
Evaluating the Quality of Studies Assessing COVID-19 Vaccine Neutralizing Antibody Immunogenicity

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Study Selection
2.2. Quality Assessment Tool (QAT) Development and Update
2.3. QAT Evaluation Process
2.4. Data Analysis
3. Results
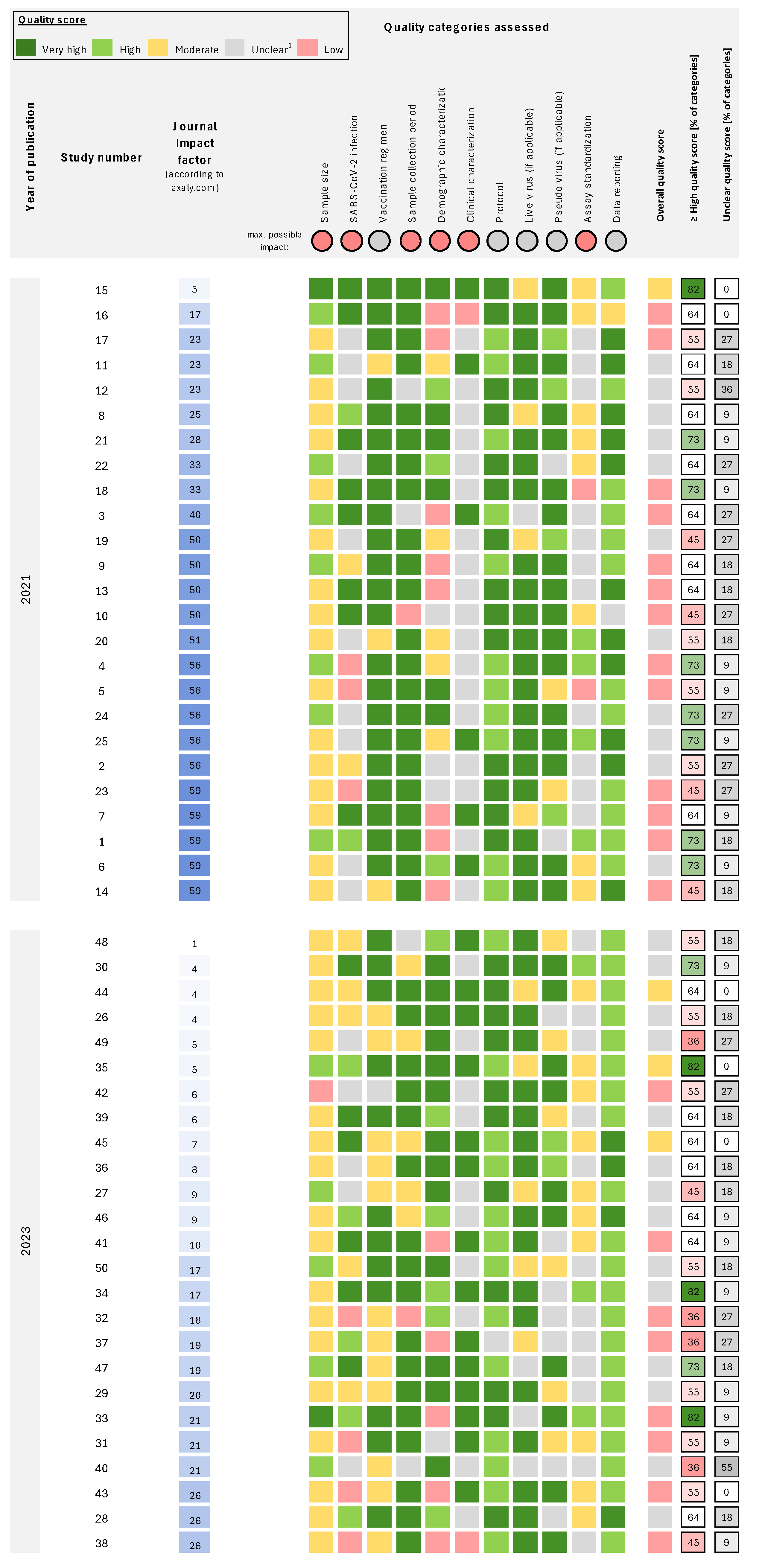
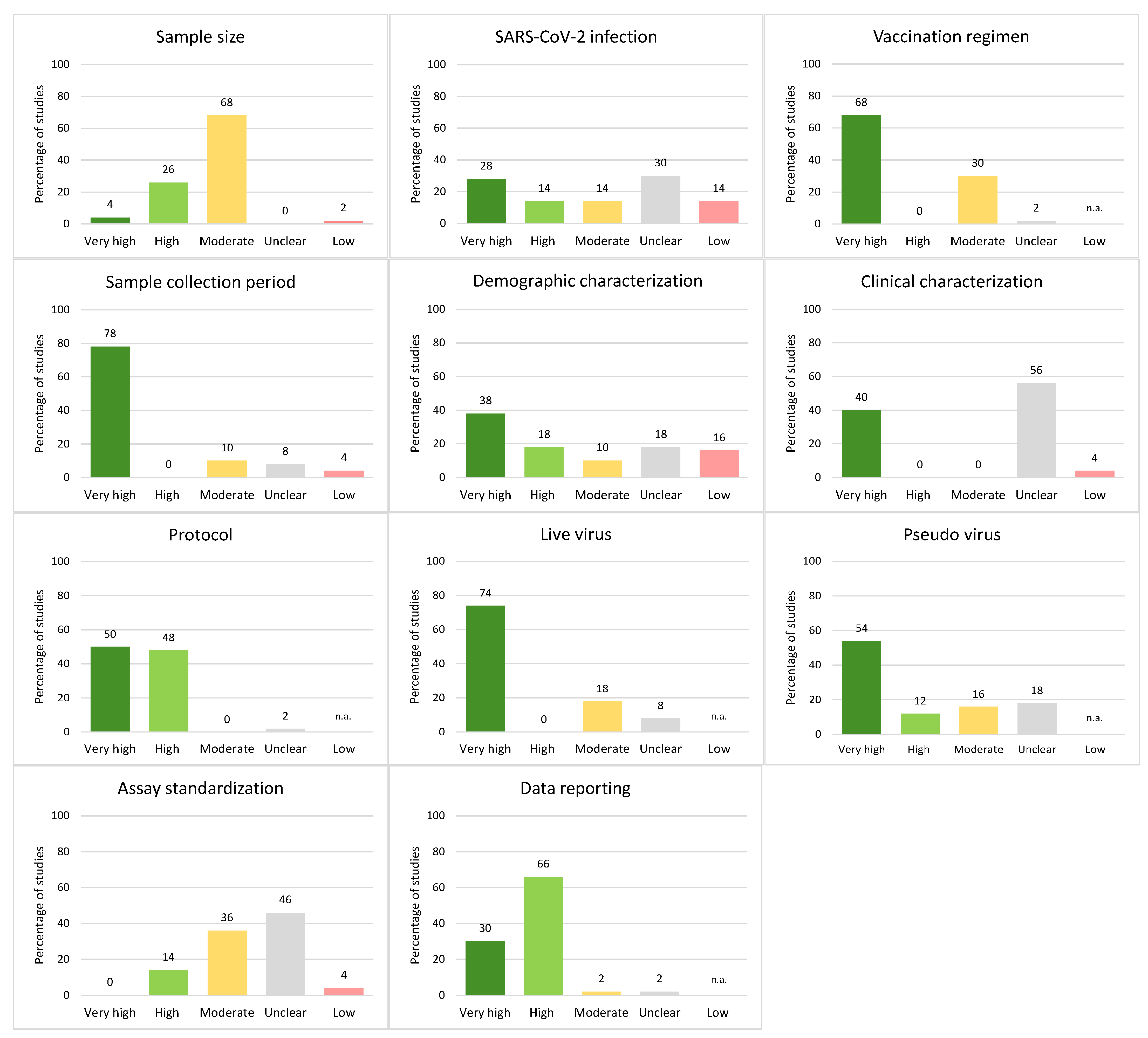
3.1. Evaluation of Reliability and Reporting Quality Across COVID-19 Studies
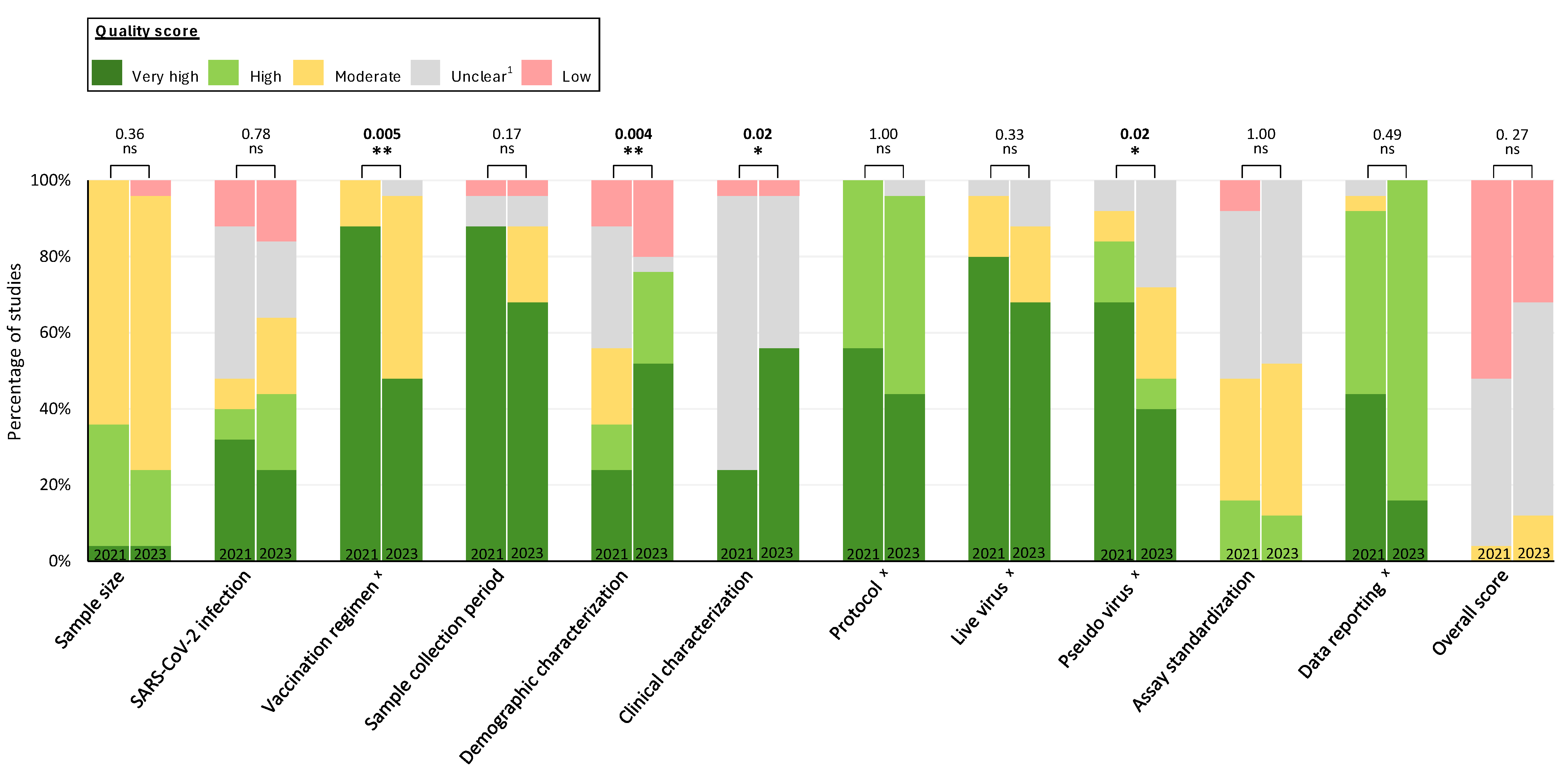
3.2. Temporal Trends in Reporting Quality and Reliability of COVID-19 Studies
4. Discussion
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- COVID-19 Cases|WHO COVID-19 Dashboard. Available online: https://data.who.int/dashboards/covid19/cases (accessed on 10 July 2024).
- Jacobsen, H.; Katzmarzyk, M.; Higdon, M.M.; Jiménez, V.C.; Sitaras, I.; Bar-Zeev, N.; Knoll, M.D. Post-Vaccination Neutralization Responses to Omicron Sub-Variants. Vaccines 2022, 10, 1757. [Google Scholar] [CrossRef]
- Zhan, X.-Y.; Chen, Y.; Zhang, X.; Shi, Q.; Chen, K.; Zeng, C.; Zhang, Y.; Liang, Y.; Li, W.; Li, M.; et al. Characterization of SARS-CoV-2-specific humoral immunity and associated factors in the healthy population post-vaccination. Vaccine 2024, 42, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Kang, A.Y.H.; Tay, C.J.X.; Li, H.E.; Elyana, N.; Tan, C.W.; Yap, W.C.; Lim, J.M.E.; Le Bert, N.; Chan, K.R.; et al. Correlates of protection against symptomatic SARS-CoV-2 in vaccinated children. Nat. Med. 2024, 30, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- McClelland, L.; Hare, R. The adsorption of influenza virus by red cells and a new in vitro method of measuring antibodies for influenza virus. Can. Public Health J. 1941, 32, 530–538. [Google Scholar]
- Donald, H.B.; Isaacs, A. Counts of influenza virus particles. J. Gen. Microbiol. 1954, 10, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Hertz, T.; Levy, S.; Ostrovsky, D.; Oppenheimer, H.; Zismanov, S.; Kuzmina, A.; Friedman, L.M.; Trifkovic, S.; Brice, D.; Chun-Yang, L.; et al. Correlates of protection for booster doses of the SARS-CoV-2 vaccine BNT162b2. Nat. Commun. 2023, 14, 4575. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Lustig, Y.; Joseph, G.; Gilboa, M.; Barda, N.; Gens, I.; Indenbaum, V.; Halpern, O.; Katz-Likvornik, S.; Levin, T.; et al. Correlates of protection against COVID-19 infection and intensity of symptomatic disease in vaccinated individuals exposed to SARS-CoV-2 in households in Israel (ICoFS): A prospective cohort study. Lancet Microbe 2023, 4, e309–e318. [Google Scholar] [CrossRef]
- Mbaeyi, S.; Oliver, S.E.; Collins, J.P.; Godfrey, M.; Goswami, N.D.; Hadler, S.C.; Jones, J.; Moline, H.; Moulia, D.; Reddy, S.; et al. The Advisory Committee on Immunization Practices’ Interim Recommendations for Additional Primary and Booster Doses of COVID-19 Vaccines—United States, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1545–1552. [Google Scholar] [CrossRef]
- Riepler, L.; Rössler, A.; Falch, A.; Volland, A.; Borena, W.; von Laer, D.; Kimpel, J. Comparison of Four SARS-CoV-2 Neutralization Assays. Vaccines 2020, 9, 13. [Google Scholar] [CrossRef]
- Jacobsen, H.; Sitaras, I.; Katzmarzyk, M.; Cobos Jiménez, V.; Naughton, R.; Higdon, M.M.; Deloria Knoll, M. Systematic review and meta-analysis of the factors affecting waning of post-vaccination neutralizing antibody responses against SARS-CoV-2. NPJ Vaccines 2023, 8, 159. [Google Scholar] [CrossRef] [PubMed]
- Sitaras, I.; Jacobsen, H.; Higdon, M.M.; Dowling, W.E.; Bar-Zeev, N.; Deloria Knoll, M. Systematic review of primary and booster COVID-19 sera neutralizing ability against SARS-CoV-2 omicron variant. NPJ Vaccines 2022, 7, 147. [Google Scholar] [CrossRef]
- VIEW-Hub by IVAC. Neutralization Studies|ViewHub. Available online: https://view-hub.org/vaccine/covid/neutralization-studies (accessed on 10 July 2024).
- Katzmarzyk, M.; Clesle, D.C.; van den Heuvel, J.; Hoffmann, M.; Garritsen, H.; Pöhlmann, S.; Jacobsen, H.; Čičin-Šain, L. Systematical assessment of the impact of single spike mutations of SARS-CoV-2 Omicron sub-variants on the neutralization capacity of post-vaccination sera. Front. Immunol. 2023, 14, 1288794. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, H.; Sitaras, I.; Jurgensmeyer, M.; Mulders, M.N.; Goldblatt, D.; Feikin, D.R.; Bar-Zeev, N.; Higdon, M.M.; Knoll, M.D. Assessing the Reliability of SARS-CoV-2 Neutralization Studies That Use Post-Vaccination Sera. Vaccines 2022, 10, 850. [Google Scholar] [CrossRef]
- Xie, X.; Liu, Y.; Liu, J.; Zhang, X.; Zou, J.; Fontes-Garfias, C.R.; Xia, H.; Swanson, K.A.; Cutler, M.; Cooper, D.; et al. Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K and N501Y variants by BNT162b2 vaccine-elicited sera. Nat. Med. 2021, 27, 620–621. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Dejnirattisai, W.; Supasa, P.; Liu, C.; Mentzer, A.J.; Ginn, H.M.; Zhao, Y.; Duyvesteyn, H.M.E.; Tuekprakhon, A.; Nutalai, R.; et al. Evidence of escape of SARS-CoV-2 variant B.1.351 from natural and vaccine-induced sera. Cell 2021, 184, 2348–2361.e6. [Google Scholar] [CrossRef]
- Garcia-Beltran, W.F.; Lam, E.C.; St Denis, K.; Nitido, A.D.; Garcia, Z.H.; Hauser, B.M.; Feldman, J.; Pavlovic, M.N.; Gregory, D.J.; Poznansky, M.C.; et al. Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. Cell 2021, 184, 2372–2383.e9. [Google Scholar] [CrossRef]
- Wang, P.; Casner, R.G.; Nair, M.S.; Wang, M.; Yu, J.; Cerutti, G.; Liu, L.; Kwong, P.D.; Huang, Y.; Shapiro, L.; et al. Increased resistance of SARS-CoV-2 variant P.1 to antibody neutralization. Cell Host Microbe 2021, 29, 747–751.e4. [Google Scholar] [CrossRef]
- Collier, D.A.; de Marco, A.; Ferreira, I.A.T.M.; Meng, B.; Datir, R.P.; Walls, A.C.; Kemp, S.A.; Bassi, J.; Pinto, D.; Silacci-Fregni, C.; et al. Sensitivity of SARS-CoV-2 B.1.1.7 to mRNA vaccine-elicited antibodies. Nature 2021, 593, 136–141. [Google Scholar] [CrossRef]
- Muik, A.; Wallisch, A.-K.; Sänger, B.; Swanson, K.A.; Mühl, J.; Chen, W.; Cai, H.; Maurus, D.; Sarkar, R.; Türeci, Ö.; et al. Neutralization of SARS-CoV-2 lineage B.1.1.7 pseudovirus by BNT162b2 vaccine-elicited human sera. Science 2021, 371, 1152–1153. [Google Scholar] [CrossRef]
- Wu, K.; Werner, A.P.; Koch, M.; Choi, A.; Narayanan, E.; Stewart-Jones, G.B.E.; Colpitts, T.; Bennett, H.; Boyoglu-Barnum, S.; Shi, W.; et al. Serum Neutralizing Activity Elicited by mRNA-1273 Vaccine. N. Engl. J. Med. 2021, 384, 1468–1470. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Baillie, V.; Cutland, C.L.; Voysey, M.; Koen, A.L.; Fairlie, L.; Padayachee, S.D.; Dheda, K.; Barnabas, S.L.; Bhorat, Q.E.; et al. Efficacy of the ChAdOx1 nCoV-19 Covid-19 Vaccine against the B.1.351 Variant. N. Engl. J. Med. 2021, 384, 1885–1898. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Arora, P.; Groß, R.; Seidel, A.; Hörnich, B.F.; Hahn, A.S.; Krüger, N.; Graichen, L.; Hofmann-Winkler, H.; Kempf, A.; et al. SARS-CoV-2 variants B.1.351 and P.1 escape from neutralizing antibodies. Cell 2021, 184, 2384–2393.e12. [Google Scholar] [CrossRef] [PubMed]
- Kuzmina, A.; Khalaila, Y.; Voloshin, O.; Keren-Naus, A.; Boehm-Cohen, L.; Raviv, Y.; Shemer-Avni, Y.; Rosenberg, E.; Taube, R. SARS-CoV-2 spike variants exhibit differential infectivity and neutralization resistance to convalescent or post-vaccination sera. Cell Host Microbe 2021, 29, 522–528.e2. [Google Scholar] [CrossRef]
- Edara, V.V.; Norwood, C.; Floyd, K.; Lai, L.; Davis-Gardner, M.E.; Hudson, W.H.; Mantus, G.; Nyhoff, L.E.; Adelman, M.W.; Fineman, R.; et al. Infection- and vaccine-induced antibody binding and neutralization of the B.1.351 SARS-CoV-2 variant. Cell Host Microbe 2021, 29, 516–521.e3. [Google Scholar] [CrossRef] [PubMed]
- Stamatatos, L.; Czartoski, J.; Wan, Y.-H.; Homad, L.J.; Rubin, V.; Glantz, H.; Neradilek, M.; Seydoux, E.; Jennewein, M.F.; MacCamy, A.J.; et al. mRNA vaccination boosts cross-variant neutralizing antibodies elicited by SARS-CoV-2 infection. Science 2021, 372, 1413–1418. [Google Scholar] [CrossRef]
- Planas, D.; Bruel, T.; Grzelak, L.; Guivel-Benhassine, F.; Staropoli, I.; Porrot, F.; Planchais, C.; Buchrieser, J.; Rajah, M.M.; Bishop, E.; et al. Sensitivity of infectious SARS-CoV-2 B.1.1.7 and B.1.351 variants to neutralizing antibodies. Nat. Med. 2021, 27, 917–924. [Google Scholar] [CrossRef]
- Emary, K.R.W.; Golubchik, T.; Aley, P.K.; Ariani, C.V.; Angus, B.; Bibi, S.; Blane, B.; Bonsall, D.; Cicconi, P.; Charlton, S.; et al. Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern 202012/01 (B.1.1.7): An exploratory analysis of a randomised controlled trial. Lancet 2021, 397, 1351–1362. [Google Scholar] [CrossRef]
- Dejnirattisai, W.; Zhou, D.; Supasa, P.; Liu, C.; Mentzer, A.J.; Ginn, H.M.; Zhao, Y.; Duyvesteyn, H.M.E.; Tuekprakhon, A.; Nutalai, R.; et al. Antibody evasion by the P.1 strain of SARS-CoV-2. Cell 2021, 184, 2939–2954.e9. [Google Scholar] [CrossRef]
- Shen, X.; Tang, H.; McDanal, C.; Wagh, K.; Fischer, W.; Theiler, J.; Yoon, H.; Li, D.; Haynes, B.F.; Sanders, K.O.; et al. SARS-CoV-2 variant B.1.1.7 is susceptible to neutralizing antibodies elicited by ancestral spike vaccines. Cell Host Microbe 2021, 29, 529–539.e3. [Google Scholar] [CrossRef]
- Wang, P.; Nair, M.S.; Liu, L.; Iketani, S.; Luo, Y.; Guo, Y.; Wang, M.; Yu, J.; Zhang, B.; Kwong, P.D.; et al. Antibody resistance of SARS-CoV-2 variants B.1.351 and B.1.1.7. Nature 2021, 593, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, J.; Xia, H.; Zhang, X.; Fontes-Garfias, C.R.; Swanson, K.A.; Cai, H.; Sarkar, R.; Chen, W.; Cutler, M.; et al. Neutralizing Activity of BNT162b2-Elicited Serum. N. Engl. J. Med. 2021, 384, 1466–1468. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, J.; Xia, H.; Zhang, X.; Zou, J.; Fontes-Garfias, C.R.; Weaver, S.C.; Swanson, K.A.; Cai, H.; Sarkar, R.; et al. BNT162b2-Elicited Neutralization against New SARS-CoV-2 Spike Variants. N. Engl. J. Med. 2021, 385, 472–474. [Google Scholar] [CrossRef] [PubMed]
- Bates, T.A.; Leier, H.C.; Lyski, Z.L.; McBride, S.K.; Coulter, F.J.; Weinstein, J.B.; Goodman, J.R.; Lu, Z.; Siegel, S.A.R.; Sullivan, P.; et al. Neutralization of SARS-CoV-2 variants by convalescent and BNT162b2 vaccinated serum. Nat. Commun. 2021, 12, 5135. [Google Scholar] [CrossRef]
- Wang, G.-L.; Wang, Z.-Y.; Duan, L.-J.; Meng, Q.-C.; Jiang, M.-D.; Cao, J.; Yao, L.; Zhu, K.-L.; Cao, W.-C.; Ma, M.-J. Susceptibility of Circulating SARS-CoV-2 Variants to Neutralization. N. Engl. J. Med. 2021, 384, 2354–2356. [Google Scholar] [CrossRef]
- Geers, D.; Shamier, M.C.; Bogers, S.; den Hartog, G.; Gommers, L.; Nieuwkoop, N.N.; Schmitz, K.S.; Rijsbergen, L.C.; van Osch, J.A.T.; Dijkhuizen, E.; et al. SARS-CoV-2 variants of concern partially escape humoral but not T-cell responses in COVID-19 convalescent donors and vaccinees. Sci. Immunol. 2021, 6, eabj1750. [Google Scholar] [CrossRef]
- Anichini, G.; Terrosi, C.; Gori Savellini, G.; Gandolfo, C.; Franchi, F.; Cusi, M.G. Neutralizing Antibody Response of Vaccinees to SARS-CoV-2 Variants. Vaccines 2021, 9, 517. [Google Scholar] [CrossRef]
- Cao, Y.; Yisimayi, A.; Bai, Y.; Huang, W.; Li, X.; Zhang, Z.; Yuan, T.; An, R.; Wang, J.; Xiao, T.; et al. Humoral immune response to circulating SARS-CoV-2 variants elicited by inactivated and RBD-subunit vaccines. Cell Res. 2021, 31, 732–741. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.; Dulovic, A.; Junker, D.; Ruetalo, N.; Kaiser, P.D.; Pinilla, Y.T.; Heinzel, C.; Haering, J.; Traenkle, B.; Wagner, T.R.; et al. Immune response to SARS-CoV-2 variants of concern in vaccinated individuals. Nat. Commun. 2021, 12, 3109. [Google Scholar] [CrossRef]
- Tan, N.H.; Geers, D.; Sablerolles, R.S.G.; Rietdijk, W.J.R.; Goorhuis, A.; Postma, D.F.; Visser, L.G.; Bogers, S.; van Dijk, L.L.A.; Gommers, L.; et al. Immunogenicity of bivalent omicron (BA.1) booster vaccination after different priming regimens in health-care workers in the Netherlands (SWITCH ON): Results from the direct boost group of an open-label, multicentre, randomised controlled trial. Lancet Infect. Dis. 2023, 23, 901–913. [Google Scholar] [CrossRef]
- Chen, J.-J.; Li, L.-B.; Peng, H.-H.; Tian, S.; Ji, B.; Shi, C.; Qian, C.; Jiang, W.-G.; Liu, M.-C.; Li, T.-T.; et al. Neutralization against XBB.1 and XBB.1.5 after omicron subvariants breakthrough infection or reinfection. Lancet Reg. Health West. Pac. 2023, 33, 100759. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ciric, C.; Gibson, T.; Anderson, L.J.; Anderson, E.J.; Rostad, C.A. Longitudinal Neutralizing and Functional Antibody Responses to Severe Acute Respiratory Syndrome Coronavirus 2 Variants Following Messenger RNA Coronavirus Disease 2019 Vaccination. Open Forum Infect. Dis. 2023, 10, ofad167. [Google Scholar] [CrossRef]
- Chen, Z.; Huang, T.; He, T.; Zha, G.; Zhu, Q.; Zhang, G.; Xiang, D.; Chen, M.; Li, H.; Ling, N.; et al. Humoral responses after primary and booster SARS-CoV-2 inactivated vaccination in patients with chronic hepatitis B virus infection: A longitudinal observational study. J. Med. Virol. 2023, 95, e28695. [Google Scholar] [CrossRef]
- Yamasoba, D.; Uriu, K.; Plianchaisuk, A.; Kosugi, Y.; Pan, L.; Zahradnik, J.; Ito, J.; Sato, K. Virological characteristics of the SARS-CoV-2 omicron XBB.1.16 variant. Lancet Infect. Dis. 2023, 23, 655–656. [Google Scholar] [CrossRef] [PubMed]
- Ren, W.; Zhang, Y.; Rao, J.; Wang, Z.; Lan, J.; Liu, K.; Zhang, X.; Hu, X.; Yang, C.; Zhong, G.; et al. Evolution of Immune Evasion and Host Range Expansion by the SARS-CoV-2 B.1.1.529 (Omicron) Variant. mBio 2023, 14, e0041623. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Zhang, Q.; Zhong, J.; Chen, L.; Jiang, W.; Huang, T.; Li, Y.; Zhang, Y.; Xu, L.; Wang, X.; et al. Omicron BA.1 breakthrough infections in inactivated COVID-19 vaccine recipients induced distinct pattern of antibody and T cell responses to different Omicron sublineages. Emerg. Microbes Infect. 2023, 12, 2202263. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, Z.; Zhuang, X.; Zhang, S.; Chen, Z.; Zou, Y.; Sheng, J.; Li, T.; Tai, W.; Yu, J.; et al. Inactivated vaccine-elicited potent antibodies can broadly neutralize SARS-CoV-2 circulating variants. Nat. Commun. 2023, 14, 2179. [Google Scholar] [CrossRef]
- Hernández, J.; Dehesa-Canseco, F.; Vázquez-López, A.B.; Reséndiz-Sandoval, M.; Caire-Juvera, G.; Solís-Hernández, M.; Valenzuela, O.; Gómez-Gil, B.; Mata-Haro, V. Neutralization of Omicron BA.1, BA.5.1.6, BQ.1.3 and XBB1.1 induced by heterologous vaccination Ad5-nCoV and mRNA-1273. Signal Transduct. Target. Ther. 2023, 8, 174. [Google Scholar] [CrossRef]
- Diem, G.; Jäger, M.; Dichtl, S.; Bauer, A.; Lass-Flörl, C.; Reindl, M.; Wilflingseder, D.; Posch, W. Vaccination and Omicron BA.1/BA.2 Convalescence Enhance Systemic but Not Mucosal Immunity against BA.4/5. Microbiol. Spectr. 2023, 11, e0516322. [Google Scholar] [CrossRef]
- Yamamoto, S.; Matsuda, K.; Maeda, K.; Oshiro, Y.; Inamura, N.; Mizoue, T.; Konishi, M.; Takeuchi, J.S.; Horii, K.; Ozeki, M.; et al. Omicron BA.1 neutralizing antibody response following Delta breakthrough infection compared with booster vaccination of BNT162b2. BMC Infect. Dis. 2023, 23, 282. [Google Scholar] [CrossRef]
- Cui, Z.; Luo, W.; Chen, R.; Li, Y.; Wang, Z.; Liu, Y.; Liu, S.; Feng, L.; Jia, Z.; Cheng, R.; et al. Comparing T- and B-cell responses to COVID-19 vaccines across varied immune backgrounds. Signal Transduct. Target. Ther. 2023, 8, 179. [Google Scholar] [CrossRef]
- Faraone, J.N.; Qu, P.; Evans, J.P.; Zheng, Y.-M.; Carlin, C.; Anghelina, M.; Stevens, P.; Fernandez, S.; Jones, D.; Lozanski, G.; et al. Neutralization escape of Omicron XBB, BR.2, and BA.2.3.20 subvariants. Cell Rep. Med. 2023, 4, 101049. [Google Scholar] [CrossRef]
- Carr, E.J.; Wu, M.Y.; Gahir, J.; Harvey, R.; Townsley, H.; Bailey, C.; Fowler, A.S.; Dowgier, G.; Hobbs, A.; Herman, L.; et al. Neutralising immunity to omicron sublineages BQ.1.1, XBB, and XBB.1.5 in healthy adults is boosted by bivalent BA.1-containing mRNA vaccination and previous Omicron infection. Lancet Infect. Dis. 2023, 23, 781–784. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Huang, B.; Deng, Y.; Zhang, S.; Liu, X.; Wang, L.; Liu, Q.; Zhao, L.; Tang, L.; Wang, W.; et al. Neutralizing antibody levels associated with injectable and aerosolized Ad5-nCoV boosters and BA.2 infection. BMC Med. 2023, 21, 233. [Google Scholar] [CrossRef]
- Vikse, E.L.; Fossum, E.; Erdal, M.S.; Hungnes, O.; Bragstad, K. Poor neutralizing antibody responses against SARS-CoV-2 Omicron BQ.1.1 and XBB in Norway in October 2022. Influenza Other Respir. Viruses 2023, 17, e13144. [Google Scholar] [CrossRef]
- Toyoda, M.; Tan, T.S.; Motozono, C.; Barabona, G.; Yonekawa, A.; Shimono, N.; Minami, R.; Nagasaki, Y.; Miyashita, Y.; Oshiumi, H.; et al. Evaluation of Neutralizing Activity against Omicron Subvariants in BA.5 Breakthrough Infection and Three-Dose Vaccination Using a Novel Chemiluminescence-Based, Virus-Mediated Cytopathic Assay. Microbiol. Spectr. 2023, 11, e0066023. [Google Scholar] [CrossRef]
- Yang, J.; Hong, W.; Lei, H.; He, C.; Lei, W.; Zhou, Y.; Zhao, T.; Alu, A.; Ma, X.; Li, J.; et al. Low levels of neutralizing antibodies against XBB Omicron subvariants after BA.5 infection. Signal Transduct. Target. Ther. 2023, 8, 252. [Google Scholar] [CrossRef]
- Muangnoicharoen, S.; Wiangcharoen, R.; Nanthapisal, S.; Kamolratakul, S.; Lawpoolsri, S.; Jongkaewwattana, A.; Thitithanyanont, A.; Luvira, V.; Chinwangso, P.; Thanthamnu, N.; et al. Single Ad26.COV2.S booster dose following two doses of BBIBP-CorV vaccine against SARS-CoV-2 infection in adults: Day 28 results of a phase 1/2 open-label trial. Vaccine 2023, 41, 4648–4657. [Google Scholar] [CrossRef]
- Radion, E.I.; Mukhin, V.E.; Kholodova, A.V.; Vladimirov, I.S.; Alsaeva, D.Y.; Zhdanova, A.S.; Ulasova, N.Y.; Bulanova, N.V.; Makarov, V.V.; Keskinov, A.A.; et al. Functional Characteristics of Serum Anti-SARS-CoV-2 Antibodies against Delta and Omicron Variants after Vaccination with Sputnik V. Viruses 2023, 15, 1349. [Google Scholar] [CrossRef] [PubMed]
- Jin, P.-F.; Guo, X.-L.; Gou, J.-B.; Hou, L.-H.; Song, Z.-Z.; Zhu, T.; Pan, H.-X.; Zhu, J.-H.; Shi, F.-J.; Du, P.; et al. Immunogenicity and safety of heterologous immunisation with Ad5-nCOV in healthy adults aged 60 years and older primed with an inactivated SARS-CoV-2 vaccine (CoronaVac): A phase 4, randomised, observer-blind, non-inferiority trial. Lancet Reg. Health West. Pac. 2023, 38, 100829. [Google Scholar] [CrossRef] [PubMed]
- Dowell, A.C.; Lancaster, T.; Bruton, R.; Ireland, G.; Bentley, C.; Sylla, P.; Zuo, J.; Scott, S.; Jadir, A.; Begum, J.; et al. Immunological imprinting of humoral immunity to SARS-CoV-2 in children. Nat. Commun. 2023, 14, 3845. [Google Scholar] [CrossRef] [PubMed]
- Varasi, I.; Lai, A.; Fiaschi, L.; Bergna, A.; Gatti, A.; Caimi, B.; Biba, C.; Della Ventura, C.; Balotta, C.; Riva, A.; et al. Neutralizing antibodies response to novel SARS-CoV-2 omicron sublineages in long-term care facility residents after the fourth dose of monovalent BNT162b2 COVID-19 vaccination. J. Infect. 2023, 87, 270–272. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Goguet, E.; Paz, S.; Vassell, R.; Pollett, S.; Mitre, E.; Weiss, C.D. Bivalent Coronavirus Disease 2019 Vaccine Antibody Responses to Omicron Variants Suggest That Responses to Divergent Variants Would Be Improved With Matched Vaccine Antigens. J. Infect. Dis. 2023, 228, 439–443. [Google Scholar] [CrossRef]
- Lyke, K.E.; Atmar, R.L.; Dominguez Islas, C.; Posavad, C.M.; Deming, M.E.; Branche, A.R.; Johnston, C.; El Sahly, H.M.; Edupuganti, S.; Mulligan, M.J.; et al. Immunogenicity of NVX-CoV2373 heterologous boost against SARS-CoV-2 variants. npj Vaccines 2023, 8, 98. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Nie, J.; Li, Q.; Wu, J.; Zhao, C.; Hao, H.; Liu, H.; Zhang, L.; Nie, L.; Qin, H.; Wang, M.; et al. Establishment and validation of a pseudovirus neutralization assay for SARS-CoV-2. Emerg. Microbes Infect. 2020, 9, 680–686. [Google Scholar] [CrossRef]
- Pastorio, C.; Noettger, S.; Nchioua, R.; Zech, F.; Sparrer, K.M.J.; Kirchhoff, F. Impact of mutations defining SARS-CoV-2 Omicron subvariants BA.2.12.1 and BA.4/5 on Spike function and neutralization. iScience 2023, 26, 108299. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.J.; Lapedes, A.S.; De-Jong, J.C.; Bestebroer, T.M.; Jones, T.C.; Rimmelzwaan, G.F.; Osterhaus, A.D.M.; Fouchier, R.A.M. Mutations, Drift, and the Influenza Archipelago. Discov. Med. 2009, 4, 371–377. [Google Scholar]
- Smith, D.J.; Lapedes, A.S.; de Jong, J.C.; Bestebroer, T.M.; Rimmelzwaan, G.F.; Osterhaus, A.D.M.E.; Fouchier, R.A.M. Mapping the antigenic and genetic evolution of influenza virus. Science 2004, 305, 371–376. [Google Scholar] [CrossRef]
- Yamanaka, T.; Cullinane, A.; Gildea, S.; Bannai, H.; Nemoto, M.; Tsujimura, K.; Kondo, T.; Matsumura, T. The potential impact of a single amino-acid substitution on the efficacy of equine influenza vaccines. Equine Vet. J. 2015, 47, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Categories | Parameters | ||
|---|---|---|---|
| 1 | Sample size | 1.1 | How many samples were included? |
| 2 | SARS-CoV-2 infection | 2.1 | Was any SARS-CoV-2 infection prior to completion of the primary vaccine regimen considered? |
| 2.2 | Was presence or absence of pre-vaccination infection confirmed? | ||
| 2.3 | Were breakthrough infections considered in the study cohort? | ||
| 2.4 | Were breakthrough infections confirmed? | ||
| 2.5 | Were infection-naïve/previously infected/ breakthrough infected samples stratified in the analyses? | ||
| 3 | Vaccination regimen | 3.1 | Do the authors report booster dosing interval? |
| 3.2 | Are the booster dosing intervals comparable? | ||
| 3.3 | Do the authors stratify for partial and complete primary regimen? | ||
| 4 | Sample collection period | 4.1 | Were all samples taken at least seven days post last immunogenic event? |
| 4.2 | Are the results stratified, OR are all samples taken ≥ two weeks and ≤ 4 months post-last immunogenic event? | ||
| 5 | Demographic characterization | 5.1 | Is the age distribution of all subjects reported? |
| 5.2 | Are results stratified by age group? | ||
| 5.3 | Is the sex distribution of all participants reported? | ||
| 5.4 | If only a subgroup of the initial study cohort was analyzed, did the cohort selection happen unbiased? | ||
| 5.5 | Was the infecting variant/ or variant prevalence reported? | ||
| 5.6 | Was the study period and geographic location reported? | ||
| 5.7 | If (multiple) breakthrough infections occurred, were the results stratified for the infecting variant(s)? | ||
| 6 | Clinical characterization | 6.1 | Is any relevant clinical characterization reported? |
| 6.2 | Are the results stratified for immunocompromised? | ||
| 7 | Protocol | 7.1 | Is the precise assay type and endpoint reported? |
| 7.2 | Do the authors provide a precise protocol for the neutralization assay within the manuscript? | ||
| 8 | Live virus | 8.1 | Is the virus lineage reported? |
| 8.2 | Has the sequence been confirmed by sequencing? | ||
| 9 | Pseudo-virus | 9.1 | Are the construct details reported? |
| 9.2 | Are all variant-associated spike mutations included in the pseudo-virus? | ||
| 9.3 | Has the sequence been confirmed by sequencing? | ||
| 10 | Assay standardization | 10.1 | Is the amount of infectious virus input (virus titer) used for neutralization assays reported, and if so, are they consistent and have a small input variance? |
| 10.2 | Was the intended virus titer used for neutralization assays confirmed by back-titration or virus controls? | ||
| 10.3 | Are precise details on cell culture reported? | ||
| 11 | Data reporting | 11.1 | Is the raw data for neutralization titers reported? |
| 11.2 | Is the reference virus used for calculating variant-specific fold changes reasonable? | ||
| 11.3 | Are appropriate statistics provided? | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katzmarzyk, M.; Naughton, R.; Sitaras, I.; Jacobsen, H.; Higdon, M.M.; Deloria Knoll, M. Evaluating the Quality of Studies Assessing COVID-19 Vaccine Neutralizing Antibody Immunogenicity. Vaccines 2024, 12, 1238. https://doi.org/10.3390/vaccines12111238
Katzmarzyk M, Naughton R, Sitaras I, Jacobsen H, Higdon MM, Deloria Knoll M. Evaluating the Quality of Studies Assessing COVID-19 Vaccine Neutralizing Antibody Immunogenicity. Vaccines. 2024; 12(11):1238. https://doi.org/10.3390/vaccines12111238
Chicago/Turabian StyleKatzmarzyk, Maeva, Robert Naughton, Ioannis Sitaras, Henning Jacobsen, Melissa M. Higdon, and Maria Deloria Knoll. 2024. "Evaluating the Quality of Studies Assessing COVID-19 Vaccine Neutralizing Antibody Immunogenicity" Vaccines 12, no. 11: 1238. https://doi.org/10.3390/vaccines12111238
APA StyleKatzmarzyk, M., Naughton, R., Sitaras, I., Jacobsen, H., Higdon, M. M., & Deloria Knoll, M. (2024). Evaluating the Quality of Studies Assessing COVID-19 Vaccine Neutralizing Antibody Immunogenicity. Vaccines, 12(11), 1238. https://doi.org/10.3390/vaccines12111238