
Within-Country Inequality in COVID-19 Vaccination Coverage: A Scoping Review of Academic Literature




Abstract
1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Screening Process
- Wrong article type;
- Does not pertain to humans;
- Study objective not relevant;
- Does not meet criteria for COVID-19 vaccination coverage;
- Does not meet criteria for dimension of inequality;
- Only reports on between-country inequality;
- Full text not available;
- Insufficient information to assess eligibility.
2.3. Data Extraction and Analysis
3. Results
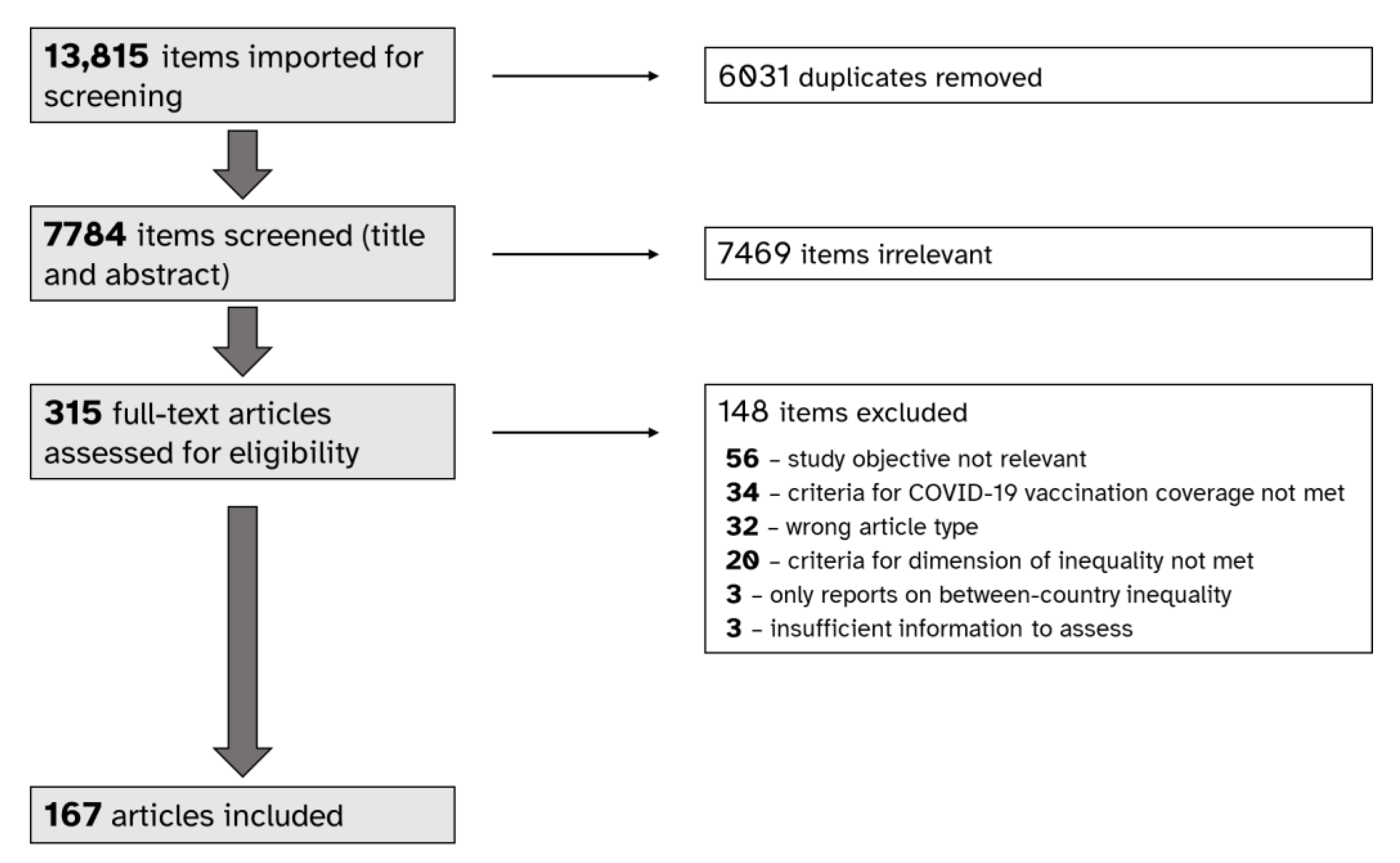
3.1. Selection of Sources
3.2. Study Characteristics
3.2.1. Setting and Study Populations
3.2.2. COVID-19 Vaccination Coverage
3.2.3. Dimensions of Inequality
3.2.4. Reporting Practices
3.3. Study Findings: Preliminary Trends for Selected Dimensions of Inequality
3.3.1. Age
3.3.2. Race, Ethnicity, Cultural Group, Language, Nationality or Country of Birth
3.3.3. Sex or Gender
4. Discussion
Limitations and Further Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in Health: Definitions, Concepts, and Theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef] [PubMed]
- High-Level Committee on Programmes Inequalities Task Team. COVID-19, Inequalities and Building Back Better: Policy Brief by the HLCP Inequalities Task Team; United Nations: New York, NY, USA, 2020. [Google Scholar]
- Burström, B.; Tao, W. Social Determinants of Health and Inequalities in COVID-19. Eur. J. Public Health 2020, 30, 617–618. [Google Scholar] [CrossRef] [PubMed]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global Impact of the First Year of COVID-19 Vaccination: A Mathematical Modelling Study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Kumari, M.; Lu, R.-M.; Li, M.-C.; Huang, J.-L.; Hsu, F.-F.; Ko, S.-H.; Ke, F.-Y.; Su, S.-C.; Liang, K.-H.; Yuan, J.P.-Y.; et al. A Critical Overview of Current Progress for COVID-19: Development of Vaccines, Antiviral Drugs, and Therapeutic Antibodies. J. Biomed. Sci. 2022, 29, 68. [Google Scholar] [CrossRef]
- World Health Organization. WHO SAGE Roadmap for Prioritizing Uses of COVID-19 Vaccines; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A Global Database of COVID-19 Vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef]
- Ndugga, N.; Pham, O.; Hill, L.; Artiga, S.; Mengistu, S. Early State Vaccination Data Raise Warning Flags for Racial Equity; Kaiser Family Foundation: Oakland, CA, USA, 2021. [Google Scholar]
- Bergen, N.; Kirkby, K.; Fuertes, C.V.; Schlotheuber, A.; Menning, L.; Mac Feely, S.; O’Brien, K.; Hosseinpoor, A.R. Global State of Education-Related Inequality in COVID-19 Vaccine Coverage, Structural Barriers, Vaccine Hesitancy, and Vaccine Refusal: Findings from the Global COVID-19 Trends and Impact Survey. Lancet Glob. Health 2023, 11, e207–e217. [Google Scholar] [CrossRef]
- Bolcato, M.; Rodriguez, D.; Feola, A.; Di Mizio, G.; Bonsignore, A.; Ciliberti, R.; Tettamanti, C.; Trabucco Aurilio, M.; Aprile, A. COVID-19 Pandemic and Equal Access to Vaccines. Vaccines 2021, 9, 538. [Google Scholar] [CrossRef]
- Bayati, M.; Noroozi, R.; Ghanbari-Jahromi, M.; Jalali, F.S. Inequality in the Distribution of COVID-19 Vaccine: A Systematic Review. Int. J. Equity Health 2022, 21, 122. [Google Scholar] [CrossRef]
- World Health Organization. Handbook on Health Inequality Monitoring: With a Special Focus on Low-and Middle-Income Countries; World Health Organization: Geneva, Switzerland, 2013; ISBN 92-4-154863-0. [Google Scholar]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11—Scoping Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: North Adelaide, Australia, 2020. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. PROGRESS-Plus. Available online: https://methods.cochrane.org/equity/projects/evidence-equity/progress-plus (accessed on 12 January 2023).
- The World Bank Group. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 31 January 2023).
- Barry, V.; Dasgupta, S.; Weller, D.L.; Kriss, J.L.; Cadwell, B.L.; Rose, C.; Pingali, C.; Musial, T.; Sharpe, J.D.; Flores, S.A.; et al. Patterns in COVID-19 Vaccination Coverage, by Social Vulnerability and Urbanicity—United States, December 14, 2020–May 1, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Murthy, B.P.; Sterrett, N.; Weller, D.; Zell, E.; Reynolds, L.; Toblin, R.L.; Murthy, N.; Kriss, J.; Rose, C.; Cadwell, B.; et al. Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties—United States, December 14, 2020–April 10, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Qiao, S.; Li, Z.; Zhang, J.; Sun, X.; Garrett, C.; Li, X. Social Capital, Urbanization Level, and COVID-19 Vaccination Uptake in the United States: A National Level Analysis. Vaccines 2022, 10, 625. [Google Scholar] [CrossRef] [PubMed]
- Saelee, R.; Zell, E.; Murthy, B.P.; Castro-Roman, P.; Fast, H.; Meng, L.; Shaw, L.; Gibbs-Scharf, L.; Chorba, T.; Harris, L.Q.; et al. Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties—United States, December 14, 2020–January 31, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Tessier, E.; Rai, Y.; Clarke, E.; Lakhani, A.; Tsang, C.; Makwana, A.; Heard, H.; Rickeard, T.; Lakhani, S.; Roy, P.; et al. Characteristics Associated with COVID-19 Vaccine Uptake among Adults Aged 50 Years and above in England (8 December 2020–17 May 2021): A Population-Level Observational Study. BMJ Open 2022, 12, e055278. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xu, R.; Qu, S.; Schwartz, M.; Adams, A.; Chen, X. Health Inequities in COVID-19 Vaccination among the Elderly: Case of Connecticut. J. Infect. Public Health 2021, 14, 1563–1565. [Google Scholar] [CrossRef] [PubMed]
- Spetz, M.; Lundberg, L.; Nwaru, C.; Li, H.; Santosa, A.; Leach, S.; Gisslén, M.; Hammar, N.; Rosvall, M.; Nyberg, F. The Social Patterning of Covid-19 Vaccine Uptake in Older Adults: A Register-Based Cross-Sectional Study in Sweden. Lancet Reg. Health Eur. 2022, 15, 100331. [Google Scholar] [CrossRef]
- Khatatbeh, M.; Albalas, S.; Khatatbeh, H.; Momani, W.; Melhem, O.; Al Omari, O.; Tarhini, Z.; A’aqoulah, A.; Al-Jubouri, M.; Nashwan, A.J.; et al. Children’s Rates of COVID-19 Vaccination as Reported by Parents, Vaccine Hesitancy, and Determinants of COVID-19 Vaccine Uptake among Children: A Multi-Country Study from the Eastern Mediterranean Region. BMC Public Health 2022, 22, 1375. [Google Scholar] [CrossRef]
- Efendi, D.; Rifani, S.R.; Milanti, A.; Efendi, F.; Wong, C.L.; Rustina, Y.; Wanda, D.; Sari, D.; Fabanjo, I.J.; De Fretes, E.D.; et al. The Role of Knowledge, Attitude, Confidence, and Sociodemographic Factors in COVID-19 Vaccination Adherence among Adolescents in Indonesia: A Nationwide Survey. Vaccines 2022, 10, 1489. [Google Scholar] [CrossRef]
- Gray, A.; Fisher, C.B. Determinants of COVID-19 Vaccine Uptake in Adolescents 12–17 Years Old: Examining Pediatric Vaccine Hesitancy among Racially Diverse Parents in the United States. Front. Public Health 2022, 10, 844310. [Google Scholar] [CrossRef]
- Murthy, N.C.; Zell, E.; Fast, H.E.; Murthy, B.P.; Meng, L.; Saelee, R.; Vogt, T.; Chatham-Stephens, K.; Ottis, C.; Shaw, L.; et al. Disparities in First Dose COVID-19 Vaccination Coverage among Children 5–11 Years of Age, United States. Emerg. Infect. Dis. 2022, 28, 986–989. [Google Scholar] [CrossRef]
- Yan, Y.-Y.; Wang, H.-T.; Fan, T.-Y.; Sun, X.-J.; Du, Z.-H.; Sun, X.-M. Vaccination Coverage among COVID-19 Prevention and Control Management Teams at Primary Healthcare Facilities in China and Their Attitudes towards COVID-19 Vaccine: A Cross-Sectional Online Survey. BMJ Open 2022, 12, e056345. [Google Scholar] [CrossRef] [PubMed]
- Elkhayat, M.R.; Hashem, M.K.; Helal, A.T.; Shaaban, O.M.; Ibrahim, A.K.; Meshref, T.S.; Elkhayat, H.; Moustafa, M.; Mohammed, M.N.A.; Ezzeldin, A.M.; et al. Determinants of Obtaining COVID-19 Vaccination among Health Care Workers with Access to Free COVID-19 Vaccination: A Cross-Sectional Study. Vaccines 2022, 10, 39. [Google Scholar] [CrossRef]
- Nicolo, M.; Kawaguchi, E.S.; Ghanem-Uzqueda, A.; Kim, A.E.; Soto, D.; Deva, S.; Shanker, K.; Rogers, C.; Lee, R.; Casagrande, Y.; et al. Characteristics Associated with COVID-19 Vaccination Status among Staff and Faculty of a Large, Diverse University in Los Angeles: The Trojan Pandemic Response Initiative. Prev. Med. Rep. 2022, 27, 101802. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.H.; Irvine, S.; Epstein, R.; Allen, J.D.; Corlin, L. Prior COVID-19 Infection, Mental Health, Food and Financial Insecurity, and Association with COVID-19 Vaccination Coverage and Intent among College-Aged Young Adults, US, 2021. Prev. Chronic Dis. 2021, 18, 210260. [Google Scholar] [CrossRef]
- Shapiro, G.; Bez, M.; Talmy, T.; Shakargy, J.D.; Furer, A.; Karp, E.; Segal, D. SARS-CoV-2 Vaccine Acceptance Disparity among Israeli Defense Forces Personnel. Mil. Med. 2022, 187, 279. [Google Scholar] [CrossRef]
- Jones, A.; Wallis, D. Using the Health Belief Model to Identify Predictors of COVID-19 Vaccine Acceptance among a Sample of Pregnant Women in the U.S.: A Cross-Sectional Survey. Vaccines 2022, 10, 842. [Google Scholar] [CrossRef]
- Cheng, J.Y.J.; Loong, S.S.E.; Ho, C.E.S.M.; Ng, K.J.; Ng, M.M.Q.; Chee, R.C.H.; Chin, T.X.L.; Fong, F.J.Y.; Goh, S.L.G.; Venkatesh, K.N.S.; et al. Knowledge, Attitudes, and Practices of COVID-19 Vaccination among Adults in Singapore: A Cross-Sectional Study. Am. J. Trop. Med. Hyg. 2022, 107, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Kriss, J.L.; Hung, M.-C.; Srivastav, A.; Black, C.L.; Lindley, M.C.; Lee, J.T.; Koppaka, R.; Tsai, Y.; Lu, P.-J.; Yankey, D.; et al. COVID-19 Vaccination Coverage, by Race and Ethnicity—National Immunization Survey Adult COVID Module, United States, December 2020–November 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 757–763. [Google Scholar] [CrossRef]
- Baker, L.; Phillips, B.; Faherty, L.J.; Ringel, J.S.; Kranz, A.M. Racial and Ethnic Disparities in COVID-19 Booster Uptake: Study Examines Racial and Ethnic Disparities in the Uptake of COVID-19 Booster Shots. Health Aff. 2022, 41, 1202–1207. [Google Scholar] [CrossRef]
- DiRago, N.V.; Li, M.; Tom, T.; Schupmann, W.; Carrillo, Y.; Carey, C.M.; Gaddis, S.M. COVID-19 Vaccine Rollouts and the Reproduction of Urban Spatial Inequality: Disparities Within Large US Cities in March and April 2021 by Racial/Ethnic and Socioeconomic Composition. J. Urban Health 2022, 99, 191–207. [Google Scholar] [CrossRef]
- Diesel, J.; Sterrett, N.; Dasgupta, S.; Kriss, J.L.; Barry, V.; Vanden Esschert, K.; Whiteman, A.; Cadwell, B.L.; Weller, D.; Qualters, J.R.; et al. COVID-19 Vaccination Coverage among Adults—United States, December 14, 2020–May 22, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Ryerson, A.B.; Rice, C.E.; Hung, M.-C.; Patel, S.A.; Weeks, J.D.; Kriss, J.L.; Peacock, G.; Lu, P.-J.; Asif, A.F.; Jackson, H.L.; et al. Disparities in COVID-19 Vaccination Status, Intent, and Perceived Access for Noninstitutionalized Adults, by Disability Status—National Immunization Survey Adult COVID Module, United States, May 30–June 26, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Low, A.; Wright, C.; Platt, J.; Chang, C.; Mantell, J.E.; Romero, E.; Hoos, D.; Mannheimer, S.; Greenleaf, A.; Castor, D.; et al. COVID-19 Vaccine Uptake and Factors Associated with Being Unvaccinated among Lesbian, Gay, Bisexual, Transgender, Queer, and Other Sexual Identities (LGBTQ+) New Yorkers. Open Forum Infect. Dis. 2022, 9, ofac260. [Google Scholar] [CrossRef] [PubMed]
- McNaghten, A.D.; Brewer, N.T.; Hung, M.-C.; Lu, P.-J.; Daskalakis, D.; Abad, N.; Kriss, J.; Black, C.; Wilhelm, E.; Lee, J.T.; et al. COVID-19 Vaccination Coverage and Vaccine Confidence by Sexual Orientation and Gender Identity—United States, August 29–October 30, 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 171–176. [Google Scholar] [CrossRef]
- Heidari, S.; Ahumada, C.; Kurbanova, Z. Towards the Real-Time Inclusion of Sex- and Age-Disaggregated Data in Pandemic Responses. BMJ Glob. Health 2020, 5, e003848. [Google Scholar] [CrossRef]
- Yaya, S.; Yeboah, H.; Charles, C.H.; Otu, A.; Labonte, R. Ethnic and Racial Disparities in COVID-19-Related Deaths: Counting the Trees, Hiding the Forest. BMJ Glob. Health 2020, 5, e002913. [Google Scholar] [CrossRef]
- Kocher, K.; Delot-Vilain, A.; Spencer, D.; LoTempio, J.; Délot, E.C. Paucity and Disparity of Publicly Available Sex-Disaggregated Data for the COVID-19 Epidemic Hamper Evidence-Based Decision-Making. Arch. Sex Behav. 2021, 50, 407–426. [Google Scholar] [CrossRef]
- Pareek, M.; Bangash, M.N.; Pareek, N.; Pan, D.; Sze, S.; Minhas, J.S.; Hanif, W.; Khunti, K. Ethnicity and COVID-19: An Urgent Public Health Research Priority. Lancet 2020, 395, 1421–1422. [Google Scholar] [CrossRef]
- Hosseinpoor, A.R.; Bergen, N. Area-Based Units of Analysis for Strengthening Health Inequality Monitoring. Bull. World Health Organ. 2016, 94, 856–858. [Google Scholar] [CrossRef]
- Dolman, A.J.; Fraser, T.; Panagopoulos, C.; Aldrich, D.P.; Kim, D. Opposing Views: Associations of Political Polarization, Political Party Affiliation, and Social Trust with COVID-19 Vaccination Intent and Receipt. J. Public Health 2022, fdab401. [Google Scholar] [CrossRef]
- Machida, M.; Kikuchi, H.; Kojima, T.; Nakamura, I.; Saito, R.; Nakaya, T.; Hanibuchi, T.; Takamiya, T.; Odagiri, Y.; Fukushima, N.; et al. Individual-Level Social Capital and COVID-19 Vaccine Hesitancy in Japan: A Cross-Sectional Study. Hum. Vaccines Immunother. 2022, 18, 2086773. [Google Scholar] [CrossRef]
- World Health Organization. Explorations of Inequality: Childhood Immunization; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Inequality Monitoring in Immunization: A Step-by-Step Manual; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International Estimates of Intended Uptake and Refusal of COVID-19 Vaccines: A Rapid Systematic Review and Meta-Analysis of Large Nationally Representative Samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef] [PubMed]
- Nehal, K.R.; Steendam, L.M.; Campos Ponce, M.; van der Hoeven, M.; Smit, G.S.A. Worldwide Vaccination Willingness for COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2021, 9, 1071. [Google Scholar] [CrossRef] [PubMed]
- Liao, Q.; Cowling, B.J.; Lam, W.W.T.; Fielding, R. Factors Affecting Intention to Receive and Self-Reported Receipt of 2009 Pandemic (H1N1) Vaccine in Hong Kong: A Longitudinal Study. PLoS ONE 2011, 6, e17713. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Country Income Group Classification | Countries |
|---|---|
| High income | Australia (2 articles); Canada (6 articles); Czech Republic (1 article); France (2 articles); Germany (1 article); Greece (2 articles); Hong Kong (5 articles); Hungary (2 articles); Israel (7 articles); Italy (2 articles); Japan a (2 articles); Kuwait a (1 article); Latvia (1 article); Netherlands (1 article); New Zealand (1 article); Norway a (1 article); Qatar a (1 article); Romania (1 article); Saudi Arabia a (3 articles); Singapore (2 articles); Slovakia a (1 article); Spain (1 article); Sweden a (4 articles); United Arab Emirates a (2 articles); United Kingdom a (15 articles); United States of America a (86 articles) |
| Upper-middle income | Belarus (1 article); Brazil (2 articles); China (3 articles); Guatemala a (1 article); Iraq a (1 article); Jordan a (1 article); Kazakhstan a (1 article); Mexico a (3 articles); Peru (1 article); Serbia (1 article); Thailand (1 article) |
| Lower-middle income | Bangladesh (1 article); Egypt (1 article); India a (3 articles); Indonesia (1 article); Lebanon a (1 article); Pakistan (1 article) |
| Low income | Ethiopia (1 article); Guinea (1 article); Malawi (2 articles) |
| Not classified | Palestine a (3 articles) |
| Dimension of Inequality | Number of Articles (% of Total) a | Illustrative Examples of Measurement Criteria b |
|---|---|---|
| Age | 127 (76%) | years; parental age; above or below median age of population |
| Race, ethnicity, cultural group, language, nationality or country of birth | 117 (70%) | White, Black, Hispanic, Asian or Other (applicable to studies based in the United States); language at home; national or foreigner |
| Sex or gender | 103 (62%) | male or female; transgender or non-binary (yes/no) |
| Occupation- or employment-related factor | 81 (49%) | employed or unemployed; employment in healthcare industry (yes/no); essential worker, non-essential worker, or non-working status; public or private sector employee; military ranking; profession |
| Education level | 76 (46%) | years of schooling; highest level of schooling completed; highest qualification |
| Subnational region or area | 68 (41%) | state/province; region; municipality; census tract; county; health zone |
| Economic status | 68 (41%) | household income; above or below defined poverty line; self-perceived financial status; level of difficulty covering household expenses |
| Place of residence | 39 (23%) | urban or rural; metro or non-metro; urban, rural or camp; population size of zip code |
| Vulnerability, deprivation or poverty index | 38 (23%) | Social Vulnerability Index (applicable to studies based in the United States); Index of Multiple Deprivation (applicable to studies based in the United Kingdom); Human Development Index; Multi-Dimensional Poverty Index |
| Marital status | 30 (18%) | single, married, cohabitating, divorced, widowed; living with partner (yes/no) |
| Family size or composition | 27 (16%) | number of children; household size; elderly living with family (yes/no); children living in household (yes/no); living alone (yes/no) |
| Health insurance | 27 (16%) | insured or uninsured status; private or public health insurance type |
| Disability status | 10 (6%) | self-reported living with a disability (yes/no); extent of daily activity limitation |
| Religion | 8 (5%) | religious affiliation (e.g., Christian, Buddhist, Hindu, Jewish, Muslim, Sikh, other, none) |
| Housing type or characteristic | 7 (4%) | homeless (yes/no); house owned, private rented, social rented, other; type of housing: mobile, detached house, attached house, multiunit apartment, etc. |
| Migration status | 5 (3%) | citizen, landed immigrant, refugee, temporary/other; migration history (yes/no) |
| Social capital | 3 (2%) | trust in others; civic participation; social capital index |
| Sexual orientation | 3 (2%) | bisexual, gay/lesbian, heterosexual |
| Other: food security, incarceration status, income inequality, car ownership, computer ownership, school type | 1–2 each |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© World Health Organization 2023. Licensee MDPI. This article is distributed under the terms of the Creative Commons Attribution IGO License. (https://creativecommons.org/licenses/by/3.0/igo/) which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted. This notice should be preserved along with the article’s original URL.
Share and Cite
Bergen, N.; Johns, N.E.; Chang Blanc, D.; Hosseinpoor, A.R. Within-Country Inequality in COVID-19 Vaccination Coverage: A Scoping Review of Academic Literature. Vaccines 2023, 11, 517. https://doi.org/10.3390/vaccines11030517
Bergen N, Johns NE, Chang Blanc D, Hosseinpoor AR. Within-Country Inequality in COVID-19 Vaccination Coverage: A Scoping Review of Academic Literature. Vaccines. 2023; 11(3):517. https://doi.org/10.3390/vaccines11030517
Chicago/Turabian StyleBergen, Nicole, Nicole E. Johns, Diana Chang Blanc, and Ahmad Reza Hosseinpoor. 2023. "Within-Country Inequality in COVID-19 Vaccination Coverage: A Scoping Review of Academic Literature" Vaccines 11, no. 3: 517. https://doi.org/10.3390/vaccines11030517
APA StyleBergen, N., Johns, N. E., Chang Blanc, D., & Hosseinpoor, A. R. (2023). Within-Country Inequality in COVID-19 Vaccination Coverage: A Scoping Review of Academic Literature. Vaccines, 11(3), 517. https://doi.org/10.3390/vaccines11030517