3811. [Google Scholar] [CrossRef] [PubMed]
- Democratic Republic of Congo. Severe Malaria Observatory. Available online: https://www.severemalaria.org/countries/democratic-republic-of-congo (accessed on 25 March 2023).
- Malaria—Level 3 Cause. Institute for Health Metrics and Evaluation. Published 15 October 2020. Available online: https://www.healthdata.org/results/gbd_summaries/2019/malaria-level-3-cause (accessed on 25 March 2023).
- Collins, W.E.; Jeffery, G.M. Plasmodium malariae: Parasite and disease. Clin. Microbiol. Rev. 2007, 20, 579–592. [Google Scholar] [CrossRef] [PubMed]
- Democratic Republic of Congo|Zero Malaria Starts with Me. Available online: https://zeromalaria.africa/country/cod (accessed on 26 March 2023).
- Laurens, M.B. RTS,S/AS01 vaccine (MosquirixTM): An overview. Hum. Vaccines Immunother. 2019, 16, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Malaria Vaccine Implementation Programme. Available online: https://www.who.int/initiatives/malaria-vaccine-implementation-programme (accessed on 26 March 2023).
- Aaby, P.; Rodrigues, A.; Kofoed, P.E.; Benn, C.S. RTS,S/AS01 malaria vaccine and child mortality. Lancet Lond Engl. 2015, 386, 1735–1736. [Google Scholar] [CrossRef] [PubMed][Green Version]
- WHO Recommends R21/Matrix-M Vaccine for Malaria Prevention in Updated Advice on Immunization. Available online: https://www.who.int/news/item/02-10-2023-who-recommends-r21-matrix-m-vaccine-for-malaria-prevention-in-updated-advice-on-immunization (accessed on 25 March 2023).
- Bukavu, Democratic Republic of the Congo Population (2023)—Population Stat. Available online: https://populationstat.com/democratic-republic-of-the-congo/bukavu (accessed on 26 March 2023).
- WHO. Understanding the behavioural and social drivers of vaccine uptake WHO position paper—May 2022. Wkly. Epidemiol. Rec. 2022, 97, 209–224. [Google Scholar]
- Cameroon Kicks off Malaria Vaccine Rollout. WHO|Regional Office for Africa. Published 22 January 2024. Available online: https://www.afro.who.int/countries/cameroon/news/cameroon-kicks-malaria-vaccine-rollout (accessed on 24 January 2024).
- Kibongani Volet, A.; Scavone, C.; Catalán-Matamoros, D.; Capuano, A. Vaccine Hesitancy Among Religious Groups: Reasons Underlying This Phenomenon and Communication Strategies to Rebuild Trust. Front Public Health 2022, 10. Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2022.824560 (accessed on 24 January 2024).
- Soni, G.K.; Bhatnagar, A.; Gupta, A.; Kumari, A.; Arora, S.; Seth, S.; Rastogi, A.; Kanagat, N.; Fields, R. Engaging Faith-Based Organizations for Promoting the Uptake of COVID-19 Vaccine in India: A Case Study of a Multi-Faith Society. Vaccines 2023, 11, 837. [Google Scholar] [CrossRef] [PubMed]
- Ghilardi, L.; Okello, G.; Nyondo-Mipando, L.; Chirambo, C.M.; Malongo, F.; Hoyt, J.; Lee, J.; Sedekia, Y.; Parkhurst, J.; Lines, J.; et al. How useful are malaria risk maps at the country level? Perceptions of decision-makers in Kenya, Malawi and the Democratic Republic of Congo. Malar J. 2020, 19, 353. [Google Scholar] [CrossRef] [PubMed]
- Deutsch-Feldman, M.; Parr, J.B.; Keeler, C.; Brazeau, N.F.; Goel, V.; Emch, M.; Edwards, J.K.; Kashamuka, M.; Tshefu, A.K.; Meshnick, S.R. The Burden of Malaria in the Democratic Republic of the Congo. J. Infect. Dis. 2020, 223, 1948–1952. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Schuster, M.; Eskola, J.; Duclos, P. SAGE Working Group on Vaccine Hesitancy. Review of vaccine hesitancy: Rationale, remit and methods. Vaccine 2015, 33, 4157–4160. [Google Scholar] [CrossRef] [PubMed]
- Ilemona, A.B. Awareness and Willingness to Accept Malaria Vaccine among Care-Givers of under-5 Children in Ibadan North Local Government, Nigeria. Master’s Thesis, Department of Epidemiology, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadana, Oyo, Nigeria, 2012. Available online: https://library.adhl.africa/handle/123456789/11995 (accessed on 26 March 2023).
- Asmare, G. Willingness to accept malaria vaccine among caregivers of under-5 children in Southwest Ethiopia: A community based cross-sectional study. Malar J. 2022, 21, 146. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, S.K.; Musa, M.S.; Tsiga-Ahmed, F.I.; Dayyab, F.M.; Sulaiman, A.K.; Bako, A.T. A systematic review and meta-analysis of the prevalence of caregiver acceptance of malaria vaccine for under-five children in low-income and middle-income countries (LMICs). PLoS ONE 2022, 17, e0278224. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.C.; Hung, H.F.; Chen, M.K.; Chen, S.L.S.; Fann, J.C.Y.; Chiu, S.Y.H.; Yen, A.M.F.; Huang, K.C.; Chen, H.H.; Wang, S.T. Cost-effectiveness analysis of universal influenza vaccination: Application of the susceptible–infectious–complication–recovery model. Int. J. Infect. Dis. 2018, 73, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T.A.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Tamba, J. Lutte Contre Paludisme Dans Les Secteurs Public et au Niveau Communautaire. Available online: https://www.sanru.cd/index.php/component/k2/item/1252-lutte-contre-le-paludisme-dans-le-secteur-public (accessed on 26 March 2023).
- World Health Organization. 18 Million Doses of First-Ever Malaria Vaccine Allocated to 12 African Countries for 2023–2025: Gavi, WHO and UNICEF. Available online: https://www.who.int/news/item/05-07-2023-18-million-doses-of-first-ever-malaria-vaccine-allocated-to-12-african-countries-for-2023-2025--gavi--who-and-unicef (accessed on 10 February 2024).


{kind=link}
| Characteristics | Total | Acceptability of Malaria Vaccine for Self (N, %) | Malaria Vaccine for Under-Five Children (N, %) | |||||
|---|---|---|---|---|---|---|---|---|
| Acceptance | Hesitancy | p-Value | Acceptance | Hesitancy | p-Value | |||
| Overall | 1612 (100%) | 750 (46.53%) | 862 (53.47%) | 848 (52.61%) | 764 (47.39%) | |||
| Age, years | 0.01 | <0.001 | ||||||
| 18–24 | 276 (17.12%) | 139 (50.36%) | 137 (49.63%) | 168 (60.86%) | 108 (39.14%) | |||
| 25–39 | 536 (33.26%) | 268 (50.00%) | 268 (50.00%) | 310 (57.84%) | 226 (42.16%) | |||
| 40–54 | 408 (25.31%) | 174 (42.65%) | 234 (57.35%) | 187 (45.83%) | 221 (54,17%) | |||
| 55–64 | 278 (17.24%) | 130 (46.77%) | 148 (53.23%) | 138 (49.64%) | 140 (50.36%) | |||
| ≥65 | 114 (7.07%) | 39 (34.21%) | 75 (65.78%) | 45 (39.47%) | 69 (60.53%) | |||
| Gender | 0.04 | 0.01 | ||||||
| Female | 744 (46.15%) | 326 (43.81%) | 418 (56.19%) | 483 (64.92%) | 385 (35.08%) | |||
| Male | 868 (53.85%) | 424 (48.84%) | 444 (51.16%) | 365 (42.05%) | 379 (57.95%) | |||
| Religion | 0.35 | 0.20 | ||||||
| Non-Christian | 46 (2.85%) | 25 (54.34%) | 21 (45.66%) | 29 (63.04%) | 17 (36.96%) | |||
| Christian | 1566 (97.15%) | 725 (48.21%) | 841 (51.79%) | 819 (52.30%) | 747 (47.70%) | |||
| Relig. Accept. Vac. * | <0.001 | <0.001 | ||||||
| Yes | 859 (53.29%) | 457 (53.21%) | 402 (46.79%) | 506 (58.90%) | 353 (41.10%) | |||
| No | 753 (46.71%) | 293 (40.02%) | 460 (59.98%) | 342 45.42%) | 411 (54.58%) | |||
| Location | 0.17 | <0.001 | ||||||
| Semi-rural | 880 (54.59%) | 396 (45.00%) | 484 (55.00%) | 417 (47.39%) | 463 (52.61%) | |||
| Urban | 732 (45.41%) | 354 (47.13%) | 378 (52.87%) | 431 (58.87%) | 301 (41.13%) | |||
| Level of education | <0.001 | <0.001 | ||||||
| Low | 44 (2.73%) | 12 (27.27%) | 32 (72.73%) | 11 (25.00%) | 33 (75.00%) | |||
| Medium | 564 (34.98%) | 336 (59.57%) | 228 (40.43%) | 260 (46.10%) | 304 (53.90%) | |||
| High | 1004 (62.29%) | 510 (50.80%) | 494 (49.20%) | 577 (57.47%) | 427 (42.53%) | |||
| Profession | <0.001 | <0.001 | ||||||
| No student/no healthcare worker | 961 (59.61%) | 380 (39.55%) | 581 (60.45%) | 442 (46.00%) | 519 (64.00%) | |||
| Student | 302 (18.74%) | 176 (58.28%) | 126 (41.72%) | 184 (60.92%) | 118 (39.08%) | |||
| Healthcare worker | 349 (21.65%) | 194 (55.59%) | 155 (44.41%) | 222 (63.61%) | 127 (36.39%) | |||
| Monthly income, $ USD | <0.001 | <0.001 | ||||||
| <50 | 459 (40.15%) | 158 (34.43%) | 301 (65.57%) | 202 (44.01%) | 257 (55.99%) | |||
| 50–200 | 457 (39.98%) | 215 (47.05%) | 242 (52.95%) | 252 (55.15%) | 205 (44.85%) | |||
| 200–500 | 186 (16.27%) | 108 (58.06%) | 78 (41.94%) | 114 (61.30%) | 72 (38.70%) | |||
| >500 | 41 (3.60%) | 20 (48.79%) | 21 (51.21%) | 22 (53.66%) | 19 (46.34%) | |||
| Characteristics | aOR | 95% CI | p | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age, years | 18–24 | Reference | |||
| 25–39 | 0.83 | 0.51 | 1.35 | 0.44 | |
| 40–54 | 0.68 | 0.41 | 1.12 | 0.13 | |
| 55–64 | 0.96 | 0.58 | 1.61 | 0.88 | |
| ≥65 | 0.81 | 0.43 | 1.50 | 0.50 | |
| Gender | Male | Reference | |||
| Female | 1.01 | 0.79 | 1.30 | 0.93 | |
| Religion | Christian | Reference | |||
| Non-Christian | 1.67 | 0.73 | 3.88 | 0.22 | |
| Location | Urban | Reference | |||
| Semi-rural | 1.04 | 0.81 | 1.33 | 0.79 | |
| Religious acceptance of vaccine | No | Reference | |||
| Yes | 1.54 | 1.20 | 1.99 | <0.001 | |
| Level of education | High | Reference | |||
| Low | 0.61 | 0.28 | 1.23 | 0.17 | |
| Medium | 0.84 | 0.62 | 1.13 | 0.24 | |
| Profession | HCW | Reference | |||
| No Student No HCW | 0.58 | 0.42 | 0.78 | <0.001 | |
| Student | - | ||||
| Monthly Income, USD | <50 | Reference | |||
| 50–200 | 1.23 | 0.91 | 1.67 | 0.18 | |
| 200–500 | 1.87 | 1.25 | 2.80 | <0.01 | |
| >500 | 1.21 | 0.61 | 2.40 | 0.58 | |
| Characteristics | aOR | 95% CI | p | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age,years | 18–24 | Reference | |||
| 25–39 | 1.93 | 1.63 | 3.26 | 0.01 | |
| 40–54 | 2.53 | 1.58 | 4.48 | <0.001 | |
| 55–64 | 1.96 | 1.16 | 3.38 | 0.01 | |
| >= 65 | 2.07 | 1.11 | 3.94 | 0.02 | |
| Gender | Male | Reference | |||
| Female | 1.18 | 0.92 | 1.52 | 0.18 | |
| Religious acceptance of vaccination | No | Reference | |||
| Yes | 1.44 | 1.12 | 1.86 | <0.01 | |
| Profession | Healthcare worker | Reference | |||
| No Student No Healthcare Worker | 1.88 | 1.37 | 2.59 | <0.001 | |
| Student | - | ||||
| Location | Urban | Reference | |||
| Semi-rural | 1.63 | 1.27 | 2.10 | <0.001 | |
| Level of education | Low | Reference | |||
| Medium | 2.64 | 1.29 | 5.79 | 0.01 | |
| High | 1.32 | 0.98 | 1.78 | 0.06 | |
| Monthly Income, USD | <50 | Reference | |||
| 50–200 | 0.94 | 0.69 | 1.27 | 0.46 | |
| 200–500 | 0.84 | 0.55 | 1.26 | 0.69 | |
| >500 | 1.30 | 0.64 | 2.60 | 0.39 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nyalundja, A.D.; Bugeme, P.M.; Guillaume, A.S.; Ntaboba, A.B.; Hatu’m, V.U.; Tamuzi, J.L.; Ndwandwe, D.; Iwu-Jaja, C.; Wiysonge, C.S.; Katoto, P.D.M.C. Socio-Demographic Factors Influencing Malaria Vaccine Acceptance for Under-Five Children in a Malaria-Endemic Region: A Community-Based Study in the Democratic Republic of Congo. Vaccines 2024, 12, 380. https://doi.org/10.3390/vaccines12040380
Nyalundja AD, Bugeme PM, Guillaume AS, Ntaboba AB, Hatu’m VU, Tamuzi JL, Ndwandwe D, Iwu-Jaja C, Wiysonge CS, Katoto PDMC. Socio-Demographic Factors Influencing Malaria Vaccine Acceptance for Under-Five Children in a Malaria-Endemic Region: A Community-Based Study in the Democratic Republic of Congo. Vaccines. 2024; 12(4):380. https://doi.org/10.3390/vaccines12040380
Chicago/Turabian StyleNyalundja, Arsene Daniel, Patrick Musole Bugeme, Ashuza Shamamba Guillaume, Alain Balola Ntaboba, Victoire Urbain Hatu’m, Jacques Lukenze Tamuzi, Duduzile Ndwandwe, Chinwe Iwu-Jaja, Charles S. Wiysonge, and Patrick D. M. C. Katoto. 2024. "Socio-Demographic Factors Influencing Malaria Vaccine Acceptance for Under-Five Children in a Malaria-Endemic Region: A Community-Based Study in the Democratic Republic of Congo" Vaccines 12, no. 4: 380. https://doi.org/10.3390/vaccines12040380
APA StyleNyalundja, A. D., Bugeme, P. M., Guillaume, A. S., Ntaboba, A. B., Hatu’m, V. U., Tamuzi, J. L., Ndwandwe, D., Iwu-Jaja, C., Wiysonge, C. S., & Katoto, P. D. M. C. (2024). Socio-Demographic Factors Influencing Malaria Vaccine Acceptance for Under-Five Children in a Malaria-Endemic Region: A Community-Based Study in the Democratic Republic of Congo. Vaccines, 12(4), 380. https://doi.org/10.3390/vaccines12040380