
Weaker Effects of the Fourth Dose of BNT162b2 SARS-CoV-2 Vaccine on the Elderly Human Population


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Antibodies against SARS-CoV-2 Spike Protein
2.3. Antibodies against SARS-CoV-2 Nucleocapsid Protein
2.4. SARS-CoV-2 Neutralizing Antibodies
2.5. Molecular Diagnosis
2.6. Statistical Analyses
3. Results
3.1. Patient Characteristics
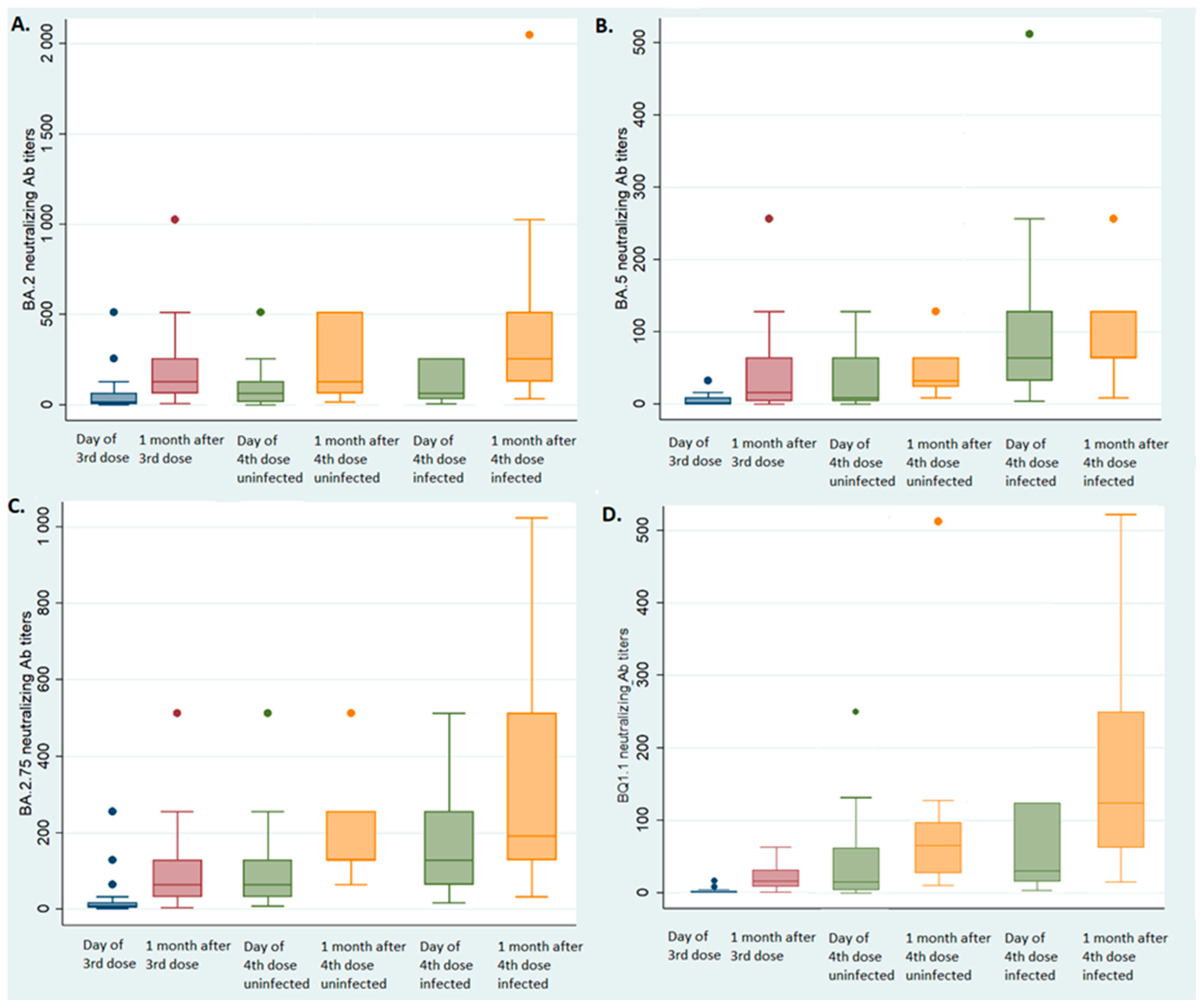
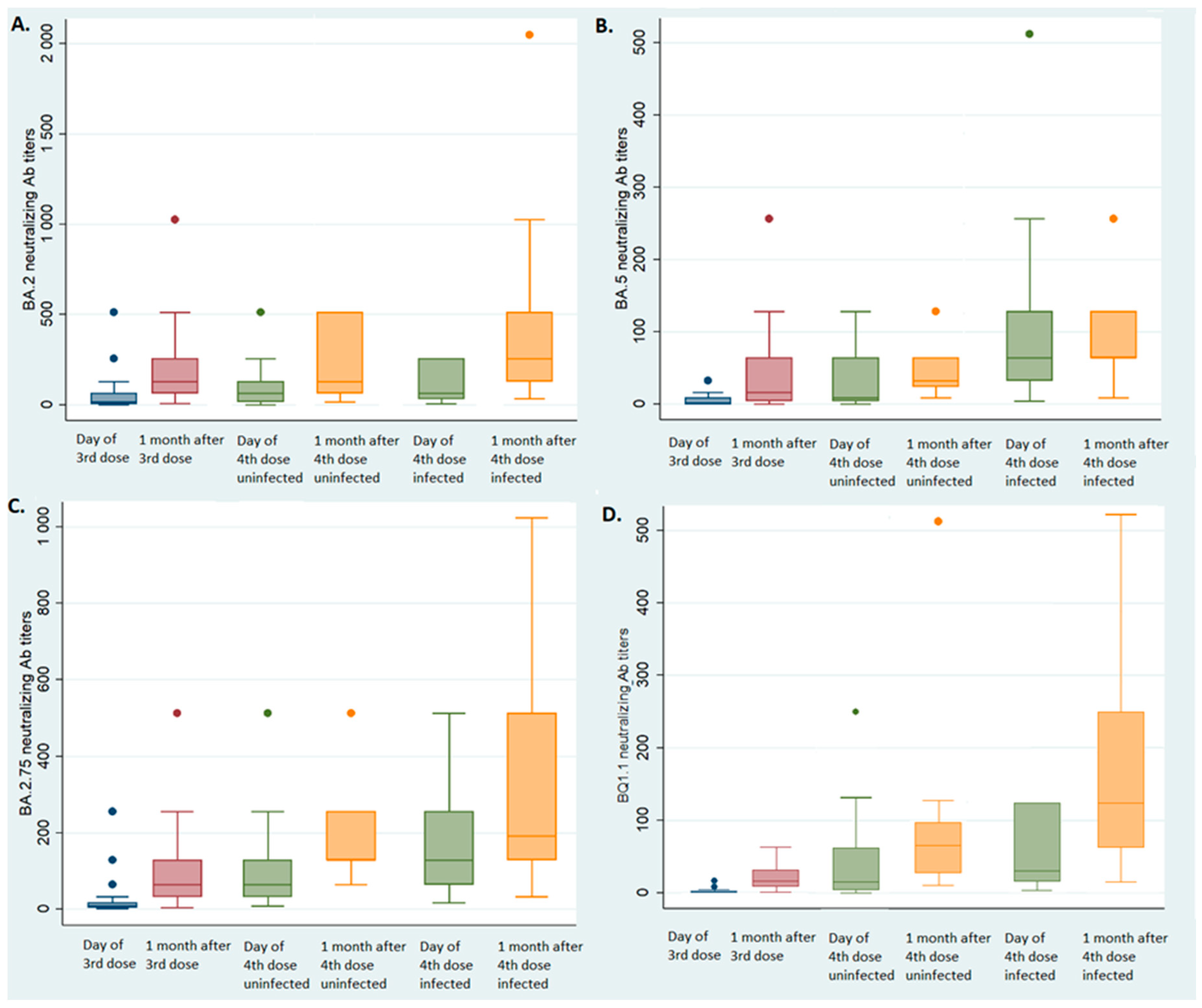
3.2. Effect of the Third and the Fourth Vaccine Dose on NAb
3.3. Effect of the Third Vaccine Dose
3.4. Effect of the Fourth Vaccine Dose in Uninfected Individuals
3.5. Effect of the Fourth Dose on Individuals Infected between the Third and Fourth Vaccine Doses
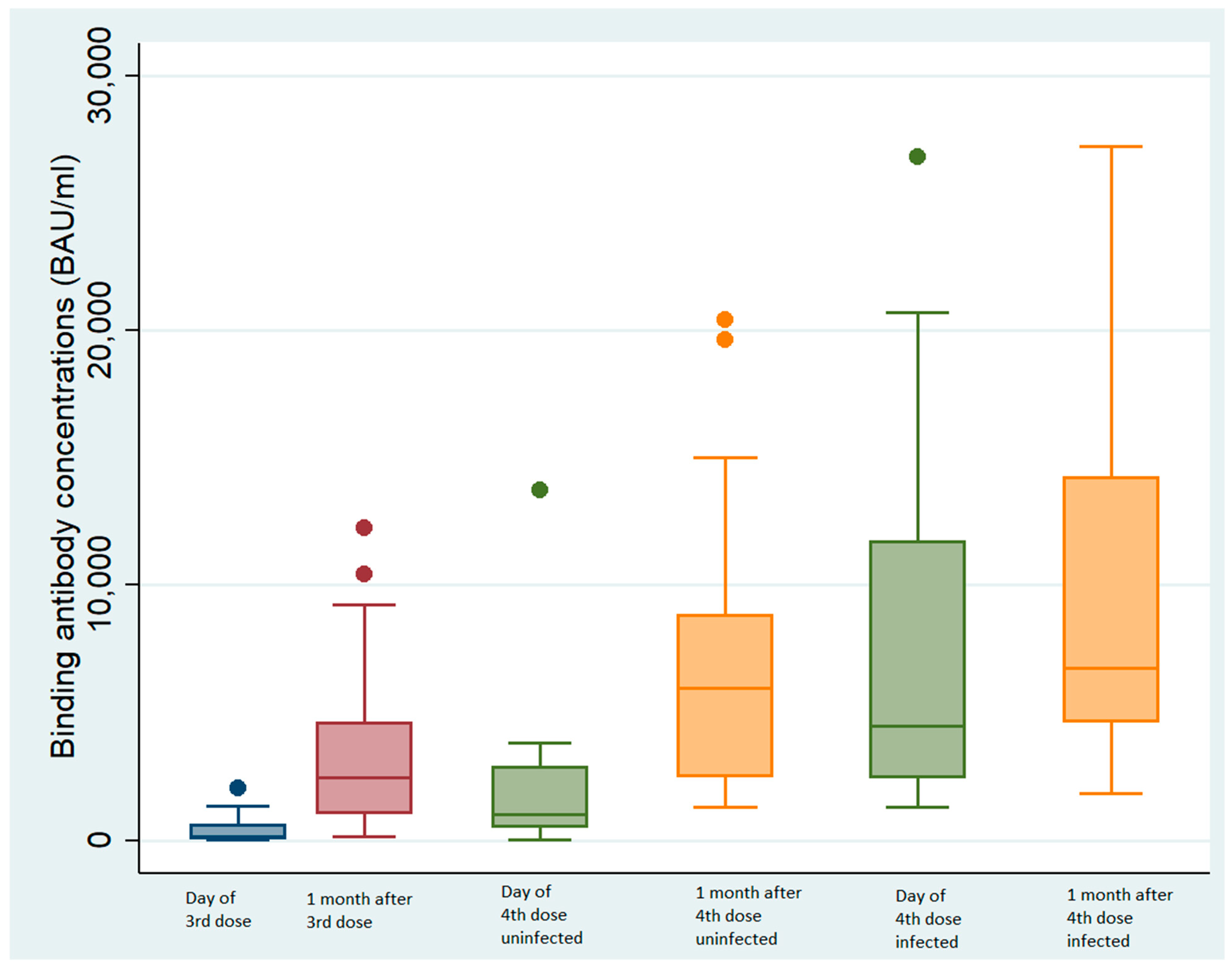
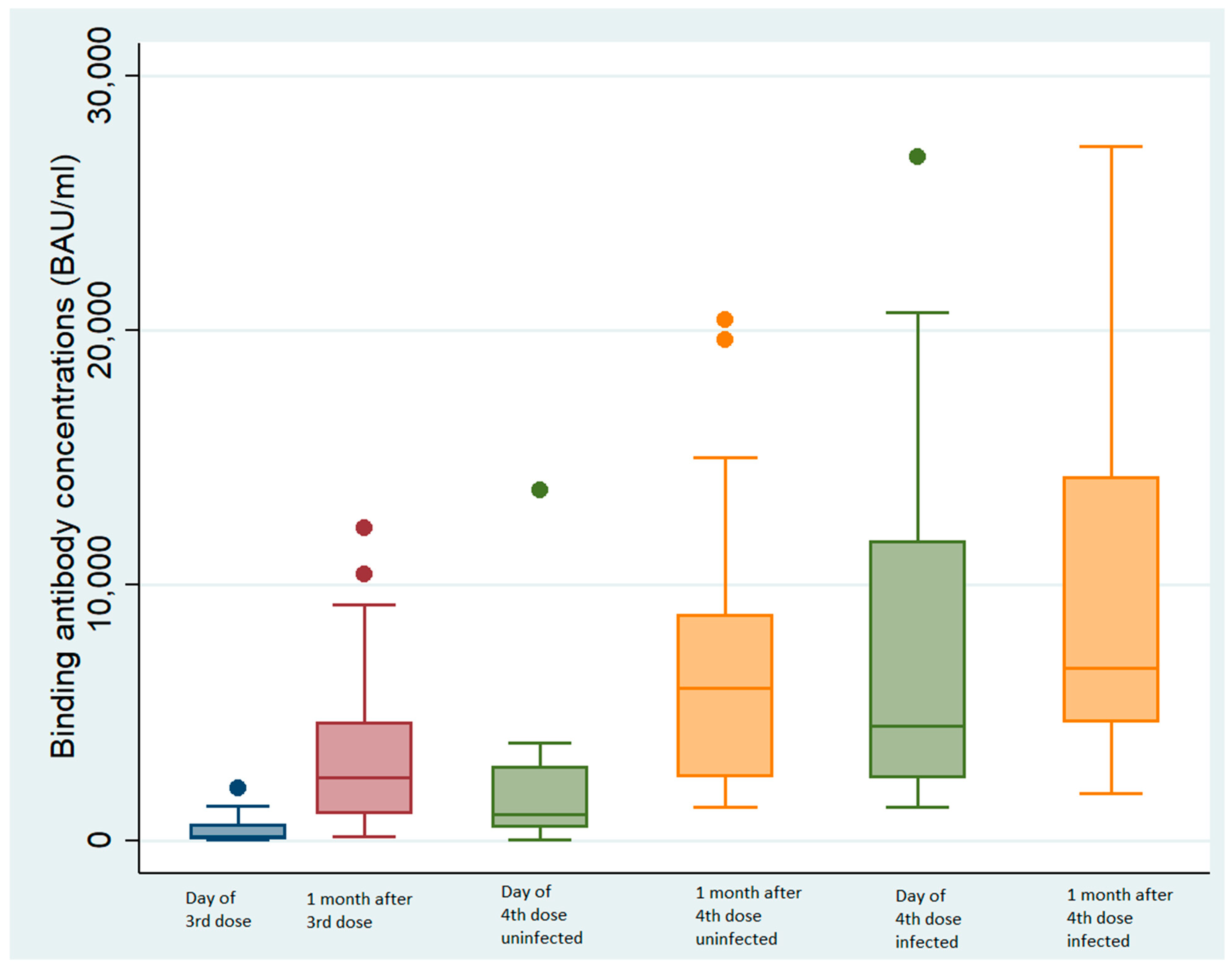
3.6. Effect of the Third and Fourth Doses on BAb
3.6.1. Third Dose
3.6.2. Fourth Dose in Uninfected Individuals
3.6.3. Fourth Dose on Individuals Infected between the Third and the Fourth Antibody Doses
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bartleson, J.M.; Radenkovic, D.; Covarrubias, A.J.; Furman, D.; Winer, D.A.; Verdin, E. SARS-CoV-2, COVID-19 and the aging immune system. Nat. Aging 2021, 1, 769–782. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. COVID-19: What do we know about omicron sublineages? BMJ 2022, 376, o358. [Google Scholar] [CrossRef] [PubMed]
- Collier, D.A.; Ferreira, I.A.; Kotagiri, P.; Datir, R.P.; Lim, E.Y.; Touizer, E.; Meng, B.; Abdullahi, A.; Elmer, A.; Kingston, N.; et al. Age-related immune response heterogeneity to SARS-CoV-2 vaccine BNT162b2. Nature 2021, 596, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Muhsen, K.; Maimon, N.; Mizrahi, A.; Varticovschi, B.; Bodenheimer, O.; Gelbshtein, U.; Grotto, I.; Cohen, D.; Dagan, R. Effects of BNT162b2 COVID-19 Vaccine Booster in Long-Term Care Facilities in Israel. N. Engl. J. Med. 2022, 386, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Muhsen, K.; Maimon, N.; Mizrahi, A.; Bodenheimer, O.; Cohen, D.; Dagan, R. Association of BNT162b2 vaccine third dose receipt with incidence of SARS-CoV-2 infection, COVID-19-related hospitalization, and death among residents of long-term care facilities, August–October 2021. JAMA Netw. Open 2022, 5, e2219940. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.-Y.; Li, Q.-L.; Jia, Z.-J.; Wu, M.-J.; Liu, Y.-Y.; Lin, L.-R.; Liu, L.-L.; Yang, T.-C. Is the fourth COVID-19 vaccine dose urgently needed? Revelation from a prospective cohort study. J. Infect. 2022, 85, e66–e68. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.M.; Lee, E.J.; Won O, S.; Choi, Y.J.; Lee, H.; Oh, S.J.; Kim, J.-M.; Park, A.K.; Lee, C.Y.; Kim, J.M.; et al. A Seroprevalence Study on Residents in a Senior Care Facility with Breakthrough SARS-CoV-2 Omicron Infection. Viral Immunol. 2023, 36, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Haute Autorité de Santé, Press Release July 2022. Available online: https://www.has-sante.fr/jcms/p_3352553/fr/covid-19-une-dose-de-rappel-vaccinal-additionnelle-ouverte-a-davantage-de-personnes-et-des-delais-precises (accessed on 10 April 2023).
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Amir, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection by a Fourth Dose of BNT162b2 against Omicron in Israel. N. Engl. J. Med. 2022, 386, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Chapuy-Regaud, S.; Miédougé, M.; Abravanel, F.; Da Silva, I.; Porcheron, M.; Fillaux, J.; Diméglio, C.; Izopet, J. Evaluation of Three Quantitative Anti-SARS-CoV-2 Antibody Immunoassays. Microbiol. Spectr. 2021, 9, e01376-21. [Google Scholar] [CrossRef]
- Nicot, F.; Trémeaux, P.; Latour, J.; Carcenac, R.; Demmou, S.; Jeanne, N.; Ranger, N.; De Smet, C.; Raymond, S.; Dimeglio, C.; et al. Whole-genome single molecule real-time sequencing of SARS-CoV-2 Omicron. J. Med. Virol. 2023, 95, e28564. [Google Scholar] [CrossRef] [PubMed]
- Gazit, S.; Saciuk, Y.; Perez, G.; Peretz, A.; Pitzer, V.E.; Patalon, T. Short term, relative effectiveness of four doses versus three doses of BNT162b2 vaccine in people aged 60 years and older in Israel: Retrospective, test negative, case-control study. BMJ 2022, 377, e071113. [Google Scholar] [CrossRef]
- Arbel, R.; Sergienko, R.; Friger, M.; Peretz, A.; Beckenstein, T.; Yaron, S.; Netzer, D.; Hammerman, A. Effectiveness of a second BNT162b2 booster vaccine against hospitalization and death from COVID-19 in adults aged over 60 years. Nat. Med. 2022, 28, 1486–1490. [Google Scholar] [CrossRef] [PubMed]
- Nordström, P.; Ballin, M.; Nordström, A. Effectiveness of a fourth dose of mRNA COVID-19 vaccine against all-cause mortality in long-term care facility residents and in the oldest old: A nationwide, retrospective cohort study in Sweden. Lancet Reg. Health-Eur. 2022, 21, 100466. [Google Scholar] [CrossRef] [PubMed]
- Tseng, H.F.; Ackerson, B.K.; Luo, Y.; Sy, L.S.; Talarico, C.A.; Tian, Y.; Bruxvoort, K.J.; Tubert, E.; Florea, A.; Qian, L.; et al. Effectiveness of mRNA-1273 against SARS-CoV-2 Omicron and Delta variants. Nat. Med. 2022, 28, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of COVID-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.-W.; Lim, B.-L.; Young, B.E.; Yeoh, A.Y.-Y.; Yung, C.-F.; Yap, W.-C.; Althaus, T.; Chia, W.-N.; Zhu, F.; Lye, D.C.; et al. Comparative neutralisation profile of SARS-CoV-2 omicron subvariants BA.2.75 and BA.5. Lancet Microbe 2022, 3, e898. [Google Scholar] [CrossRef] [PubMed]
- Qu, P.; Evans, J.P.; Zheng, Y.-M.; Carlin, C.; Saif, L.J.; Oltz, E.M.; Xu, K.; Gumina, R.J.; Liu, S.-L. Evasion of neutralizing antibody responses by the SARS-CoV-2 BA.2.75 variant. Cell Host Microbe 2022, 30, 1518–1526.e4. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.-L.; Zhu, K.-L.; Wang, X.-J.; Wang, G.-L.; Li, Y.-K.; He, X.-J.; Sun, W.-K.; Huang, P.-X.; Zhang, J.-Z.; Gao, H.-X.; et al. Omicron BQ.1 and BQ.1.1 escape neutralisation by omicron subvariant breakthrough infection. Lancet Infect. Dis. 2023, 23, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Canetti, M.; Barda, N.; Gilboa, M.; Indenbaum, V.; Asraf, K.; Gonen, T.; Weiss-Ottolenghi, Y.; Amit, S.; Doolman, R.; Mendelson, E.; et al. Six-Month Follow-up after a Fourth BNT162b2 Vaccine Dose. N. Engl. J. Med. 2022, 387, 2092–2094. [Google Scholar] [CrossRef] [PubMed]
- Dimeglio, C.; Trémeaux, P.; Herin, F.; Da-Silva, I.; Porcheron, M.; Martin-Blondel, G.; Gernigon, C.; Chapuy-Regaud, S.; Villars, H.; Izopet, J. Post-vaccination SARS-CoV-2 antibody kinetics and protection duration against Omicron in elderly population. J. Infect. 2022, 85, 702–769. [Google Scholar] [CrossRef] [PubMed]
- Vikström, L.; Fjällström, P.; Gwon, Y.-D.; Sheward, D.J.; Wigren-Byström, J.; Evander, M.; Bladh, O.; Widerström, M.; Molnar, C.; Rasmussen, G.; et al. Vaccine-induced correlate of protection against fatal COVID-19 in older and frail adults during waves of neutralization-resistant variants of concern: An observational study. Lancet Reg. Health-Eur. 2023; in press. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimeglio, C.; Da-Silva, I.; Porcheron, M.; Panero, M.-P.; Staes, L.; Trémeaux, P.; Villars, H.; Izopet, J. Weaker Effects of the Fourth Dose of BNT162b2 SARS-CoV-2 Vaccine on the Elderly Human Population. Vaccines 2023, 11, 1095. https://doi.org/10.3390/vaccines11061095
Dimeglio C, Da-Silva I, Porcheron M, Panero M-P, Staes L, Trémeaux P, Villars H, Izopet J. Weaker Effects of the Fourth Dose of BNT162b2 SARS-CoV-2 Vaccine on the Elderly Human Population. Vaccines. 2023; 11(6):1095. https://doi.org/10.3390/vaccines11061095
Chicago/Turabian StyleDimeglio, Chloé, Isabelle Da-Silva, Marion Porcheron, Marie-Pierre Panero, Laetitia Staes, Pauline Trémeaux, Hélène Villars, and Jacques Izopet. 2023. "Weaker Effects of the Fourth Dose of BNT162b2 SARS-CoV-2 Vaccine on the Elderly Human Population" Vaccines 11, no. 6: 1095. https://doi.org/10.3390/vaccines11061095
APA StyleDimeglio, C., Da-Silva, I., Porcheron, M., Panero, M.-P., Staes, L., Trémeaux, P., Villars, H., & Izopet, J. (2023). Weaker Effects of the Fourth Dose of BNT162b2 SARS-CoV-2 Vaccine on the Elderly Human Population. Vaccines, 11(6), 1095. https://doi.org/10.3390/vaccines11061095