
The Potential Risk Compensation after Receiving HPV Vaccination among Men Who Have Sex with Men in Southwest China: A HAPA-Based Analysis


Abstract
:1. Introduction
2. Materials and Methods
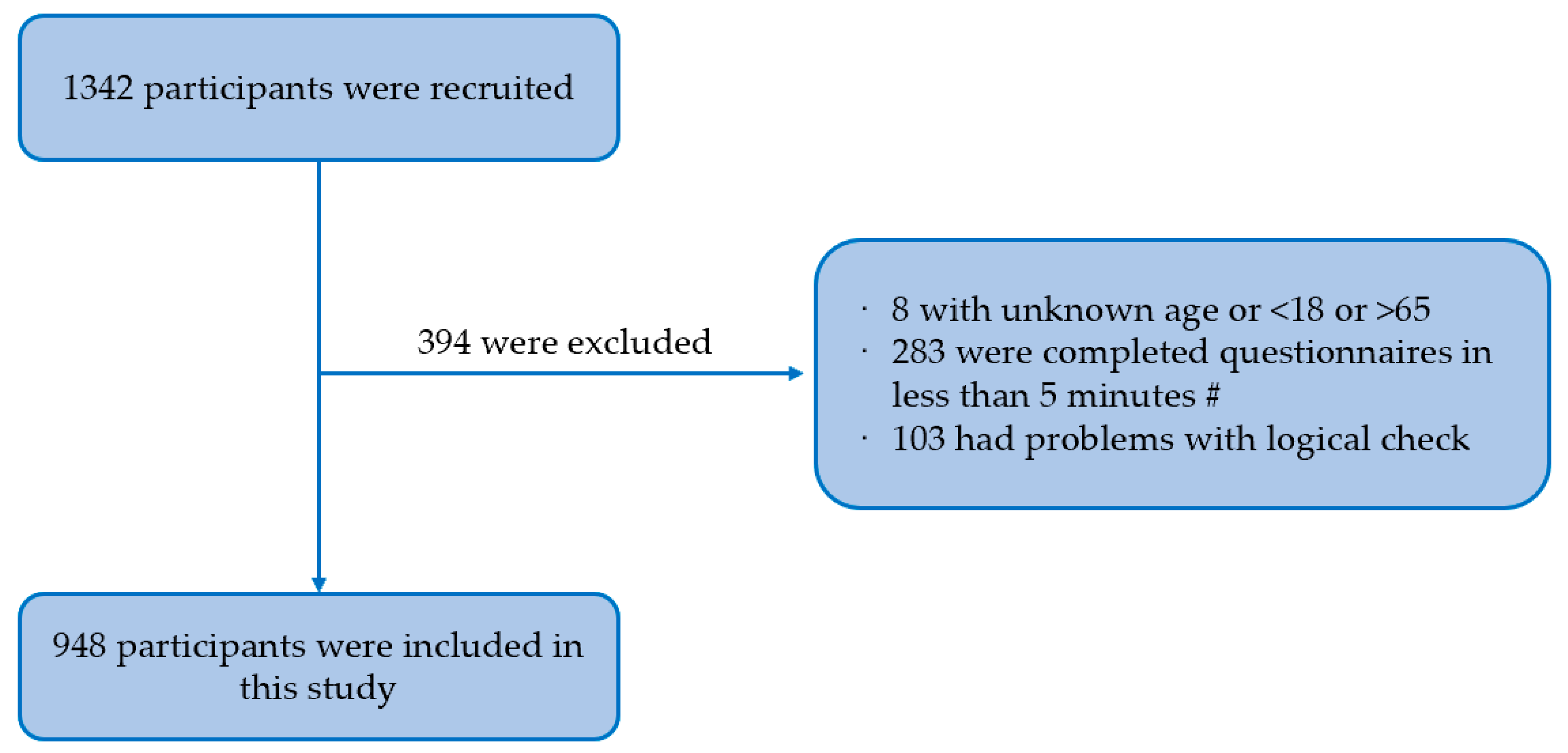
2.1. Participants and Recruitment
2.2. Measurements
2.2.1. Background Characteristics
2.2.2. HAPA Scale
2.3. Statistical Analysis
3. Results
3.1. Background Characteristics
3.2. Measurement Model
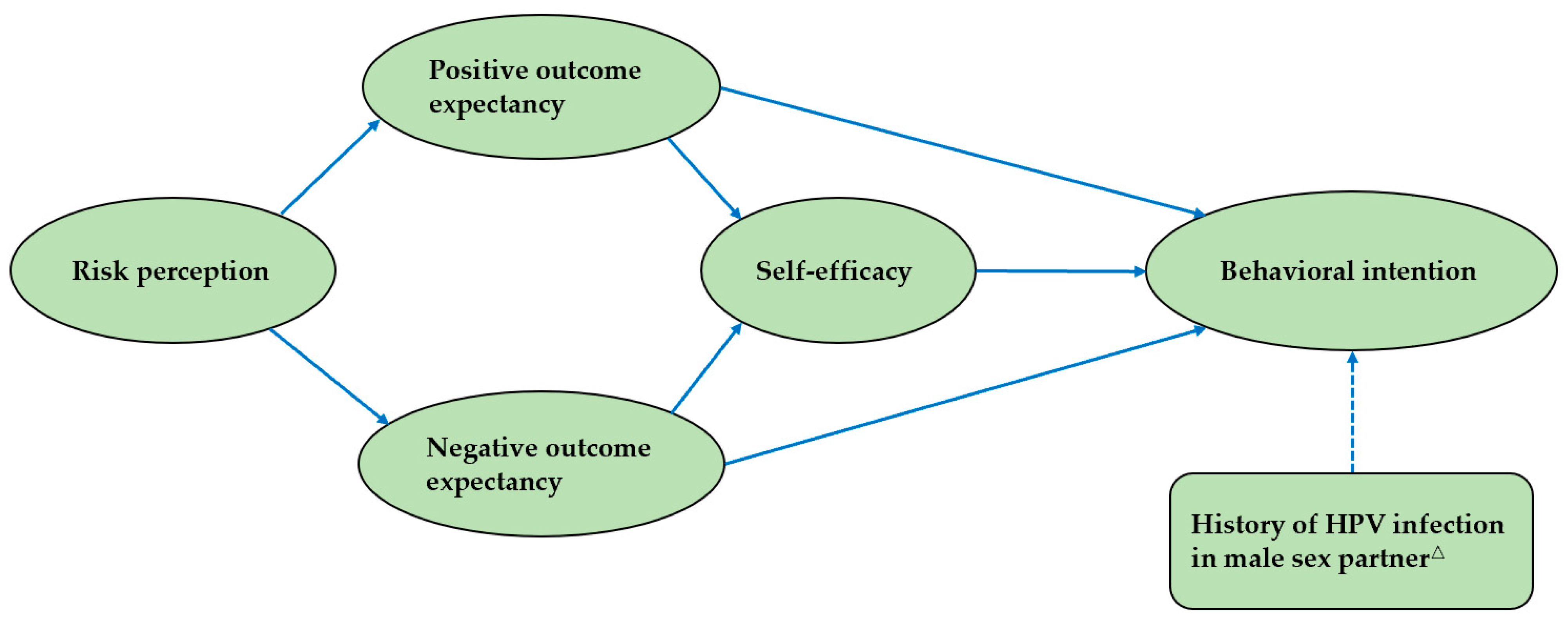
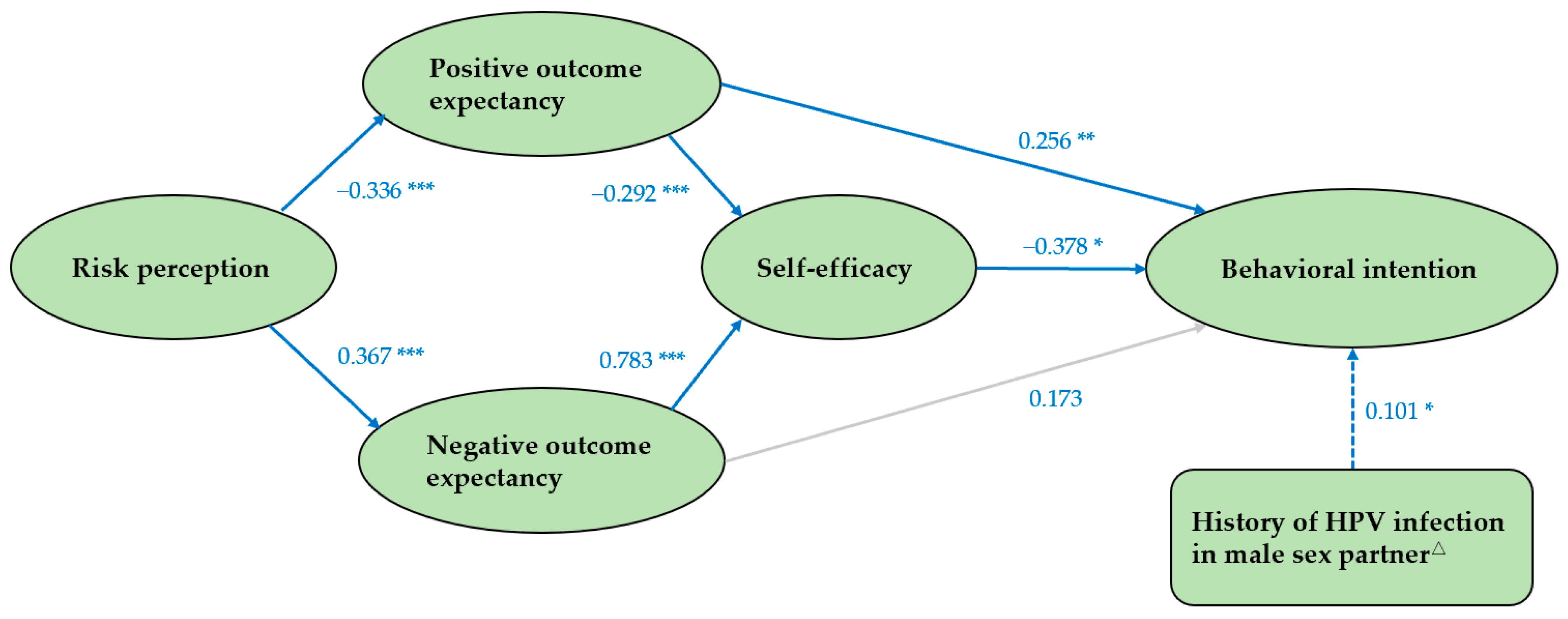
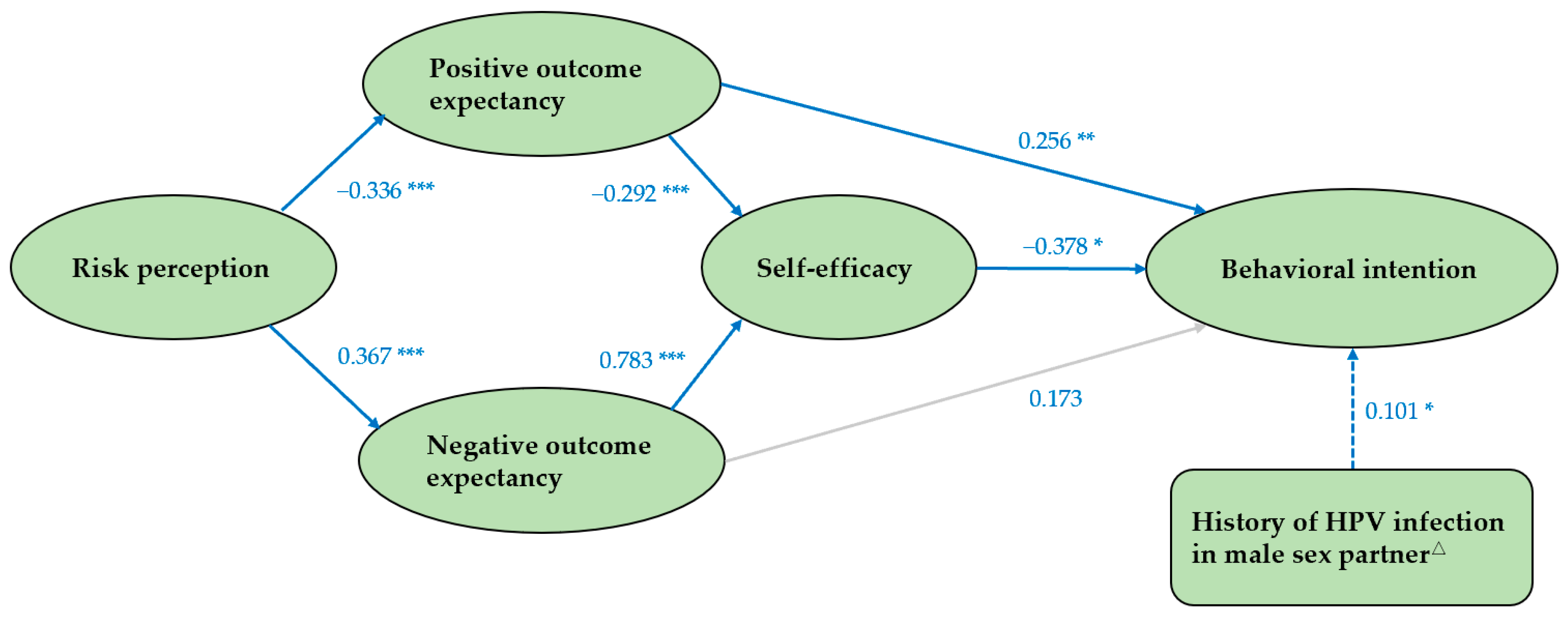
3.3. Structural Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tian, T.; Wang, D.; Papamichael, C.; Yan, Z.; Guoyao, S.; Zhanlin, Z.; Mahan, Y.; Xiaoqing, T.; Zheng, G.; Jianghong, D. HPV vaccination acceptability among men who have sex with men in Urumqi, China. Hum. Vaccin. Immunother. 2019, 15, 1005–1012. [Google Scholar] [CrossRef]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Marra, E.; Lin, C.; Clifford, G.M. Type-Specific Anal Human Papillomavirus Prevalence Among Men, According to Sexual Preference and HIV Status: A Systematic Literature Review and Meta-Analysis. J. Infect. Dis. 2019, 219, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Wang, Q.; Ong, J.J.; Fairley, C.K.; Su, S.; Peng, P.; Jing, J.; Wang, L.; Soe, N.N.; Cheng, F.; et al. Prevalence of human papillomavirus by geographical regions, sexual orientation and HIV status in China: A systematic review and meta-analysis. Sex. Transm. Infect. 2018, 94, 434–442. [Google Scholar] [CrossRef]
- Zhou, Y.; Lin, Y.F.; Gao, L.; Dai, J.; Luo, G.; Li, L.; Yuan, T.; Li, P.; Zhan, Y.; Gao, Y.; et al. Human papillomavirus prevalence among men who have sex with men in China: A systematic review and meta-analysis. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2021, 40, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Machalek, D.A.; Poynten, M.; Jin, F.; Fairley, C.K.; Farnsworth, A.; Garland, S.M.; Hillman, R.J.; Petoumenos, K.; Roberts, J.; Tabrizi, S.N.; et al. Anal human papillomavirus infection and associated neoplastic lesions in men who have sex with men: A systematic review and meta-analysis. Lancet Oncol. 2012, 13, 487–500. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.P.; Tucker, J.D.; Wong, F.Y.; Nehl, E.J.; Wang, Y.; Zhuang, X.; Zhang, L. Disparities and risks of sexually transmissible infections among men who have sex with men in China: A meta-analysis and data synthesis. PLoS ONE 2014, 9, e89959. [Google Scholar] [CrossRef] [PubMed]
- Lacey, C.J.; Lowndes, C.M.; Shah, K.V. Chapter 4: Burden and management of non-cancerous HPV-related conditions: HPV-6/11 disease. Vaccine 2006, 24 (Suppl. S3), S35–S41. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; Chaturvedi, A.K.; Lowy, D.R. HPV prophylactic vaccines and the potential prevention of noncervical cancers in both men and women. Cancer 2008, 113, 3036–3046. [Google Scholar] [CrossRef] [PubMed]
- Olesen, T.B.; Sand, F.L.; Rasmussen, C.L.; Albieri, V.; Toft, B.G.; Norrild, B.; Munk, C.; Kjær, S.K. Prevalence of human papillomavirus DNA and p16(INK4a) in penile cancer and penile intraepithelial neoplasia: A systematic review and meta-analysis. Lancet Oncol. 2019, 20, 145–158. [Google Scholar] [CrossRef]
- Ren, X.; Qiu, L.; Ke, W.; Zou, H.; Liu, A.; Wu, T. Awareness and acceptance of HPV vaccination for condyloma acuminata among men who have sex with men in China. Hum. Vaccin. Immunother. 2022, 18, 2115267. [Google Scholar] [CrossRef]
- Petrosky, E.; Bocchini, J.A., Jr.; Hariri, S.; Chesson, H.; Curtis, C.R.; Saraiya, M.; Unger, E.R.; Markowitz, L.E. Use of 9-valent human papillomavirus (HPV) vaccine: Updated HPV vaccination recommendations of the advisory committee on immunization practices. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 300–304. [Google Scholar] [PubMed]
- Zhang, L.; Regan, D.G.; Ong, J.J.; Gambhir, M.; Chow, E.P.F.; Zou, H.; Law, M.; Hocking, J.; Fairley, C.K. Targeted human papillomavirus vaccination for young men who have sex with men in Australia yields significant population benefits and is cost-effective. Vaccine 2017, 35, 4923–4929. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J. Targeted human papillomavirus vaccination of men who have sex with men in the USA: A cost-effectiveness modelling analysis. Lancet Infect. Dis. 2010, 10, 845–852. [Google Scholar] [CrossRef]
- Ben Hadj Yahia, M.B.; Jouin-Bortolotti, A.; Dervaux, B. Extending the Human Papillomavirus Vaccination Programme to Include Males in High-Income Countries: A Systematic Review of the Cost-Effectiveness Studies. Clin. Drug Investig. 2015, 35, 471–485. [Google Scholar] [CrossRef]
- Markowitz, L.E.; Dunne, E.F.; Saraiya, M.; Chesson, H.W.; Curtis, C.R.; Gee, J.; Bocchini, J.A., Jr.; Unger, E.R. Human papillomavirus vaccination: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2014, 63, 1–30. [Google Scholar]
- Human papillomavirus vaccines: WHO position paper, May 2017-Recommendations. Vaccine 2017, 35, 5753–5755. [CrossRef] [PubMed]
- Huang, R.; Wang, Z.; Yuan, T.; Nadarzynski, T.; Qian, H.Z.; Li, P.; Meng, X.; Wang, G.; Zhou, Y.; Luo, D.; et al. Using protection motivation theory to explain the intention to initiate human papillomavirus vaccination among men who have sex with men in China. Tumour Virus Res. 2021, 12, 200222. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Pan, H.; Lin, B.; Zhong, X. Analysis of HPV Vaccination Willingness amongst HIV-Negative Men Who Have Sex with Men in China. Vaccines 2021, 9, 1069. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; He, W.; Lin, B.; Zhong, X. Factors influencing HPV vaccination willingness among men who have sex with men in China: A structural equation modeling analysis. Hum. Vaccin. Immunother. 2022, 18, 2038504. [Google Scholar] [CrossRef]
- Wilde, G.J. Risk homeostasis theory: An overview. Inj. Prev. J. Int. Soc. Child Adolesc. Inj. Prev. 1998, 4, 89–91. [Google Scholar] [CrossRef]
- Traeger, M.W.; Cornelisse, V.J.; Asselin, J.; Price, B.; Roth, N.J.; Willcox, J.; Tee, B.K.; Fairley, C.K.; Chang, C.C.; Armishaw, J.; et al. Association of HIV Preexposure Prophylaxis With Incidence of Sexually Transmitted Infections Among Individuals at High Risk of HIV Infection. JAMA 2019, 321, 1380–1390. [Google Scholar] [CrossRef] [PubMed]
- Golub, S.A.; Kowalczyk, W.; Weinberger, C.L.; Parsons, J.T. Preexposure prophylaxis and predicted condom use among high-risk men who have sex with men. J. Acquir. Immune Defic. Syndr. 2010, 54, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Qu, S.; Fang, Y.; Ip, M.; Wang, Z. Behavioral intention to perform risk compensation behaviors after receiving HPV vaccination among men who have sex with men in China. Hum. Vaccin. Immunother. 2019, 15, 1737–1744. [Google Scholar] [CrossRef]
- Hansen, B.T. No evidence that HPV vaccination leads to sexual risk compensation. Hum. Vaccin. Immunother. 2016, 12, 1451–1453. [Google Scholar] [CrossRef]
- Schwarzer, R.; Schuz, B.; Ziegelmann, J.P.; Lippke, S.; Luszczynska, A.; Scholz, U. Adoption and maintenance of four health behaviors: Theory-guided longitudinal studies on dental flossing, seat belt use, dietary behavior, and physical activity. Ann. Behav. Med. Publ. Soc. Behav. Med. 2007, 33, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Lippke, S.; Luszczynska, A. Mechanisms of health behavior change in persons with chronic illness or disability: The Health Action Process Approach (HAPA). Rehabil. Psychol. 2011, 56, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.R.; Kroon, J.; Schwarzer, R.; Hamilton, K. Social-cognitive predictors of parental supervised toothbrushing: An application of the health action process approach. Br. J. Health Psychol. 2021, 26, 995–1015. [Google Scholar] [CrossRef] [PubMed]
- Tsui, H.Y.; Lau, J.T.; Wang, Z.; Gross, D.L.; Wu, A.M.; Cao, W.; Gu, J.; Li, S. Applying the pre-intentional phase of the Health Action Process Approach (HAPA) Model to investigate factors associated with intention on consistent condom use with various types of female sex partners among males who inject drugs in China. AIDS Care 2016, 28, 1079–1088. [Google Scholar] [CrossRef]
- Williams, R.J.; Herzog, T.A.; Simmons, V.N. Risk perception and motivation to quit smoking: A partial test of the Health Action Process Approach. Addict. Behav. 2011, 36, 789–791. [Google Scholar] [CrossRef] [PubMed]
- Scholz, U.; Keller, R.; Perren, S. Predicting behavioral intentions and physical exercise: A test of the health action process approach at the intrapersonal level. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2009, 28, 702–708. [Google Scholar] [CrossRef]
- Payaprom, Y.; Bennett, P.; Alabaster, E.; Tantipong, H. Using the Health Action Process Approach and implementation intentions to increase flu vaccine uptake in high risk Thai individuals: A controlled before-after trial. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2011, 30, 492–500. [Google Scholar] [CrossRef]
- Yu, Y.; Jia, W.; Lau, M.M.C.; Lau, J.T.F. Levels and factors derived from the Health Action Process Approach of behavioral intentions to take up COVID-19 vaccination: A random population-based study. Vaccine 2022, 40, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Ni, Y.; Lu, Y.; He, X.; Li, Y.; Li, Y.; Guo, S.; Ong, J.J.; Xu, C.; Wang, X.; Yan, X.; et al. Self-sampled specimens demonstrate comparable accuracy and consistency to clinician-sampled specimens for HPV detection among men who have sex with men in China. Sex. Transm. Infect. 2022, 99, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Luo, Y.; Zhong, R.; Law, P.T.Y.; Boon, S.S.; Chen, Z.; Wong, C.H.; Chan, P.K.S. Role of polycyclic aromatic hydrocarbons as a co-factor in human papillomavirus-mediated carcinogenesis. BMC Cancer 2019, 19, 138. [Google Scholar] [CrossRef]
- Vawda, N.; Banerjee, R.N.; Debenham, B.J. Impact of Smoking on Outcomes of HPV-related Oropharyngeal Cancer Treated with Primary Radiation or Surgery. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Camargo, M.; Del Río-Ospina, L.; Soto-De León, S.C.; Sánchez, R.; Pineda-Peña, A.C.; Sussmann, O.; Patarroyo, M.E.; Patarroyo, M.A. Association of HIV status with infection by multiple HPV types. Trop. Med. Int. Health TM IH 2018, 23, 1259–1268. [Google Scholar] [CrossRef]
- Giannini, A.; Di Donato, V.; Sopracordevole, F.; Ciavattini, A.; Ghelardi, A.; Vizza, E.; D’Oria, O.; Simoncini, T.; Plotti, F.; Casarin, J.; et al. Outcomes of High-Grade Cervical Dysplasia with Positive Margins and HPV Persistence after Cervical Conization. Vaccines 2023, 11, 698. [Google Scholar] [CrossRef]
- Newman, P.A.; Lee, S.J.; Duan, N.; Rudy, E.; Nakazono, T.K.; Boscardin, J.; Kakinami, L.; Shoptaw, S.; Diamant, A.; Cunningham, W.E. Preventive HIV vaccine acceptability and behavioral risk compensation among a random sample of high-risk adults in Los Angeles (LA VOICES). Health Serv. Res. 2009, 44, 2167–2179. [Google Scholar] [CrossRef]
- Marlow, L.A.; Forster, A.S.; Wardle, J.; Waller, J. Mothers’ and adolescents’ beliefs about risk compensation following HPV vaccination. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2009, 44, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.X.; Chen, L.L.; Chen, W.Y.; Zhang, M.X.; Yang, M.G.; Mo, L.C.; Zhu, J.J.; Tung, T.H.; Li, F.P. Association between health behaviours and the COVID-19 vaccination: Risk compensation among healthcare workers in Taizhou, China. Hum. Vaccin. Immunother. 2022, 18, 2029257. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Lau, J.T.; Gu, J. Acceptability of circumcision among clients of female sex worker in Hong Kong. AIDS Behav. 2012, 16, 1836–1845. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.T.; Zhang, J.; Yan, H.; Lin, C.; Choi, K.C.; Wang, Z.; Hao, C.; Huan, X.; Yang, H. Acceptability of circumcision as a means of HIV prevention among men who have sex with men in China. AIDS Care 2011, 23, 1472–1482. [Google Scholar] [CrossRef]
- Newman, P.A.; Roungprakhon, S.; Tepjan, S.; Yim, S. Preventive HIV vaccine acceptability and behavioral risk compensation among high-risk men who have sex with men and transgenders in Thailand. Vaccine 2010, 28, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Feng, T.; Lau, J.T. Prevalence and associated factors of behavioral intention for risk compensation following voluntary medical male circumcision among male sexually transmitted diseases patients in China. AIDS Care 2016, 28, 1332–1337. [Google Scholar] [CrossRef] [PubMed]
- Giano, Z.; Kavanaugh, K.E.; Durham, A.R.; Currin, J.M.; Wheeler, D.L.; Croff, J.M.; Hubach, R.D. Factors Associated with Condom Use among a Sample of Men Who Have Sex with Men (MSM) Residing in Rural Oklahoma. J. Homosex. 2020, 67, 1881–1901. [Google Scholar] [CrossRef]
- Hoff, C.C.; Chakravarty, D.; Beougher, S.C.; Neilands, T.B.; Darbes, L.A. Relationship characteristics associated with sexual risk behavior among MSM in committed relationships. AIDS Patient Care STDs 2012, 26, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Klein, H. Condom use self-efficacy and HIV risk practices among men who use the internet to find male partners for unprotected sex. Am. J. Men’s Health 2014, 8, 190–204. [Google Scholar] [CrossRef]
- Tucker, J.S.; Elliott, M.N.; Wenzel, S.L.; Hambarsoomian, K. Relationship commitment and its implications for unprotected sex among impoverished women living in shelters and low-income housing in Los Angeles County. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2007, 26, 644–649. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, A.; Jemmott, L.S.; Jemmott, J.B. Mediation analysis of an effective sexual risk-reduction intervention for women: The importance of self-efficacy. Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2008, 27, S180–S184. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Constructs | Value Assignment |
|---|---|
| Risk perception RP1 How likely you think HPV infection is to cause anal, penile, or oral cancer. RP2 HPV infection increases the risk of HIV infection. RP3 Genital warts can be a serious hazard to your health. RP4 Cancer of the anus, penis, or mouth can cause serious harm to your health. | 1 = very small, 2 = small, 3 = average, 4 = large, 5 = very large 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree |
| Positive outcome expectancy POE1 Condomless anal intercourse will increase intimacy between you and your male sex partner. POE2 Condomless anal intercourse will increase trust between you and your male sex partner. | 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree |
| Negative outcome expectancy NOE1 Condomless anal intercourse can give you HPV. NOE2 Condomless anal intercourse can give you other STDs. NOE3 Condomless anal intercourse will make you worried. | 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree |
| Self-efficacy SE1 You are confident to use condoms consistently no matter what your condition is. SE2 You are confident to use condom consistently even when your sex partner is not willing to use it. SE3 Even if you want to be intimate with your sex partner, you have the confidence to use condom consistently. SE4 You are confident that you can suggest condom use without your sex partner thinking that you are worried about him getting an STD. | 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree |
| Behavioral intention BI How condom use may change when you have anal sex with your male sex partner after receiving HPV vaccination. | 1 = very likely to increase, 2 = likely to increase, 3 = remain the same, 4 = likely to reduce, 5 = very likely to reduce |
| Variable | N | % | Variable | N | % |
|---|---|---|---|---|---|
| Sociodemographic characteristics | Sexual behavior characteristics | ||||
| Age | (in the past six months) | ||||
| 18–27 | 567 | 59.8 | Number of male partners | ||
| 28–45 | 310 | 32.7 | 0 | 217 | 22.9 |
| >45 | 71 | 7.5 | 1 | 415 | 43.8 |
| Household registration | ≥2 | 316 | 33.3 | ||
| Urban areas | 566 | 59.7 | Condom use when having anal sex with a male partner | ||
| Rural areas | 382 | 40.3 | Every time | 460 | 48.5 |
| Ethnicity | Sometimes | 140 | 14.8 | ||
| Han nationality | 907 | 95.7 | Rarely | 62 | 6.5 |
| Other ethnic minorities | 41 | 4.3 | No anal sex | 286 | 30.2 |
| Educational level | Whether had male sex partners who had been infected with HPV | ||||
| Junior high and below | 59 | 6.2 | No | 720 | 76 |
| High school | 158 | 16.7 | Unclear | 208 | 21.9 |
| Junior college | 213 | 22.5 | Yes | 20 | 2.1 |
| College and above | 518 | 54.6 | Whether had been diagnosed with an STD by a doctor | ||
| Employment status | No | 916 | 96.6 | ||
| Employed | 522 | 55.1 | Yes | 32 | 3.4 |
| Retired or unemployed | 96 | 10.1 | HPV-related preventive behavior # | ||
| Students | 330 | 34.8 | HPV counseling | ||
| Marital status | Done | 393 | 41.5 | ||
| Unmarried | 792 | 83.5 | Never | 555 | 58.5 |
| Married | 80 | 8.4 | HPV vaccine-related intentions | ||
| Divorced/widowed | 76 | 8.0 | Whether were willing to receive HPV vaccine | ||
| Personal monthly income | very unwilling or unwilling | 17 | 1.8 | ||
| 1000 RMB or less | 139 | 14.7 | uncertain | 102 | 10.8 |
| 1001~3000 RMB | 317 | 33.4 | very willing or willing | 829 | 87.5 |
| 3001~5000 RMB | 233 | 24.6 | How condom use may change when having anal sex with male sex partner after receiving HPV vaccination | ||
| 5001~10,000 RMB | 195 | 20.6 | very likely or likely to increase | 251 | 26.5 |
| 10,000 RMB or more | 64 | 6.8 | remain the same | 563 | 59.4 |
| very likely or likely to reduce | 134 | 14.1 |
| Construct | Mean | SD | Factor Loading | CR (>0.7) | AVE (>0.5) | Cronbach’s Alpha |
|---|---|---|---|---|---|---|
| RP | 3.637 | 0.784 | 0.578–0.863 | 0.836 | 0.567 | 0.766 |
| POE | 2.613 | 1.154 | 0.929–0.931 | 0.928 | 0.865 | 0.899 |
| NOE | 3.817 | 0.846 | 0.733–0.909 | 0.889 | 0.729 | 0.830 |
| SE | 3.922 | 0.865 | 0.863–0.931 | 0.949 | 0.823 | 0.930 |
| BI | 2.759 | 0.999 | - | - | - | - |
| RP | POE | NOE | SE | BI | |
|---|---|---|---|---|---|
| RP | 0.753 | ||||
| POE | −0.336 *** | 0.930 | |||
| NOE | 0.367 *** | −0.123 *** | 0.854 | ||
| SE | 0.386 *** | −0.389 *** | 0.819 *** | 0.907 | |
| BI | −0.168 *** | 0.382 *** | −0.168 ** | −0.336 *** | — |
| Path | Standardized Direct Effect | Standardized Indirect Effect | Standardized Total Effect |
|---|---|---|---|
| Risk perception → Behavioral intention | - | −0.232 * | −0.232 * |
| Positive outcome expectancy → Behavioral intention | 0.256 * | 0.110 * | 0.366 * |
| Negative outcome expectancy → Behavioral intention | - | −0.296 * | −0.296 * |
| Self-efficacy → Behavioral intention | −0.378 * | - | −0.378 * |
| History of HPV infection in male sex partner → Behavioral intention | 0.101 * | - | 0.101 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, Z.; Jiang, H.; He, W.; Pan, H.; Zhang, C.; Zhong, X. The Potential Risk Compensation after Receiving HPV Vaccination among Men Who Have Sex with Men in Southwest China: A HAPA-Based Analysis. Vaccines 2023, 11, 1429. https://doi.org/10.3390/vaccines11091429
Cao Z, Jiang H, He W, Pan H, Zhang C, Zhong X. The Potential Risk Compensation after Receiving HPV Vaccination among Men Who Have Sex with Men in Southwest China: A HAPA-Based Analysis. Vaccines. 2023; 11(9):1429. https://doi.org/10.3390/vaccines11091429
Chicago/Turabian StyleCao, Zhen, Han Jiang, Wei He, Haiying Pan, Cong Zhang, and Xiaoni Zhong. 2023. "The Potential Risk Compensation after Receiving HPV Vaccination among Men Who Have Sex with Men in Southwest China: A HAPA-Based Analysis" Vaccines 11, no. 9: 1429. https://doi.org/10.3390/vaccines11091429
APA StyleCao, Z., Jiang, H., He, W., Pan, H., Zhang, C., & Zhong, X. (2023). The Potential Risk Compensation after Receiving HPV Vaccination among Men Who Have Sex with Men in Southwest China: A HAPA-Based Analysis. Vaccines, 11(9), 1429. https://doi.org/10.3390/vaccines11091429