
Immunogenicity and Safety of Anti-SARS-CoV-2 mRNA Vaccines in a Cohort of Patients with Hereditary Angioedema

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Disease Activity Assessment
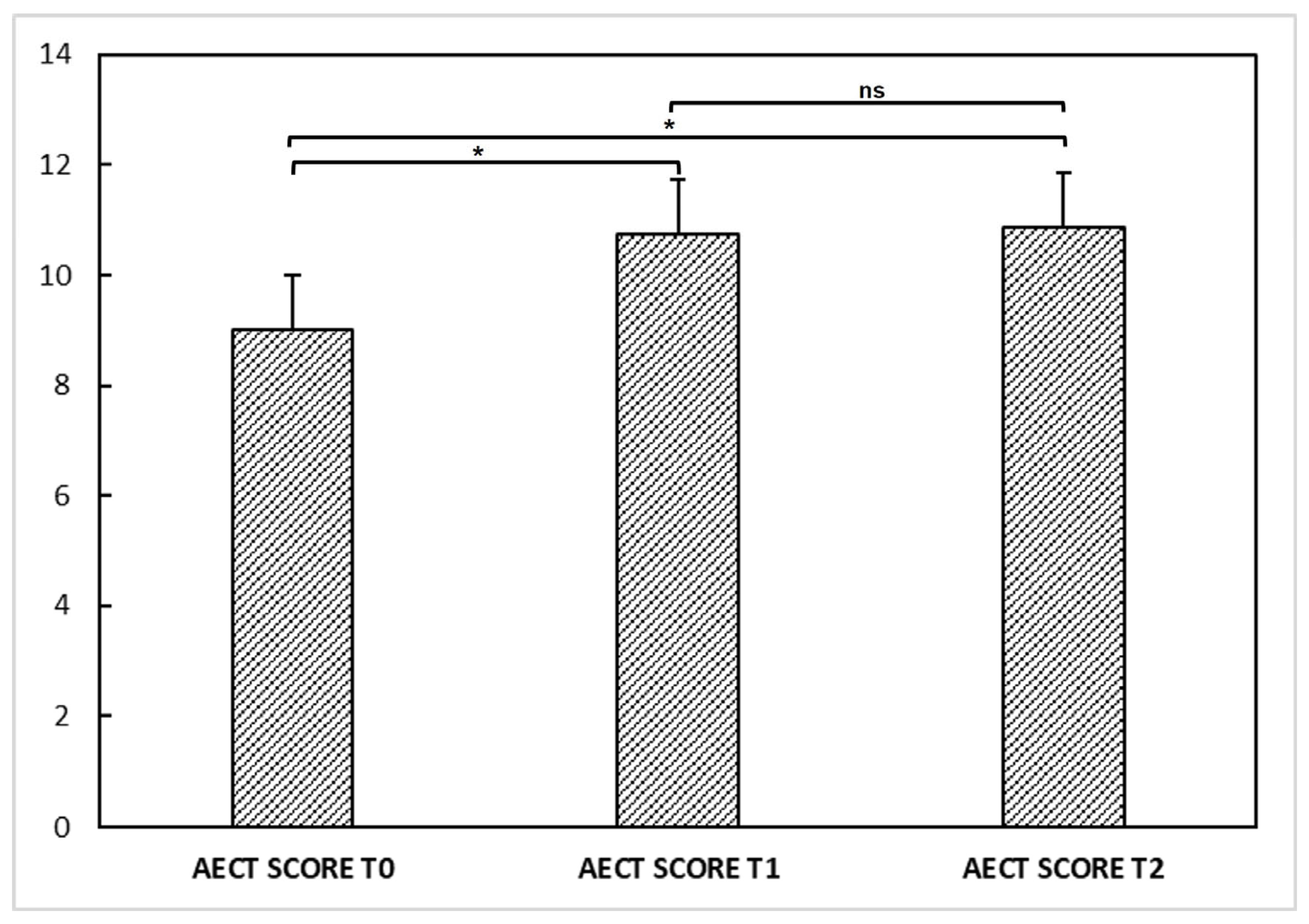
2.2.1. Angioedema Control Test
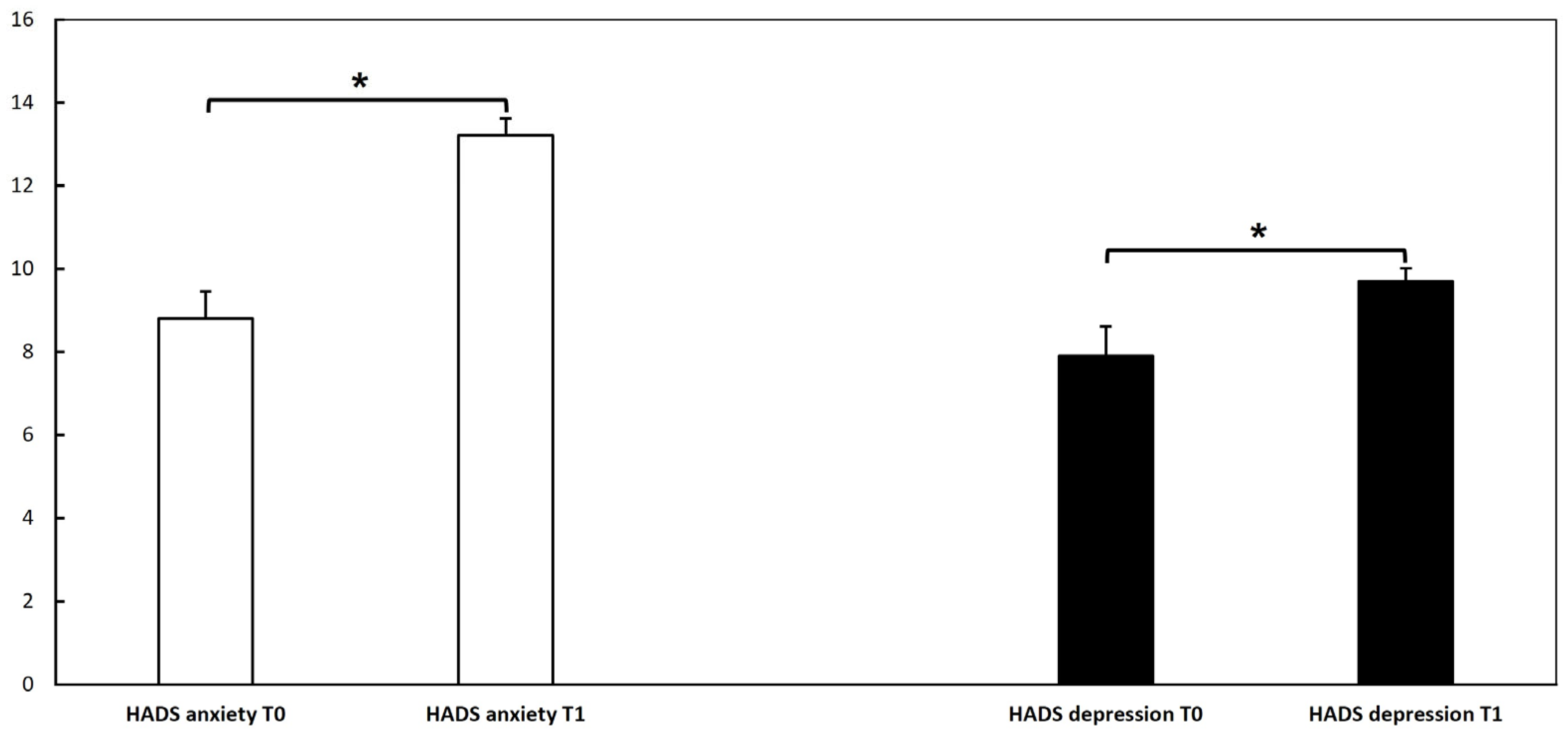
2.2.2. The Hospital Anxiety and Depression Scale
2.2.3. Severity Score
2.3. Blood Sample Collection
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Clinical Evaluation
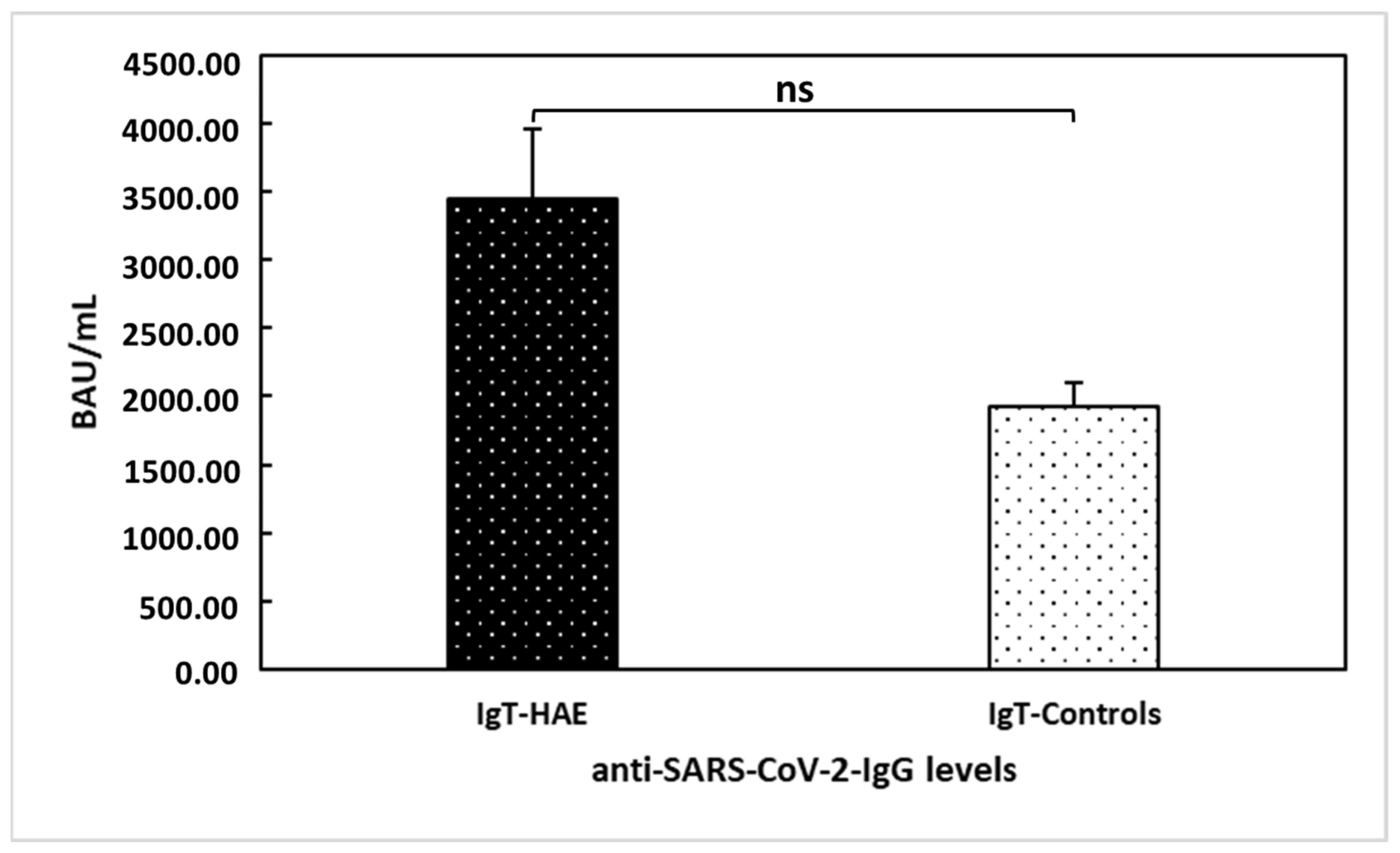
3.3. Anti-SARS-CoV-2 Vaccine Immunogenicity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lang, D.M.; Aberer, W.; Bernstein, J.A.; Chng, H.H.; Grumach, A.S.; Hide, M.; Maurer, M.; Weber, R.; Zuraw, B. International consensus on hereditary and acquired angioedema. Ann. Allergy Asthma Immunol. 2012, 109, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Busse, P.J.; Christiansen, S.C.; Riedl, M.A.; Banerji, A.; Bernstein, J.A.; Castaldo, A.J.; Craig, T.; Davis-Lorton, M.; Frank, M.M.; Li, H.H.; et al. US HAEA Medical Advisory Board 2020 Guidelines for the Management of Hereditary Angioedema. J. Allergy Clin. Immunol. Pract. 2021, 9, 132–150.E3. [Google Scholar] [CrossRef]
- Cicardi, M.; Zuraw, B.L. Angioedema Due to Bradykinin Dysregulation. J. Allergy Clin. Immunol. Pract. 2018, 6, 1132–1141. [Google Scholar] [CrossRef]
- Santacroce, R.; D’Andrea, G.; Maffione, A.B.; Margaglione, M.; d’Apolito, M. The Genetics of Hereditary Angioedema: A Review. J. Clin. Med. 2021, 10, 2023. [Google Scholar] [CrossRef]
- Longhurst, H.J.; Bork, K. Hereditary angioedema: An update on causes, manifestations and treatment. Br. J. Hosp. Med. 2019, 80, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Bova, M.; De Feo, G.; Parente, R.; De Pasquale, T.; Gravante, C.; Pucci, S.; Nettis, E.; Triggiani, M. Hereditary and Acquired Angioedema: Heterogeneity of Pathogenesis and Clinical Phenotypes. Int. Arch. Allergy Immunol. 2018, 175, 126–135. [Google Scholar] [CrossRef]
- Ariano, A.; D’Apolito, M.; Bova, M.; Bellanti, F.; Loffredo, S.; D’Andrea, G.; Intrieri, M.; Petraroli, A.; Maffione, A.B.; Spadaro, G.; et al. A myoferlin gain-of-function variant associates with a new type of hereditary angioedema. Allergy 2020, 75, 2989–2992. [Google Scholar] [CrossRef]
- Bork, K.; Wulff, K.; Möhl, B.S.; Steinmüller-Magin, L.; Witzke, G.; Hardt, J.; Meinke, P. Novel hereditary angioedema linked with a heparan sulfate 3-O-sulfotransferase 6 gene mutation. J. Allergy Clin. Immunol. 2021, 148, 1041–1048. [Google Scholar] [CrossRef] [PubMed]
- Mormile, I.; Bova, M.; Cocchiaro, A.; Rossi, F.W.; Granata, F.; Spadaro, G.; de Paulis, A.; Petraroli, A. Clinical features and burden of genital attacks in hereditary angioedema. J. Allergy Clin. Immunol. Pract. 2022, 10, 643–644. [Google Scholar] [CrossRef]
- Mormile, I.; Cocchiaro, A.; Bova, M.; Loffredo, S.; de Paulis, A.; Spadaro, G.; Petraroli, A. Gastrointestinal manifestations of angioedema: A potential area of misdiagnosis. Eur. J. Gastroenterol. Hepatol. 2021, 33, 787–793. [Google Scholar] [CrossRef]
- Bork, K.; Hardt, J.; Witzke, G. Fatal laryngeal attacks and mortality in hereditary angioedema due to C1-INH deficiency. J. Allergy Clin. Immunol. 2012, 130, 692–697. [Google Scholar] [CrossRef]
- McNeil, M.M.; Weintraub, E.S.; Duffy, J.; Sukumaran, L.; Jacobsen, S.J.; Klein, N.P.; Hambidge, S.J.; Lee, G.M.; Jackson, L.A.; Irving, S.A.; et al. Risk of anaphylaxis after vaccination in children and adults. J. Allergy Clin. Immunol. 2016, 137, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Worm, M.; Bauer, A.; Wedi, B.; Treudler, R.; Pfuetzner, W.; Brockow, K.; Buhl, T.; Zuberbier, T.; Fluhr, J.; Wurpts, G.; et al. Practical recommendations for the allergological risk assessment of the COVID-19 vaccination—A harmonized statement of allergy centers in Germany. Allergol. Sel. 2021, 5, 72–76. [Google Scholar] [CrossRef]
- Kleine-Tebbe, J.; Klimek, L.; Hamelmann, E.; Pfaar, O.; Taube, C.; Wagenmann, M.; Werfel, T.; Worm, M. Severe allergic reactions to the COVID-19 vaccine—Statement and practical consequences. Allergol. Sel. 2021, 5, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Mormile, I.; Petraroli, A.; Loffredo, S.; Rossi, F.W.; Mormile, M.; Del Mastro, A.; Spadaro, G.; de Paulis, A.; Bova, M. Episodic Angioedema with Hypereosinophilia (Gleich’s Syndrome): A Case Report and Extensive Review of the Literature. J. Clin. Med. 2021, 10, 1442. [Google Scholar] [CrossRef] [PubMed]
- Weller, K.; Donoso, T.; Magerl, M.; Aygören-Pürsün, E.; Staubach, P.; Martinez-Saguer, I.; Hawro, T.; Altrichter, S.; Krause, K.; Siebenhaar, F.; et al. Validation of the Angioedema Control Test (AECT)—A Patient-Reported Outcome Instrument for Assessing Angioedema Control. J. Allergy Clin. Immunol. Pract. 2020, 8, 2050–2057.e4. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Bygum, A.; Fagerberg, C.R.; Ponard, D.; Monnier, N.; Lunardi, J.; Drouet, C. Mutational spectrum and phenotypes in Danish families with hereditary angioedema because of C1 inhibitor deficiency. Allergy 2011, 66, 76–84. [Google Scholar] [CrossRef]
- Monami, M.; Gori, D.; Guaraldi, F.; Montalti, M.; Nreu, B.; Burioni, R.; Mannucci, E. COVID-19 Vaccine Hesitancy and Early Adverse Events Reported in a Cohort of 7,881 Italian Physicians. Ann. Ig. 2022, 34, 344–357. [Google Scholar] [CrossRef]
- Mormile, I.; Della Casa, F.; Petraroli, A.; Furno, A.; Granata, F.; Portella, G.; Rossi, F.W.; de Paulis, A. Immunogenicity and Safety of mRNA Anti-SARS-CoV-2 Vaccines in Patients with Systemic Lupus Erythematosus. Vaccines 2022, 10, 1221. [Google Scholar] [CrossRef]
- Veronez, C.L.; Christiansen, S.C.; Smith, T.D.; Riedl, M.A.; Zuraw, B.L. COVID-19 and hereditary angioedema: Incidence, outcomes, and mechanistic implications. Allergy Asthma Proc. 2021, 42, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Roche, J.A.; Roche, R. A hypothesized role for dysregulated bradykinin signaling in COVID-19 respiratory complications. FASEB J. 2020, 34, 7265–7269. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Risitano, A.M.; Mastellos, D.C.; Huber-Lang, M.; Yancopoulou, D.; Garlanda, C.; Ciceri, F.; Lambris, J.D. Complement as a target in COVID-19? Nat. Rev. Immunol. 2020, 20, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Van de Veerdonk, F.L.; Netea, M.G.; van Deuren, M.; van der Meer, J.W.; de Mast, Q.; Brüggemann, R.J.; van der Hoeven, H. Kallikrein-kinin blockade in patients with COVID-19 to prevent acute respiratory distress syndrome. Elife 2020, 9, e57555. [Google Scholar] [CrossRef]
- Brogi, S.; Calderone, V. Off-target ACE2 ligands: Possible therapeutic option for COVID-19? Br. J. Clin. Pharmacol. 2020, 86, 1178–1179. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus infections and immune responses. J. Med. Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Mastellos, D.C.; Ricklin, D.; Lambris, J.D. Clinical promise of next-generation complement therapeutics. Nat. Rev. Drug Discov. 2019, 18, 707–729. [Google Scholar] [CrossRef]
- Gralinski, L.E.; Sheahan, T.P.; Morrison, T.E.; Menachery, V.D.; Jensen, K.; Leist, S.R.; Whitmore, A.; Heise, M.T.; Baric, R.S. Complement Activation Contributes to Severe Acute Respiratory Syndrome Coronavirus Pathogenesis. mBio 2018, 9, e01753-18. [Google Scholar] [CrossRef]
- Can Bostan, O.; Tuncay, G.; Damadoglu, E.; Karakaya, G.; Kalyoncu, A.F. Effect of COVID-19 on hereditary angioedema activity and quality of life. Allergy Asthma Proc. 2021, 42, 403–408. [Google Scholar] [CrossRef]
- Eyice Karabacak, D.; Demir, S.; Yeğit, O.O.; Can, A.; Terzioğlu, K.; Ünal, D.; Olgaç, M.; Coşkun, R.; Çolakoğlu, B.; Büyüköztürk, S.; et al. Impact of anxiety, stress and depression related to COVID-19 pandemic on the course of hereditary angioedema with C1-inhibitor deficiency. Allergy 2021, 76, 2535–2543. [Google Scholar] [CrossRef] [PubMed]
- Oztop, N.; Demir, S.; Toprak, I.D.; Unal, D.; Gelincik, A. Positive perception of COVID-19 vaccination in HAE: No significant impact of vaccination on disease course. Allergy Asthma Proc. 2022, 43, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Savarese, L.; Mormile, I.; Bova, M.; Petraroli, A.; Maiello, A.; Spadaro, G.; Freda, M.F. Psychology and hereditary angioedema: A systematic review. Allergy Asthma Proc. 2021, 42, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Savarese, L.; Bova, M.; Maiello, A.; Petraroli, A.; Mormile, I.; Cancian, M.; Senter, R.; Zanichelli, A.; Spadaro, G.; Freda, M.F. Psychological processes in the experience of hereditary angioedema in adult patients: An observational study. Orphanet. J. Rare Dis. 2021, 16, 23. [Google Scholar] [CrossRef]
- Gambardella, J.; Sorriento, D.; Bova, M.; Rusciano, M.; Loffredo, S.; Wang, X.; Petraroli, A.; Carucci, L.; Mormile, I.; Oliveti, M.; et al. Role of Endothelial G Protein-Coupled Receptor Kinase 2 in Angioedema. Hypertension 2020, 76, 1625–1636. [Google Scholar] [CrossRef]
- Cesoni Marcelli, A.; Loffredo, S.; Petraroli, A.; Carucci, L.; Mormile, I.; Ferrara, A.L.; Spadaro, G.; Genovese, A.; Bova, M. Nailfold Videocapillaroscopy Findings in Bradykinin-Mediated Angioedema. J. Investig. Allergol. Clin. Immunol. 2021, 31, 404–416. [Google Scholar] [CrossRef]
- Maurer, M.; Magerl, M.; Ansotegui, I.; Aygoren-Pürsün, E.; Betschel, S.; Bork, K.; Bowen, T.; Balle Boysen, H.; Farkas, H.; Grumach, A.S.; et al. The international WAO/EAACI guideline for the management of hereditary angioedema-The 2017 revision and update. Allergy 2018, 73, 1575–1596. [Google Scholar] [CrossRef]
- Fijen, L.M.; Levi, M.; Cohn, D.M. COVID-19 vaccination and the risk of swellings in patients with hereditary angioedema. J. Allergy Clin. Immunol. Pract. 2021, 9, 4156–4158. [Google Scholar] [CrossRef]
- Kannemeier, C.; Shibamiya, A.; Nakazawa, F.; Trusheim, H.; Ruppert, C.; Markart, P.; Song, Y.; Tzima, E.; Kennerknecht, E.; Niepmann, M.; et al. Extracellular RNA constitutes a natural procoagulant cofactor in blood coagulation. Proc. Natl. Acad. Sci. USA 2007, 104, 6388–6393. [Google Scholar] [CrossRef]
- Wu, M.A.; Casella, F.; Perego, F.; Suffritti, C.; Afifi Afifi, N.; Tobaldini, E.; Zanichelli, A.; Cogliati, C.; Montano, N.; Cicardi, M. Hereditary angioedema: Assessing the hypothesis for underlying autonomic dysfunction. PLoS ONE 2017, 12, e0187110. [Google Scholar] [CrossRef]
- Banerji, A.; Davis, K.H.; Brown, T.M.; Hollis, K.; Hunter, S.M.; Long, J.; Jain, G.; Devercelli, G. Patient-reported burden of hereditary angioedema: Findings from a patient survey in the United States. Ann. Allergy Asthma Immunol. 2020, 124, 600–607. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | C1-INH-HAE Type 1 | C1-INH-HAE Type 2 | FXII-HAE | MYOF-HAE |
|---|---|---|---|---|
| No. of patients (%) | 23 (74.2%) | 3 (9.7 %) | 2 (6.4 %) | 3 (9.7%) |
| Female gender = 22 (71%) (n, %) | 16 (69.6%) | 1 (33.3%) | 2 (100%) | 3 (100%) |
| Caucasian ethnicity (n, %) | 23 (100%) | 3 (100%) | 2 (100%) | 3 (100%) |
| Age, years (mean, range) | 45.3 ± 19 (18–82) | 57.7 ± 9.1 (51–68) | 49 ± 14.1 (39–59) | 29 ± 16.8 (16–48) |
| Time from diagnosis (years; mean ± SD) | 17.7 ± 14 | 20.3 ± 16 | 6 ± 1.4 | 1 ± 0 |
| Attack frequency (mean/year) | 17/year | 23/year | 0/year * | 1/year |
| Severity score | 7.04 | 6.3 | 0 | 3 |
| LTP (n, %) | 11 (54.6%) | 2 (66.7 %) | - | - |
| Attenuated androgens (n, %) | 6 (45.4%) | 2 (100%) | - | - |
| pdC1-INH (n, %) | 5 (36.4%) | - | - | - |
| Tranexamic acid (n, %) | - | - | - | - |
| Symptom | HAE First Dose n (%) | Italian Subjects First Dose n (%) | HAE Second Dose n (%) | Italian Subjects Second Dose n (%) |
|---|---|---|---|---|
| Pain, itching, paraesthesia (Vaccination site) | 18 (58%) | 3164 (50.7%) | 18 (58%) | 811 (48.5%) |
| Fever | 6 (19.3%) | 285 (4.6%) | 8 (25.8%) | 275 (16.5%) |
| Fatigue | 0 (0%) | 1435 (23.0%) | 6 (19.3%) | 871 (52.1%) |
| Myalgia/arthralgia | 1 (3.2%) | 800 (12.8%) | 8 (25.8%) | 797 (47.7%) |
| Headache | 4 (12.9%) | 1148 (18.4%) | 7 (22.5%) | 650 (38.9%) |
| Nausea and/or vomiting | 2 (6.4%) | 111 (1.8%) | 2 (6.4%) | 34 (2.0%) |
| Diarrhea | 1 (3.2%) | 138 (2.2%) | 0 (0%) | 93 (5.6%) |
| Limb paraesthesia | 1 (3.2%) | 15 (0.2%) | 0 (0%) | 5 (0.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mormile, I.; Gigliotti, M.C.; Petraroli, A.; Cocchiaro, A.; Furno, A.; Granata, F.; Rossi, F.W.; Portella, G.; de Paulis, A. Immunogenicity and Safety of Anti-SARS-CoV-2 mRNA Vaccines in a Cohort of Patients with Hereditary Angioedema. Vaccines 2023, 11, 215. https://doi.org/10.3390/vaccines11020215
Mormile I, Gigliotti MC, Petraroli A, Cocchiaro A, Furno A, Granata F, Rossi FW, Portella G, de Paulis A. Immunogenicity and Safety of Anti-SARS-CoV-2 mRNA Vaccines in a Cohort of Patients with Hereditary Angioedema. Vaccines. 2023; 11(2):215. https://doi.org/10.3390/vaccines11020215
Chicago/Turabian StyleMormile, Ilaria, Maria Celeste Gigliotti, Angelica Petraroli, Antonio Cocchiaro, Alessandro Furno, Francescopaolo Granata, Francesca Wanda Rossi, Giuseppe Portella, and Amato de Paulis. 2023. "Immunogenicity and Safety of Anti-SARS-CoV-2 mRNA Vaccines in a Cohort of Patients with Hereditary Angioedema" Vaccines 11, no. 2: 215. https://doi.org/10.3390/vaccines11020215
APA StyleMormile, I., Gigliotti, M. C., Petraroli, A., Cocchiaro, A., Furno, A., Granata, F., Rossi, F. W., Portella, G., & de Paulis, A. (2023). Immunogenicity and Safety of Anti-SARS-CoV-2 mRNA Vaccines in a Cohort of Patients with Hereditary Angioedema. Vaccines, 11(2), 215. https://doi.org/10.3390/vaccines11020215