
Could Prior COVID-19 Affect the Neutralizing Antibody after the Third BNT162b2 Booster Dose: A Longitudinal Study

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Samples Collection
2.2. Antibody Testing
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Aleem, A.; Akbar Samad, A.B.; Slenker, A.K. Emerging Variants of SARS-CoV-2 And Novel Therapeutics Against Coronavirus (COVID-19). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Alamer, E.; Alhazmi, A.; Qasir, N.A.; Alamer, R.; Areeshi, H.; Gohal, G.; Qadri, M.; Hashem, A.M.; Algaissi, A. Side Effects of COVID-19 Pfizer-BioNTech mRNA Vaccine in Children Aged 12–18 Years in Saudi Arabia. Vaccines 2021, 9, 1297. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Lee, A.; Grigoryan, L.; Arunachalam, P.S.; Scott, M.K.D.; Trisal, M.; Wimmers, F.; Sanyal, M.; Weidenbacher, P.A.; Feng, Y.; et al. Mechanisms of innate and adaptive immunity to the Pfizer-BioNTech BNT162b2 vaccine. Nat. Immunol. 2022, 23, 543–555. [Google Scholar] [CrossRef] [PubMed]
- Tarke, A.; Sidney, J.; Methot, N.; Yu, E.D.; Zhang, Y.; Dan, J.M.; Goodwin, B.; Rubiro, P.; Sutherland, A.; Wang, E.; et al. Impact of SARS-CoV-2 variants on the total CD4+ and CD8+ T cell reactivity in infected or vaccinated individuals. Cell Rep. Med. 2021, 2, 100355. [Google Scholar] [CrossRef] [PubMed]
- Redjoul, R.; Le Bouter, A.; Parinet, V.; Fourati, S.; Maury, S. Antibody response after third BNT162b2 dose in recipients of allogeneic HSCT. Lancet Haematol. 2021, 8, e681–e683. [Google Scholar] [CrossRef] [PubMed]
- Sasso, B.L.; Giglio, R.; Vidali, M.; Scazzone, C.; Bivona, G.; Gambino, C.; Ciaccio, A.; Agnello, L.; Ciaccio, M. Evaluation of Anti-SARS-Cov-2 S-RBD IgG Antibodies after COVID-19 mRNA BNT162b2 Vaccine. Diagnostics 2021, 11, 1135. [Google Scholar] [CrossRef] [PubMed]
- Sancilio, A.E.; D’Aquila, R.T.; McNally, E.M.; Velez, M.P.; Ison, M.G.; Demonbreun, A.R.; McDade, T.W. A surrogate virus neutralization test to quantify antibody-mediated inhibition of SARS-CoV-2 in finger stick dried blood spot samples. Sci. Rep. 2021, 11, 15321. [Google Scholar] [CrossRef] [PubMed]
- Dinc, H.O.; Saltoglu, N.; Can, G.; Balkan, I.I.; Budak, B.; Ozbey, D.; Caglar, B.; Karaali, R.; Mete, B.; Tuyji Tok, Y.; et al. Inactive SARS-CoV-2 vaccine generates high antibody responses in healthcare workers with and without prior infection. Vaccine 2022, 40, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Tuells, J.; Parra-Grande, M.; Santos-Calle, F.J.; Montagud, A.C.; Egoavil, C.M.; García-Rivera, C.; Caballero, P.; Gabaldón-Bravo, E.M.; Rodríguez-Diaz, J.C.; Hurtado-Sánchez, J.A. Detection of Neutralizing Antibodies against SARS-CoV-2 Post-Vaccination in Health Care Workers of a Large Tertiary Hospital in Spain by Using a Rapid Test LFIC and sVNT-ELISA. Vaccines 2022, 10, 510. [Google Scholar] [CrossRef] [PubMed]
- Dinç, H.; Demirci, M.; Özdemir, Y.E.; Sirekbasan, S.; Aktaş, A.N.; Karaali, R.; Tok, Y.T.; Özbey, D.; Akçin, R.; Gareayaghi, N.; et al. Anti-SARS-CoV-2 IgG and Neutralizing Antibody Levels in Patients with Past COVID-19 Infection: A Longitudinal Study. Balk. Med. J. 2022, 39, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Sasso, B.L.; Agnello, L.; Giglio, R.V.; Gambino, C.M.; Ciaccio, A.M.; Vidali, M.; Ciaccio, M. Longitudinal analysis of anti-SARS-CoV-2 S-RBD IgG antibodies before and after the third dose of the BNT162b2 vaccine. Sci. Rep. 2022, 12, 8679. [Google Scholar] [CrossRef] [PubMed]
- Eliakim-Raz, N.; Leibovici-Weisman, Y.; Stemmer, A.; Ness, A.; Awwad, M.; Ghantous, N.; Stemmer, S.M. Antibody Titers Before and After a Third Dose of the SARS-CoV-2 BNT162b2 Vaccine in Adults Aged ≥60 Years. JAMA 2021, 326, 2203–2204. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ibarguengoitia, M.E.; Rivera-Salinas, D.; Hernández-Ruíz, Y.G.; Armendariz-Vázquez, A.G.; González-Cantú, A.; Barco-Flores, I.A.; González-Facio, R.; Montelongo-Cruz, L.P.; Del Rio-Parra, G.F.; Garza-Herrera, M.R.; et al. Effect of the third dose of BNT162b2 vaccine on quantitative SARS-CoV-2 spike 1–2 IgG antibody titers in healthcare personnel. PLoS ONE 2022, 17, e0263942. [Google Scholar] [CrossRef] [PubMed]
- Kontopoulou, K.; Nakas, C.T.; Papazisis, G. Significant Increase in Antibody Titers after the 3rd Booster Dose of the Pfizer-BioNTech mRNA COVID-19 Vaccine in Healthcare Workers in Greece. Vaccines 2022, 10, 876. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Frenck, R.W.; Walsh, E.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Bailey, R.; Swanson, K.A.; Xu, X.; et al. SARS-CoV-2 Neutralization with BNT162b2 Vaccine Dose 3. N. Engl. J. Med. 2021, 385, 1627–1629. [Google Scholar] [CrossRef] [PubMed]
- Matula, Z.; Gönczi, M.; Bekő, G.; Kádár, B.; Ajzner, É.; Uher, F.; Vályi-Nagy, I. Antibody and T Cell Responses against SARS-CoV-2 Elicited by the Third Dose of BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) Vaccines Using a Homologous or Heterologous Booster Vaccination Strategy. Vaccines 2022, 10, 539. [Google Scholar] [CrossRef] [PubMed]
- Cassaniti, I.; Gregorini, M.; Bergami, F.; Arena, F.; Sammartino, J.C.; Percivalle, E.; Soleymaninejadian, E.; Abelli, M.; Ticozzelli, E.; Nocco, A.; et al. Effect of a Third Dose of SARS-CoV-2 mRNA BNT162b2 Vaccine on Humoral and Cellular Responses and Serum Anti-HLA Antibodies in Kidney Transplant Recipients. Vaccines 2022, 10, 921. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Chen, L.-L.; Zhang, R.R.-Q.; Tsang, O.T.-Y.; Chan, J.M.-C.; Tam, A.R.; Leung, W.-S.; Chik, T.S.-H.; Lau, D.P.-L.; Choi, C.Y.-C.; et al. Boosting of serum neutralizing activity against the Omicron variant among recovered COVID-19 patients by BNT162b2 and CoronaVac vaccines. EBioMedicine 2022, 79, 103986. [Google Scholar] [CrossRef] [PubMed]
- Guerrera, G.; Picozza, M.; D’Orso, S.; Placido, R.; Pirronello, M.; Verdiani, A.; Termine, A.; Fabrizio, C.; Giannessi, F.; Sambucci, M.; et al. BNT162b2 vaccination induces durable SARS-CoV-2-specific T cells with a stem cell memory phenotype. Sci. Immunol. 2021, 6, eabl5344. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| All Participants (n: 300) | Female (n: 154) | Male (n: 146) | Female vs. Male | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | IQR25 | IQR75 | Median | IQR25 | IQR75 | Median | IQR25 | IQR75 | p | |
| Gender (F/M) n (%) | 154 (51.3%)/146 (48.7%) | |||||||||
| Age | 32.50 | 24.00 | 38.00 | 32 | 23.5 | 45 | 33 | 24.75 | 37 | 0.869 |
| NCP_IgG_0th (S/Co) | 0.65 | 0.25 | 4.05 | 2.59 | 0.38 | 4.27 | 0.29 | 0.14 | 4.22 | 0.062 |
| NCP_IgG_15th (S/Co) | 0.59 | 0.23 | 3.99 | 2.54 | 0.38 | 4.21 | 0.27 | 0.16 | 4.16 | 0.062 |
| NCP_IgG_60th (S/Co) | 0.28 | 0.15 | 2.12 | 0.67 | 0.18 | 2.57 | 0.25 | 0.14 | 1.87 | 0.42 |
| NCP_IgG_90th (S/Co) | 0.24 | 0.06 | 1.26 | 0.25 | 0.02 | 1.57 | 0.21 | 0.13 | 1.00 | 0.425 |
| anti-S-RBD IgG II_0th (AU/mL) | 5380.45 | 2332.43 | 12,442.50 | 4218.35 | 530.40 | 11,984.03 | 6095.85 | 3273.30 | 14,375.30 | 0.236 |
| anti-S-RBD IgG II_15th (AU/mL) | 31,946.60 | 19,739.50 | 50,076.30 | 32,816.60 | 27,749.20 | 53,666.40 | 24,530.00 | 16,340.90 | 37,576.43 | 0.18 |
| anti-S-RBD IgG II_60th (AU/mL) | 19,538.70 | 13,203.05 | 30,467.30 | 19,575.40 | 17,438.60 | 32,891.60 | 16,712.10 | 11,651.23 | 27,105.03 | 0.285 |
| anti-S-RBD IgG II_90th (AU/mL) | 12,546.50 | 6604.80 | 21,720.33 | 16,027.70 | 11,419.90 | 23,096.50 | 10,364.20 | 6604.80 | 18,825.73 | 0.08 |
| snAb 0th (IH%) | 74.15 | 66.80 | 81.25 | 75.25 | 67.53 | 81.25 | 73.95 | 66.20 | 81.50 | 0.985 |
| snAb 15th (IH%) | 93.70 | 91.35 | 97.83 | 93.20 | 91.13 | 96.78 | 94.40 | 91.28 | 98.43 | 0.426 |
| snAb 60th (IH%) | 90.80 | 84.58 | 92.78 | 90.25 | 84.40 | 93.73 | 91.10 | 85.68 | 92.48 | 0.62 |
| snAb 90th (IH%) | 83.85 | 78.03 | 89.40 | 83.15 | 77.10 | 89.58 | 84.15 | 78.50 | 88.28 | 0.869 |
| All Participants | without Prior SARS-CoV-2 Infection (n:208) | with Prior SARS-CoV-2 Infection (n:92) | p | ||||
|---|---|---|---|---|---|---|---|
| Median | IQR25 | IQR75 | Median | IQR25 | IQR75 | ||
| Gender (F/M) | 98/110 | 56/36 | 0.251 | ||||
| Age | 32.00 | 23.00 | 37.00 | 33.00 | 26.00 | 44.00 | 0.558 |
| NCP_IgG_0th (S/Co) | 0.25 | 0.14 | 0.38 | 4.59 | 2.81 | 6.69 | 0.000 |
| NCP_IgG_15th (S/Co) | 0.26 | 0.13 | 0.36 | 4.51 | 2.72 | 6.39 | 0.000 |
| NCP_IgG_60th (S/Co) | 0.18 | 0.12 | 0.25 | 2.16 | 1.01 | 4.23 | 0.000 |
| NCP_IgG_90th (S/Co) | 0.13 | 0.02 | 0.18 | 1.47 | 0.36 | 2.18 | 0.000 |
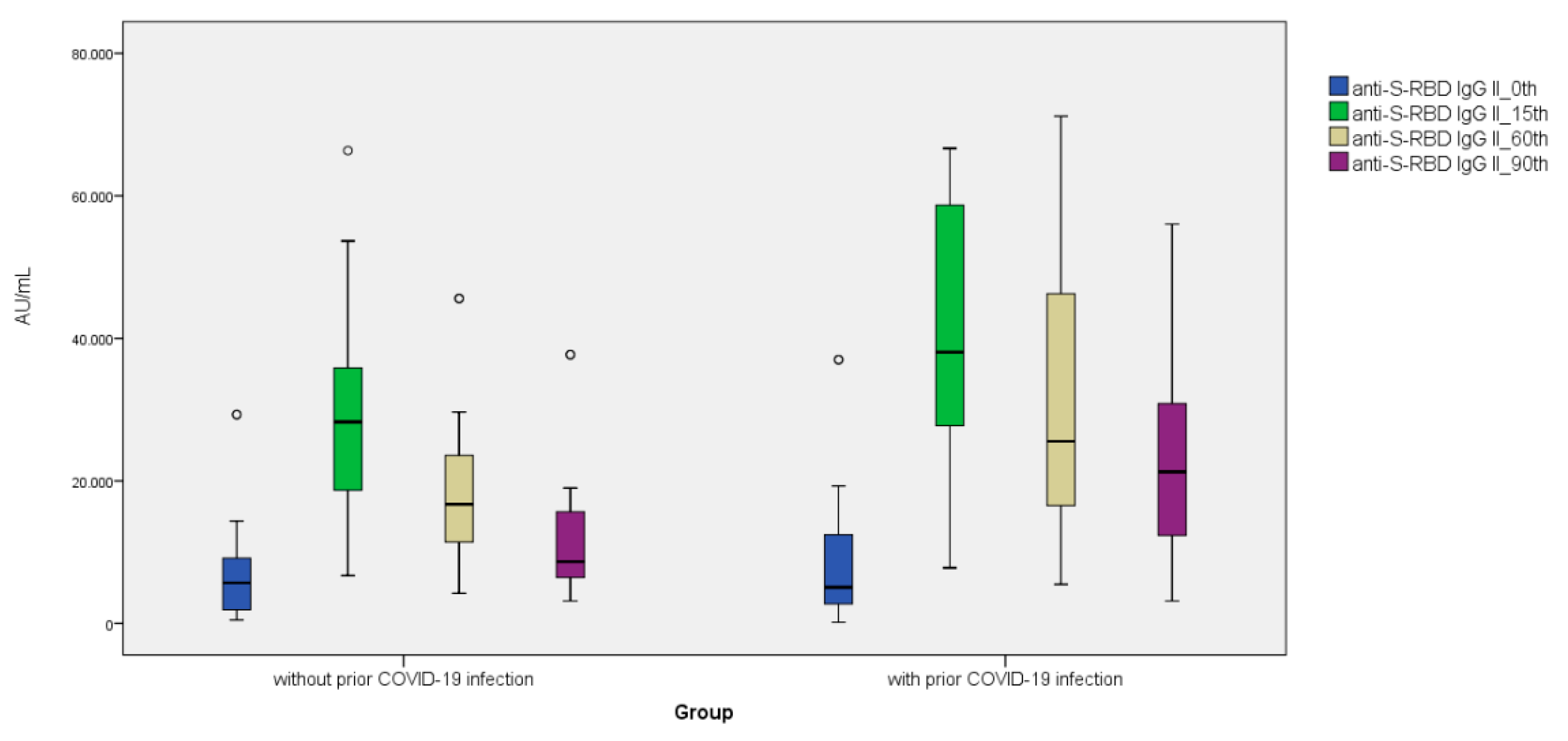
| anti-S-RBD IgG II_0th (AU/mL) | 5700.30 | 763.50 | 11,831.20 | 5060.60 | 2340.70 | 12,442.50 | 0.477 |
| anti-S-RBD IgG II_15th (AU/mL) | 28,281.10 | 16,621.30 | 36,075.00 | 38,076.90 | 27,749.20 | 61,720.00 | 0.052 |
| anti-S-RBD IgG II_60th (AU/mL) | 16,712.10 | 10,041.90 | 23,580.10 | 25,550.00 | 14,772.80 | 52,584.00 | 0.019 |
| anti-S-RBD IgG II_90th (AU/mL) | 8662.70 | 6262.30 | 16,027.70 | 21,261.60 | 12,162.50 | 34,034.50 | 0.001 |
| snAb 0th (IH%) | 71.50 | 61.80 | 76.50 | 76.50 | 73.80 | 84.30 | 0.003 |
| snAb 15th (IH%) | 92.40 | 90.30 | 97.20 | 94.80 | 92.80 | 99.10 | 0.076 |
| snAb 60th (IH%) | 90.40 | 83.50 | 91.70 | 90.90 | 86.70 | 94.50 | 0.113 |
| snAb 90th (IH%) | 80.60 | 76.50 | 85.40 | 85.40 | 79.80 | 90.10 | 0.047 |
| Female Participants | without Prior SARS-CoV-2 Infection (n:98) | with Prior SARS-CoV-2 Infection (n:56) | p | ||||
|---|---|---|---|---|---|---|---|
| Median | IQR25 | IQR75 | Median | IQR25 | IQR75 | ||
| Age | 32.00 | 24.00 | 37.00 | 36.00 | 22.00 | 45.00 | 0.570 |
| NCP_IgG_0th (S/Co) | 0.38 | 0.12 | 0.60 | 3.87 | 2.79 | 6.85 | 0.000 |
| NCP_IgG_15th (S/Co) | 0.38 | 0.12 | 0.55 | 3.81 | 2.72 | 6.79 | 0.000 |
| NCP_IgG_60th (S/Co) | 0.18 | 0.07 | 0.27 | 2.03 | 0.89 | 4.23 | 0.000 |
| NCP_IgG_90th (S/Co) | 0.02 | 0.02 | 0.13 | 1.19 | 0.25 | 2.38 | 0.000 |
| anti-S-RBD IgG II_0th (AU/mL) | 1792.10 | 504.45 | 9841.63 | 6511.20 | 2332.43 | 12,442.50 | 0.149 |
| anti-S-RBD IgG II_15th (AU/mL) | 32,040.80 | 20,282.23 | 49,154.83 | 34,154.40 | 27,749.20 | 61,720.00 | 0.470 |
| anti-S-RBD IgG II_60th (AU/mL) | 19,575.40 | 8739.48 | 29,659.20 | 22,526.00 | 17,438.60 | 37,814.70 | 0.570 |
| anti-S-RBD IgG II_90th (AU/mL) | 16,027.70 | 5757.43 | 18,995.20 | 17,044.20 | 11,419.90 | 25,831.00 | 0.606 |
| snAb 0th (IH%) | 72.35 | 60.90 | 78.98 | 76.50 | 71.45 | 82.13 | 0.080 |
| snAb 15th (IH%) | 92.35 | 89.85 | 96.50 | 94.05 | 91.70 | 97.75 | 0.382 |
| snAb 60th (IH%) | 85.45 | 83.43 | 93.00 | 90.60 | 86.60 | 94.13 | 0.142 |
| snAb 90th (IH%) | 80.15 | 76.58 | 88.13 | 85.00 | 79.43 | 90.10 | 0.150 |
| Male Participants | without Prior SARS-CoV-2 Infection (n:110) | with Prior SARS-CoV-2 Infection (n:36) | p | ||||
|---|---|---|---|---|---|---|---|
| Median | IQR25 | IQR75 | Median | IQR25 | IQR75 | ||
| Age | 34.00 | 23.00 | 37.00 | 33.00 | 30.00 | 35.00 | 0.881 |
| NCP_IgG_0th (S/Co) | 0.18 | 0.14 | 0.29 | 4.59 | 2.85 | 6.63 | 0.000 |
| NCP_IgG_15th (S/Co) | 0.16 | 0.13 | 0.27 | 4.51 | 2.82 | 6.39 | 0.000 |
| NCP_IgG_60th (S/Co) | 0.15 | 0.13 | 0.25 | 3.21 | 1.08 | 4.11 | 0.000 |
| NCP_IgG_90th (S/Co) | 0.15 | 0.12 | 0.24 | 1.88 | 0.41 | 2.45 | 0.001 |
| anti-S-RBD IgG II_0th (AU/mL) | 6491.40 | 4999.30 | 14,375.30 | 3184.20 | 2255.35 | 27,255.60 | 0.417 |
| anti-S-RBD IgG II_15th (AU/mL) | 20,778.90 | 16,340.90 | 36,075.00 | 55,588.00 | 11,585.45 | 60,615.50 | 0.111 |
| anti-S-RBD IgG II_60th (AU/mL) | 16,712.10 | 10,041.90 | 23,580.10 | 39,932.80 | 12,299.65 | 64,905.10 | 0.044 |
| anti-S-RBD IgG II_90th (AU/mL) | 6604.80 | 6262.30 | 12,065.70 | 27,637.90 | 12,546.50 | 55,502.10 | 0.001 |
| snAb 0th (IH%) | 70.90 | 63.50 | 76.50 | 76.80 | 74.20 | 88.50 | 0.016 |
| snAb 15th (IH%) | 93.10 | 91.10 | 97.30 | 98.60 | 93.15 | 99.40 | 0.052 |
| snAb 60th (IH%) | 91.10 | 85.40 | 91.70 | 92.10 | 85.95 | 95.70 | 0.297 |
| snAb 90th (IH%) | 83.60 | 74.90 | 85.40 | 85.60 | 80.45 | 90.70 | 0.121 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erdem, M.G.; Unlu, O.; Buber, S.; Demirci, M.; Kocazeybek, B.S. Could Prior COVID-19 Affect the Neutralizing Antibody after the Third BNT162b2 Booster Dose: A Longitudinal Study. Vaccines 2023, 11, 560. https://doi.org/10.3390/vaccines11030560
Erdem MG, Unlu O, Buber S, Demirci M, Kocazeybek BS. Could Prior COVID-19 Affect the Neutralizing Antibody after the Third BNT162b2 Booster Dose: A Longitudinal Study. Vaccines. 2023; 11(3):560. https://doi.org/10.3390/vaccines11030560
Chicago/Turabian StyleErdem, Mustafa Genco, Ozge Unlu, Suleyman Buber, Mehmet Demirci, and Bekir Sami Kocazeybek. 2023. "Could Prior COVID-19 Affect the Neutralizing Antibody after the Third BNT162b2 Booster Dose: A Longitudinal Study" Vaccines 11, no. 3: 560. https://doi.org/10.3390/vaccines11030560
APA StyleErdem, M. G., Unlu, O., Buber, S., Demirci, M., & Kocazeybek, B. S. (2023). Could Prior COVID-19 Affect the Neutralizing Antibody after the Third BNT162b2 Booster Dose: A Longitudinal Study. Vaccines, 11(3), 560. https://doi.org/10.3390/vaccines11030560