
Deepening Our Understanding of COVID-19 Vaccine Decision-Making amongst Healthcare Workers in Southwest Virginia, USA Using Exploratory and Confirmatory Factor Analysis

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample and Study Design
2.2. Statistical Methods
3. Results
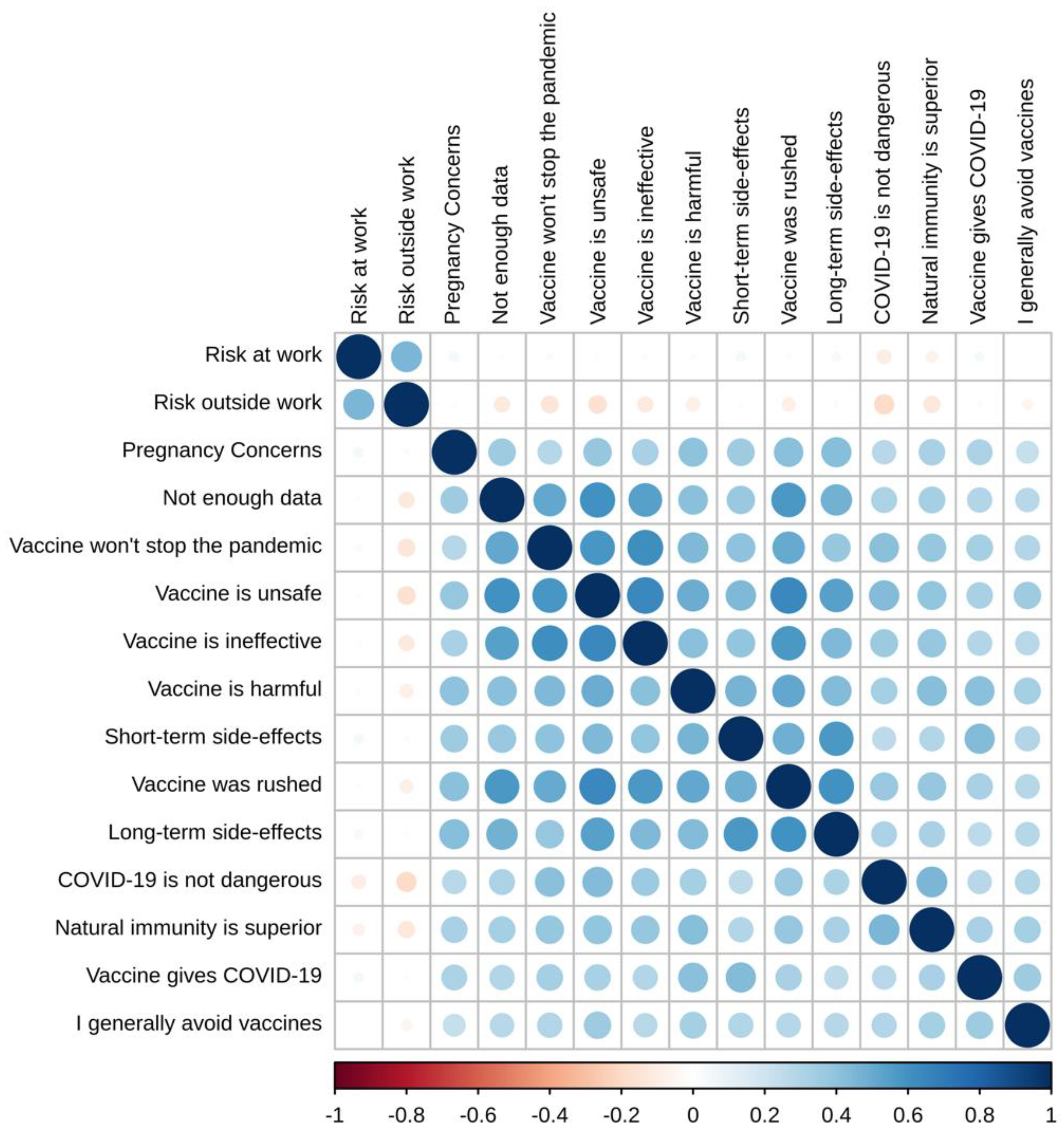
3.1. Descriptive Statistics
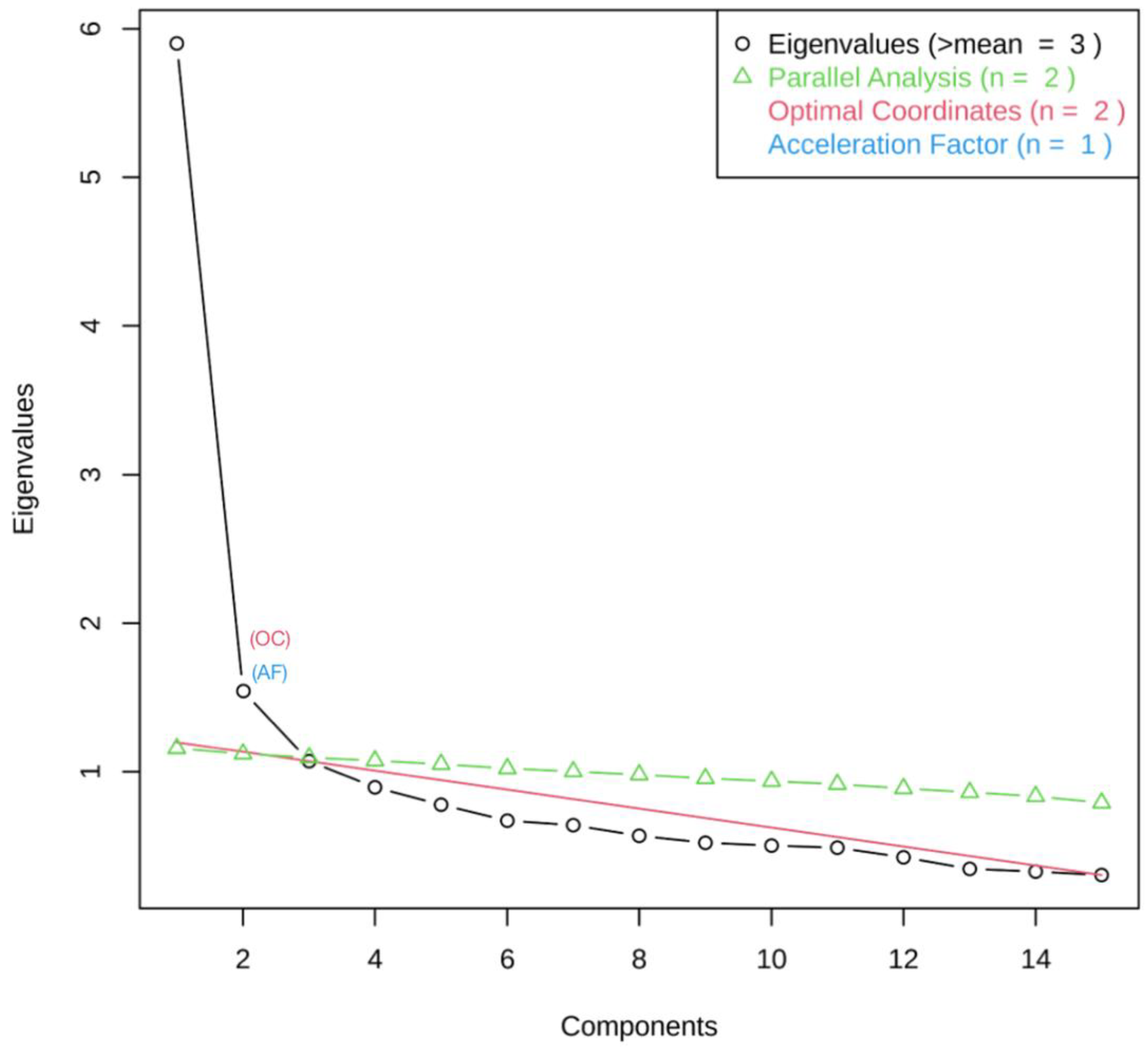
3.2. Exploratory Factor Analysis (EFA)
- Factor 1: Lack of trust in the COVID-19 vaccine
- Factor 2: Anti-science sentiment
- Factor 3: Adverse side-effects
- Factor 4: Situational risk assessment
3.3. Confirmatory Factor Analysis (CFA)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HCW | Healthcare Worker |
| EFA | Exploratory Factor Analysis |
| CFA | Confirmatory Factor Analysis |
| TLI | Tucker Lewis Index |
| CFI | Comparative Fit Index |
| RMSEA | Root Mean Square Error of Approximation |
Appendix A



{kind=link}
{kind=link}
{kind=link}
| Exploratory Factor Analysis | Confirmatory Factor Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 1 | Factor 2 | Factor 3 | Factor 4 | |
| Factor 1: Lack of trust in the COVID-19 vaccine | 1.000 | 0.767 *** | 0.724 *** | −0.211 *** | 1.000 | 0.882 *** | 0.835 *** | −0.142 ** |
| Factor 2: Anti-science sentiment | 0.767 *** | 1.000 | 0.660 *** | −0.143 *** | 0.882 *** | 1.000 | 0.843 *** | −0.163 ** |
| Factor 3: Adverse side-effects | 0.724 *** | 0.660 *** | 1.000 | 0.041 | 0.835 *** | 0.843 *** | 1.000 | 0.066 |
| Factor 4: Situational risk assessment | −0.211 *** | −0.143 *** | 0.041 | 1.000 | −0.142 ** | −0.163 ** | 0.066 | 1.000 |
References
- CDC. COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker/#datatracker-home (accessed on 21 January 2023).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Dunkle, L.M.; Kotloff, K.L.; Gay, C.L.; Áñez, G.; Adelglass, J.M.; Barrat Hernández, A.Q.; Harper, W.L.; Duncanson, D.M.; McArthur, M.A.; Florescu, D.F.; et al. Efficacy and Safety of NVX-CoV2373 in Adults in the United States and Mexico. N. Engl. J. Med. 2022, 386, 531–543. [Google Scholar] [CrossRef]
- Dubé, È.; Ward, J.K.; Verger, P.; MacDonald, N.E. Vaccine Hesitancy, Acceptance, and Anti-Vaccination: Trends and Future Prospects for Public Health. Annu. Rev. Public Health 2021, 42, 175–191. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef]
- Albrecht, D. Vaccination, politics and COVID-19 impacts. BMC Public Health 2022, 22, 96. [Google Scholar] [CrossRef]
- Leong, C.; Jin, L.; Kim, D.; Kim, J.; Teo, Y.Y.; Ho, T.H. Assessing the impact of novelty and conformity on hesitancy towards COVID-19 vaccines using mRNA technology. Commun. Med. 2022, 2, 61. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Danaee, M.; Ahmed, J.; Lachyan, A.; Cai, C.Z.; Lin, Y.; Hu, Z.; Tan, S.Y.; Lu, Y.; et al. COVID-19 vaccination intention and vaccine characteristics influencing vaccination acceptance: A global survey of 17 countries. Infect. Dis. Poverty 2021, 10, 122. [Google Scholar] [CrossRef]
- de Albuquerque Veloso Machado, M.; Roberts, B.; Wong, B.L.H.; van Kessel, R.; Mossialos, E. The Relationship Between the COVID-19 Pandemic and Vaccine Hesitancy: A Scoping Review of Literature Until August 2021. Front. Public Health 2021, 9, 747787. [Google Scholar] [CrossRef]
- Syan, S.K.; Gohari, M.R.; Levitt, E.E.; Belisario, K.; Gillard, J.; DeJesus, J.; MacKillop, J. COVID-19 Vaccine Perceptions and Differences by Sex, Age, and Education in 1,367 Community Adults in Ontario. Front. Public Health 2021, 9, 719665. [Google Scholar] [CrossRef]
- Gilboa, M.; Tal, I.; Levin, E.G.; Segal, S.; Belkin, A.; Zilberman-Daniels, T.; Biber, A.; Rubin, C.; Rahav, G.; Regev-Yochay, G. Coronavirus disease 2019 (COVID-19) vaccination uptake among healthcare workers. Infect. Control. Hosp. Epidemiol. 2022, 43, 1433–1438. [Google Scholar] [CrossRef]
- King, W.C.; Rubinstein, M.; Reinhart, A.; Mejia, R. Time trends, factors associated with, and reasons for COVID-19 vaccine hesitancy: A massive online survey of US adults from January–May 2021. PLoS ONE 2021, 16, e0260731. [Google Scholar] [CrossRef]
- Toth-Manikowski, S.M.; Swirsky, E.S.; Gandhi, R.; Piscitello, G. COVID-19 vaccination hesitancy among health care workers, communication, and policy-making. Am. J. Infect. Control. 2022, 50, 20–25. [Google Scholar] [CrossRef]
- Swann, M.C.; Bendetson, J.; Johnson, A.; Jatta, M.; Schleupner, C.J.; Baffoe-Bonnie, A. Examining drivers of coronavirus disease 2019 (COVID-19) vaccine hesitancy among healthcare workers. Infect. Control. Hosp. Epidemiol. 2022, 43, 1813–1821. [Google Scholar] [CrossRef]
- Caiazzo, V.; Witkoski Stimpfel, A. Vaccine hesitancy in American healthcare workers during the COVID-19 vaccine roll out: An integrative review. Public Health 2022, 207, 94–104. [Google Scholar] [CrossRef]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. Covid-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am. J. Infect. Control. 2021, 49, 1152–1157. [Google Scholar] [CrossRef]
- Elliott, T.R.; Perrin, P.B.; Powers, M.B.; Jacobi, K.S.; Warren, A.M. Predictors of Vaccine Hesitancy among Health Care Workers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 7123. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Intention of health care workers to accept COVID-19 vaccination and related factors: A systematic review and meta-analysis. Asian Pac. J. Trop. Med. 2021, 14, 543–554. [Google Scholar] [CrossRef]
- Huang, D.; Ganti, L.; Graham, E.W.; Shah, D.; Aleksandrovskiy, I.; Al-Bassam, M.; Fraunfelter, F.; Falgiani, M.; Leon, L.; Lopez-Ortiz, C. COVID-19 Vaccine Hesitancy Among Healthcare Providers. Health Psychol. Res. 2022, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Kandiah, S.; Iheaku, O.; Farrque, M.; Hanna, J.; Johnson, K.B.; Wiley, Z.; Franks, N.M.; Carroll, K.; Shin, S.R.; Sims, K.M.; et al. COVID-19 Vaccine Hesitancy Among Health Care Workers in Four Health Care Systems in Atlanta. Open Forum Infect. Dis. 2022, 9, ofac224. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.; Hanley, S.; Stewart, T.; Salmon, D.A.; Ortiz, C.; Trief, P.M.; Asiago Reddy, E.; Morley, C.P.; Thomas, S.J.; Anderson, K.B. Healthcare Personnel (HCP) Attitudes About Coronavirus Disease 2019 (COVID-19) Vaccination after Emergency Use Authorization. Clin. Infect. Dis. 2022, 75, e814–e821. [Google Scholar] [CrossRef]
- Browne, S.K.; Feemster, K.A.; Shen, A.K.; Green-McKenzie, J.; Momplaisir, F.M.; Faig, W.; Offit, P.A.; Kuter, B.J. Coronavirus disease 2019 (COVID-19) vaccine hesitancy among physicians, physician assistants, nurse practitioners, and nurses in two academic hospitals in Philadelphia. Infect. Control. Hosp. Epidemiol. 2022, 43, 1424–1432. [Google Scholar] [CrossRef]
- Peterson, C.J.; Lee, B.; Nugent, K. COVID-19 Vaccination Hesitancy among Healthcare Workers—A Review. Vaccines 2022, 10, 948. [Google Scholar] [CrossRef]
- Gadoth, A.; Halbrook, M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, A.W. Cross-sectional Assessment of COVID-19 Vaccine Acceptance Among Health Care Workers in Los Angeles. Ann. Intern. Med. 2021, 174, 882–885. [Google Scholar] [CrossRef]
- Díaz Luévano, C.; Sicsic, J.; Pellissier, G.; Chyderiotis, S.; Arwidson, P.; Olivier, C.; Gagneux-Brunon, A.; Botelho-Nevers, E.; Bouvet, E.; Mueller, J. Quantifying healthcare and welfare sector workers’ preferences around COVID-19 vaccination: A cross-sectional, single-profile discrete-choice experiment in France. BMJ Open 2021, 11, e055148. [Google Scholar] [CrossRef]
- Koh, S.W.C.; Liow, Y.; Loh, V.W.K.; Liew, S.J.; Chan, Y.H.; Young, D. COVID-19 vaccine acceptance and hesitancy among primary healthcare workers in Singapore. BMC Prim. Care 2022, 23, 81. [Google Scholar] [CrossRef]
- Paris, C.; Bénézit, F.; Geslin, M.; Polard, E.; Baldeyrou, M.; Turmel, V.; Tadié, É.; Garlantezec, R.; Tattevin, P. COVID-19 vaccine hesitancy among healthcare workers. Infect. Dis. Now 2021, 51, 484–487. [Google Scholar] [CrossRef]
- Thompson, B. Exploratory and Confirmatory Factor Analysis: Understanding Concepts and Applications; American Psychological Association: Washington, DC, USA, 2004. [Google Scholar] [CrossRef]
- Xiang, B.; Wong, H.M.; Cao, W.; Perfecto, A.P.; McGrath, C.P.J. Development and validation of the Oral health behavior questionnaire for adolescents based on the health belief model (OHBQAHBM). BMC Public Health 2020, 20, 701. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, X.; Wang, X.; Naqvi, A.A.; Zhang, Q.; Zang, X. Translation and validation of the Chinese version of the general medication adherence scale (GMAS) in patients with chronic illness. Curr. Med. Res. Opin. 2021, 37, 829–837. [Google Scholar] [CrossRef]
- Rhea, K.C.; Cater, M.W.; McCarter, K.; Tuuri, G. Psychometric Analyses of the Eating and Food Literacy Behaviors Questionnaire with University Students. J. Nutr. Educ. Behav. 2020, 52, 1008–1017. [Google Scholar] [CrossRef]
- Yu, X.; Xu, C.; Ni, Y.; Chang, R.; Wang, H.; Gong, R.; Wang, Y.; Wang, S.; Cai, Y. Pre-Exposure Prophylaxis (PrEP) Adherence Questionnaire: Psychometric Validation among Sexually Transmitted Infection Patients in China. Int. J. Environ. Res. Public Health 2021, 18, 10980. [Google Scholar] [CrossRef]
- Brown, C.L.; Perrin, E.M. Defining picky eating and its relationship to feeding behaviors and weight status. J. Behav. Med. 2020, 43, 587–595. [Google Scholar] [CrossRef]
- FDA. Coronavirus (COVID-19) Update: FDA Authorizes Moderna, Pfizer-BioNTech Bivalent COVID-19 Vaccines for Use as a Booster Dose. 2022. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-moderna-pfizer-biontech-bivalent-covid-19-vaccines-use (accessed on 21 January 2023).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Schumacker, R.E.; Lomax, R.G. A Beginner’s Guide to Structural Equation Modeling, 3rd ed.; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- R: A Language and Environment for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 9 March 2022).
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 2. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Al-Sanafi, M.; Sallam, M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines 2021, 9, 701. [Google Scholar] [CrossRef]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of Vaccination Readiness. Eur. J. Psychol. Assess. 2022, 38, 261–269. [Google Scholar] [CrossRef]
- Link-Gelles, R.; Levy, M.E.; Gaglani, M.; Irving, S.A.; Stockwell, M.; Dascomb, K.; DeSilva, M.B.; Reese, S.E.; Liao, I.C.; Ong, T.C.; et al. Effectiveness of 2, 3, and 4 COVID-19 mRNA Vaccine Doses Among Immunocompetent Adults During Periods when SARS-CoV-2 Omicron BA.1 and BA.2/BA.2.12.1 Sublineages Predominated—VISION Network, 10 States, December 2021–June 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Razzaghi, H.; Srivastav, A.; de Perio, M.A.; Laney, A.S.; Black, C.L. Influenza and COVID-19 Vaccination Coverage Among Health Care Personnel—United States, 2021–22. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Centers for Medicare & Medicaid Services Data. Available online: https://data.cms.gov/covid-19/covid-19-nursing-home-data (accessed on 21 January 2023).
- Chou, W.Y.S.; Budenz, A. Considering Emotion in COVID-19 Vaccine Communication: Addressing Vaccine Hesitancy and Fostering Vaccine Confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef]
- Kaim, A.; Siman-Tov, M.; Jaffe, E.; Adini, B. Effect of a Concise Educational Program on COVID-19 Vaccination Attitudes. Front. Public Health 2021, 9, 767447. [Google Scholar] [CrossRef]
- Li, P.C.; Theis, S.R.; Kelly, D.; Ocampo, T.; Berglund, A.; Morgan, D.; Markert, R.; Fisher, E.; Burtson, K. Impact of an Education Intervention on COVID-19 Vaccine Hesitancy in a Military Base Population. Mil. Med. 2022, 187, e1516–e1522. [Google Scholar] [CrossRef]
- Evans, C.T.; DeYoung, B.J.; Gray, E.L.; Wallia, A.; Ho, J.; Carnethon, M.; Zembower, T.R.; Hirschhorn, L.R.; Wilkins, J.T. Coronavirus disease 2019 (COVID-19) vaccine intentions and uptake in a tertiary-care healthcare system: A longitudinal study. Infect. Control. Hosp. Epidemiol. 2021, 43, 1806–1812. [Google Scholar] [CrossRef]
- Hornsey, M.J.; Fielding, K.S. Attitude roots and Jiu Jitsu persuasion: Understanding and overcoming the motivated rejection of science. Am. Psychol. 2017, 72, 459–473. [Google Scholar] [CrossRef]

| Characteristic | n (%) |
| Sex | |
| Female | 2019 (82.1%) |
| Male | 423 (17.2%) |
| Non-Binary | 5 (0.2%) |
| Prefer Not to Say | 12 (0.5%) |
| Age Group | |
| 18–24 | 114 (4.6%) |
| 25–34 | 560 (22.8%) |
| 35–44 | 545 (22.2%) |
| 45–54 | 613 (24.9%) |
| 55–64 | 545 (22.2%) |
| 65+ | 82 (3.3%) |
| Race/Ethnicity | |
| Asian | 41 (1.7%) |
| Black/ African American | 127 (5.2%) |
| Hispanic/Latino(a) | 39 (1.6%) |
| Native American or Alaska Native | 16 (0.7%) |
| Native Hawaiian or Other Pacific Islander | 1 (0.04%) |
| White/Caucasian | 2181 (88.7%) |
| Two or More Races | 32 (1.3%) |
| Unknown | 22 (0.9%) |
| Role at Carilion * | |
| Nursing | 827 (33.6%) |
| Provider | 194 (7.9%) |
| Management | 280 (11.4%) |
| Other Responsibilities (Patient Care) | 605 (24.6%) |
| Other Responsibilities (Non-Patient Care) | 553 (22.5%) |
| Work Setting | |
| Outpatient | 767 (31.2%) |
| Inpatient | 696 (28.3%) |
| Both | 464 (18.9%) |
| Other | 490 (19.9%) |
| Unsure | 42 (1.7%) |
| Hesitancy Status | |
| Vaccine Hesitant | 446 (18.1%) |
| Vaccine Acceptant | 2013 (81.9%) |
| Survey Item | |
| Vaccine is ineffective | |
| Mean (SD) | 2.20 (±1.02) |
| Median [Min, Max] | 2 [1, 5] |
| Vaccine is unsafe | |
| Mean (SD) | 2.19 (±1.15) |
| Median [Min, Max] | 2 [1, 5] |
| Vaccine won’t stop the pandemic | |
| Mean (SD) | 2.07 (±1.07) |
| Median [Min, Max] | 2 [1, 5] |
| Vaccine was rushed | |
| Mean (SD) | 2.48 (±1.25) |
| Median [Min, Max] | 2 [1, 5] |
| Vaccine gives COVID-19 | |
| Mean (SD) | 1.32 (±0.74) |
| Median [Min, Max] | 1 [1, 5] |
| Natural immunity is superior | |
| Mean (SD) | 2.30 (±1.11) |
| Median [Min, Max] | 2 [1, 5] |
| I generally avoid vaccines | |
| Mean (SD) | 1.62 (±1.06) |
| Median [Min, Max] | 1 [1, 5] |
| Vaccine is harmful | |
| Mean (SD) | 2.00 (±1.10) |
| Median [Min, Max] | 2 [1, 5] |
| COVID-19 is not dangerous | |
| Mean (SD) | 1.45 (±0.86) |
| Median [Min, Max] | 1 [1, 5] |
| Long-term side-effects | |
| Mean (SD) | 3.09 (±1.31) |
| Median [Min, Max] | 3 [1, 5] |
| Short-term side-effects | |
| Mean (SD) | 2.23 (±1.21) |
| Median [Min, Max] | 2 [1, 5] |
| Pregnancy concerns | |
| Mean (SD) | 1.98 (±1.18) |
| Median [Min, Max] | 1 [1, 5] |
| Risk at work | |
| Mean (SD) | 3.00 (±1.29) |
| Median [Min, Max] | 3 [1, 5] |
| Risk outside work | |
| Mean (SD) | 2.96 (±1.13) |
| Median [Min, Max] | 3 [1, 5] |
| Survey Item | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|
| Vaccine is ineffective | 0.827 | – | – | – |
| Vaccine is unsafe | 0.717 | – | – | – |
| Vaccine won’t stop the pandemic | 0.709 | – | – | – |
| Not enough data | 0.615 | – | – | – |
| Vaccine was rushed | 0.492 | – | 0.387 | – |
| Vaccine gives COVID-19 | – | 0.633 | – | – |
| Natural immunity is superior | – | 0.503 | – | – |
| I generally avoid vaccines | – | 0.499 | – | – |
| Vaccine is harmful | – | 0.457 | – | – |
| COVID-19 is not dangerous | – | 0.373 | – | – |
| Long-term side-effects | – | – | 0.694 | – |
| Short-term side-effects | – | 0.339 | 0.491 | – |
| Pregnancy concerns | – | – | – | – |
| Risk at work | – | – | – | 0.686 |
| Risk outside work | – | – | – | 0.677 |
| Proportion of Variance Explained | 0.407 | 0.259 | 0.202 | 0.133 |
| Number of Survey Items | 5 | 5 | 3 | 2 |
| Cronbach’s Alpha | 0.880 | 0.733 | 0.701 | 0.637 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bendetson, J.; Swann, M.C.; Lozano, A.; West, J.; Hanlon, A.L.; Crandell, I.; Jatta, M.; Schleupner, C.J.; Baffoe-Bonnie, A. Deepening Our Understanding of COVID-19 Vaccine Decision-Making amongst Healthcare Workers in Southwest Virginia, USA Using Exploratory and Confirmatory Factor Analysis. Vaccines 2023, 11, 556. https://doi.org/10.3390/vaccines11030556
Bendetson J, Swann MC, Lozano A, West J, Hanlon AL, Crandell I, Jatta M, Schleupner CJ, Baffoe-Bonnie A. Deepening Our Understanding of COVID-19 Vaccine Decision-Making amongst Healthcare Workers in Southwest Virginia, USA Using Exploratory and Confirmatory Factor Analysis. Vaccines. 2023; 11(3):556. https://doi.org/10.3390/vaccines11030556
Chicago/Turabian StyleBendetson, Jesse, Mandy C. Swann, Alicia Lozano, Jennifer West, Alexandra L. Hanlon, Ian Crandell, Maimuna Jatta, Charles J. Schleupner, and Anthony Baffoe-Bonnie. 2023. "Deepening Our Understanding of COVID-19 Vaccine Decision-Making amongst Healthcare Workers in Southwest Virginia, USA Using Exploratory and Confirmatory Factor Analysis" Vaccines 11, no. 3: 556. https://doi.org/10.3390/vaccines11030556
APA StyleBendetson, J., Swann, M. C., Lozano, A., West, J., Hanlon, A. L., Crandell, I., Jatta, M., Schleupner, C. J., & Baffoe-Bonnie, A. (2023). Deepening Our Understanding of COVID-19 Vaccine Decision-Making amongst Healthcare Workers in Southwest Virginia, USA Using Exploratory and Confirmatory Factor Analysis. Vaccines, 11(3), 556. https://doi.org/10.3390/vaccines11030556