
Concentrations, Number of Doses, and Formulations of Aluminium Adjuvants in Vaccines: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Clinical Trials

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Trials for This Review
2.2. Types of Outcomes
2.3. Search Methods for Identification of Trials
2.4. Data Collection
2.5. Measures of Treatment Effect and Data Synthesis
2.5.1. Meta-Analysis
2.5.2. Trial Sequential Analysis
2.5.3. Subgroup Analysis and Sensitivity Analyses
2.5.4. Summary of Findings and Assessment of the Certainty of the Evidence
2.6. Patient and Public Involvement
3. Results
3.1. Results of the Search
3.2. Characteristics of Included Trials
3.2.1. Interventions and Comparisons
Types of Aluminium Adjuvants
3.2.2. Vaccines against Different Viruses, Bacteria, Toxins, or Diseases
3.2.3. Number of Vaccinations
3.2.4. Aluminium Concentrations
3.2.5. Control Groups
3.2.6. Follow-Up
3.2.7. Sponsorship of Trials
3.2.8. Risk of Bias
3.3. Effects of Interventions
3.3.1. Comparison 1: Higher vs. Lower Concentration of Aluminium Adjuvants
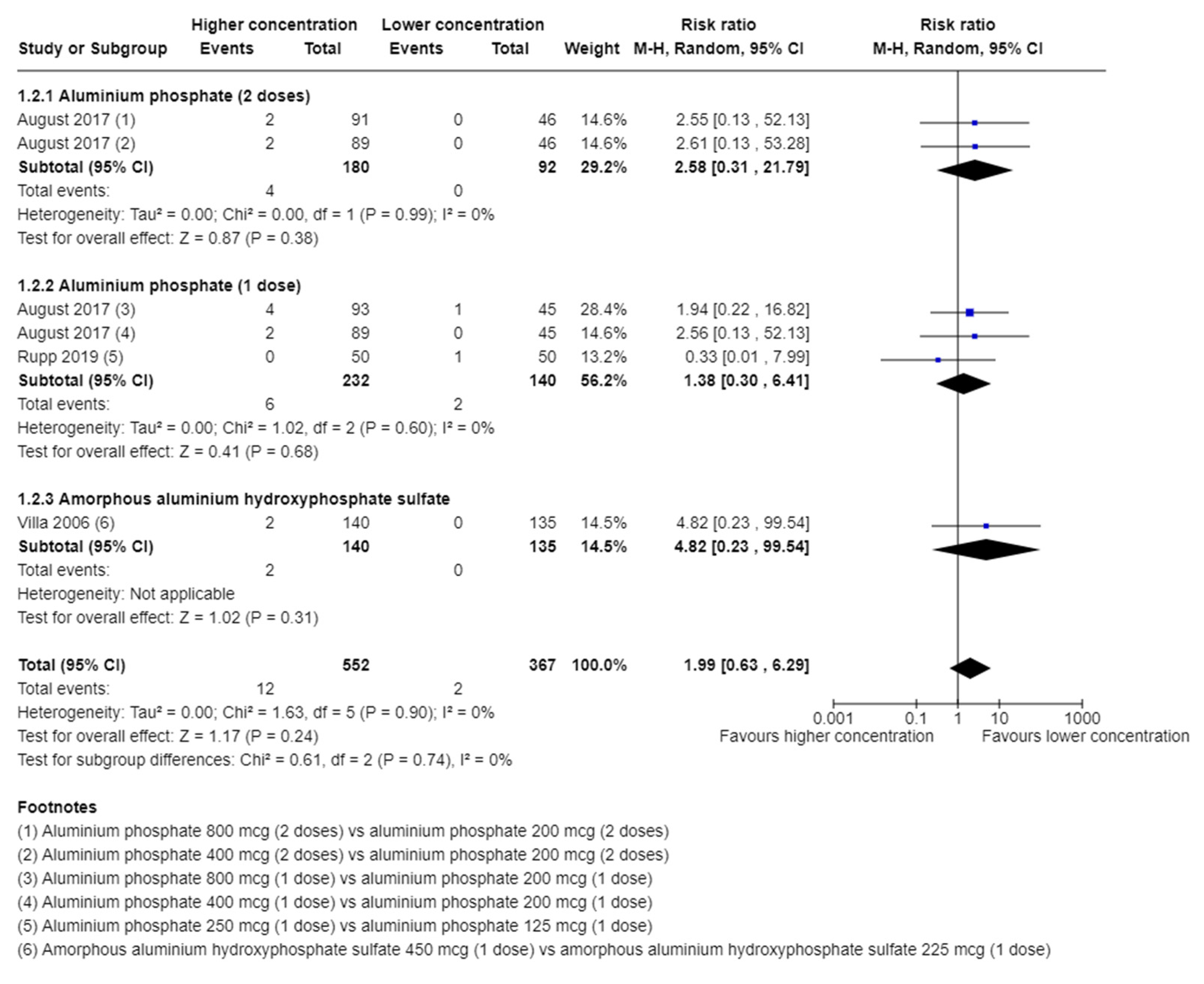
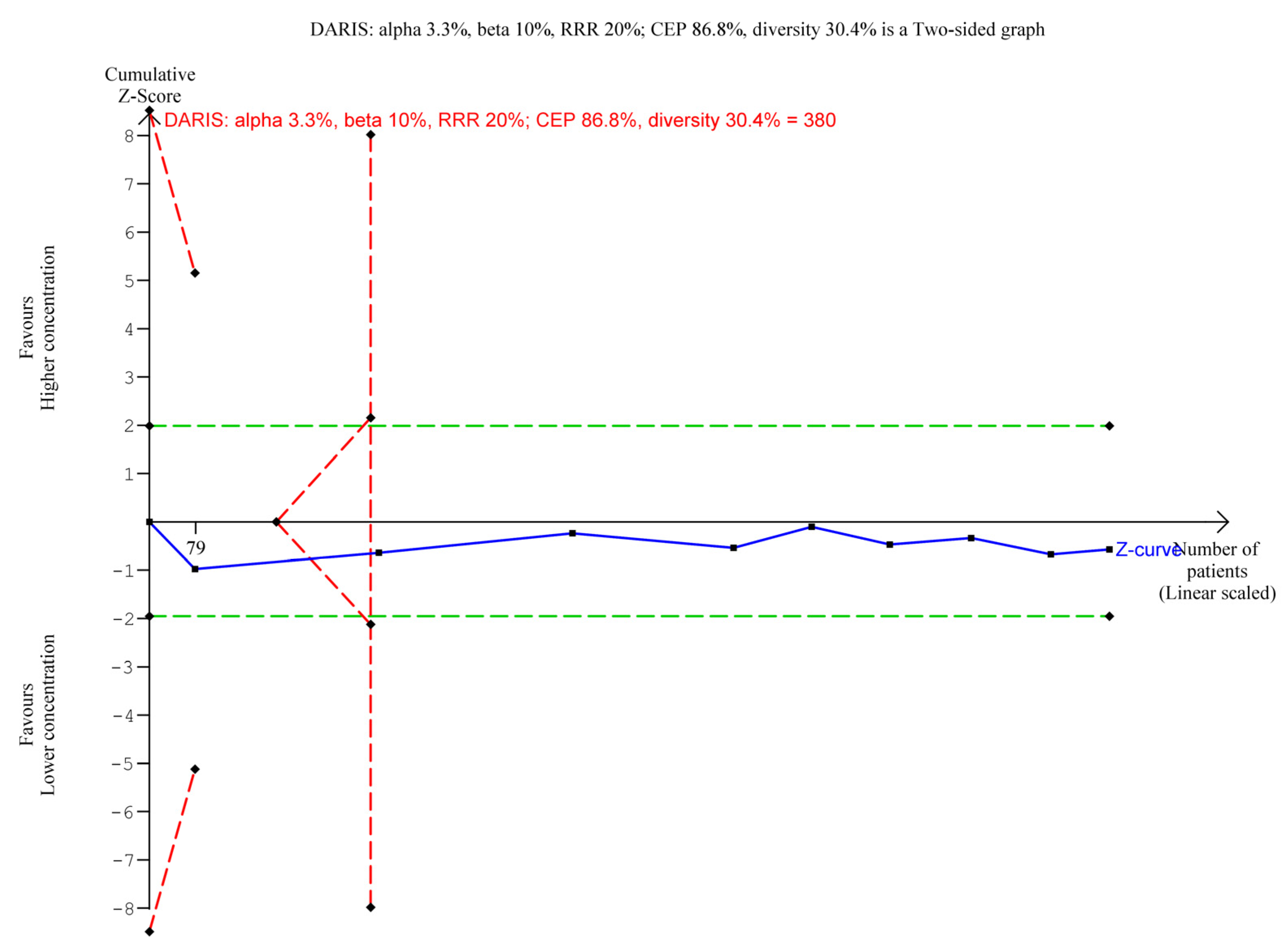
Serious Adverse Events
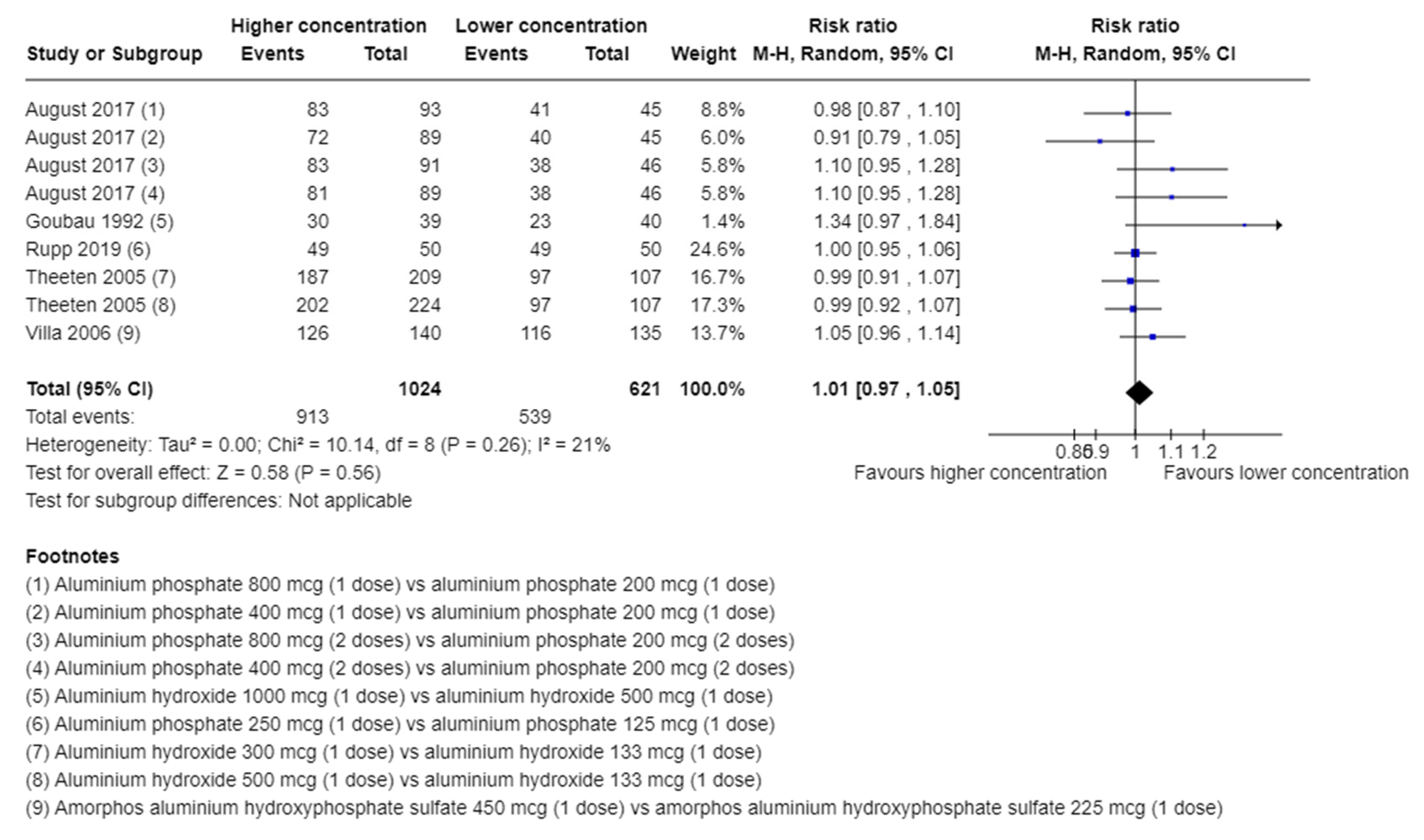
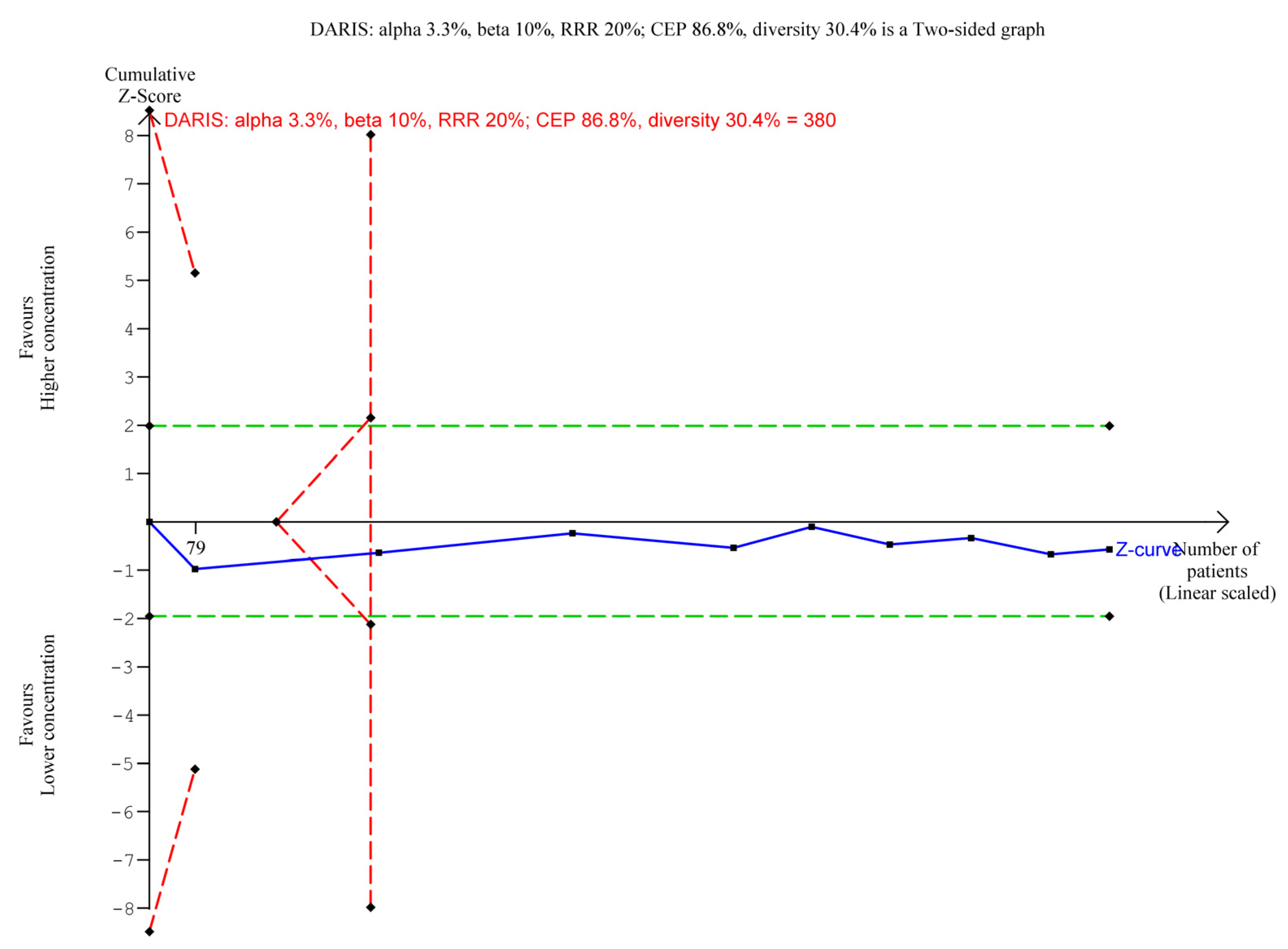
Adverse Events Not Considered Serious
Serological Response
3.3.2. Comparison 2: Higher vs. lower Number of Doses of Aluminium Adjuvants
All-Cause Mortality
Serious Adverse Events
Adverse Events Not Considered Serious
Serological Response
3.3.3. Comparison 3: Aluminium Phosphate Adjuvant Compared with Aluminium Hydroxide Adjuvant
All-Cause Mortality
Serious Adverse Events
Adverse Events Not Considered Serious
Serological Response
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fedson, D.S. Measuring protection: Efficacy versus effectiveness. Dev. Biol. Stand. 1998, 95, 195–201. [Google Scholar] [PubMed]
- Kocourkova, A.; Honegr, J.; Kuca, K.; Danova, J. Vaccine Ingredients: Components that Influence Vaccine Efficacy. Mini Rev. Med. Chem. 2017, 17, 451–466. [Google Scholar] [CrossRef] [PubMed]
- O’Hagan, D.T.; De Gregorio, E. The path to a successful vaccine adjuvant—‘the long and winding road’. Drug Discov. Today 2009, 14, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Coffman, R.L.; Sher, A.; Seder, R.A. Vaccine adjuvants: Putting innate immunity to work. Immunity 2010, 33, 492–503. [Google Scholar] [CrossRef] [PubMed]
- Carter, D.; Reed, S.G. Role of adjuvants in modeling the immune response. Curr. Opin. HIV AIDS 2010, 5, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Reed, S.G.; Orr, M.T.; Fox, C.B. Key roles of adjuvants in modern vaccines. Nat. Med. 2013, 19, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
- Facciolà, A.; Visalli, G.; Laganà, A.; Di Pietro, A. An Overview of Vaccine Adjuvants: Current Evidence and Future Perspectives. Vaccines 2022, 10, 819. [Google Scholar] [CrossRef]
- Tritto, E.; Mosca, F.; De Gregorio, E. Mechanism of action of licensed vaccine adjuvants. Vaccine 2009, 27, 3331–3334. [Google Scholar] [CrossRef]
- CoronaVac. COVID-19 Vaccine (Vero Cell), Inactivated. 2021. Available online: www.extranet.who.int/pqweb/sites/default/files/documents/COR-WHO-Adu-40_vials-insert.pdf (accessed on 21 March 2023).
- WHO. Evidence Assessment: Sinopharm/BBIBP COVID-19 Vaccine. 2021. Available online: www.cdn.who.int/media/docs/default-source/immunization/sage/2021/april/2_sage29apr2021_critical-evidence_sinopharm.pdf (accessed on 21 March 2023).
- Masson, J.D.; Angrand, L.; Badran, G.; de Miguel, R.; Crépeaux, G. Clearance, biodistribution, and neuromodulatory effects of aluminum-based adjuvants. Systematic review and meta-analysis: What do we learn from animal studies? Crit. Rev. Toxicol. 2022, 52, 403–419. [Google Scholar] [CrossRef]
- Krauss, S.R.; Barbateskovic, M.; Klingenberg, S.L.; Djurisic, S.; Petersen, S.B.; Kenfelt, M.; Kong, Z.; Jakobsen, J.C.; Gluud, C. Aluminium adjuvants versus placebo or no intervention in vaccine randomised clinical trials: A systematic review with meta-analysis and Trial Sequential Analysis. BMJ Open 2022, 12, e058795. [Google Scholar] [CrossRef]
- Djurisic, S.; Jakobsen, J.C.; Petersen, S.B.; Kenfelt, M.; Klingenberg, S.L.; Gluud, C. Aluminium adjuvants used in vaccines. Cochrane Database Syst. Rev. 2018, CD013086. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; John Wiley & Sons: Chichester, UK, 2021. [Google Scholar]
- Jakobsen, J.C.; Wetterslev, J.; Winkel, P.; Lange, T.; Gluud, C. Thresholds for statistical and clinical significance in systematic reviews with meta-analytic methods. BMC Med. Res. Methodol. 2014, 14, 120. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Sterne, J.A. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions, Version 5.2.0; Higgins, J.P., Churchill, R., Chandler, J., Cumpston, M.S., Eds.; John Wiley & Sons: Chichester, UK, 2017. [Google Scholar]
- RevMan Web. Review Manager Web (RevMan Web) [Computer Program]. Version 4.27.0; The Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- TSA. Trial Sequential Analysis [Computer Program], Version 0.9.5.10 Beta; Copenhagen Trial Unit: Copenhagen, Denmark, 2020. [Google Scholar]
- Thorlund, K.; Engstrøm, J.; Wetterslev, J.; Brok, J.; Imberger, G.; Gluud, C. User Manual for Trial Sequential Analysis (TSA), 2nd ed.; Copenhagen Trial Unit: Copenhagen, Denmark, 2017. [Google Scholar]
- Demets, D.L. Methods for combining randomized clinical trials: Strengths and limitations. Stat. Med. 1987, 6, 341–350. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Pogue, J.M.; Yusuf, S. Cumulating evidence from randomized trials: Utilizing sequential monitoring boundaries for cumulative meta-analysis. Control Clin. Trials 1997, 18, 580–593. [Google Scholar] [CrossRef]
- Mascha, E.J. Alpha, beta, meta: Guidelines for assessing power and type I error in meta-analyses. Anesth. Analg. 2015, 121, 1430–1433. [Google Scholar] [CrossRef] [PubMed]
- Terkawi, A.S.; Mavridis, D.; Flood, P.; Wetterslev, J.; Terkawi, R.S.; Bin Abdulhak, A.A.; Nunemaker, M.S.; Tiouririne, M. Does ondansetron modify sympathectomy due to subarachnoid anesthesia? Meta-analysis, meta-regression, and Trial Sequential Analysis. Anesthesiology 2016, 124, 846–869. [Google Scholar] [CrossRef]
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 39. [Google Scholar] [CrossRef]
- Imberger, G.; Gluud, C.; Boylan, J.; Wetterslev, J. Systematic reviews of anesthesiologic interventions reported as statistically significant: Problems with power, precision, and type 1 error protection. Anesth. Analg. 2015, 121, 1611–1622. [Google Scholar] [CrossRef]
- Higgins, J.P.; Whitehead, A.; Simmonds, M. Sequential methods for random-effects meta-analysis. Stat. Med. 2011, 30, 903–921. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- GRADEpro GDT. GRADEpro Guideline Development Tool; McMaster University and Evidence Prime: Hamilton, ON, Canada, 2020. [Google Scholar]
- Murphy, M.D.; Rasnack, J.; Dickson, H.D.; Dietch, M.; Brunell, P.A. Evaluation of the pertussis components of diphtheria-tetanus-pertussis vaccine. Pediatrics 1983, 71, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Goubau, P.; Van Gerven, V.; Safary, A.; Delem, A.; Knops, J.; D’Hondt, E.; André, F.E.; Desmyter, J. Effect of virus strain and antigen dose on immunogenicity and reactogenicity of an inactivated hepatitis A vaccine. Vaccine 1992, 10 (Suppl. S1), S114–S118. [Google Scholar] [CrossRef]
- de Kleijn, E.D.; de Groot, R.; Lafeber, A.B.; Labadie, J.; van Limpt, K.C.; Visser, J.; Berbers, G.A.; van Alphen, L.; Rümke, H.C. Immunogenicity and safety of monovalent p1.7(h),4 meningococcal outer membrane vesicle vaccine in toddlers: Comparison of two vaccination schedules and two vaccine formulations. Vaccine 2000, 19, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Theeten, H.; Van Damme, P.; Hoppenbrouwers, K.; Vandermeulen, C.; Leback, E.; Sokal, E.M.; Wolter, J.; Schuerman, L. Effects of lowering the aluminium content of a dTpa vaccine on its immunogenicity and reactogenicity when given as a booster to adolescents. Vaccine 2005, 23, 1515–1521. [Google Scholar] [CrossRef] [PubMed]
- Villa, L.L.; Ault, K.A.; Giuliano, A.R.; Costa, R.L.; Petta, C.A.; Andrade, R.P.; Brown, D.R.; Ferenczy, A.; Harper, D.M.; Koutsky, L.A.; et al. Immunologic responses following administration of a vaccine targeting human papillomavirus Types 6, 11, 16, and 18. Vaccine 2006, 24, 5571–5583. [Google Scholar] [CrossRef] [PubMed]
- NCT00562237. Immunogenicity and Safety of Two Adjuvant Formulations of an Egg-Derived Pandemic Vaccine [Randomized, Observer-Blind, Placebo-Controlled Study to Assess the Immunogenicity and Safety of Two Adjuvant Formulations of an Egg-derived Pandemic Surface Antigen Influenza Vaccine in Healthy Adults Aged ≥18 Years and ≤49 Years]. 2007. Available online: https://clinicaltrials.gov/ct2/show/NCT00562237 (accessed on 23 July 2023).
- Leroux-Roels, G.; Clément, F.; Vandepapelière, P.; Fourneau, M.; Heineman, T.C.; Dubin, G. Immunogenicity and safety of different formulations of an adjuvanted glycoprotein D genital herpes vaccine in healthy adults: A double-blind randomized trial. Hum. Vaccin. Immunother. 2013, 9, 1254–1262. [Google Scholar] [CrossRef]
- Schwameis, M.; Roppenser, B.; Firbas, C.; Gruener, C.S.; Model, N.; Stich, N.; Roetzer, A.; Buchtele, N.; Jilma, B.; Eibl, M.M. Safety, tolerability, and immunogenicity of a recombinant toxic shock syndrome toxin (rTSST)-1 variant vaccine: A randomised, double-blind, adjuvant-controlled, dose escalation first-in-man trial. Lancet Infect. Dis. 2016, 16, 1036–1044. [Google Scholar] [CrossRef]
- August, A.; Glenn, G.M.; Kpamegan, E.; Hickman, S.P.; Jani, D.; Lu, H.; Thomas, D.N.; Wen, J.; Piedra, P.A.; Fries, L.F. A Phase 2 randomized, observer-blind, placebo-controlled, dose-ranging trial of aluminum-adjuvanted respiratory syncytial virus F particle vaccine formulations in healthy women of childbearing age. Vaccine 2017, 35, 3749–3759. [Google Scholar] [CrossRef]
- Rupp, R.; Hurley, D.; Grayson, S.; Li, J.; Nolan, K.; McFetridge, R.D.; Hartzel, J.; Abeygunawardana, C.; Winters, M.; Pujar, H.; et al. A dose ranging study of 2 different formulations of 15-valent pneumococcal conjugate vaccine (PCV15) in healthy infants. Hum. Vaccin. Immunother. 2019, 15, 549–559. [Google Scholar] [CrossRef]
- Vermont, C.L.; van Dijken, H.H.; van Limpt, C.J.; de Groot, R.; van Alphen, L.; van Den Dobbelsteen, G.P. Antibody avidity and immunoglobulin G isotype distribution following immunization with a monovalent meningococcal B outer membrane vesicle vaccine. Infect. Immun. 2002, 70, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; John Wiley & Sons: Chichester, UK, 2011. [Google Scholar]
- Jefferson, T.; Rudin, M.; Di Pietrantonj, C. Adverse events after immunisation with aluminium-containing DTP vaccines: Systematic review of the evidence. Lancet Infect. Dis. 2004, 4, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.J.; Shih, Y.J.; Chen, C.H.; Fang, C.T. Aluminum salts as an adjuvant for pre-pandemic influenza vaccines: A meta-analysis. Sci. Rep. 2018, 8, 11460. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- European Medicines Agency. Guideline for Good Clinical Practice E6(R2); European Medicines Agency: Amsterdam, The Netherlands, 2016. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-guideline-good-clinical-practice-e6r2-step-5_en.pdf (accessed on 14 October 2023).
- Chan, A.W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Study ID | Vaccine Indication | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 |
|---|---|---|---|---|---|---|---|
| August 2017 [38] | Respiratory Syncytial Virus | 800 mcg AlPO4 (2 doses) | 400 mcg AlPO4 (2 doses) | 200 mcg AlPO4 (2 doses) | 800 mcg AlPO4 | 400 mcg AlPO4 | 200 mcg AlPO4 |
| de Kleijn, 2000 [32] | Neisseria meningitidis | 860 mcg AlOH3 (2 doses) | 860 mcg AlOH3 (3 doses) | 1340 mcg AlPO4 (2 doses) | 1340 mcg AlPO4 (3 doses) | ||
| Goubau, 1992 [31] | Hepatitis A | 1000 mcg AlOH3 | 500 mcg AlOH3 | ||||
| Leroux-Roels, 2013 [36] | Genital herpes | 500 mcg AlOH3 | 500 mcg | ||||
| Murphy, 1983 [30] | Dipteria, tetanus, pertussis (dTp) | Alum (extracted Ag) | AlPO4 (extracted Ag) | Alum (whole cell Ag) | AlPO4 (whole cell Ag) | ||
| NCT00562237 [35] | Influenzae | 1250 mcg AlOH3 (2 doses) | 500 mcg AlOH3 (2 doses) | ||||
| Rupp, 2019 [39] | Streptococcus pneumonia | 250 mcg AlPO4 | 125 mcg AlPO4 | ||||
| Schwameis, 2016 [37] | Staphylococcus aureus | 1000 mcg AlOH3 | 600 mcg AlOH3 | 200 mcg AlOH3 | |||
| Theeten, 2005 [33] | Dipteria, tetanus pertussis (dTp) | 500 mcg AlOH3 | 300 mcg AlOH3 | 133 mcg AlOH3 | |||
| Villa, 2006 [34] | No antigen | 450 mcg AAHS | 225 mcg AAHS |
| Outcomes | Anticipated Absolute Effects ** (95% CI) | Relative Effect (95% CI) | No of Participants (Trials) | Certainty of the Evidence (GRADE) | |
|---|---|---|---|---|---|
| Risk with Lower Concentration or Doses, or Aluminium Hydroxide | Risk with Higher Concentration or Doses, or Aluminium Phosphate | ||||
| Comparison 1—Higher versus lower concentration of aluminium adjuvants | |||||
| All-cause mortality * | - | - | - | - | - |
| Participants with disease being vaccinated against * | - | - | - | - | - |
| Proportion of participants with serious adverse events | 5 per 1000 | 11 per 1000 (3 to 34) | RR 1.99 (0.63 to 6.29) | 919 (3 RCTs) | ⨁◯◯◯ Very low a,b,§ |
| Health-related quality of life * | - | - | - | - | - |
| Proportion of participants with adverse events not considered serious | 868 per 1000 | 877 per 1000 (842 to 911) | RR 1.01 (0.97 to 1.05) | 1645 (5 RCTs) | ⨁⨁◯◯ Low a,§ |
| Comparison 2—Higher versus lower number of doses of aluminium adjuvants | |||||
| All-cause mortality | not pooled | not pooled | not pooled ‡ | 672 (2 RCTs) | ⨁◯◯◯ Very low a,c,§ |
| Participants with disease being vaccinated against * | - | - | - | - | - |
| Proportion of participants with serious adverse events | 21 per 1000 | 13 per 1000 (4 to 42) | RR 0.62 (0.19 to 2.00) | 675 (2 RCTs) | ⨁◯◯◯ Very low a,b,§ |
| Health-related quality of life * | - | - | - | - | - |
| Proportion of participants with adverse events not considered serious | 868 per 1000 | 0 per 1000 (0 to 0) | not estimable | 544 (1 RCT) | ⨁◯◯◯ Very low a,d,§ |
| Comparison 3—Aluminium phosphate adjuvant versus aluminium hydroxide adjuvant | |||||
| All-cause mortality | not pooled | not pooled | not pooled ‡ | 188 (2 RCTs) | ⨁◯◯◯ Very low a,c,§ |
| Participants with disease being vaccinated against * | - | - | - | - | - |
| Proportion of participants with serious adverse events | 10 per 1000 | 31 per 1000 (1 to 730) | RR 3.00 (0.13 to 70.83) | 188 (2 RCTs) | ⨁◯◯◯ Very low a,b,§ |
| Health-related quality of life * | - | - | - | - | - |
| Proportion of participants with adverse events not considered serious | 500 per 1000 | 0 per 1000 (0 to 0) | not estimable | 60 (1 RCT) | ⨁◯◯◯ Very low a,d,§ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbateskovic, M.; Klingenberg, S.L.; Krauss, S.R.; Kong, D.; Wu, Z.; Petersen, S.B.; Kenfelt, M.; Gluud, C. Concentrations, Number of Doses, and Formulations of Aluminium Adjuvants in Vaccines: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Clinical Trials. Vaccines 2023, 11, 1763. https://doi.org/10.3390/vaccines11121763
Barbateskovic M, Klingenberg SL, Krauss SR, Kong D, Wu Z, Petersen SB, Kenfelt M, Gluud C. Concentrations, Number of Doses, and Formulations of Aluminium Adjuvants in Vaccines: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Clinical Trials. Vaccines. 2023; 11(12):1763. https://doi.org/10.3390/vaccines11121763
Chicago/Turabian StyleBarbateskovic, Marija, Sarah Louise Klingenberg, Sara Russo Krauss, Dezhao Kong, Zhangtong Wu, Sesilje B. Petersen, Mette Kenfelt, and Christian Gluud. 2023. "Concentrations, Number of Doses, and Formulations of Aluminium Adjuvants in Vaccines: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Clinical Trials" Vaccines 11, no. 12: 1763. https://doi.org/10.3390/vaccines11121763
APA StyleBarbateskovic, M., Klingenberg, S. L., Krauss, S. R., Kong, D., Wu, Z., Petersen, S. B., Kenfelt, M., & Gluud, C. (2023). Concentrations, Number of Doses, and Formulations of Aluminium Adjuvants in Vaccines: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Randomized Clinical Trials. Vaccines, 11(12), 1763. https://doi.org/10.3390/vaccines11121763