

Worldwide Estimation of Parental Acceptance of COVID-19 Vaccine for Their Children: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
Study Aims
- Assessment of heterogeneity and its possible sources for estimated pooled prevalence of parental acceptance/willingness to vaccinate their children with the COVID-19 vaccine;
- Moderator analyses to determine influential variables sources for estimated pooled prevalence of parental acceptance/willingness to vaccinate their children with the COVID-19 vaccine;
- Determining influential factors for parents to accept COVID-19 vaccination for their children.
2. Materials and Methods
2.1. Protocol and Registration
2.2. Systematic Review Questions
2.3. Eligibility Criteria
2.4. Information Sources
2.5. Search Strategy
2.6. Study Selection
2.7. Data Collection Process and Data Items
2.8. Risk of Bias in Individual Studies
2.9. Summary Measures and Data Synthesis
2.10. Risk of Bias across Studies
2.11. Additional Analyses
3. Results
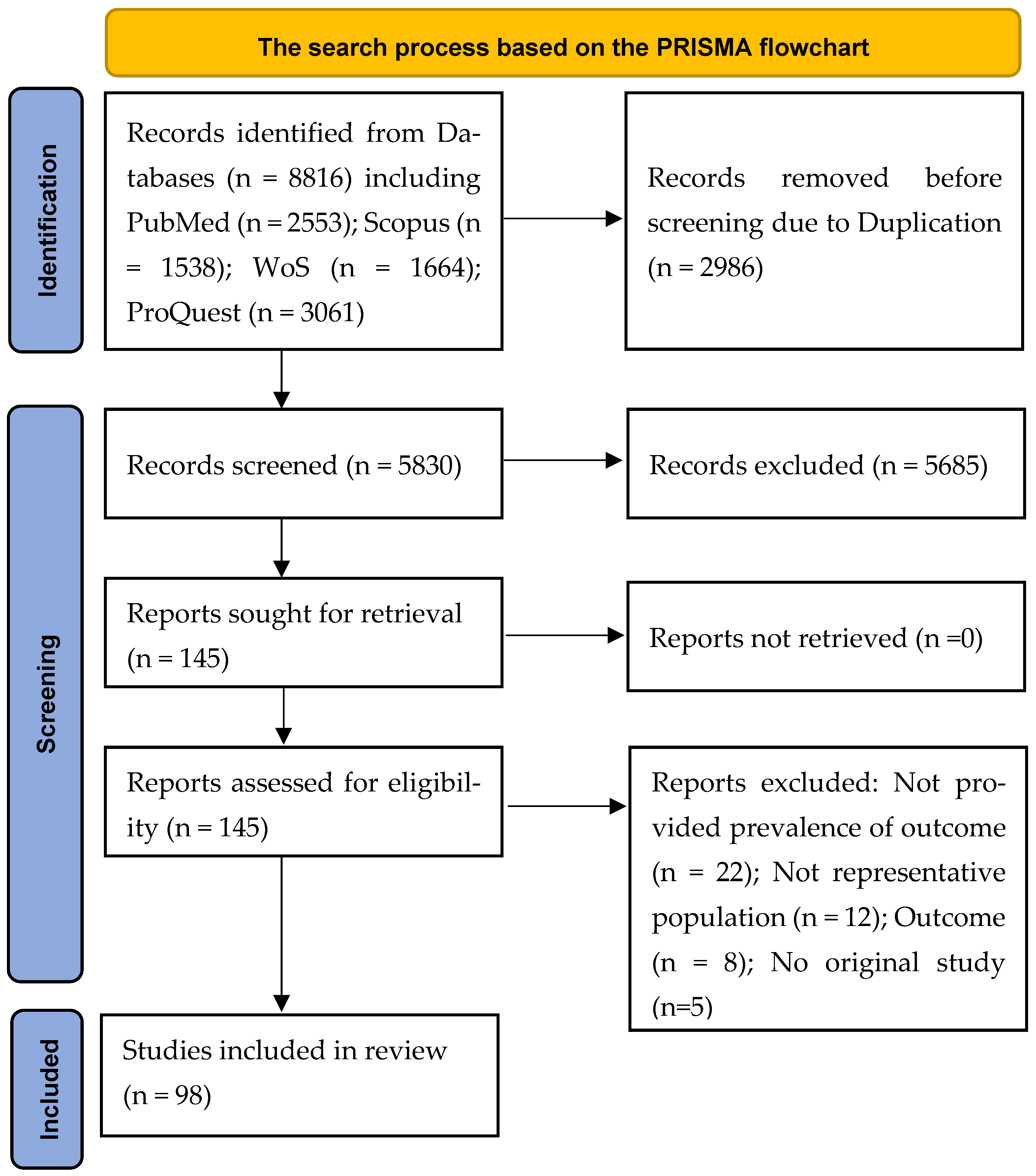
3.1. Study Screening and Selection Process
3.2. Description of the Included Studies
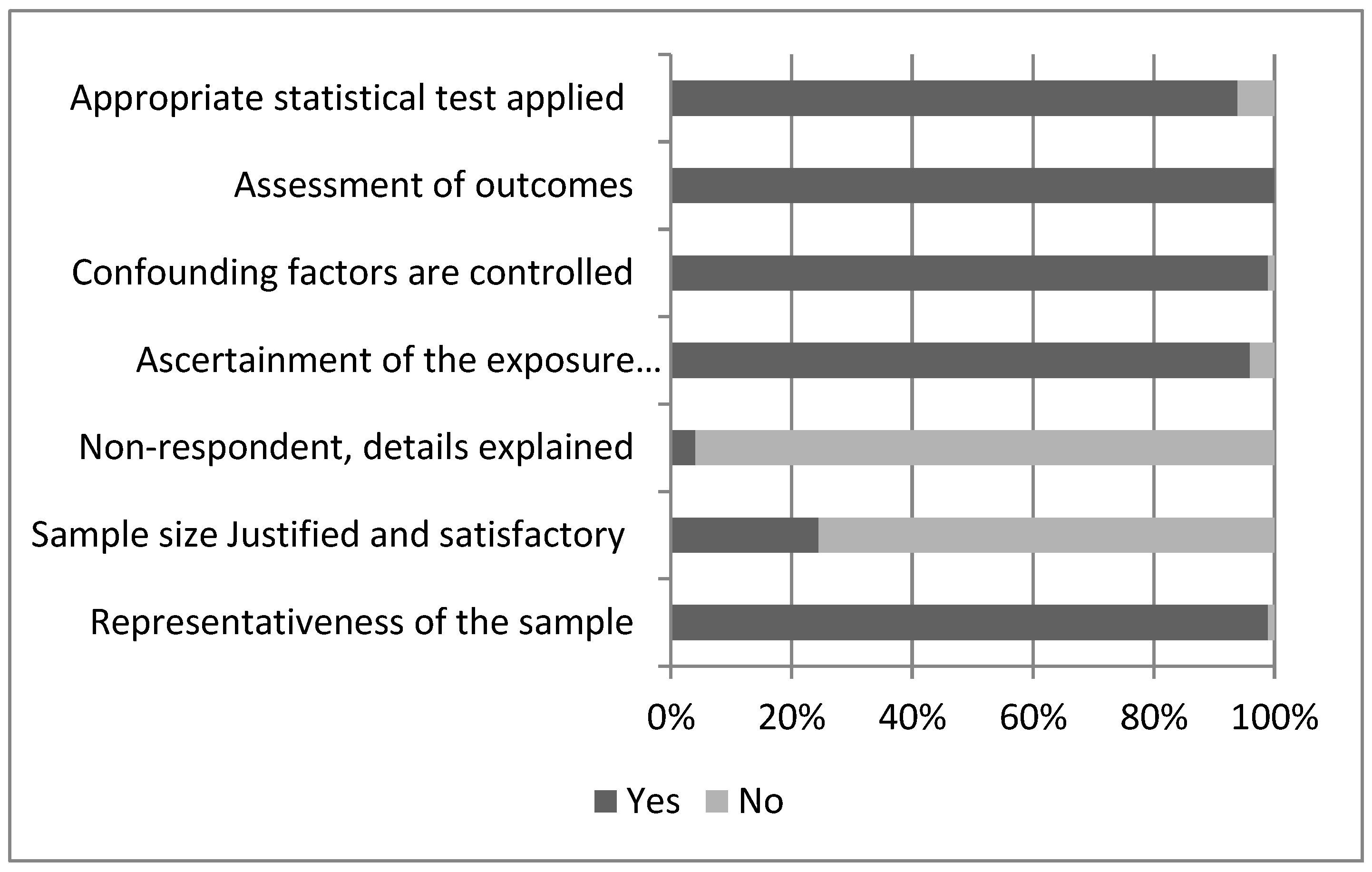
3.3. Methodological Quality Appraisal
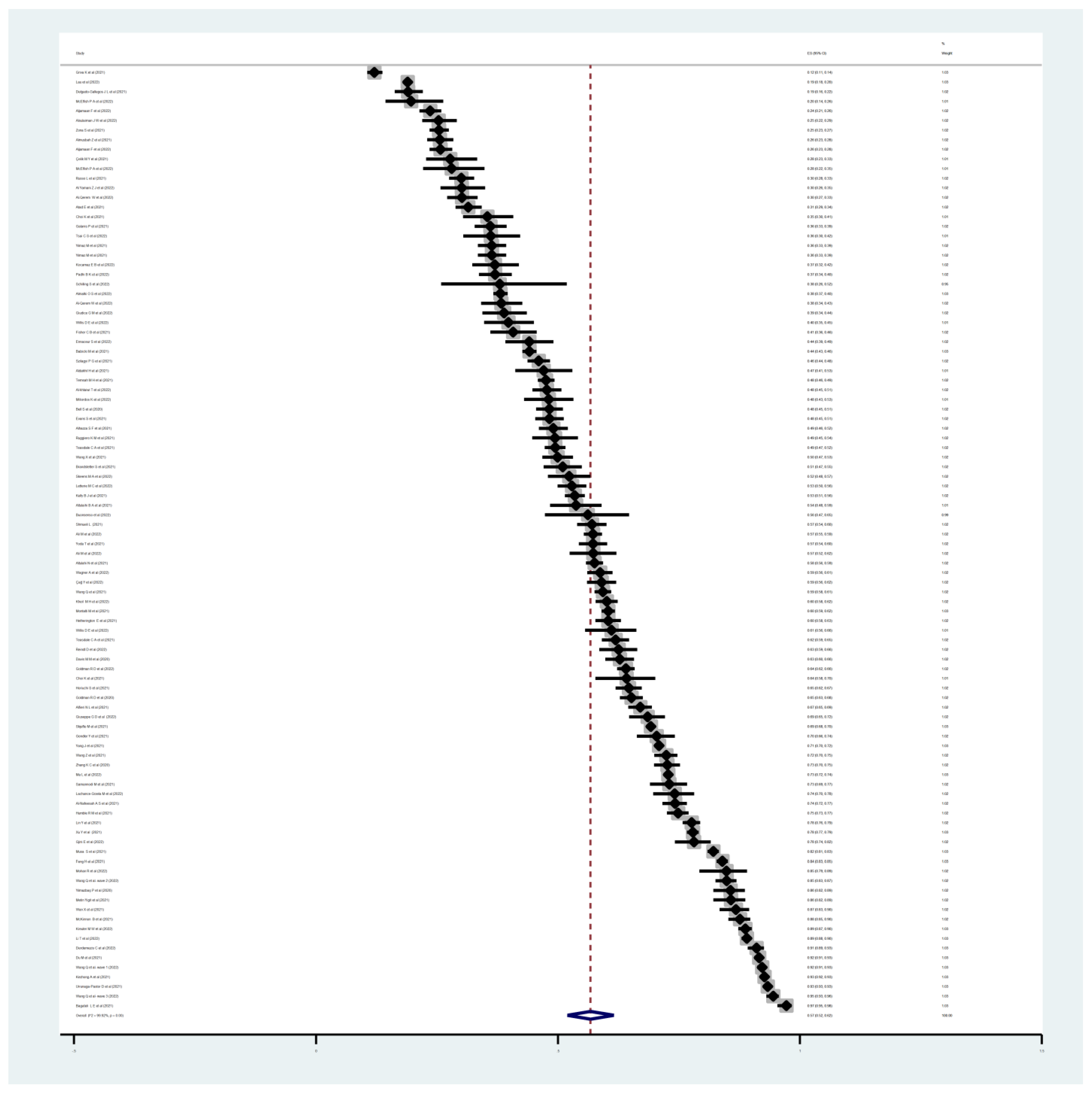
3.4. Pooled Prevalence of COVID-19 Vaccine Willingness
3.5. Predictor Variables of Parental Willingness
3.6. Contributing Factors of Parental Willingness
3.6.1. Family Related Contributing Factors
3.6.2. Vaccine Related Factors
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, E.; Arledge, S. Individual characteristics and demographics associated with mask wearing during the COVID-19 pandemic in the United States. Asian J. Soc. Health Behav. 2022, 5, 3–9. [Google Scholar] [CrossRef]
- Prasiska, D.; Muhlis, A.; Megatsari, H. Effectiveness of the emergency public activity restrictions on COVID-19 epidemiological parameter in East Java Province, Indonesia: An ecological study. Asian J. Soc. Health Behav. 2022, 5, 33–39. [Google Scholar] [CrossRef]
- Sandya, P.; Shetty, K.; Jaise, J.; Manikappa, S.; Pai, N. Stress and burden among caregivers of persons with bipolar affective disorder during the COVID-19 pandemic in India. Asian J. Soc. Health Behav. 2022, 5, 51–56. [Google Scholar] [CrossRef]
- Sangma, R.; Kumar, P.; Nerli, L.; Khanna, A.; Vasavada, D.; Tiwari, D. Social stigma and discrimination in Coronavirus Disease-2019 survivors and its changing trend: A longitudinal study at tertiary care center Gujarat, India. Asian J. Soc. Health Behav. 2022, 5, 68–74. [Google Scholar] [CrossRef]
- Soltani, R.; Shamsi, M.; Moradi, A. Do perceived barriers, benefits, and severity have effect on mask-wearing habits during the coronavirus disease-2019 pandemic? Asian J. Soc. Health Behav. 2022, 5, 186–192. [Google Scholar] [CrossRef]
- Vicerra, P.; Pano, J.; Estanislao, J. Nutrition status of lower-income older adults in Thailand during COVID-19 pandemic. Asian J. Soc. Health Behav. 2022, 5, 147–153. [Google Scholar] [CrossRef]
- WHO. WHO COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 31 January 2023).
- Bonaccorsi, G.; Pierri, F.; Cinelli, M.; Flori, A.; Galeazzi, A.; Porcelli, F.; Schmidt, A.L.; Valensise, C.M.; Scala, A.; Quattrociocchi, W. Economic and social consequences of human mobility restrictions under COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 15530–15535. [Google Scholar] [CrossRef]
- Yee, A.; Hodori, N.A.M.; Tung, Y.-Z.; Ooi, P.-L.; Latif, S.A.B.A.; Isa, H.M.; Ng, D.-L.-C.; Chai, C.-S.; Tan, S.-B. Depression level and coping responses toward the movement control order and its impact on quality of life in the Malaysian community during the COVID-19 pandemic: A web-based cross-sectional study. Ann. Gen. Psychiatry 2021, 20, 31. [Google Scholar] [CrossRef]
- WHO. Pandemic Fatigue: Reinvigorating the Public to Prevent COVID-19: Policy Considerations for Member States in the WHO European Region. Available online: https://apps.who.int/iris/handle/10665/335820. (accessed on 24 January 2023).
- Auger, K.A.; Shah, S.S.; Richardson, T.; Hartley, D.; Hall, M.; Warniment, A.; Timmons, K.; Bosse, D.; Ferris, S.A.; Brady, P.W. Association between statewide school closure and COVID-19 incidence and mortality in the US. JAMA 2020, 324, 859–870. [Google Scholar] [CrossRef]
- Liu, J.J.; Bao, Y.; Huang, X.; Shi, J.; Lu, L. Mental health considerations for children quarantined because of COVID-19. Lancet Child Adolesc. Health 2020, 4, 347–349. [Google Scholar] [CrossRef]
- Hajj Hussein, I.; Chams, N.; Chams, S.; El Sayegh, S.; Badran, R.; Raad, M.; Gerges-Geagea, A.; Leone, A.; Jurjus, A. Vaccines through centuries: Major cornerstones of global health. Front. Public Health 2015, 3, 269. [Google Scholar] [CrossRef]
- Rodrigues, C.M.; Plotkin, S.A. Impact of vaccines; health, economic and social perspectives. Front. Microbiol. 2020, 11, 1526. [Google Scholar] [CrossRef]
- Andre, F.E.; Booy, R.; Bock, H.L.; Clemens, J.; Datta, S.K.; John, T.J.; Lee, B.W.; Lolekha, S.; Peltola, H.; Ruff, T. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef]
- Opel, D.J.; Diekema, D.S.; Ross, L.F. Should we mandate a COVID-19 vaccine for children? JAMA Pediatr. 2021, 175, 125–126. [Google Scholar] [CrossRef]
- Kotecha, I.; Vasavada, D.; Kumar, P.; Nerli, L.; Tiwari, D.; Parmar, D. Knowledge, attitude, and belief of health-care workers toward COVID-19 Vaccine at a tertiary care center in India. Asian J. Soc. Health Behav. 2022, 5, 63–67. [Google Scholar] [CrossRef]
- Nascimento, M.; Nunes, A.; Juchem, L. “I believe in science and in all vaccines:” Older adult and the intention for a vaccine against COVID-19. Asian J. Soc. Health Behav. 2022, 5, 108–114. [Google Scholar] [CrossRef]
- Rieger, M. Willingness to vaccinate against COVID-19 might be systematically underestimated. Asian J. Soc. Health Behav. 2021, 4, 81–83. [Google Scholar] [CrossRef]
- Araf, Y.; Akter, F.; Tang, Y.d.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef]
- Schoch-Spana, M.; Brunson, E.K.; Long, R.; Ruth, A.; Ravi, S.J.; Trotochaud, M.; Borio, L.; Brewer, J.; Buccina, J.; Connell, N. The public’s role in COVID-19 vaccination: Human-centered recommendations to enhance pandemic vaccine awareness, access, and acceptance in the United States. Vaccine 2021, 39, 6004–6012. [Google Scholar] [CrossRef]
- Bronstein, M.V.; Kummerfeld, E.; MacDonald III, A.; Vinogradov, S. Willingness to vaccinate against SARS-CoV-2: The role of reasoning biases and conspiracist ideation. Vaccine 2022, 40, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Geoghegan, S.; O’Callaghan, K.P.; Offit, P.A. Vaccine safety: Myths and misinformation. Front. Microbiol. 2020, 11, 372. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Chen, A.; Cui, B.; Liao, W. Exploring public perceptions of the COVID-19 vaccine online from a cultural perspective: Semantic network analysis of two social media platforms in the United States and China. Telemat. Inform. 2021, 65, 101712. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Shakeel, C.S.; Mujeeb, A.A.; Mirza, M.S.; Chaudhry, B.; Khan, S.J. Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors. Vaccines 2022, 10, 110. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip. Healthc. 2022, 15, 21–45. [Google Scholar] [CrossRef] [PubMed]
- Yasmin, F.; Najeeb, H.; Moeed, A.; Naeem, U.; Asghar, M.S.; Chughtai, N.U.; Yousaf, Z.; Seboka, B.T.; Ullah, I.; Lin, C.-Y. COVID-19 vaccine hesitancy in the United States: A systematic review. Front. Public Health 2021, 9, 770985. [Google Scholar] [CrossRef]
- Altenbuchner, A.; Haug, S.; Schnell, R.; Scharf, A.; Weber, K. Impfbereitschaft von Eltern mit einem COVID-19-Vakzin. Pädiatrie Pädologie 2021, 56, 230–234. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or not? The association of age, gender, and education with potential acceptance of a COVID-19 vaccine: A country-level analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef]
- Schernhammer, E.; Weitzer, J.; Laubichler, M.D.; Birmann, B.M.; Bertau, M.; Zenk, L.; Caniglia, G.; Jäger, C.C.; Steiner, G. Correlates of COVID-19 vaccine hesitancy in Austria: Trust and the government. J. Public Health 2022, 44, e106–e116. [Google Scholar] [CrossRef] [PubMed]
- Umakanthan, S.; Lawrence, S. Predictors of COVID-19 vaccine hesitancy in Germany: A cross-sectional, population-based study. Postgrad. Med. J. 2022, 98, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Morgan, L.; Schwartz, J.L.; Sisti, D.A. COVID-19 vaccination of minors without parental consent: Respecting emerging autonomy and advancing public health. JAMA Pediatr. 2021, 175, 995–996. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Willingness, refusal and influential factors of parents to vaccinate their children against the COVID-19: A systematic review and meta-analysis. Prev. Med. 2022, 157, 106994. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; He, Y.; Shi, Y. Parents’ and guardians’ willingness to vaccinate their children against COVID-19: A systematic review and meta-analysis. Vaccines 2022, 10, 179. [Google Scholar] [CrossRef]
- Bagateli, L.E.; Saeki, E.Y.; Fadda, M.; Agostoni, C.; Marchisio, P.; Milani, G.P. COVID-19 vaccine hesitancy among parents of children and adolescents living in Brazil. Vaccines 2021, 9, 1115. [Google Scholar] [CrossRef]
- Marquez, R.R.; Gosnell, E.S.; Thikkurissy, S.; Schwartz, S.B.; Cully, J.L. Caregiver acceptance of an anticipated COVID-19 vaccination. J. Am. Dent. Assoc. 2021, 152, 730–739. [Google Scholar] [CrossRef]
- Ali, K.; Berman, G.; Zhou, H.; Deng, W.; Faughnan, V.; Coronado-Voges, M.; Ding, B.; Dooley, J.; Girard, B.; Hillebrand, W. Evaluation of mRNA-1273 SARS-CoV-2 vaccine in adolescents. N. Engl. J. Med. 2021, 385, 2241–2251. [Google Scholar] [CrossRef]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A. Evaluation of the BNT162b2 COVID-19 vaccine in children 5 to 11 years of age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef]
- Alimoradi, Z.; Pakpour, A. Challenges to Parents in COVID-19 Vaccination for Children. PROSPERO 2022 CRD42022333342. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=333342 (accessed on 5 January 2023).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta-Anal. 2017, 5, 80–84. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp (accessed on 22 August 2022).
- Hox, J.J.; Leeuw, E.D.d. Multilevel models for meta-analysis. In Multilevel Modeling: Methodological Advances, Issues, and Applications; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2003; pp. 90–111. [Google Scholar]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Rothstein, H.R.; Sutton, A.J.; Borenstein, M. Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2005; pp. 1–7. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Hedges, L.V.; Olkin, I. Statistical Methods for Meta-Analysis; Academic Press: Cambridge, MA, USA; Elsevier Inc.: Amsterdam, The Netherlands, 1985. [Google Scholar] [CrossRef]
- Yang, J.; Zhang, T.; Qi, W.; Zhang, X.; Jia, M.; Leng, Z.; Wang, Q.; Yang, Y.; Yang, W.; Ma, L. COVID-19 vaccination in Chinese children: A cross-sectional study on the cognition, psychological anxiety state and the willingness toward vaccination. Hum. Vaccines Immunother. 2022, 18, 1–7. [Google Scholar] [CrossRef]
- Yılmazbas, P.; Terzi, O.; Ozceker, D. Did COVID-19 Pandemic Changed Parents’ Approach to Vaccination? Soc. Behav. 2021, 43, 130–134. [Google Scholar] [CrossRef]
- Kelly, B.J.; Southwell, B.G.; McCormack, L.A.; Bann, C.M.; MacDonald, P.D.; Frasier, A.M.; Bevc, C.A.; Brewer, N.T.; Squiers, L.B. Predictors of willingness to get a COVID-19 vaccine in the US. BMC Infect. Dis. 2021, 21, 338. [Google Scholar]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Chinese parents’ intentions to vaccinate their children against SARS-CoV-2 infection and vaccine preferences. Hum. Vaccines Immunother. 2021, 17, 4806–4815. [Google Scholar] [CrossRef]
- Goldman, R.D.; Yan, T.D.; Seiler, M.; Cotanda, C.P.; Brown, J.C.; Klein, E.J.; Hoeffe, J.; Gelernter, R.; Hall, J.E.; Davis, A.L. Caregiver willingness to vaccinate their children against COVID-19: Cross sectional survey. Vaccine 2020, 38, 7668–7673. [Google Scholar] [CrossRef]
- Goldman, R.D.; Ceballo, R.; Group, I.C.P.A.S. Parental gender differences in attitudes and willingness to vaccinate against COVID-19. J. Paediatr. Child Health 2022, 58, 1016–1021. [Google Scholar] [CrossRef]
- Hetherington, E.; Edwards, S.A.; MacDonald, S.E.; Racine, N.; Madigan, S.; McDonald, S.; Tough, S. SARS-CoV-2 vaccination intentions among mothers of children aged 9 to 12 years: A survey of the All Our Families cohort. Can. Med. Assoc. Open Access J. 2021, 9, E548–E555. [Google Scholar] [CrossRef] [PubMed]
- Ennaceur, S.; Al-Mohaithef, M. Parents’ Willingness to Vaccinate Children against COVID-19 in Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 156. [Google Scholar] [CrossRef] [PubMed]
- Brandstetter, S.; Böhmer, M.M.; Pawellek, M.; Seelbach-Göbel, B.; Melter, M.; Kabesch, M.; Apfelbacher, C. Parents’ intention to get vaccinated and to have their child vaccinated against COVID-19: Cross-sectional analyses using data from the KUNO-Kids health study. Eur. J. Pediatr. 2021, 180, 3405–3410. [Google Scholar] [CrossRef]
- Davis, M.M.; Zickafoose, J.S.; Halvorson, A.E.; Patrick, S.W. Parents’ likelihood to vaccinate their children and themselves against COVID-19. MedRxiv 2020. [Google Scholar] [CrossRef]
- Gjini, E.; Moramarco, S.; Carestia, M.; Cenko, F.; Ylli, A.; Mehmeti, I.; Palombi, L.; Buonomo, E. Parents’ and caregivers’ role toward childhood vaccination in Albania: Assessment of predictors of vaccine hesitancy. Ann. Di Ig. Med. Prev. E Di Comunita 2022, 35, 75–83. [Google Scholar]
- Kezhong, A.; Lu, X.; Wang, J.; Hu, L.; Li, B.; Lu, Y. Association between adult vaccine hesitancy and parental acceptance of childhood COVID-19 vaccines: A web-based survey in a northwestern region in China. Vaccines 2021, 9, 1088. [Google Scholar]
- Çelik, M.Y. The thoughts of parents to vaccinate their children against COVID-19: An assessment of situations that may affect them. J. Child Adolesc. Psychiatr. Nurs. 2022, 35, 189–195. [Google Scholar] [CrossRef]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.Q.; Zhou, X.; Wang, Z. Parental acceptability of COVID-19 vaccination for children under the age of 18 years: Cross-sectional online survey. JMIR Pediatr. Parent. 2020, 3, e24827. [Google Scholar] [CrossRef]
- Wang, Q.; Xiu, S.; Yang, L.; Han, Y.; Cui, T.; Shi, N.; Liu, M.; Yi, Y.; Liu, C.; Wang, X. Changes in Parental Attitudes Toward COVID-19 Vaccination and Routine Childhood Vaccination During the COVID-19 Pandemic: Repeated Cross-sectional Survey Study. JMIR Public Health Surveill. 2022, 8, e33235. [Google Scholar] [CrossRef]
- Letterie, M.C.; Patrick, S.W.; Halvorson, A.E.; Dupont, W.D.; Carroll, K.N.; Zickafoose, J.S.; Williams, S.E. Factors Associated With Parental COVID-19 Vaccination Acceptance. Clin. Pediatr. 2022, 61, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Xiu, S.; Zhao, S.; Wang, J.; Han, Y.; Dong, S.; Huang, J.; Cui, T.; Yang, L.; Shi, N. Vaccine hesitancy: COVID-19 and influenza vaccine willingness among parents in Wuxi, China—A cross-sectional study. Vaccines 2021, 9, 342. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; She, R.; Chen, X.; Li, L.; Li, L.; Huang, Z.; Lau, J.T. Parental acceptability of COVID-19 vaccination for children under the age of 18 years among Chinese doctors and nurses: A cross-sectional online survey. Hum. Vaccines Immunother. 2021, 17, 3322–3332. [Google Scholar] [CrossRef] [PubMed]
- Altulahi, N.; AlNujaim, S.; Alabdulqader, A.; Alkharashi, A.; AlMalki, A.; AlSiari, F.; Bashawri, Y.; Alsubaie, S.; AlShahrani, D.; AlGoraini, Y. Willingness, beliefs, and barriers regarding the COVID-19 vaccine in Saudi Arabia: A multiregional cross-sectional study. BMC Fam. Pract. 2021, 22, 247. [Google Scholar] [CrossRef] [PubMed]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Reindl, D.; Catma, S. A pre-vaccine analysis using the Health Belief Model to explain parents’ willingness to vaccinate (WTV) their children in the United States: Implications for vaccination programs. Expert Rev. Pharm. Outcomes Res. 2022, 22, 753–761. [Google Scholar] [CrossRef]
- Feng, H.; Zhu, H.; Zhang, H.; Cao, L.; Li, L.; Wang, J.; Huang, Y.; Lai, X.; Lyu, Y.; Jing, R. Caregivers’ intentions to COVID-19 vaccination for their children in China: A cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 4799–4805. [Google Scholar] [CrossRef]
- Montalti, M.; Rallo, F.; Guaraldi, F.; Bartoli, L.; Po, G.; Stillo, M.; Perrone, P.; Squillace, L.; Dallolio, L.; Pandolfi, P. Would parents get their children vaccinated against SARS-CoV-2? Rate and predictors of vaccine hesitancy according to a survey over 5000 families from Bologna, Italy. Vaccines 2021, 9, 366. [Google Scholar] [CrossRef]
- Padhi, B.K.; Satapathy, P.; Rajagopal, V.; Rustagi, N.; Vij, J.; Jain, L.; Chakrapani, V.; Patro, B.K.; Kar, S.S.; Singh, R. Parents’ Perceptions and Intention to Vaccinate Their Children Against COVID-19: Results From a Cross-Sectional National Survey in India. Front. Med. 2022, 9, 806702. [Google Scholar] [CrossRef]
- Humble, R.M.; Sell, H.; Dubé, E.; MacDonald, N.E.; Robinson, J.; Driedger, S.M.; Sadarangani, M.; Meyer, S.B.; Wilson, S.; Benzies, K.M. Canadian parents’ perceptions of COVID-19 vaccination and intention to vaccinate their children: Results from a cross-sectional national survey. Vaccine 2021, 39, 7669–7676. [Google Scholar] [CrossRef]
- Xu, Y.; Zhang, R.; Zhou, Z.; Fan, J.; Liang, J.; Cai, L.; Peng, L.; Ren, F.; Lin, W. Parental psychological distress and attitudes towards COVID-19 vaccination: A cross-sectional survey in Shenzhen, China. J. Affect. Disord. 2021, 292, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Tao, L.; Liu, J. The association between risk perception and COVID-19 vaccine hesitancy for children among reproductive women in China: An online survey. Front. Med. 2021, 8, 1494. [Google Scholar] [CrossRef] [PubMed]
- Alsulaiman, J.W.; Mazin, M.; Al-Shatanawi, T.N.; Kheirallah, K.A.; Allouh, M.Z. Parental Willingness to Vaccinate Their Children Against SARS-CoV-2 in Jordan: An Explanatory Cross-Sectional Study. Risk Manag. Healthc. Policy 2022, 15, 955. [Google Scholar] [CrossRef] [PubMed]
- Aldakhil, H.; Albedah, N.; Alturaiki, N.; Alajlan, R.; Abusalih, H. Vaccine hesitancy towards childhood immunizations as a predictor of mothers’ intention to vaccinate their children against COVID-19 in Saudi Arabia. J. Infect. Public Health 2021, 14, 1497–1504. [Google Scholar] [CrossRef]
- Kreuter, M.W.; Garg, R.; Marsh, A.; Thompson, T.; Caburnay, C.; Teshome, E.; Kulkarni, S.; Tanpattana, T.; Wolff, J.; McQueen, A. Intention to vaccinate children for COVID-19: A segmentation analysis among Medicaid parents in Florida. Prev. Med. 2022, 156, 106959. [Google Scholar] [CrossRef]
- Wan, X.; Huang, H.; Shang, J.; Xie, Z.; Jia, R.; Lu, G.; Chen, C. Willingness and influential factors of parents of 3-6-year-old children to vaccinate their children with the COVID-19 vaccine in China. Hum. Vaccines Immunother. 2021, 17, 3969–3974. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yan, W.; Lu, L.; Cao, L.; Tian, Y.; Zhou, K. Chinese parent intention to vaccinate children with special diseases against COVID-19. Front. Public Health 2021, 9, 725980. [Google Scholar] [CrossRef]
- Evans, S.; Klas, A.; Mikocka-Walus, A.; German, B.; Rogers, G.; Ling, M.; Fernando, J.; Kothe, E.; Westrupp, E. “Poison” or “protection”? A mixed methods exploration of Australian parents’ COVID-19 vaccination intentions. J. Psychosom. Res. 2021, 150, 110626. [Google Scholar] [CrossRef]
- Delgado-Gallegos, J.L.; Padilla-Rivas, G.R.; Gastelum-Arias, L.J.; Zuñiga-Violante, E.; Avilés-Rodríguez, G.; Arellanos-Soto, D.; Franco-Villareal, H.; Garza-Treviño, E.N.; Cosío-León, M.d.l.Á.; Romo-Cardenas, G.S. Parent’s perspective towards child COVID-19 vaccination: An online cross-sectional study in Mexico. Int. J. Environ. Res. Public Health 2021, 19, 290. [Google Scholar] [CrossRef]
- Yılmaz, M.; Sahin, M.K. Parents’ willingness and attitudes concerning the COVID-19 vaccine: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e14364. [Google Scholar] [CrossRef]
- Al-Khlaiwi, T.; Meo, S.A.; Almousa, H.A.; Almebki, A.A.; Albawardy, M.K.; Alshurafa, H.H.; Althunayan, M.A.; Alsayyari, M.S. National COVID-19 vaccine program and parent’s perception to vaccinate their children: A cross-sectional study. Vaccines 2022, 10, 168. [Google Scholar] [CrossRef] [PubMed]
- Derdemezis, C.; Markozannes, G.; Rontogianni, M.O.; Trigki, M.; Kanellopoulou, A.; Papamichail, D.; Aretouli, E.; Ntzani, E.; Tsilidis, K.K. Parental Hesitancy towards the Established Childhood Vaccination Programmes in the COVID-19 Era: Assessing the Drivers of a Challenging Public Health Concern. Vaccines 2022, 10, 814. [Google Scholar] [CrossRef] [PubMed]
- Szilagyi, P.G.; Shah, M.D.; Delgado, J.R.; Thomas, K.; Vizueta, N.; Cui, Y.; Vangala, S.; Shetgiri, R.; Kapteyn, A. Parents’ intentions and perceptions about COVID-19 vaccination for their children: Results from a national survey. Pediatrics 2021, 14, e2021052335. [Google Scholar] [CrossRef] [PubMed]
- Çağ, Y.; Bektemür, G.; Karabela, Ş.; Öztürk-Engin, D.; Çağ, Y.; Aktaş, S.; Kart-Yaşar, K. Parents’ Attitudes Toward COVID-19 Vaccination and Childhood Vaccines During the COVID-19 Pandemic. Asia Pac. J. Public Health 2022, 34, 270–272. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, C.A.; Borrell, L.N.; Shen, Y.; Kimball, S.; Rinke, M.L.; Fleary, S.A.; Nash, D. Parental plans to vaccinate children for COVID-19 in New York city. Vaccine 2021, 39, 5082–5086. [Google Scholar] [CrossRef]
- Teasdale, C.A.; Borrell, L.N.; Kimball, S.; Rinke, M.L.; Rane, M.; Fleary, S.A.; Nash, D. Plans to vaccinate children for coronavirus disease 2019: A survey of United States parents. J. Pediatr. 2021, 237, 292–297. [Google Scholar] [CrossRef]
- Schilling, S.; Orr, C.J.; Delamater, A.M.; Flower, K.B.; Heerman, W.J.; Perrin, E.M.; Rothman, R.L.; Yin, H.S.; Sanders, L. COVID-19 vaccine hesitancy among low-income, racially and ethnically diverse US parents. Patient Educ. Couns. 2022, 105, 2771–2777. [Google Scholar] [CrossRef]
- Skeens, M.A.; Hill, K.; Olsavsky, A.; Buff, K.; Stevens, J.; Akard, T.F.; Shah, N.; Gerhardt, C.A. Factors affecting COVID-19 vaccine hesitancy in parents of children with cancer. Pediatr. Blood Cancer 2022, 69, e29707. [Google Scholar] [CrossRef]
- Alfieri, N.L.; Kusma, J.D.; Heard-Garris, N.; Davis, M.M.; Golbeck, E.; Barrera, L.; Macy, M.L. Parental COVID-19 vaccine hesitancy for children: Vulnerability in an urban hotspot. BMC Public Health 2021, 21, 1662. [Google Scholar] [CrossRef]
- Lachance-Grzela, M.; Charbonneau, A.; Dubé, A.; Jbilou, J.; Richard, J. Parents and caregivers’ willingness to vaccinate their children against COVID-19. Can. J. Behav. Sci./Rev. Can. Des Sci. Du Comport. 2022, 1–6. [Google Scholar] [CrossRef]
- Yoda, T.; Katsuyama, H. Parents’ hesitation about getting their children vaccinated against COVID-19 in Japan. Hum. Vaccines Immunother. 2021, 17, 4993–4998. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, G.; Pelullo, C.P.; Volgare, A.S.; Napolitano, F.; Pavia, M. Parents’ Willingness to Vaccinate Their Children With COVID-19 Vaccine: Results of a Survey in Italy. J. Adolesc. Health 2022, 70, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Musa, S.; Dergaa, I.; Abdulmalik, M.A.; Ammar, A.; Chamari, K.; Saad, H.B. BNT162b2 COVID-19 vaccine hesitancy among parents of 4023 young adolescents (12–15 years) in Qatar. Vaccines 2021, 9, 981. [Google Scholar] [CrossRef]
- Atad, E.; Netzer, I.; Peleg, O.; Landsman, K.; Dalyot, K.; Reuven, S.E.; Baram-Tsabari, A. Vaccine-hesitant parents’ considerations regarding COVID-19 vaccination of adolescents. medRxiv 2021. [Google Scholar] [CrossRef]
- Al-Nafeesah, A.S.; Aldamigh, A.S.; Almansoor, B.A.; Al-Wutayd, O. The impact of the COVID-19 pandemic on parents’ behavior toward scheduled pediatric vaccinations in Saudi Arabia. J. Infect. Dev. Ctries. 2021, 15, 1054–1058. [Google Scholar] [CrossRef]
- Choi, S.-H.; Jo, Y.H.; Jo, K.J.; Park, S.E. Pediatric and parents’ attitudes towards COVID-19 vaccines and intention to vaccinate for children. J. Korean Med. Sci. 2021, 36, e227. [Google Scholar] [CrossRef]
- Wagner, A.; Liberatore, F.; Schmelzer, S.; Dratva, J. Confident and altruistic–parents’ motives to vaccinate their children against COVID-19: A cross-sectional online survey in a Swiss vaccination centre. Swiss Med. Wkly. 2022, 152, w30156. [Google Scholar] [CrossRef]
- Babicki, M.; Pokorna-Kałwak, D.; Doniec, Z.; Mastalerz-Migas, A. Attitudes of parents with regard to vaccination of children against COVID-19 in Poland. a nationwide online survey. Vaccines 2021, 9, 1192. [Google Scholar] [CrossRef]
- Horiuchi, S.; Sakamoto, H.; Abe, S.K.; Shinohara, R.; Kushima, M.; Otawa, S.; Yui, H.; Akiyama, Y.; Ooka, T.; Kojima, R. Factors of parental COVID-19 vaccine hesitancy: A cross sectional study in Japan. PLoS ONE 2021, 16, e0261121. [Google Scholar] [CrossRef]
- Choi, K.; Becerra-Culqui, T.; Bhakta, B.; Bruxvoort, K.; Coleman, K.J. Parent intentions to vaccinate children with autism spectrum disorder against COVID-19. J. Pediatr. Nurs. 2022, 63, 108–110. [Google Scholar] [CrossRef]
- Samannodi, M.; Alwafi, H.; Naser, A.Y.; Alabbasi, R.; Alsahaf, N.; Alosaimy, R.; Minshawi, F.; Almatrafi, M.; Khalifa, R.; Ekram, R. Assessment of caregiver willingness to vaccinate their children against COVID-19 in Saudi Arabia: A cross-sectional study. Hum. Vaccines Immunother. 2021, 17, 4857–4864. [Google Scholar] [CrossRef]
- Gendler, Y.; Ofri, L. Investigating the influence of vaccine literacy, vaccine perception and vaccine hesitancy on Israeli parents’ acceptance of the COVID-19 vaccine for their children: A cross-sectional study. Vaccines 2021, 9, 1391. [Google Scholar] [CrossRef] [PubMed]
- Zona, S.; Partesotti, S.; Bergomi, A.; Rosafio, C.; Antodaro, F.; Esposito, S. Anti-COVID vaccination for adolescents: A survey on determinants of vaccine parental hesitancy. Vaccines 2021, 9, 1309. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, B.; Quach, C.; Dubé, È.; Nguyen, C.T.; Zinszer, K. Social inequalities in COVID-19 vaccine acceptance and uptake for children and adolescents in Montreal, Canada. Vaccine 2021, 39, 7140–7145. [Google Scholar] [CrossRef] [PubMed]
- Almusbah, Z.; Alhajji, Z.; Alshayeb, Z.; Alhabdan, R.; Alghafli, S.; Almusabah, M.; Almuqarrab, F.; Aljazeeri, I.; Almuhawas, F. Caregivers’ willingness to vaccinate their children against COVID-19 in Saudi Arabia: A cross-sectional survey. Cureus 2021, 13, e17243. [Google Scholar] [CrossRef]
- Urrunaga-Pastor, D.; Herrera-Añazco, P.; Uyen-Cateriano, A.; Toro-Huamanchumo, C.J.; Rodriguez-Morales, A.J.; Hernandez, A.V.; Benites-Zapata, V.A.; Bendezu-Quispe, G. Prevalence and factors associated with parents’ non-intention to vaccinate their children and adolescents against COVID-19 in Latin America and the Caribbean. Vaccines 2021, 9, 1303. [Google Scholar] [CrossRef]
- Kocamaz, E.B.; Kocamaz, H. Awareness of COVID-19 and attitudes toward vaccination in parents of children between 0 and 18 years: A cross-sectional study. J. Pediatr. Nurs. 2022, 65, 75–81. [Google Scholar] [CrossRef]
- Griva, K.; Tan, K.Y.; Chan, F.H.; Periakaruppan, R.; Ong, B.W.; Soh, A.S.; Chen, M.I. Evaluating Rates and Determinants of COVID-19 Vaccine Hesitancy for Adults and Children in the Singapore Population: Strengthening Our Community’s Resilience against Threats from Emerging Infections (SOCRATEs) Cohort. Vaccines 2021, 9, 1415. [Google Scholar] [CrossRef]
- Alhazza, S.F.; Altalhi, A.M.; Alamri, K.M.; Alenazi, S.S.; Alqarni, B.A.; Almohaya, A.M. Parents’ Hesitancy to Vaccinate Their Children Against COVID-19, a Country-Wide Survey. Front. Public Health 2022, 10, 755073. [Google Scholar] [CrossRef]
- McElfish, P.A.; Willis, D.E.; Shah, S.K.; Reece, S.; Andersen, J.A.; Schootman, M.; Richard-Davis, G.; Selig, J.P.; Warmack, T.S. Parents’ and Guardians’ Intentions to Vaccinate Children against COVID-19. Vaccines 2022, 10, 361. [Google Scholar] [CrossRef]
- Russo, L.; Croci, I.; Campagna, I.; Pandolfi, E.; Villani, A.; Reale, A.; Barbieri, M.A.; Raponi, M.; Gesualdo, F.; Tozzi, A.E. Intention of Parents to Immunize Children against SARS-CoV-2 in Italy. Vaccines 2021, 9, 1469. [Google Scholar] [CrossRef] [PubMed]
- Temsah, M.-H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O. Parental attitudes and hesitancy about COVID-19 vs. routine childhood vaccinations: A national survey. Front. Public Health 2021, 9, 752323. [Google Scholar] [CrossRef] [PubMed]
- Mohan, R.; Pandey, V.; Kumar, A.; Gangadevi, P.; Goel, A.D.; Joseph, J.; Kurien, N. Acceptance and Attitude of Parents Regarding COVID-19 Vaccine for Children: A Cross-Sectional Study. Cureus 2022, 14, 24518. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Moisoglou, I.; Kaitelidou, D. Predictors of parents’ intention to vaccinate their children against the COVID-19 in Greece: A cross-sectional study. medRxiv 2021. [Google Scholar] [CrossRef]
- Willis, D.E.; Schootman, M.; Shah, S.K.; Reece, S.; Selig, J.P.; Andersen, J.A.; McElfish, P.A. Parent/guardian intentions to vaccinate children against COVID-19 in the United States. Hum. Vaccines Immunother. 2022, 18, 2071078. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, L. Parents’ intention to vaccinate their 5-11 years old children with the COVID-19 vaccine: Rates, predictors and the role of incentives. MedRxiv 2021. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Yang, J.; Zhang, T.; Han, X.; Huang, Q.; Yang, Y.; Feng, L.; Yang, W.; Wang, C. Willingness toward COVID-19 vaccination, coadministration with other vaccines and receive a COVID-19 vaccine booster: A cross-sectional study on the guardians of children in China. Hum. Vaccines Immunother. 2022, 18, 2049169. [Google Scholar] [CrossRef]
- Ali, M.; Ahmed, S.; Bonna, A.S.; Sarkar, A.-s.; Islam, M.A.; Urmi, T.A.; Proma, T.S. Parental coronavirus disease vaccine hesitancy for children in Bangladesh: A cross-sectional study. F1000Research 2022, 11, 90. [Google Scholar] [CrossRef]
- Li, T.; Qiu, X.; Gong, X.; Zhan, R.; Zheng, X. The cross-sectional survey on COVID-19 vaccine hesitancy and it predictors among Chinese parents of 3–17 years aged children in Shenzhen City. Ann. Agric. Environ. Med. 2022, 29, 120–125. [Google Scholar] [CrossRef]
- Ali, M.; Proma, T.S.; Tasnim, Z.; Islam, M.; Urmi, T.A.; Ahmed, S.; Sarkar, A.-S.; Bonna, A.S.; Khan, U.S. Parental COVID-19 vaccine hesitancy for children with neurodevelopmental disorders: A cross-sectional survey. Trop. Med. Health 2022, 50, 24. [Google Scholar] [CrossRef]
- Fisher, C.B.; Gray, A.; Sheck, I. COVID-19 pediatric vaccine hesitancy among racially diverse parents in the United States. Vaccines 2021, 10, 31. [Google Scholar] [CrossRef]
- Al-Qerem, W.; Al Bawab, A.Q.; Hammad, A.; Jaber, T.; Khdair, S.I.; Kalloush, H.; Ling, J.; Mosleh, R. Parents’ attitudes, knowledge and practice towards vaccinating their children against COVID-19: A cross-sectional study. Hum. Vaccines Immunother. 2022, 18, 2044257. [Google Scholar] [CrossRef]
- Tsai, C.-S.; Wang, L.-J.; Hsiao, R.C.; Yen, C.-F. Second Wave of the Study of Taiwanese Caregivers of Children with ADHD in the COVID-19 Pandemic: Intentions to Vaccinate Their Children for COVID-19, and Related Factors. Vaccines 2022, 10, 753. [Google Scholar] [CrossRef]
- Kheil, M.H.; Jain, D.; Jomaa, J.; Askar, B.; Alcodray, Y.; Wahbi, S.; Brikho, S.; Kadouh, A.; Harajli, D.; Jawad, Z.N. COVID-19 Vaccine Hesitancy among Arab Americans. Vaccines 2022, 10, 610. [Google Scholar] [CrossRef]
- Al-Qerem, W.; Jarab, A.; Hammad, A.; Alasmari, F.; Ling, J.; Alsajri, A.H.; Al-Hishma, S.W.; Abu Heshmeh, S.R. Iraqi Parents’ Knowledge, Attitudes, and Practices towards Vaccinating Their Children: A Cross-Sectional Study. Vaccines 2022, 10, 820. [Google Scholar] [CrossRef] [PubMed]
- Almalki, O.S.; Alfayez, O.M.; Al Yami, M.S.; Asiri, Y.A.; Almohammed, O.A. Parents’ Hesitancy to Vaccinate Their 5–11-Year-Old Children Against COVID-19 in Saudi Arabia: Predictors From the Health Belief Model. Front. Public Health 2022, 10, 842862. [Google Scholar] [CrossRef] [PubMed]
- Miraglia del Giudice, G.; Napoli, A.; Corea, F.; Folcarelli, L.; Angelillo, I.F. Evaluating COVID-19 Vaccine Willingness and Hesitancy among Parents of Children Aged 5–11 Years with Chronic Conditions in Italy. Vaccines 2022, 10, 396. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Valentini, P.; Macchi, M.; Folino, F.; Pensabene, C.; Patria, M.F.; Agostoni, C.; Castaldi, S.; Lecce, M.; Giannì, M.L. Caregivers’ Attitudes Toward COVID-19 Vaccination in Children and Adolescents With a History of SARS-CoV-2 Infection. Front. Pediatr. 2022, 10, 867968. [Google Scholar] [CrossRef]
- Miliordos, K.; Giannouchos, T.; Steletou, E.; Sanidas, G.; Karkania, A.; Vervenioti, A.; Dimitriou, G.; Gkentzi, D. Parental attitudes towards vaccination against COVID-19 of children 5–11 years old in Greece. J. Eval. Clin. Pract. 2022, 28, 943–947. [Google Scholar] [CrossRef]
- Lau, E.Y.H.; Li, J.-B.; Chan, D.K.C. Intention to vaccinate young children against COVID-19: A large-scale survey of Hong Kong parents. Hum. Vaccines Immunother. 2022, 18, 2065838. [Google Scholar] [CrossRef]
- Aljamaan, F.; Alhaboob, A.; Saddik, B.; Bassrawi, R.; Assiri, R.; Saeed, E.; Alhasan, K.; Alenezi, S.; Alarabi, M.; Alrabiaah, A. In-Person Schooling Amidst Children’s COVID-19 Vaccination: Exploring Parental Perceptions Just after Omicron Variant Announcement. Vaccines 2022, 10, 768. [Google Scholar] [CrossRef] [PubMed]
- Altulaihi, B.A.; Alaboodi, T.; Alharbi, K.G.; Alajmi, M.S.; Alkanhal, H.; Alshehri, A. Perception of parents towards COVID-19 vaccine for children in Saudi population. Cureus 2021, 13, e18342. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, K.M.; Wong, J.; Sweeney, C.F.; Avola, A.; Auger, A.; Macaluso, M.; Reidy, P. Parents’ intentions to vaccinate their children against COVID-19. J. Pediatr. Health Care 2021, 35, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Al Yamani, Z.J.; AlJohani, M.M. Vaccine Hesitancy among Parents and its Determinants in PHC in Al Madinah City 2020. Egypt. J. Hosp. Med. 2022, 87, 1619–1625. [Google Scholar] [CrossRef]
- Yigit, M.; Ozkaya-Parlakay, A.; Senel, E. Evaluation of COVID-19 vaccine refusal in parents. Pediatr. Infect. Dis. J. 2021, 40, e134–e136. [Google Scholar] [CrossRef]
- Wilde, G.J. The theory of risk homeostasis: Implications for safety and health. Risk Anal. 1982, 2, 209–225. [Google Scholar] [CrossRef]
- DiLillo, D.; Tremblay, G. Maternal and child reports of behavioral compensation in response to safety equipment usage. J. Pediatr. Psychol. 2001, 26, 175–184. [Google Scholar] [CrossRef]
- Wallach, M.A.; Kogan, N.; Bem, D.J. Diffusion of responsibility and level of risk taking in groups. J. Abnorm. Soc. Psychol. 1964, 68, 263. [Google Scholar] [CrossRef]
- Hudson, J.M.; Bruckman, A.S. The bystander effect: A lens for understanding patterns of participation. J. Learn. Sci. 2004, 13, 165–195. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Publication Year | Data Collection Time | Country, WHO Region, Developing Status, Income Level | N Mother s % Parents Mean Age Children Mid-Range of Age | Study Design Sampling Method Recruitment Method | NOS Score/ Category |
|---|---|---|---|---|---|
| Yang, J. et al., 2021 [52] | 2020.02 | China, WPR, Developing, Upper intermediate income | 12,872 73.09 34 NR | cross sectional Non-random sampling online | 5/ High risk of bias |
| Yılmazbaş, P. et al., 2020 [53] | 2020.04 | USA, AMR, Developed, High income | 440 70.5 33.5 5 | cross sectional Non-random sampling online | 4/ High risk of bias |
| Kelly, B.J. et al., 2021 [54] | 2020.04 | USA, AMR, Developed, High income | 2247 52 41.5 9 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Bell, S. et al., 2020 [55] | 2020.04 to 05 | England, EUR, Developed, High income | 1252 95 42 1 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Lin, Y. et al., 2021 [56] | 2020.05 | China, WPR, Developing, Upper intermediate income | 2026 48.5 34 6.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Goldman, R.D. et al., 2020 [57] | 2020.04 to 05 | six countries, Developed | 1541 NR 39.9 7.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Goldman, R.D. et al., 2022 [58] | 2020.03 to 06 | USA, AMR, Developed, High income | 2687 75.36 35 9.5 | cohort Not identified online | 5/ High risk of bias |
| Hetherington, E. et al., 2021 [59] | 2020.05 to 06 | Canada, AMR, Developed, High income | 1321 100 42.2 10.5 | cohort Not identified self-administration | 6/ Low risk of bias |
| Ennaceur, S. et al., 2022 [60] | 2020.03 to 06 | Saudi Arabia, EMR, Developing, High income | 379 49.6 29 NR | cross sectional Non-random sampling online | 5/ High risk of bias |
| Brandstetter, S. et al., 2021 [61] | 2020.05 | Germany, EUR, Developed, High income | 612 NR NR 3.4 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Davis, M.M. et al., 2020 [62] | 2020.06 | USA, AMR, Developed, High income | 1008 55 41.5 NR | cross sectional Non-random sampling self-administration | 5/ High risk of bias |
| Gjini, E. et al., 2022 [63] | 2020.06 | Albania, EUR, Developing, Upper intermediate income | 475 89.6 41.5 4 | cross sectional Non-random sampling self-administration | 5/ High risk of bias |
| Kezhong, A. et al., 2021 [64] | 2020.06 to 07 | China, WPR, Developing, Upper intermediate income | 13,451 NR 34.5 9 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Çelik, M.Y. et al., 2021 [65] | 2020.07 to 09 | Turkey, EUR, Developed, Upper intermediate income | 274 65.7 36 3.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Zhang, K.C. et al., 2020 [66] | 2020.09 | China, WPR, Developing, Upper intermediate income | 1052 62.5 41.5 9.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Wang, Q. et al- wave 1, 2022 [67] | 2020.09 to 10 | China, WPR, Developing, Upper intermediate income | 2881 74.5 41.5 NR | cross sectional Non-random sampling online | 7/ Low risk of bias |
| Letterie, M.C. et al., 2022 [68] | 2020.10 to 11 | Korea, SEAR, Developed, High income | 1066 58 41.5 NR | cross sectional Random sampling online | 5/ High risk of bias |
| Wang, Q. et al., 2021 [69] | 2020.09 to 10 | China, WPR, Developing, Upper intermediate income | 3079 49.2 45.5 9 | cross sectional Non-random sampling self-administration | 7/ Low risk of bias |
| Wang, Z. et al., 2021 [70] | 2020.10 to 11 | China, WPR, Developing, Upper intermediate income | 1332 89.4 41.5 9.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Altulahi, N. et al., 2021 [71] | 2020.11 to 12 | Saudi Arabia, EMR, Developing, High income | 3038 54.2 34 9 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Skjefte, M. et al., 2021 [72] | 2020.11 | Sixteen countries | 17,054 100 41.5 NR | cross sectional Non-random sampling online | 5/ High risk of bias |
| Reindl, D. et al., 2022 [73] | 2020.11 | USA, AMR, Developed, High income | 582 56 41.5 NR | cross sectional Non-random sampling online | 5/ High risk of bias |
| Feng, H. et al., 2021 [74] | 2020.11 to 2021.01 | China, WPR, Developing, Upper intermediate income | 3703 57.1 40 NR | cross sectional Non-random sampling face to face interview | 5/ High risk of bias |
| Montalti, M. et al., 2021 [75] | 2020.12 to 2021.01 | Italy, EUR, Developed, High income | 4993 76.56 41.5 9 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Padhi, B.K. et al., 2022 [76] | 2020.11 to 2021.01 | China, WPR, Developing, Upper intermediate income | 770 39.6 41.5 9 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Humble, R.M. et al., 2021 [77] | 2020.12 | Canada, AMR, Developed, High income | 1435 55.3 41 8.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Xu, Y. et al., 2021 [78] | 2020.12 | China, WPR, Developing, Upper intermediate income | 4430 76 41.5 9.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Du, M. et al., 2021 [79] | 2020.12 to 2021.01 | China, WPR, Developing, Upper intermediate income | 3011 100 41.5 9.5 | cross sectional Random sampling online | 7/ Low risk of bias |
| Alsulaiman, J.W. et al., 2022 [80] | 2021.10 to 11 | Jordan, EMR, Developing, Upper intermediate income | 564 82.8 35 8.5 | cross sectional Not identified online | 3/ High risk of bias |
| Aldakhil, H. et al., 2021 [81] | 2021.01 to 02 | Saudi Arabia, EMR, Developing, High income | 270 100 33 3 | cross sectional Non-random sampling self-administration | 6/ Low risk of bias |
| Kreuter, M.W. et al., 2022 [82] | 2021.01 | USA, AMR, Developed, High income | 1951 96 26 2.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Wan, X. et al., 2021 [83] | 2020.12 to 2021.02 | China, WPR, Developing, Upper intermediate income | 468 68.38 30.5 4.5 | cross sectional Random sampling self-administration | 5/ High risk of bias |
| Wang, X. et al., 2021 [84] | 2020.09 to 2021.04 | China, WPR, Developing, Upper intermediate income | 941 NR NR 1.4 | cross sectional Non-random sampling face-to-face interview | 5/ High risk of bias |
| Evans, S. et al., 2021 [85] | 2021.01 | Australia, WPR, Developed, High income | 1094 83.1 39.2 8.9 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Delgado-Gallegos, J.L. et al., 2021 [86] | 2020.12 to 2021.02 | México, AMR, Developing, Upper intermediate income | 699 69.1 42 NR | cross sectional Non-random sampling online | 7/ Low risk of bias |
| Yılmaz, M. et al., 2021 [87] | 2021.02 | Turkey, EUR, Developed, Upper intermediate income | 1035 77.8 41.5 8.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Al-khlaiwi, T. et al., 2022 [88] | 2021.01 to 03 | Saudi Arabia, EMR, Developing, High income | 1052 73.8 34 8.5 | cross sectional Non-random sampling online | 4/ High risk of bias |
| Derdemezis, C. et al., 2022 [89] | 2020.10 to 2021.04 | Greece, EUR, Developing, High income | 1095 65.3 50.25 NR | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Yılmaz, M. et al., 2021 [87] | 2021.02 | Turkey, EUR, Developed, Upper intermediate income | 1035 77.8 41.5 2 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Szilagyi, P.G. et al., 2021 [90] | 2021.02 to 03 | USA, AMR, Developed, High income | 1745 57.91 34 9 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Wang, Q. et al- wave 2, 2022 [67] | 2021.02 to 03 | China, WPR, Developing, Upper intermediate income | 1038 67.3 41.5 NR | cross sectional Non-random sampling online | 7/ Low risk of bias |
| Çağ, Y. et al., 2022 [91] | 2021.03 to 04 | Turkey, EUR, Developed, Upper intermediate income | 1018 79.5 41.5 5.52 | cross sectional Random sampling face to face interview | 5/ High risk of bias |
| Teasdale, C.A. et al., 2021 [92] | 2021.03 to 04 | USA, AMR, Developed, High income | 1119 59 41.5 6 | cross sectional Random sampling self-administration | 5/ High risk of bias |
| Teasdale, C.A. et al., 2021 [93] | 2021.03 | USA, AMR, Developed, High income | 2074 49.5 41.5 6 | cross sectional Random sampling self-administration | 5/ High risk of bias |
| Schilling, S. et al., 2022 [94] | 2021.02 to 03 | USA, AMR, Developed, High income | 50 98 32 9 | cross sectional Non-random sampling face to face interview | 6/ Low risk of bias |
| Skeens, M.A. et al., 2022 [95] | 2021.02 to 05 | USA, AMR, Developed, High income | 491 89.5 38.79 9.16 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Alfieri, N.L. et al., 2021 [96] | 2021.03 | USA, AMR, Developed, High income | 1425 NR NR 8.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Lachance-Grzela, M. et al., 2022 [97] | 2021.03 to 04 | Canada, AMR, Developed, High income | 406 NR NR 8.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Yoda, T. et al., 2021 [98] | 2021.04 | Japan, WPR, Developing, High income | 1100 57.5 38.5 2.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Di Giuseppe, G. et al., 2022 [99] | 2021.04 to 05 | Italy, EUR, Developed, High income | 607 82.4 42.5 9.5 | cross sectional Random sampling online | 6/ Low risk of bias |
| Bagateli, L.E. et al., 2021 [38] | 2021.05 to 06 | Brazil, AMR, Developing, Upper intermediate | 501 85 34 8.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Wang, Q. et al- wave 3, 2022 [67] | 2021.05 to 06 | China, WPR, Developing, Upper intermediate income | 1183 57.5 41.5 NR | cross sectional Non-random sampling online | 7/ Low risk of bias |
| Musa, S. et al., 2021 [100] | 2021.05 to 06 | Qatar, EMR, Developed, High income | 4023 NR NR 13.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Atad, E. et al., 2021 [101] | 2021.04 to 05 | Israel, EUR, Developed, High income | 1118 NR NR 13.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Al-Nafeesah, A.S. et al., 2021 [102] | 2021.05 | Saudi Arabia, EMR, Developing, High income | 1143 88 41.5 3 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Choi, S.-H. et al., 2021 [103] | 2021.05 to 06 | Korea, SEAR, Developed, High income | 226 79.6 41.5 14 | cross sectional Non-random sampling self-administration | 5/ High risk of bias |
| Wagner, A. et al., 2022 [104] | 2021.05 | Switzerland, EUR, Developed, High income | 1344 44.8 41 13.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Babicki, M. et al., 2021 [105] | 2021.05 | Poland, EUR, Developed, High income | 4432 77.6 34 13.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Horiuchi, S. et al., 2021 [106] | 2021.05 to 06 | Japan, WPR, Developing, High income | 1200 49.1 34 8.5 | cross sectional Not identified online | 6/ Low risk of bias |
| Choi, K. et al., 2021 [107] | 2021.05 to 07 | USA, AMR, Developed, High income | 322 NR NR 9.5 | cross sectional Random sampling self-administration | 5/ High risk of bias |
| Samannodi, M. et al., 2021 [108] | 2021.06 to 07 | Saudi Arabia, EMR, Developing, High income | 508 61.3 39 9 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Gendler, Y. et al., 2021 [109] | 2021.06 | Israel, EUR, Developed, High income | 520 77.1 44.76 13.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Zona, S. et al., 2021 [110] | 2021.05 to 07 | Italy, EUR, Developed, High income | 1799 72.4 34 14.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| McKinnon, B. et al., 2021 [111] | 2021.05 to 06 | Canada, AMR, Developed, High income | 809 NR NR 10 | cohort Not identified online | 5/ High risk of bias |
| Almusbah, Z. et al., 2021 [112] | 2021.05 to 06 | Saudi Arabia, EMR, Developing, High income | 1000 47 NR 7 | cross sectional Non-random sampling online | 4/ High risk of bias |
| Urrunaga-Pastor, D. et al., 2021 [113] | 2021.05 to 07 | Latin American countries, AMR, Developed | 227,740 38.37 36 NR | cross sectional Non-random sampling online | 5/ High risk of bias |
| Kocamaz, E.B. et al., 2022 [114] | 2021.05 to 06 | Turkey, EUR, Developed, Upper-intermediate income | 384 68.8 43 9 | cross sectional Non-random sampling online | 7/ Low risk of bias |
| Griva, K. et al., 2021 [115] | 2021.06 to 07 | Singapore, WPR, Developing, High income | 1623 60.8 46.3 15 | cohort Not identified face to face | 5/ High risk of bias |
| Alhazza, S.F. et al., 2021 [116] | 2021.06 | Saudi Arabia, EMR, Developing, High income | 1052 51.5 35 10 | cross sectional Not identified online | 7/ Low risk of bias |
| McElfish, P.A. et al., 2022 [117] | 2021.07 | USA, AMR, Developed, High income | 189 53 41.5 14.5 | cross sectional Random sampling phone interview | 5/ High risk of bias |
| Russo, L. et al., 2021 [118] | 2021.07 to 08 | Italy, EUR, Developed, High income | 1205 81.6 42 6 | cross sectional Non-random sampling online | 5/ High risk of bias |
| McElfish, P.A. et al., 2022 [117] | 2021.07 | USA, AMR, Developed, High income | 168 48 41.5 5.5 | cross sectional Random sampling phone interview | 5/ High risk of bias |
| Temsah, M.H. et al., 2021 [119] | 2021.07 | India, SEAR, Developing, Low income | 3167 65 41.5 15 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Mohan, R. et al., 2022 [120] | 2021.07 to 09 | India, SEAR, Developing, Low income | 204 49.5 34 8.5 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Galanis, P. et al., 2021 [121] | 2021.09 | Greece, EUR, Developing, High income | 813 76.1 42.3 14.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Willis, D.E. et al., 2022, sample 1 [122] | 2021.09 to 10 | USA, AMR, Developed, High income | 342 54.39 35 5.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Shmueli, L., 2021 [123] | 2021.09 to 10 | Israel, EUR, Developed, High income | 1012 NR NR 8 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Willis, D.E. et al., 2022, sample 2 [122] | 2021.09 to 10 | USA, AMR, Developed, High income | 321 51.09 35 14.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Ma, L. et al., 2022 [124] | 2021.09 to 10 | China, WPR, Developing, Upper-intermediate income | 9424 74.79 40 3 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Ali, M. et al., 2022 [125] | 2021.10 | Bangladesh, SEAR, Developing, Low income | 2633 52.8 35 9 | cross sectional Random sampling face-to-face interview | 7/ Low risk of bias |
| Li, T. et al., 2022 [126] | 2021.10 to 11 | China, WPR, Developing, Upper-intermediate income | 3342 64 41.5 10 | cross sectional Non-random sampling online | 6/ Low risk of bias |
| Ali, M. et al., 2022 [127] | 2021.10 | Bangladesh, SEAR, Developing, Low income | 396 60.4 34.5 8.5 | cross sectional Random sampling face-to-face interview | 7/ Low risk of bias |
| Fisher, C.B. et al., 2021 [128] | 2021.10 | USA, AMR, Developed, High income | 400 NR 35 7.4 | cross sectional Non-random sampling online | 4/ High risk of bias |
| Al-Qerem, W. et al., 2022 [129] | 2021.09 to 11 | Jordan, EMR, Developing, Upper-intermediate income | 819 70.9 39 9 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Tsai, C.S. et al., 2022 [130] | 2021.08 to 2022.01 | Taiwan, WPR, Developed, High income | 252 NR 42.23 11.5 | cross sectional Not identified self-administration | 6/ Low risk of bias |
| Kheil, M.H. et al., 2022 [131] | 2021.10 to 11 | USA, AMR, Developed, High income | 1746 55 53 NR | cross sectional Non-random sampling online | 5/ High risk of bias |
| Al-Qerem, W. et al., 2022 [132] | 2021.09 to 2022.02 | Iraq, EMR, Developing, Upper intermediate income | 491 59.3 29 9 | cross sectional Non-random sampling online | 7/ Low risk of bias |
| Almalki, O.S. et al., 2022 [133] | 2021.11 | Saudi Arabia, EMR, Developing, High income | 4135 81 41.5 8 | cross sectional Random sampling online | 5/ High risk of bias |
| Miraglia del Giudice, G. et al., 2022 [134] | 2021.12 to 2022.01 | Italy, EUR, Developed, High income | 427 86.5 41 8 | cross sectional Random sampling phone interview | 7/ Low risk of bias |
| Buonsenso et al., 2022 [135] | 2021.11 to 2022.01 | Italy, EUR, Developed, High income | 121 80 42.5 7 | cross sectional Non-random sampling phone interview | 5/ High risk of bias |
| Miliordos, K. et al., 2022 [136] | 2021.12 to 2022.01 | Greece, EUR, Developing, High income | 366 58.2 35 8 | cross sectional Not identified face-to-face interview | 5/ High risk of bias |
| Lau et al., 2022 [137] | 2022.01 | Hong Kong, WPR, Developed, High income | 11,141 86 40 8.5 | cross sectional Non-random sampling online | 5/ High risk of bias |
| Aljamaan, F. et al., 2022 [138] | 2022.01 | Saudi Arabia, EMR, Developing, High income | 1340 65.3 44.5 8 | cross sectional Non-random sampling online | 4/ High risk of bias |
| Aljamaan, F. et al., 2022 [138] | 2022.01 | Saudi Arabia, EMR, Developing, High income | 1340 65.3 44.5 15 | cross sectional Non-random sampling online | 4/ High risk of bias |
| Altulaihi, B.A. et al., 2021 [139] | NR | Saudi Arabia, EMR, Developing, High income | 333 NR 41.5 8.5 | cross sectional Non-random sampling self-administration | 3/ High risk of bias |
| Ruggiero, K.M. et al., 2021 [140] | NR | USA, AMR, Developed, High income | 427 NR NR 9.5 | cross sectional Non-random sampling online | 7/ Low risk of bias |
| Al Yamani, Z.J. et al., 2022 [141] | NR | Saudi Arabia, EMR, Developing, High income | 375 33.9 NR 3.5 | cross sectional Random sampling self-administration | 6/ Low risk of bias |
| Yigit, M. et al., 2021 [142] | NR | Turkey, EUR, Developed, Upper intermediate income | 428 63.6 39.7 NR | cross sectional Non-random sampling face-to-face interview | 5/ High risk of bias |
| Subgroups | No. of Studies | ES (95% CI) | I2 (%) | Heterogeneity between Subgroups | |
|---|---|---|---|---|---|
| Risk of bias | Low risk of bias | 40 | 61 (56; 67) | 99.76 | 0.13 |
| High Risk of bias | 58 | 54 (46; 62) | 99.94 | ||
| Country development status | Developed | 53 | 55 (47; 63) | 99.93 | 0.46 |
| Developing | 45 | 59 (52; 66) | 99.87 | ||
| Country Income level | Low income | 4 | 62 (50; 73) | 98.61 | 0.01 |
| Upper-intermediate income | 29 | 65 (59; 71) | 99.80 | ||
| High income | 62 | 52 (46; 58) | 99.75 | ||
| Multiple countries | 3 | 76 (56; 96) | - | ||
| Country location in WHO’s regions | Americas (AMRO) | 27 | 58 (50; 67) | 99.82 | <0.001 |
| South-East Asia (SEARO) | 5 | 62 (52; 72) | 98.22 | ||
| Europe (EURO) | 24 | 51 (43; 59) | 99.49 | ||
| Eastern Mediterranean (EMRO) | 17 | 45 (34; 56) | 99.70 | ||
| Western Pacific (WPRO) | 23 | 67 (56; 78) | 99.95 | ||
| Multiple countries | 2 | 69 (68; 70) | - | ||
| Sampling method | Random sampling | 15 | 52 (39; 65) | 99.74 | 0.46 |
| Non-random sampling | 74 | 59 (53; 64) | 99.92 | ||
| Not identified | 9 | 50 (31; 69) | 99.79 | ||
| Validated measure for assessing parents’ willingness to vaccinate their children | Yes | 50 | 56 (50; 62) | 99.90 | 0.13 |
| No | 40 | 56 (48; 64) | 99.87 | ||
| Not identified | 8 | 67 (57; 77) | 99.52 | ||
| Data collection method | Online | 72 | 58 (53; 64) | 99.93 | 0.02 |
| Self-administered | 13 | 56 (48; 63) | 98.52 | ||
| Phone interview | 4 | 35 (22; 49) | 94.42 | ||
| Face-to-face Interview | 9 | 55 (33; 76) | 99.85 | ||
| Variable | Number of Studies | Coefficient | S.E. | p | I2 res. (%) | Adj. R2 (%) | τ2 |
|---|---|---|---|---|---|---|---|
| Percentage of mothers participated in study | 83 | 0.001 | 0.002 | 0.51 | 99.87 | −0.68 | 0.04 |
| Mean age of parents | 86 | −0.004 | 0.005 | 0.46 | 99.90 | −0.51 | 0.05 |
| Mid-range of children’s age | 82 | −0.007 | 0.007 | 0.27 | 99.86 | 0.32 | 0.04 |
| Data collection time | 94 | −0.14 | 0.04 | 0.001 | 99.92 | 9.78 | 0.04 |
| Country % of people received at least one dose of COVID-19 vaccine at time of data collection | 70 | −0.001 | 0.001 | 0.11 | 99.83 | 2.39 | 0.04 |
| Country % of people fully vaccinated with COVID-19 vaccine at time of data collection | 70 | −0.001 | 0.001 | 0.15 | 99.83 | 1.63 | 0.04 |
| Variable | Coefficient | S.E. | p | Model Summary |
|---|---|---|---|---|
| Data collection time | −0.13 | 0.04 | 0.003 | Number of studies: 91 tau2: 0.04 |
| Country income level | −0.07 | 0.04 | 0.06 | I2 res. (%): 99.76 |
| Country location in WHO’s regions | 0.003 | 0.01 | 0.82 | Adj. R2 (%): 11.44 |
| Data collection method | 0.007 | 0.03 | 0.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alimoradi, Z.; Lin, C.-Y.; Pakpour, A.H. Worldwide Estimation of Parental Acceptance of COVID-19 Vaccine for Their Children: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 533. https://doi.org/10.3390/vaccines11030533
Alimoradi Z, Lin C-Y, Pakpour AH. Worldwide Estimation of Parental Acceptance of COVID-19 Vaccine for Their Children: A Systematic Review and Meta-Analysis. Vaccines. 2023; 11(3):533. https://doi.org/10.3390/vaccines11030533
Chicago/Turabian StyleAlimoradi, Zainab, Chung-Ying Lin, and Amir H. Pakpour. 2023. "Worldwide Estimation of Parental Acceptance of COVID-19 Vaccine for Their Children: A Systematic Review and Meta-Analysis" Vaccines 11, no. 3: 533. https://doi.org/10.3390/vaccines11030533
APA StyleAlimoradi, Z., Lin, C.-Y., & Pakpour, A. H. (2023). Worldwide Estimation of Parental Acceptance of COVID-19 Vaccine for Their Children: A Systematic Review and Meta-Analysis. Vaccines, 11(3), 533. https://doi.org/10.3390/vaccines11030533